
Abstract
Background:
Interleukin-17 (IL-17), which is secreted by Th17 cells, is a proinflammatory cytokine that is implicated in the pathogenesis of multiple sclerosis (MS) and plays a role in nonresponse of MS patients to interferon-β (IFN-β) therapy.
Objectives:
The purpose of this study was to establish a correlation between nonresponders (NR) and IL-17A serum titers and binding antibodies (BAbs) to IFN-β, as well as to find a correlation between IL-17A serum levels and other features of MS patients.
Methods:
Our prospective study included 72 inactive relapsing–remitting multiple sclerosis (RRMS) patients that had been treated for at least 18 months with IFN-β and 15 healthy subjects. We determined the serum levels of IL-17A and of BAbs. IL-17A levels were considered elevated (IL-17A+) if the recorded value was greater than 1.6 pg/ml.
Results:
Twenty-seven patients (37.5%) were NR and had a significantly higher serum IL-17A level compared to the responders group. Nineteen patients (26.4%) were IL-17A+ and had had a significantly higher number of relapses in the previous year and a higher Expanded Disability Status Score. The majority of IL-17A+ patients were NR and had a shorter MS duration.
Conclusions:
RRMS patients with high serum IL-17A levels do not respond well to IFN-β therapy and have shorter MS duration compared to patients with low IL-17A levels. This response is not influenced by the presence of BAbs.
Keywords
Introduction
Until recently, relapsing–remitting multiple sclerosis (RRMS) was considered a homogeneous form of multiple sclerosis (MS). Variability both in the immunopathology of active demyelinating lesions in MS and in response to immunomodulatory treatments has demonstrated that RRMS is a heterogeneous form of MS. 1,2
An overwhelming number of trials have supported the use of interferon-β (IFN-β) as a first-line immunomodulatory treatment in RRMS. Approximately 30% of IFN-β treated RRMS patients are nonresponders (NR) to treatment. Despite vast clinical experience in the use of IFN-β, its mechanisms of action have not been fully clarified. 3
Interleukin-17 (IL-17) is a proinflammatory cytokine that is secreted by a lineage of T cells named Th17 cells. The Th17 chemokine pathways are essential for the development of central nervous system (CNS) autoimmune diseases such as MS. A high IL-17 concentration in the serum of people with RRMS is associated with nonresponse to IFN-β therapy. Some animal and human studies have shown that IFN-β inhibits the activity of Th17 cells. 4 –6
One consequence of IFN-β treatment is the development of binding antibodies (BAbs). BAbs can bind to the IFN-β molecule at a variety of locations, and some of these interactions inhibit IFN-β receptors and determine the appearance of neutralizing antibodies (NAbs). 7
Objectives
The primary objective was to establish a correlation between NR to IFN-β treated RRMS patients and the IL-17A serum titer and BAbs.
The secondary objectives were to determine: (a) whether the pathological increase of IL-17A serum levels correlates with the presence of BAbs or with other MS patient characteristics (age, gender, number of MS relapses, Expanded Disability Status Score (EDSS), MS duration, changes in the EDSS in the previous year, type of the IFN-β administrated); (b) whether there are correlations between IL-17A and BAbs titers and the above mentioned patient characteristics; (c) the clinical characteristics of NR patients.
Materials and methods
Patients
Our study was a prospective study that included 72 RRMS patients (70.83% women, 29.17% men, median age 36.7 years) treated in the Regional MS Centre, Târgu Mureş, Romania and 15 healthy subjects. Eligible patients had RRMS according to the revised McDonald criteria. 8
All patients had inactive RRMS (no relapse one month before blood collection) and had been treated for at least 18 months with IFN-β (Avonex, Rebif, Betaferon). Patients were excluded if: (a) they had been treated in the last 30 days with methylprednisolone; (b) they had changed their IFN-β preparation within the last 18 months; (c) they had other chronic diseases associated with MS; (d) they had been previously treated with immunosuppressive agents.
All of the patients and healthy subjects had negative blood tests for other auto-immune or infectious diseases, including: antiphospholipid syndrome, lupus, Lyme disease, Human Immunodeficiency Virus (HIV) and syphilis.
Informed consent was obtained from all of the subjects. The study was approved by the local ethics committee and was carried out according to the Declaration of Helsinki.
All of the patients were neurologically examined both 12 months before IL-17A testing and at the time of testing. In addition, for each RRMS patient, we obtained the following: (a) demo-graphic data; (b) medical history; (c) age; (d) MS duration; (e) EDSS; (f) changes in EDSS within the last 12 months of treatment; (g) number of relapses in the last year.
The patients were classified according to treatment response as either responders (RS) (no relapse or an increase of 0.5 points or less on the EDSS in the previous year under IFN-β therapy) or NR (minimum one relapse and/or an increase of at least 1 EDSS point in the last year).
IL-17A measurement
Blood samples were collected at least 24 hours after the last IFN-β injection. Serum was obtained by centrifugation at 2000 x g for 15 m and stored at −70°C until all of the samples were gathered. The blood collection, period for the IL-17A and BAbs measurements was from 1 July 2010–15 December 2011. IL-17A and BAbs serum titers were determined in 15 healthy blood donors whose age and gender were comparable to the patients. A DRG International IL-17A semiquantitative Enzyme-linked immunosorbent assay (ELISA) kit (code DRG, EIA-4840) was used for the semiquantitative detection of human IL-17A. According to the kit instructions provided, IL-17A levels were considered ‘elevated’ if the measured value exceeded 1.6 pg/ml (patients considered IL-17A+). The serum IL-17A value for each patient was noted. For the statistical measurements, values ≤1.6 pg/ml were recorded as 0, and the patient was considered IL-17A–. Even if such data transformation were necessary, due to the type of the ELISA test we had at our disposal, and even if we accept that this is an important limitation and drawback of our data analysis, we may still conclude that the reported statistical significance is real. We are aware that one limitation of our results is the large standard deviation in the IL-17A titer values. In healthy subjects, all of the IL-17A levels were ≤1.6 pg/ml.
BAbs measurement
Our study was based on BAbs measurements, but we did not survey NAbs for technical reasons. BAbs were determined using a direct quantitative test, the Buhlmann anti-IFN-β antibodies ELISA kit. Patients were considered BAbs+ if they had a positive sample with an optical density (OD) that was higher than the mean+3×standard deviation (SD) of the OD of the control sample. 5,7
Statistical methods
The groups were compared using the Mann-Whitney non-parametric test, and correlation analyses were conducted using the Spearman rank correlation coefficient. Logistic regression analysis was used to determine patient characteristics with the RS and NR as one criterion and serum IL-17A+ versus IL-17A– status, as the other. All reported p values are based on two-tailed statistical tests, with a significance level of 0.05. Before using the above tests, we applied the Kolmogorov-Smirnov Normality Test, which indicated that our data followed a non-Gaussian distribution, thus non-parametric statistical tests were required. 9
Results
The main clinical and therapeutic features of RRMS patients are summarized in Table 1. Likewise, we included the characteristics of patient subgroups in the same table: RS, NR, IL-17A+, IL-17A– and healthy subjects.
Demographics, clinical and therapeutic characteristics of the relapsing–remitting multiple sclerosis (RRMS) patients and controls.
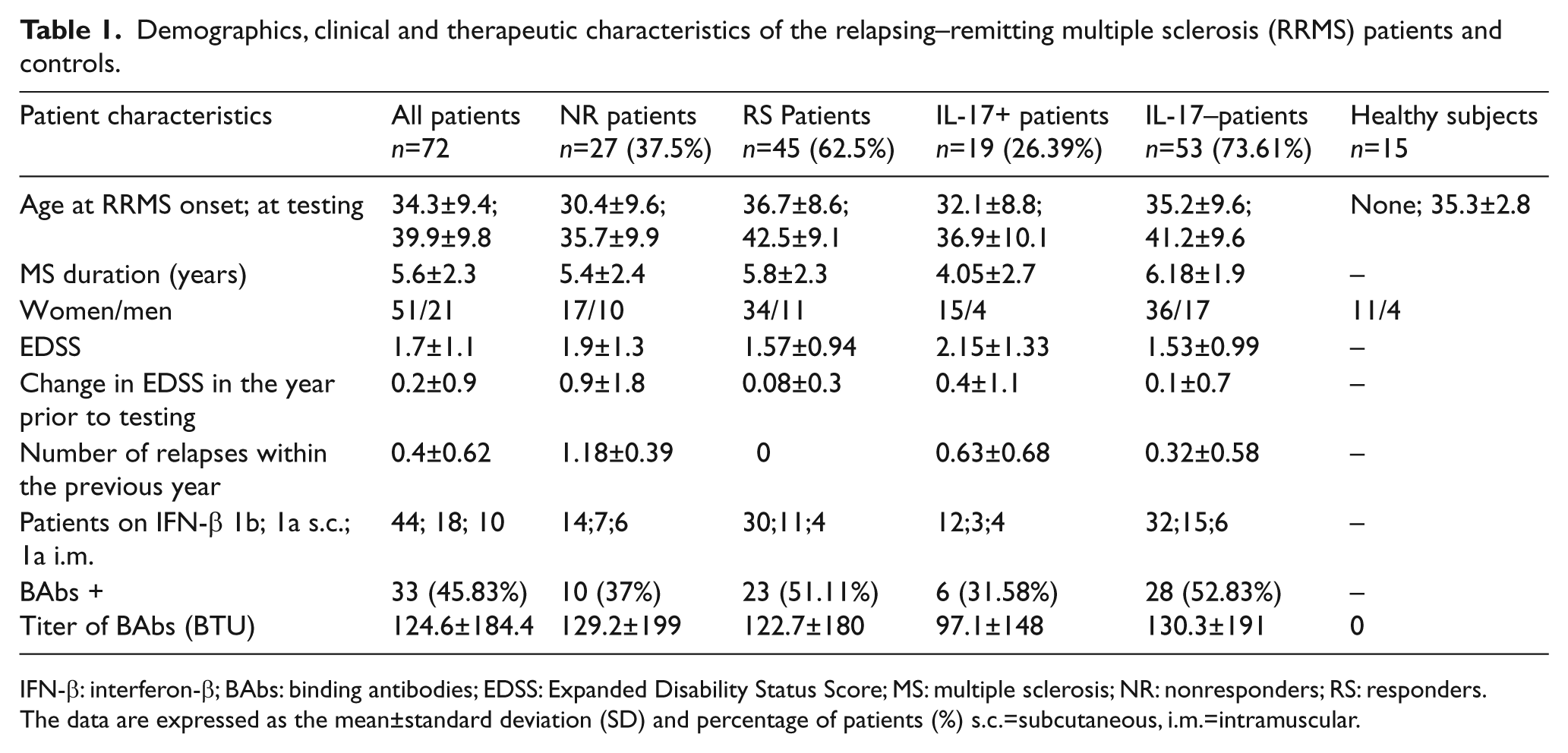
IFN-β: interferon-β; BAbs: binding antibodies; EDSS: Expanded Disability Status Score; MS: multiple sclerosis; NR: nonresponders; RS: responders.
The data are expressed as the mean±standard deviation (SD) and percentage of patients (%) s.c.=subcutaneous, i.m.=intramuscular.
By dividing the patients into the RS and NR groups, we found that 27 (37.5%) were NR, and they had a significantly higher level of serum IL-17A versus the RS group (p=0.02; Mann-Whitney test).The mean serum level of IL-17A in the NR group was 9.98±22 pg/ml. In contrast, the MS cases that had no relapse and stable EDSS had an IL-17A with a relative mean value of 1.78±6.74 pg/ml (Figure 1).
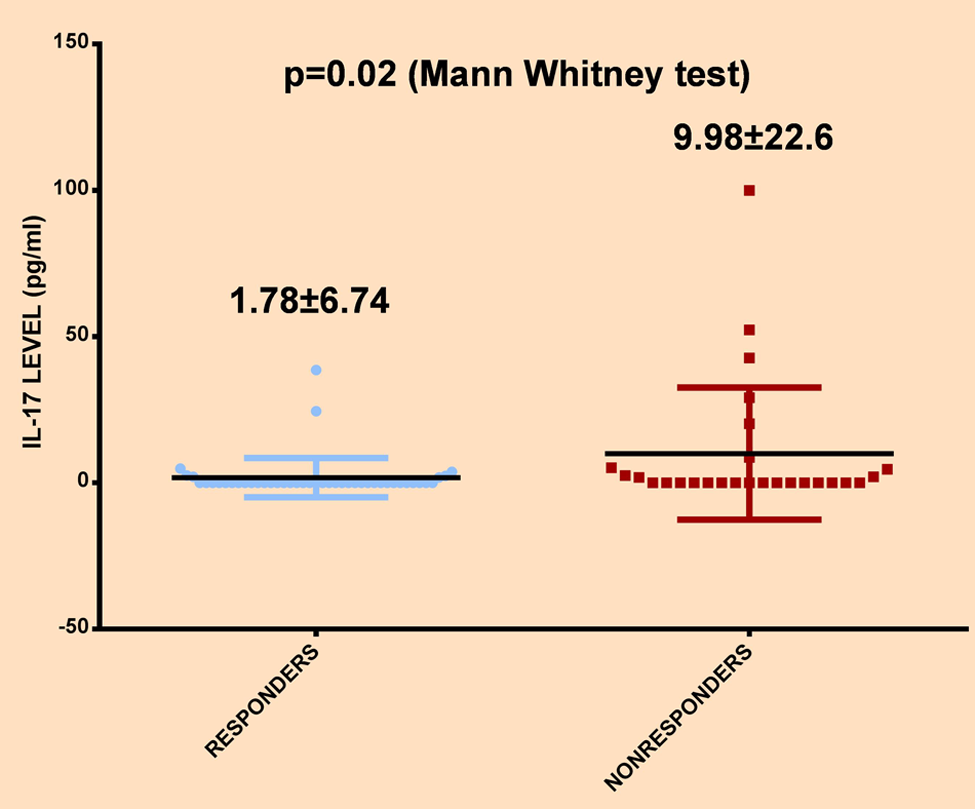
IL-17A level (pg/ml) in responders and nonresponders. Scatter dot plot.
As shown in Table 1, patients in the NR group had a higher EDSS than the RS (1.9 versus 1.57), but the difference was not statistically significant. The mean change in EDSS was higher in the NR group versus the RS group (according to the NR definition the difference was significant). No other significant differences were found with regards to gender, age, disease duration, type of IFN-β used, BAbs presence or titer between the RS and the NR groups.
A total of 19 patients (26.39%) had IL-17A titers above 1.6 pg/ml (18.4±15.4 pg/ml). Comparing the IL-17A+ and IL-17A– patients, we found that the IL-17A+ patients had a significantly higher number of relapses within the previous year (0.63 versus 0.32; p=0.04, Mann-Whitney test) and a higher EDSS (2.15 versus 1.53; p=0.05, Mann-Whitney test) in comparison with the rest of the patients. The difference in EDSS between these groups of patients showed a trend toward aggravation in the IL-17A+ patients, but the differences were not statistically significant (p=0.054).
A very interesting and convincing result was that the IL-17A+ patients had a significantly lower RRMS duration than the IL-17A– patients: the shorter the MS duration, the higher the IL-17A titer (4.05 versus 6.18 years; p=0.002, Mann-Whitney test) (Figure 2). In this group of 19 IL-17A+ patients, 10 (52.63%) were NR; in contrast, among the 53 IL-17A– patients, 17 (32.07%) were NR. This result was statistically significant. No other differences were found with regards to gender, age (both of MS onset and at time of the study), type of IFN-β, BAbs presence and titer between the two groups of patients.
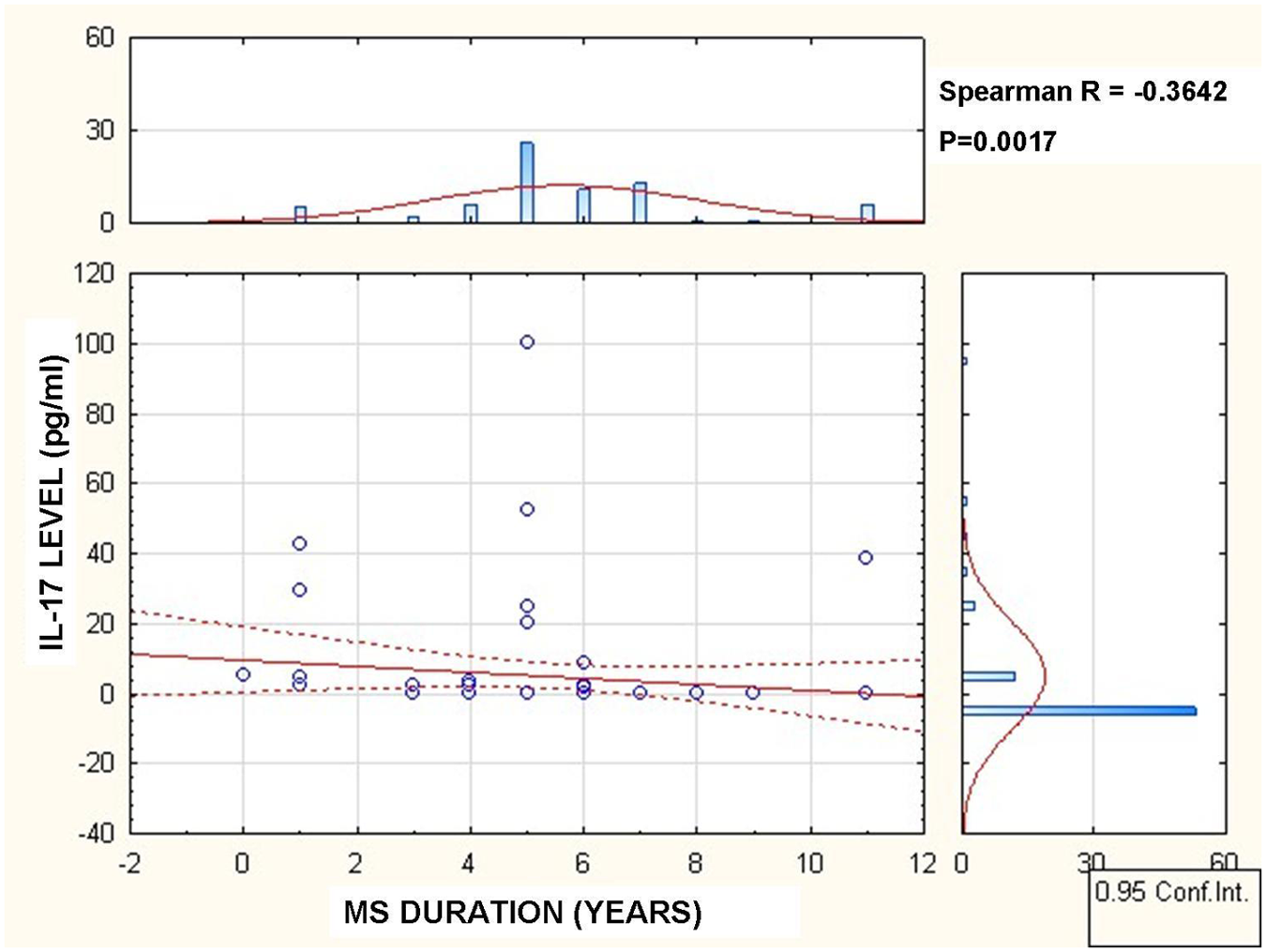
Correlation between relapsing–remitting multiple sclerosis (RRMS) duration and IL-17A serum titer.
When we analyzed the correlation between the IL-17A titers and different characteristics, we found interesting results. The mean IL-17A serum value correlated significantly and directly with the number of relapses (p<0.05) and the change in EDSS (p=0.05) but did not correlate with age at MS onset or age at inclusion, gender, BAbs or type of IFN-β used.
Discussion
IFN-β acts principally by inhibiting T-cell activation and migration into the CNS. It also diminishes the release of pro-inflammatory cytokines in the periphery and likely into the CNS. 10 A major limitation of IFN-β is persistence of MS activity despite treatment in approximately 30% of RRMS patients that are considered NR, according to proposed response criteria. 1,11,12
Like other authors, we have assumed that the best way to evaluate the patients’ response to IFN-β was through the number of relapses, EDSS and change in EDSS during the previous year of treatment. 1,13,14
The limitations of some previous studies include the lack of control for BAbs/NAbs in MS patients treated with IFN-β and the timing of sample collection in relation to IFN-β injection. We tested patients who had received IFN-β treatment for a minimum of 18 months, and the sample collection occurred at least 24 h after IFN-β injection. 5,7
The role of IL-17 in MS pathology is partially known. Axtell et al. 15 examined a group of RRMS patients according to relapse rates after IFN-β therapy. Both IL-17 and endogenous IFN-β serum levels, measured before IFN-β treatment, were elevated in NR patients to IFN-β compared to RS patients.
Similar to Axtell et al. 15 we found significant correlations between IL-17A+ status and the relapse rate, as well as EDSS. Both measurements establish the profile of NR to IFN-β therapy. In contrast, Bushnell et al. 16 were unable to validate a correlation between serum IL-17F, either pre- or post-IFN-β treatment, and as good or poor response to IFN-β. Differences in patient populations and methodology might explain this discrepancy. The ideal situation would be to analyze IL-17 serum levels pre- and post-treatment with IFN-β, the findings helping to see the in vivo effect of IFN-β towards IL-17.
Durelli et al. 11 demonstrated that patients with active MS (a relapse within 10 days) had a significant increase in peripheral blood Th17 lymphocytes compared with inactive MS patients.
Although an increase in Th17 lymphocytes is associated with disease activity in MS, we included only inactive RRMS patients who had not received corticosteroids for at least 30 days so that the IL-17A and BAbs measurements would be more accurate. In our study, the number of relapses correlated significantly with IL-17A levels, which proved that this cytokine plays a role in inflammation and its clinical counterpart in the relapses.
Data from the main MS series describing the long term of MS natural history shows that relapse rate declines with disease duration; 0.5 is an estimated yearly relapse rate in the first years of RRMS evolution. 17 Our mean annual relapse rate was 0.63 and did not correlate with MS duration . The issue remains open as to whether a higher relapse rate is ‘normal’ in the first years of MS evolution or a high IL-17 serum level determines a high relapse rate. Gathering a bigger sample might help to solve this problem and verify our results. Usually, findings based on small numbers of patients have to be validated using larger cohorts.
Changes in the EDSS that indicate disease aggravation can occur as a result of the neurodegeneration of demyelinated axons or as a result of an incomplete recovery after a relapse, which explains why this parameter had a trend towards, but no significant correlation with, the presence of, or levels of, IL-17. The role of IL-17 in pathogenesis of inflammation in MS, but not in the neurodegenerative phase, has been demonstrated. 18 –20
Michalowska-Wender et al. 18 studied the expression of IL-17 receptor (IL-17R) in 20 RRMS patients treated with IFN-β. They found that IL-17R levels were upregulated in the early period of IFN-β therapy but did not correlate with other parameters. Durelli et al. 11 and Ramgolam et al. 21 showed that IFN-β1a exerts its ameliorating effect in part through Th17 cells inhibition, which indicates that Th17 cells have an immunopathologic role in MS. The proposed mechanisms of action of IFN-β include the reduction of IL-1β, IL-23 and TGF-β, which induce Th17 cell differentiation, and the stimulation of IL-10, IL-27, IL-12 and IL-4, which suppress Th17 cell differentiation. 21,22 Investigations into experimental autoimmune encephalomyelitis (EAE) found that Th17 cells play an important role in demyelination processes, but the EAE model is not totally applicable in MS. 23 If we want to confirm that Th17 cells are driving MS disease in the NR patients, we should analyze other Th17 biomarkers, like IL-23 that regulates Th17 function during disease pathogenesis. 23
Our data shows that the NR group had a significantly higher level of serum IL-17A versus the RS group. The ameliorating effect of IFN-β is only partially attributable to the inhibition of Th17 cells. 23 Axtell et al. 4 and Comabella et al. 24 indicate that IFN-β is ineffective and might worsen clinical status in MS when a Th17 immune response is pre-eminent; Bushnell et al. 16 could not confirm these findings. Probably IFN-β does not sufficiently induce a Th17 inhibition specially in MS patients that have a high serum IL-17 level. 17,21,22 Also, it is possible that IL-17+ T cells are attracted to the CNS, or are expanded in the CNS and that they release neurotoxic products and lead to demyelination. 25 Our results do not confirm those of Durelli et al. and Ramgolam et al., but the effect of IFN-β on Th17 cells in humans must be extensively studied. The answer to this question might be the Th17/Th1 phenotypes in MS.
We found that IL-17A+ patients had a significantly lower MS duration compared to IL-17A– patients. The hypothesis that IL-17 plays a more important pathogenic role in the early phase of MS was suggested by Frisullo et al. 19 and Graber et al. 26 who found higher spontaneous production of IL-17 in patients with clinically isolated syndrome (CIS) and early MS.
We must remember that if serum IL-17 in the periphery is low, its role in the CNS might be important because IL-17 can disrupt the blood brain barrier (BBB), and Th17 cells can then penetrate the BBB. IL-17 receptors are present in MS at inflamed endothelium lesion sites, suggesting that IL-17 may potentiate the migration of inflammatory T cells across the BBB. 27 It is possible that IL-17 functions in the periphery in the early phases of MS. Later, its role becomes more important in the CNS, as IL-17 induces potent astrocyte activation and astrocytes can produce IL-17 under the influence of activating stimuli such as inflammatory cytokines. The biological roles of Th17 cells and IL-17 might be considered to be a proinflammatory loop in the brain. 25,28
In our study, there were no correlations between the type of IFN-β used and IL-17A titers, which means that serum IL-17A is not IFN-β type dependent. An in vitro study, performed by Durelli et al., 11 showed that the greater the concentrations of IFN-β the more important was the enhancement of Th17 lymphocytes apoptosis in peripheral blood mononuclear cells.
In our series, 27 patients were NR, which is greater than the number of IL-17A+ patients, so there must be other reasons why patients who are diagnosed correctly, and treated with immunomodulators, have ongoing inflammation in the CNS which leads to relapses and increased neurological disability. We chose RRMS patients treated for a minimum period of 18 months with the same IFN-β because in this interval of time both BAbs, and their subset NAbs, in the majority of cases finish the process of transformation from positive into negative. According to our previously published data, BAbs do not abrogate the clinical effect of IFN-β regardless of the clinical parameter used. 7 Pachner et al. 29 reported that NAbs measurements have some important disadvantages: they are time consuming and expensive and only indirectly measure antibodies. NAbs do not appear in patients with BAbs negative tests. The risk of NAbs is genetically influenced. 30 Goodin et al. 31 did not find a negative impact of NAbs on clinical measurements, but they did find a negative impact on Magnetic Resonance Imaging (MRI) aspects (a clinic-radiographic paradox).
A study is needed to measure NAbs in relation to IL-17. However, our study provides an indirect conclusion regarding the lack of direct correlation between IL-17A and NAbs by showing that there is no difference among patients regardless of type of IFN-β used, however NAbs are much more frequent in patients treated with IFN-β1b. 7,32
In this equation, there are two unknown variables: one is the pathogenesis of RRMS, and the other is the mechanism of action of IFN-β. One possible link might be IL-17. Focusing only on IL-17 as the effector cytokine is too simplistic. Th17 cells are unlikely to be the sole players in driving tissue damage in MS. There is a need for biomarkers and predictors of treatment responsiveness for the early recognition of NR to prevent the accumulation of disability. 33,34
Conclusions
IL-17A might play a role in RRMS pathogenesis, mainly in the first years of disease evolution. RRMS patients with high serum IL-17A levels demonstrate a poorer response to IFN-β than the patients with low IL-17A serum levels. This response is not influenced by the presence of BAbs. Serum IL-17A concentrations are associated with patients who are NR to IFN-β therapy. The role of Th17 cells in MS pathogenesis remains to be better clarified, given that it might become a target in MS treatment.
Footnotes
Funding
This paper is partially supported by the Sectoral Operational Programme for Human Resources Development, financed by the European Social Fund and by the Romanian Government under contract number POSDRU/85/1.5/S64109.
Conflict of interest
R Bălaşa has received honoraria from Bayer Shering, Merck Serono, Teva, Novartis and Biogen Idec for speaking and for consulting services.