
Abstract
Background:
Limited information is available on the use of natalizumab (NA) in pediatric multiple sclerosis (ped-MS) patients.
Objective:
The purpose of this study was to describe the long-term effects of NA in a large cohort of active ped-MS patients.
Methods:
Patients with definite ped-MS were treated with NA if in the previous year they had experienced at least two relapses or a severe relapse with incomplete recovery while on immunomodulating treatment, or at least two relapses and new magnetic resonance imaging (MRI) lesions regardless of any prior treatment.
Results:
The study included 55 patients (mean age: 14.4 years, mean number of relapses: 4.4, pre-treatment mean disease duration: 25.5 months). They received a median number of 26 infusions. Three relapses occurred during the follow-up, one female patient continued to deteriorate in cognitive functioning. Mean Expanded Disability Status Scale (EDSS) scores decreased from 2.7 to 1.9 at the last visit (p<0.001). During the follow-up the majority of patients remained free from MRI activity. Transient and mild clinical adverse events occurred in 20 patients. Mild hematological abnormalities occurred in seven patients. Anti-JCV antibodies were detected in 20/51 tested patients.
Conclusions:
NA was well tolerated in all patients. A strong suppression of disease activity was observed in the majority of patients during the follow-up.
Introduction
Interferon-beta (IFNβ) and glatiramer acetate (GA) have not been formally tested in pediatric multiple sclerosis (ped-MS) patients with a relapsing–remitting course during placebo-controlled trials. However, class III and IV evidence of effectiveness resulting from observational open-label studies have prompted their current use and recommendation. 1 –3 Nonetheless, in about 30% of ped-MS patients, the disease continues to be active despite immunomodulatory treatment, supporting the need to explore other therapeutic options. 4 Natalizumab (NA) is considered an attractive therapeutic opportunity, since it exerts robust effects in reducing clinical and magnetic resonance imaging (MRI) activity in adult patients with MS. 5,6 In ped-MS, NA was reported to be safe and effective in few single case reports 7 –10 and in two studies including 19 11 and 24 patients, 12 with a mean follow-up of 15 and 18 months respectively.
In this study, we describe the effects of NA treatment in a large cohort of ped-MS patients, also providing data from a long-term follow-up, with particular emphasis on the frequency of relapses, modification of disability as measured on EDSS, appearance of new lesions on T2-weighted sequences and gadolinium (Gd)-enhancing lesions on brain MRI, and adverse events associated with treatment.
Patients and methods
A spontaneous, non-sponsored, prospective, cooperative study, coordinated by the Italian MS Study Group-Italian Society of Neurology, was started in 2007 within the network of Italian MS Centers, with the aim of collecting MS cases treated with NA before 18 years of age and included in the Italian Medicine Agency (Agenzia Italiana del Farmaco (AIFA)) registry. Treatment with NA (300 mg i.v. every four weeks) in these patients was started based on AIFA criteria, requiring that patients with definite relapsing–remitting MS have met either of the following criteria: (a) at least two relapses in the previous year or a severe relapse with incomplete recovery (Expanded Disability Status Scale (EDSS)≥2) during the treatment with IFNβ or GA; or (b) demonstration of rapidly evolving MS, with at least two relapses in the last year and appearance of new lesions on T2-weighted sequences or Gd-enhancing lesions at brain MRI, regardless any prior treatment. 13
A form already used in a previous study including 19 patients 11 was utilized by all centers to prospectively collect complete clinical and laboratory data. Complete blood cell count and hepatic and renal function were assessed monthly in the laboratories of individual centers; toxicity levels were defined according to the local standards. Clinical and neurological evaluation was performed monthly, by also rating the EDSS score. Relapses were defined as new, worsening, or recurrent neurologic symptoms (occurring at least 30 days after a preceding relapse), lasting at least 24 hours in the absence of fever or infections, and being accompanied by one of the following: an increase of at least half a point on the EDSS; an increase of at least one point in two functional-systems scores; or an increase of at least two points in one functional-system score (excluding changes in bowel or bladder function and cognition). Presence of anti-JCV antibodies in patients’ serum was assessed since the test Stratify JCVTM (performed at Unilabs, Copenhagen, Denmark) became available in Italy (March 2011). Neutralizing antibodies (NABs) against NA were measured in patients with occurrence of allergic reactions, clinical relapses or evidences of disease activity according to Italian guidelines. 13 All patients underwent conventional brain MRI locally at study entry and, with few exceptions, every six months thereafter; MRI exams included dual-echo and post-contrast T1-weighted scans and were performed with the use of 1.5 Tesla scanners, according to a previously described protocol. 11 The analysis of MRI scans was centrally performed at the Neuroimaging Research Unit, San Raffaele Hospital, Milan, Italy. At follow-up, the number of new lesions on T2-weighted sequences and Gd-enhancing lesions was counted.
The study was conducted in accordance with the International Conference on Harmonization Guidelines of Good Clinical Practice and the Declaration of Helsinki. The protocol received approval from an ethical committee on research involving human subjects (the Ethical Committee of the coordinating center). Written informed consent was obtained from each patient participating in the study (consent for research) and her/his parents or legal guardian.
The paired t-test was used to compare annualized relapse rate and EDSS score before and after NA treatment. A Kaplan-Meier curve was generated to estimate the percentage of patients free from disease activity (defined by the occurrence of relapses, EDSS worsening by ≥0.5 points, appearance of new lesions on T2-weighted sequences or Gd-enhancing lesions) during treatment with NA.
Results
Fifty-five patients (30 females, 25 males) with a mean age of 12.5±2.6 years at MS onset were included in the study. Forty-two patients fulfilled the criterion (a) and had been previously treated with one or more agents: IFNβ (33 patients; mean treatment duration: 14.6±14.0 months, range: 2–46), GA (six patients; mean treatment duration: 7.3±7.0 months, range: 2–23), mitoxantrone (three patients: mean number of infusions: 2.7, range: 1–4), cyclophosphamide (two patients; mean number of infusions: 2.7±1.5, range: 1–4), azathioprine (1 patient; treatment duration: 26 months), i.v. Ig associated to plasma exchange followed by mitoxantrone (1 patient: treatment duration: five months). These patients were slightly younger (12.3 vs 13.6 years, p=0.06), had a longer disease duration (28.9 vs 16.0 months, p=0.02) and a higher number of relapses (4.4 vs 2.9, p=0.004) before starting NA than patients with rapidly evolving MS and receiving NA as a first treatment (criterion (b)).
Table 1 summarizes the main demographic and clinical baseline characteristics of patients.
Main baseline demographic and clinical characteristics of the 55 pediatric multiple sclerosis (ped-MS) patients treated with natalizumab (NA).
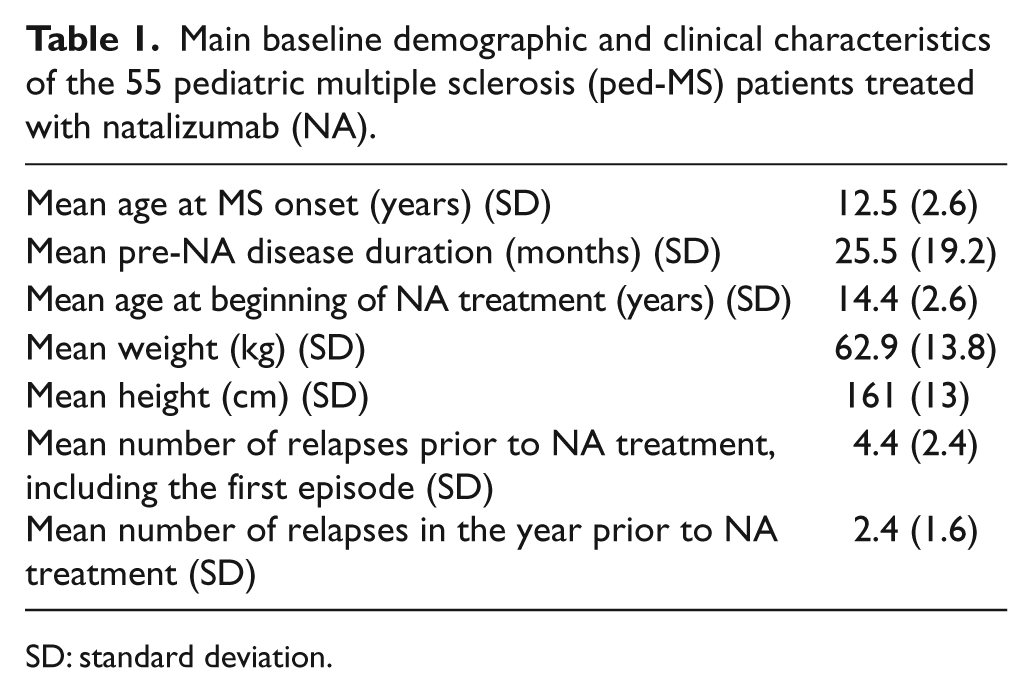
SD: standard deviation.
In the study cohort NA treatment was started at a mean age of 14.4±2.6 years, 25.5±19.2 months following disease onset with the occurrence of 4.4±2.4 total relapses (including the first episode). The mean interval between the last relapse and beginning of NA treatment was 79±49 days (range: 20–185). NA was administered every 28 days at the dose used in adults (300 mg), but in some cases infusion was delayed by a few days because of fever episodes or school/holiday scheduling. An average of 23.5±12.7 (median: 26, range: 5–52) infusions were administered during a mean follow-up of 23.3±12.8 months (median: 26, range: 5–53 months).
The annualized relapse rate decreased from 2.4±1.6 in the year prior to NA treatment to 0.1±0.2 (p<0.001) at the end of the treatment period.
Only three patients experienced relapses during treatment with NA in the entire cohort: one patient experienced a transitory worsening of pre-existing symptoms during and immediately after the first administration of NA (no additional therapy was required); another patient developed acute symptoms of brainstem, cerebellar and pyramidal dysfunction six months after NA initiation; the third patient reported visual loss after the sixth NA infusion. All cases (none of them showing antibodies against NA) recovered promptly after treatment with methylprednisolone 1 g i.v. for five consecutive days. Mean EDSS in the 55 subjects decreased from 2.7±1.2 (median: 2.5, range: 1-–6.5) at initiation of NA treatment to 1.9±1.2 (median: 1.5, range: 0–.5) at the time of last visit (p<0.001). EDSS remained stable in 13 cases, decreased by at least 0.5 point in seven cases, by 1 point in 13 cases, by ≥1.5 points in 18 cases, and increased by ≥0.5 point in three cases. One patient had no relapses but experienced a progressive deterioration of cognitive functions during the treatment period (see the Appendix).
Baseline MRI (performed within one month prior to starting NA) showed Gd-enhancing lesions in 45/55 (81.8%) patients (mean number of lesions: 4.5, median: 3, range: 1–25). New lesions on T2-weighted sequences or Gd-enhancing lesions were observed in 6/49 (12.2%) patients at six months, in 5/42 (11.9%) patients at 12 months (including the patient described in the Appendix, who discontinued NA for three months after the ninth infusion), in 2/29 (6.9%) patients at 18 months, in 1/27 (3,7%) patients at 24 months, and in 3/17 (17.6%) patients with a longer follow-up (Table 2).
Main magnetic resonance imaging (MRI) findings during natalizumab treatment.
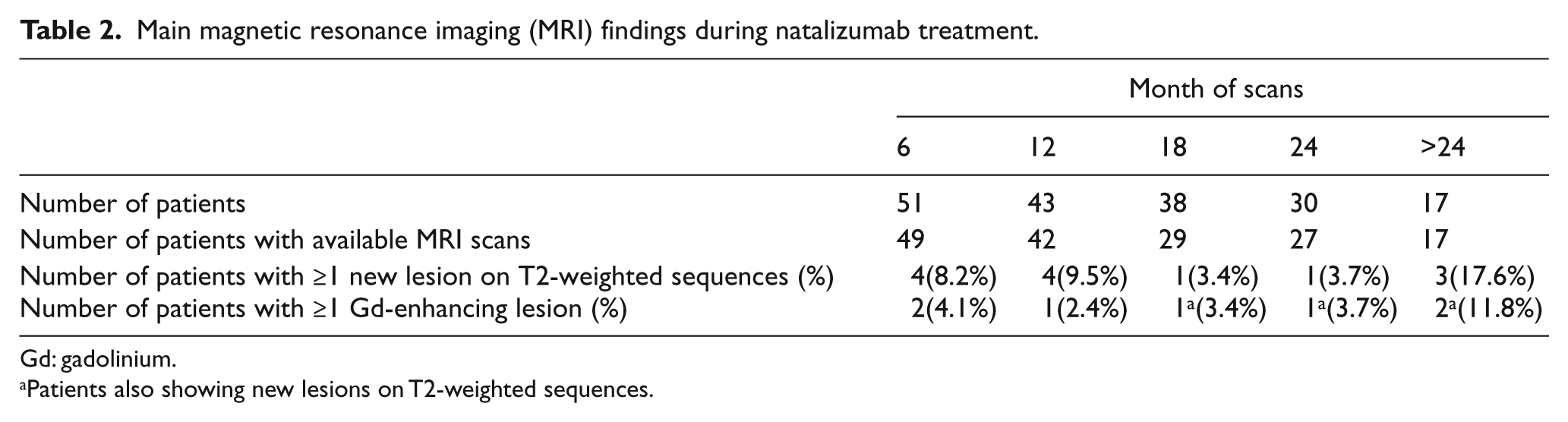
Gd: gadolinium.
Patients also showing new lesions on T2-weighted sequences.
Thirty patients were treated for 24 months or more, receiving a mean of 32.9±6.5 doses of NA. In this group only one relapse occurred and 19 patients (63%) remained free from relapses, new lesions on T2-weighted sequences or Gd-enhancing lesions during the follow-up; mean EDSS decreased from 2.6 ±1.2 (median: 2.5, range: 0–5) to 1.8±1.1 (median: 1.5, range: 0–4.5).
The frequency of patients free from clinical activity (neither relapses nor disability progression as measured by EDSS), MRI activity (no new lesions on T2-weighted sequences and no Gd-enhancing lesions), or both is reported in Figure 1: based on the defined criteria, 91%, 83% and 78% of patients and 88%, 74% and 66% were free from clinical, radiological or combined disease activity at the end of first and second year of treatment, respectively.
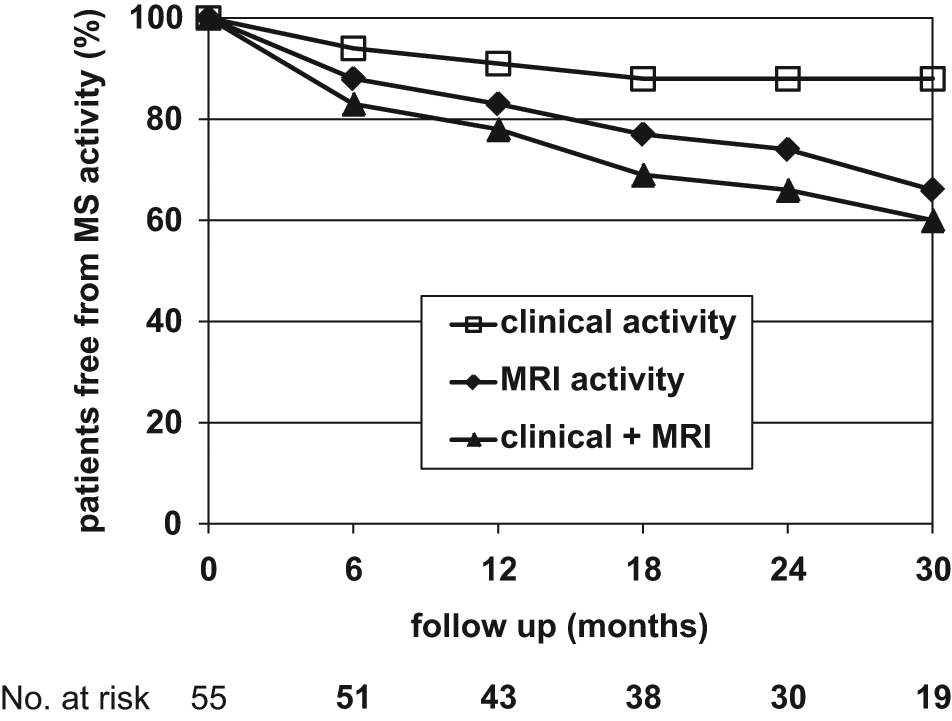
Kaplan-Meier estimates for the percentage of patients free from clinical, magnetic resonance imaging (MRI), and combined (clinical+MRI) disease activity.
Assessment of serum anti-JCV antibodies was performed in 51 patients, as four patients discontinued therapy before the test became available. The test was positive in 20 patients (39%, 13/32 of patients with criterion (a), 7/19 of those with criterion (b): only one had been previously treated with immunosuppressants and discontinued NA after nine monthly infusions (see Appendix). Six of the 20 positive patients discontinued NA treatment (Figure 2): two patients remained stable, two patients experienced relapses and restarted NA, one patient started GA treatment and developed a relapse after six months as well as Gd-enhancing lesions at MRI in two subsequent scans (after three and six months of GA treatment); the remaining subject progressively worsened despite treatment with IFNβ and azathioprine (see Appendix).
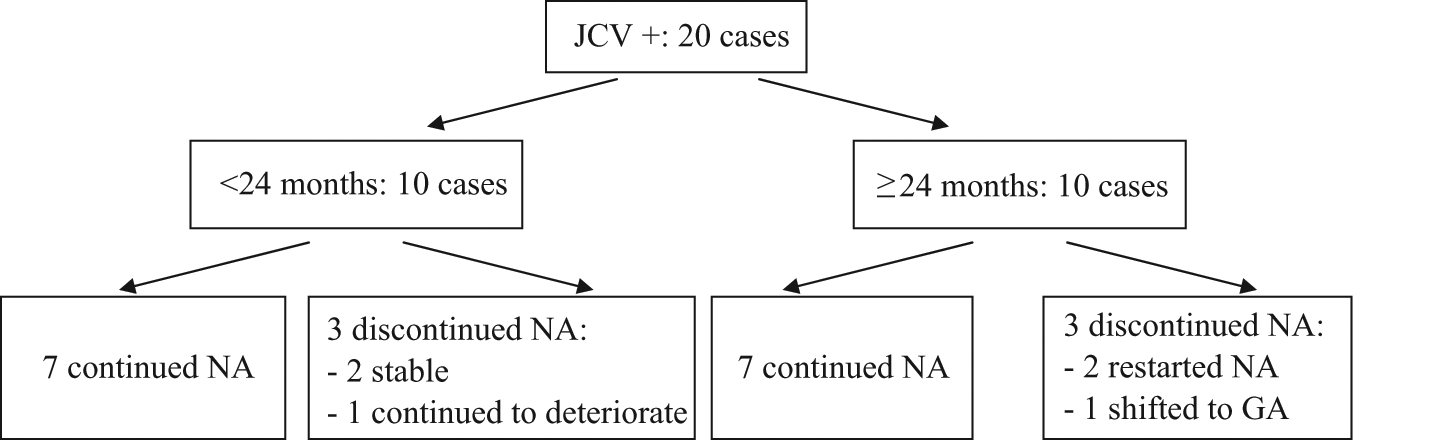
Clinical outcomes in patients with positivity at test for anti-JCV antibody.
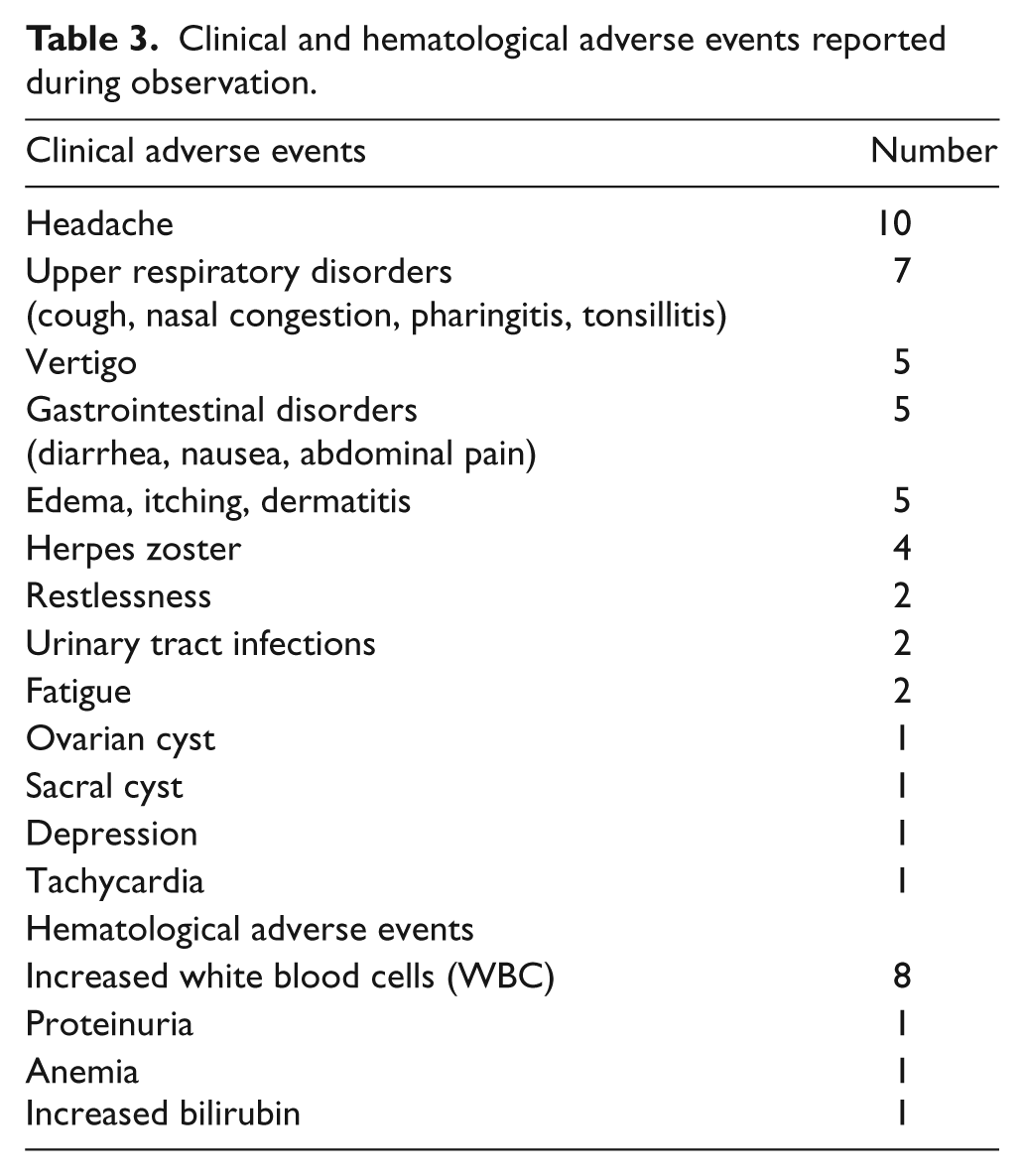
A total of forty-six clinical adverse events were observed in 20/55 patients (Table 3). All of them were transitory (lasting no more than two months) and spontaneously resolved (excluding two patients who presented with sacral and ovarian cysts); no medication was required. Mild hematological abnormalities (below toxicity level 1) were observed in 7/55 cases (Table 3): these resolved spontaneously and no intervention was required. Five patients were treated with NA before 11 years of age: transitory restlessness was recorded in one patient and a transitory increase of white blood cells (WBC) in another one.
Clinical and hematological adverse events reported during observation.
One subject developed a severe progression of neurological symptoms three months after NA withdrawal; rogressive multifocal leukoencephalopathy (PML) was initially suspected, but finally not confirmed from the treating physician. This case is briefly presented in the Appendix.
The presence of NABs was tested in 33 patients, always giving negative results.
Discussion
NA is approved for the treatment of active MS in adults either not responding to first-line treatments or with a rapidly evolving disease. The use of NA in ped-MS with an aggressive evolution has been evaluated in single case reports and in two cohorts of 19 11 and 24 patients, 12 with a mean exposure to NA of 15 and 18 months: in all cases a strong effect in reducing clinical and radiological activity was demonstrated. With respect to our previous study in which 19 patients were included, 11 we here provide additional data on THE safety and clinical efficacy of NA treatment in ped-MS: 36 new cases were included and all cases were followed for a longer time, giving a final cohort of 55 patients with a mean treatment duration of 23 months. Follow-up was longer than 24 months in 30 patients (mean number of infusions: 32.9). To our best knowledge, this is the largest prospective study evaluating the effects of NA in ped-MS over a relatively long period and including serial MRI data. All ped-MS patients were treated with NA because of active disease evolution, with a mean number of relapses in the year prior to NA initiation equal to 2.4. Despite the well-known limitations of an observational study, our presentation shows some interesting results regarding clinical effects and tolerability of NA treatment in ped-MS. Relapses were dramatically reduced following the initiation of NA treatment: only three patients developed relapses in the first six months of treatment, whereas no relapse was observed during the subsequent follow-up; one subject continued to worsen. Treatment with NA also induced an improvement in disability as measured by EDSS score in the vast majority of patients, whereas only three patients worsened over the study observational period. However, the possibility cannot be excluded that in these patients baseline EDSS was affected by the residual effects of the last relapse before NA initiation. The high number of active lesions at baseline MRI may also be explained with the short interval between the occurrence of a relapse and the beginning of NA treatment. Nevertheless, only a few patients had Gd-enhancing lesions and new lesions on T2-weighted sequences during the follow-up: 83% and 74% of patients were free from MRI activity after one and two years of treatment, respectively. This positive effect was confirmed also in 30 subjects treated for more than two years: 19 (63%) patients in this subgroup remained free from any clinical and radiological activity.
Although the administered dose of NA was the same as that used in adult patients, treatment was well tolerated and well accepted by all patients. Adverse events were recorded in 20/55 subjects: they were mild and transitory and no additional medication was required. The occurrence of rare adverse events can only be appreciated by carefully designed and conducted post-marketing surveillance studies: the most serious one associated with natalizumab exposure is represented by the occurrence of PML. Providentially, a test to detect anti-JCV antibodies is now available, allowing a fair and careful evaluation of the risk of developing PML associated to NA exposure, the risk being higher in anti-JCV antibody positive individuals, especially after the second year of treatment and when immunosuppressants therapies have been previously used. 14 –16 The frequency of patients positive for anti-JCV antibodies in our cohort was 39% which is lower than the 57% prevalence observed in an Italian cohort of adult patients. 17 Although this figure is relatively reassuring with regard to the potential risk of PML, the possibility of seroconversion over the time suggests that it might be advisable to re-test patients during the follow-up, possibly every six months. A specific study has been planned by our study group to evaluate the longitudinal seroconversion rate in the pediatric MS population.
Other immunosuppressive drugs have been tested in pediatric patients with active MS and inadequate response to first-line medications. Cyclophosphamide has been shown to reduce disease activity in a retrospective study of 17 ped-MS patients with a mean age of 15 years and a mean disease duration of 3.1 years, but many adverse events were recorded. 18 Mitoxantrone demonstrated a beneficial effect in four ped-MS cases with severe evolution, but has a safety profile which discourages its use. 19 Daclizumab has been proposed as a possible second-line treatment for pediatric cases with active MS evolution in a study of six cases. 20
The results of the present study show that NA can be a useful option for active ped-MS patients, with a satisfactory safety profile, especially since there is the possibility of identifying individuals at a higher risk of PML by using the test to detect serum anti-JCV antibodies.
A blind, controlled trial would be helpful to elucidate the real impact of NA on MS progression in pediatric patients, although its feasibility may be limited due to several reasons: ethical issues related to the presence of a placebo-treated group, unfeasibility of replicating trials already performed in adults (where clear clinical efficacy was demonstrated), and a relatively low number of suitable cases1, 2 The International Pediatric MS Study Group was established some years ago with the objective to promote clinical trials in the MS pediatric population. 2 The implementation of a registry could be an option to collect important information on long-term data about the efficacy and tolerability of new medications in ped-MS. The present study shows that this approach would be feasible in the context of a multicenter study.
Footnotes
Appendix
On October 2009, a 14 year old girl suddenly developed double vision, gait ataxia, vomiting and impaired mentation, preceded by asthenia, fever and loss of sensitivity at left side (EDSS 3.0). Brain MRI revealed evidences of a diffuse leukoencephalopathy with large lesions at the level of brainstem, semioval centers and spinal cord associated to widespread Gd-enhancement. Cerebrospinal fluid analysis showed an increased IgG index. The patient clinically improved after treatment with i.v. methylprednisolone (MP). The initial diagnosis was Acute Disseminated Encephalomyelitis (ADEM).
On January 2010 she presented a severe relapse with behavioral changes, ataxia, diplopia and urinary incontinence (EDSS 3.5). Brain MRI showed several new large lesions with ring enhancement. She was treated with MP and high dose i.v. Ig for five days, followed by three monthly infusions of mitoxantrone (8 mg/sqm) and eight plasma exchanges, with partial recovery. A follow up MRI performed two months later (April 2010) showed new demyelinating areas with ring enhancement, the most evident in the left cerebellar hemisphere. Therefore treatment with high dose MP for 10 days was started, leading to mild clinical improvement. The final diagnosis was of malignant MS. From May 2010 to December 2010 she was treated with monthly NA infusions, with improvement in motor function, but persistent mental deterioration. Due to MRI reactivation (a new temporal lesion) she stopped NA in anticipation of autologous stem cell transplantation.
On February 2011, the girl developed a clinical relapse with impairment in working and short-term memory; NA was re-started (with only one dose infused). On March 2011 brain MRI showed new lesions on T2-weighted sequences (U fibers), some of them being localized in subcortical area and Gd-enhancing, that led to a suspected diagnosis of PML. Cognitive function further deteriorated. The test for the measurement of anti-JC virus antibodies was positive. Lumbar puncture was performed: quantitative PCR (qPCR) for JC virus DNA in cerebrospinal fluid (CSF) gave a positive result with over 140 copies at the NIH laboratory, but it resulted negative at a local laboratory and at National Institute of Health (NIH) when a different aliquot of the same sample was re-tested. One month later, the patient was admitted to a third level hospital: qPCR for JCV DNA in CSF was again negative and brain MRI showed some new lesions on T2-weighted sequences, although but these findings did not lead to a confirmed diagnosis of PML. Proton magnetic resonance (MR) spectroscopy showed an increased Cho/Cr peak and a reduced N-acetylaspartate (NAA) peak, suggesting a demyelinating process. The Electroencephalogram (EEG) showed epileptic discharges. A follow up MRI performed in June 2011 showed several Gd-enhancing lesions, proton MR spectroscopy confirmed the previous pattern. Since then the girl continued to deteriorate, with predominant ataxic disturbances and severe mental deterioration (EDSS 5.5), in spite of the subsequent treatment with corticosteroids, IFNβ-1a 22 µg three times weekly followed four months later by azathioprine as an add-on therapy. The girl presented a generalized tonic-clonic seizure in August 2011. A follow-up lumbar puncture (May 2012) was negative for JCV-DNA. To conclude, clinical and MRI findings did not confirmed the initial suspicion of PML, and were consistent with a severe evolution of the inflammatory demyelinating process with diffuse axonal damage. Consistently PCR for JCV in the CSF was positive in one sample, thereafter always negative, even when retested on a different aliquot of the positive sample.
List of participants
The authors would like to thank the following list of participants:
A Ghezzi, M Zaffaroni, A Bianchi (Gallarate), C Pozzilli, L Prosperini, G Borriello (Rome), M Filippi, L Moiola, S Gerevini, MA Rocca, V Martinelli, G Comi (Milan), V Brescia-Morra, R Lanzillo (Naples), LME Grimaldi, S Bucello (Cefalù), G Lus (Naples), F Rinaldi, P Gallo (Padua), M Trojano (Bari), L Provinciali (Ancona), E Pucci (Macerata, F Bortolon (Vicenza), R Capra (Brescia, G Coniglio (Matera), C Gasperini (Rome), A Lugaresi, E Pietrolongo, D Farina, M di Ioia (Chieti), N Milani (Milan), MR Rottoli (Bergamo), P Sarchielli (Perugia).
Conflict of interest
A Ghezzi has served on scientific advisory boards for Merck Serono, Biogen Idec Teva Pharmaceutical Industries Ltd; has received speaker honoraria from Merck Serono, Biogen Idec, Bayer Schering Pharma, and Novartis, Serono Symposia International; served as a consultant for Novartis; and receives research support from Sanofi-Aventis, Biogen Idec, and Merck Serono.
C Pozzilli has served on scientific advisory boards for and has received speaker honoraria from Novartis, Merck Serono, Biogen Idec, Bayer Schering Pharma, and Sanofi-Aventis.
L Moiola has received support to participate in National and International Congresses from Biogen Idec, Bayer Schering Pharma, Merck Serono, and Sanofi-Aventis.
V Brescia-Morra has received funding for travel, speaker honoraria, and research support from Sanofi-Aventis, Bayer Schering Pharma, Merck Serono, and Biogen Idec.
LME Grimaldi has served on a scientific advisory board for Merck Serono; has received funding for travel or speaker honoraria from Merck Serono, Biogen Idec, Sanofi-Aventis, Bayer Schering Pharma and Solvay Pharmaceuticals, Inc.; has received institutional research support form Teva Pharmaceuticals Industries Ltd, Biogen Idec, Genzyme Corporation, Sanofi-Aventis, Merck Serono, Novartis and Eisai Inc.; has received research support from Merck Serono, Biogen Idec and Ministero della Salute of Italy.
Dr Lugaresi is a Biogen Idec, Merck Serono and Bayer Schering Advisory Board Member. She received travel grants and honoraria from Bayer Schering, Biogen Idec, Merck Serono, Novartis, Sanofi Aventis and Teva and research grants from Bayer Schering, Biogen Dompé, Merck Serono, Novartis, Sanofi Aventis and Teva. Prof Lugaresi has also received travel and research grants from the Associazione Italiana Sclerosi Multipla and is a Consultant of Fondazione Cesare Serono
G Lus has received speaker honoraria from Novartis, Sanofi-Aventis and receives research support from Novartis, Sanofi-Aventis, Bayer Schering, Pharma, Biogen Idec.
MA Rocca has served as consultant to Bayer Schering Pharma; received speakers’ bureaus from Biogen Idec and receives research support from Italian Ministry of Health.
M Trojano has received speaker honoraria from Merck Serono, Sanofi-Aventis, Biogen Idec, Bayer Schering Pharma; has received research support from Merck Serono and Biogen Idec.
M Filippi serves on scientific advisory boards for Teva Pharmaceutical Industries Ltd and Genmab A/S; has received funding for travel from Bayer Schering Pharma, Biogen Idec, Genmab A/S, Merck Serono, and Teva Pharmaceutical Industries Ltd; serves as a consultant to Bayer Schering Pharma, Biogen-Dompè, Genmab A/S, Merck Serono, and Teva Pharmaceutical Industries Ltd; serves on speakers’ bureaus for Bayer Schering Pharma, Biogen Idec, Genmab A/S, Merck Serono, and Teva Pharmaceutical Industries Ltd; and receives research support from Bayer Schering Pharma, Biogen Idec, Genmab A/S, Merck Serono, Teva Pharmaceutical Industries Ltd and Fondazione Italiana Sclerosi Multipla.
G Comi has served on scientific advisory boards for Bayer Schering Pharma, Merck Serono, Teva Pharmaceutical Industries Ltd, Sanofi-Aventis, Novartis, and Biogen Idec; has received speaker honoraria from Teva Pharmaceutical Industries Ltd, Sanofi-Aventis, Serono Symposia International, Foundation, Biogen Idec, Merck Serono, Novartis, and Bayer Schering Pharma.
A Bianchi and F Rinaldi report no disclosures.
Funding
This research did not receive specific grants from any funding agency in the public, commercial, or not-for-profit sectors.