
Abstract
Background:
The StratifyJCV® test is a qualitative assay to classify MS patients as anti-JC virus (JCV) antibody positive or negative. Quantification of anti-JCV antibody levels in serum and cerebrospinal fluid (CSF) of multiple sclerosis (MS) patients might add to the progressive multifocal leukoencephalopathy (PML) risk assessment.
Objective:
The objective of this study is to test sera of patients in a quantitative anti-JCV antibody assay, and to compare the results with preexisting data from the StratifyJCV® test.
Methods:
Sera of a total of 175 MS patients and matched non-MS-controls were tested for anti-JCV antibodies using glutathione S-transferase-tagged-VP1 as antigen. Antibody reactivity was quantified in arbitrary units using human immunoglobulin as standard.
Results:
The comparison of our assay with StratifyJCV® showed good inter-assay agreement (kappa 0.6), and strong correlation for antibody reactivity (r2 = 0.94). Discordant samples had low-reactive positivity, and a higher proportion (13% vs. 4%) tested positive in the StratifyJCV® test only.
Conclusions:
The method presented is a tool for the reliable quantification of anti-JCV antibodies, which demonstrates good agreement with results from StratifyJCV®. In contrast to StratifyJCV®, we pre-adsorbed all of the sera with BK virus (BKV) VP1 protein to reduce cross-reactivity. This step may account for a higher species-specificity of our assay. As such, our assay might be a promising additional tool for PML risk assessment.
Introduction
Progressive multifocal leukoencephalopathy (PML) occurs in a proportion of patients with multiple sclerosis (MS) treated with natalizumab (Tysabri®), a monoclonal antibody that targets the α4-subunit of the α4β1- and the α4β7-integrin.1–3 The human polyomavirus JC (JCV) is the causative agent of PML. 4 Consequently, a two-step enzyme-linked immunosorbent assay (ELISA; StratifyJCV®) has been introduced to stratify patients with MS for a higher or lower risk of developing PML based on a qualitative measure, the anti-JCV antibody status as a surrogate for infection with JCV.5–8 Recent data applying StratifyJCV® suggest that strong or increasing anti-JCV antibody reactivity in the serum might precede the development of PML in patients with MS treated with natalizumab.9,10 Interestingly, the antibody reactivity in larger populations as measured in optical density values (OD) in a screening ELISA resembles a continuum from nonreactive to highly reactive. As such, in the StratifyJCV® test, a second step that determines the percentage of inhibition after pre-incubation with the preparation used as ELISA antigen (soluble virus-like particle (VLP) JCV-VP1 antigen) is applied to samples with indeterminate reactivity. This is thought to reduce false-positive findings due to nonspecific binding. 5 Recently, the StratifyJCV® test has been modified, using a kit system instead of individual assay reagents to improve assay reproducibility, and index values instead of OD values for a more reliable discrimination of low-level antibody reactivity. 11 However, a continuous reactivity for the anti-JCV antibody response around the assay cut-points is still seen, in particular in a proportion of urinary JCV DNA-negative individuals. 11 Hence, not the assay format but rather the biology of the infection with JCV might explain this observation: A high proportion of individuals possibly is exposed to JCV, but differs in activity of the infection with JCV or the individual level of epitope-specific antibody response.
Furthermore, BK virus (BKV) and JCV are closely related, with about 78% amino acid sequence identity in VP1, 12 and cross-reactive epitopes shared by the two viruses have been demonstrated. 13 Previous studies suggest that the major epitopes to which these antibodies are directed are those that define JCV or BKV species specificity.14–17 Nevertheless, these results do not preclude the possibility that strong anti-BKV reactivity leads to low-reactive anti-JCV antibody positivity in a proportion of patients not infected with JCV.
The aim of this study was to develop an assay for the reliable quantification of highly species-specific anti-JCV antibody levels, and to compare the results with preexisting data from the StratifyJCV® test. For this purpose, we optimized a two-step capture ELISA protocol using glutathione S-transferase (GST)-tagged-VP1 as an antigen, and soluble BKV-VP1 fusion protein as a blocker.18–20
Materials and methods
Study population
The study was performed within the German pharmacovigilance study for natalizumab approved by the local ethical committees (Westfaelische Wilhelms-Universitaet Muenster (2010-245-f-S); Heinrich-Heine University Duesseldorf (study n3315)). Informed consent was obtained from all of the patients prior to blood sampling. Patients with MS 21 and age- and gender-matched non-MS controls were studied. The basic demographics were similar for both groups (Table 1). The MS cohort consisted of patients who were previously tested for anti-JCV antibodies using the first-generation StratifyJCV® test (41% (71/175) tested at the Central Biogen Idec laboratory (Boston, MA, USA); 59% (104/175) tested at Unilabs (Kopenhagen, Denmark)) and for whom archived frozen sera were available. The majority of these patients (74% (129/175)) had received 300 mg natalizumab for a median time of 26.5 months (range one to 56 months). None exhibited clinical signs of PML at the time of the blood collection. The control sera (n=162) derived from routine presurgery serology testing excluding patients with known underlying chronic diseases or immunosuppressive therapy.
Basic characteristics.
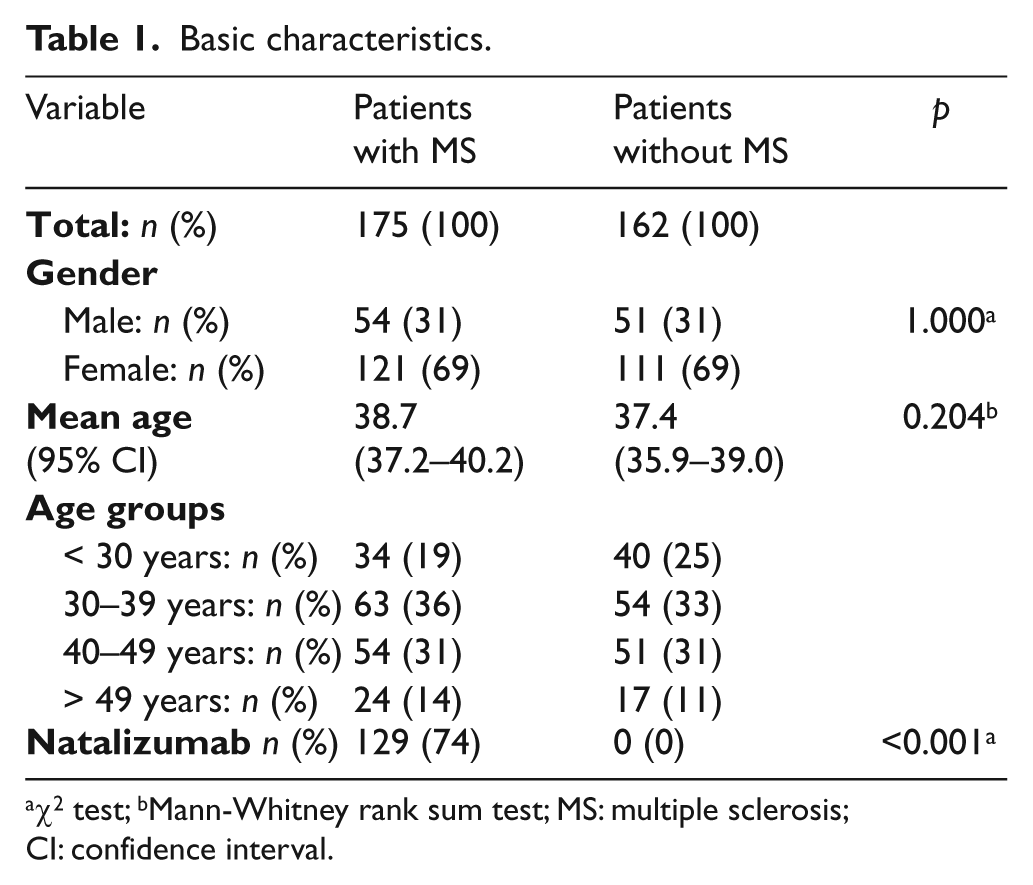
χ2 test; bMann-Whitney rank sum test; MS: multiple sclerosis; CI: confidence interval.
Anti-VP1 GST capture ELISA
The detailed protocol for the modified anti-VP1 GST capture ELISA18–20 for the detection of anti-JCV and anti-BKV antibodies is provided in the supplementary material (Appendix (e)-1). Briefly, affinity-purified JCV-VP1 and BKV-VP1 expressed as GST fusion proteins in E. coli BL21 cells in situ on gluthation casein-coated ELISA plates were used as antigen. Soluble BKV-VP1 and JCV-VP1 bacterially expressed in fusion with N-terminal maltose binding protein were generated for the pre-adsorption of all sera prior to the detection of the anti-JCV and anti-BKV antibodies,
18
respectively. Antigen-loaded ELISA plates were incubated for one hour with pre-adsorbed sera at 1:60 and 1:180 dilutions, and a polyclonal anti-human IgG peroxidase antibody (Sigma-Aldrich, Taufkirchen, Germany) and tetramethylbenzidine (BD Bioscience, Franklin Lakes, NJ, USA) were used for detection. The OD was measured at 450 nm. The antibody reactivity in arbitrary units (AU) and the dynamic range of the ELISA were determined by the serial dilution of human immunoglobulin (Ig, Privigen®, CSL Behring GmbH, Hattersheim, Germany) (Figure e-1). Sera below 15.5 AU for anti-JCV antibodies and 31.2 AU for anti-BKV antibodies were considered to be negative. Sera above 31 AU for anti-JCV antibodies and 62.5 for anti-BKV antibodies were deemed positive. Sera in the indeterminate zone (15.5 AU to 31 AU for JCV; 31.2 to 62.5 AU for BKV) were tested in an additional specificity confirmation assay: Sera with
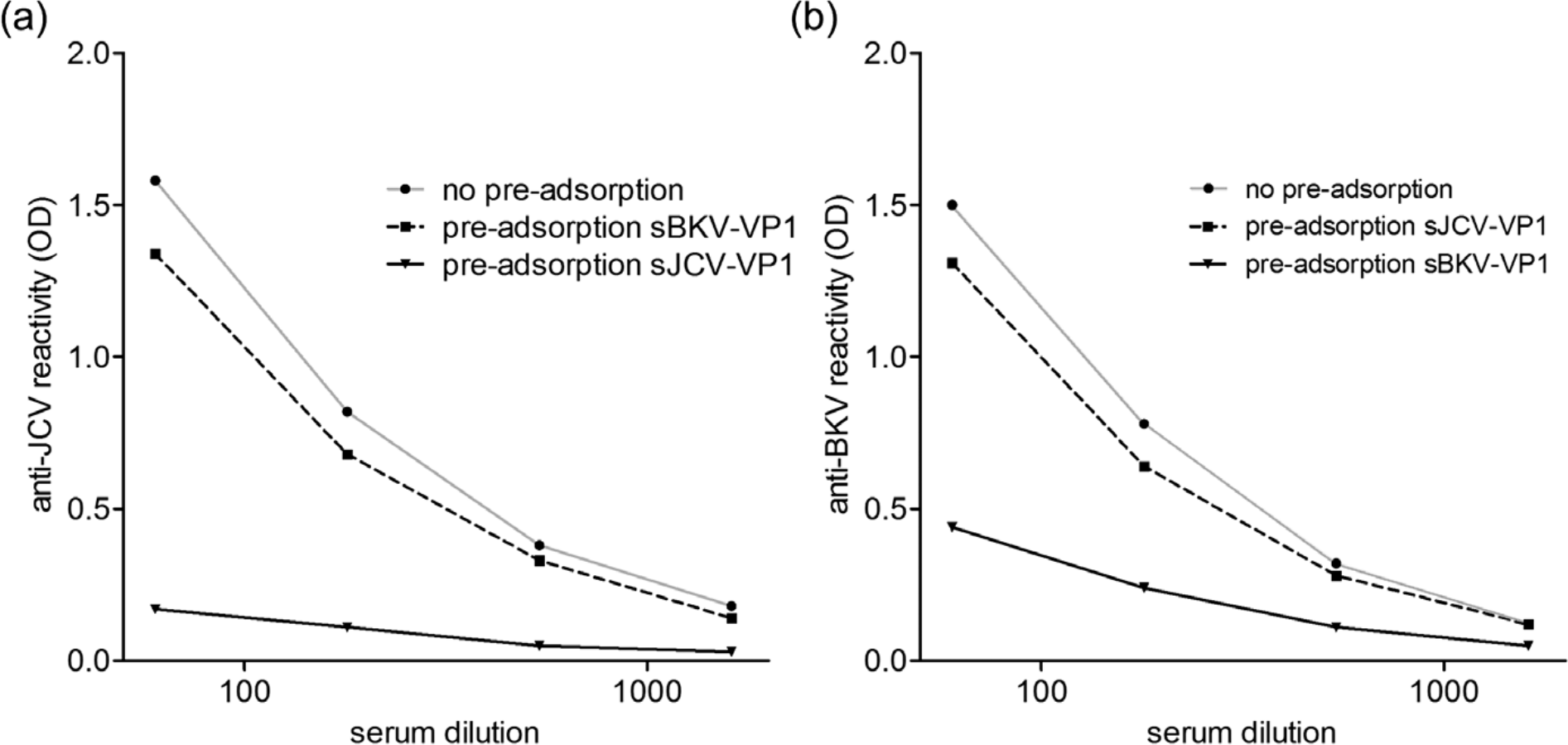
Effect of the pre-adsorption with heterologous and homologous soluble VP1-protein on anti-JCV and anti-BKV antibody reactivity. Serum samples positive for anti-JCV and anti-BKV antibodies were assessed for anti-JCV (a) or anti-BKV antibody reactivity (b) without pre-adsorption, after pre-adsorption with soluble heterologous VP1, or soluble homologous VP1. Results are shown for four different dilutions of the sera (1:3 dilution steps, starting dilution of 1:60). The pre-adsorption with soluble BKV-VP1 reduced the anti-JCV reactivity by 15.0% (1:60) or 23.3% (1:1620) as compared with the reactivity without pre-adsorption. The specificity of the anti-JCV antibody reactivity was confirmed by the reduction of anti-JCV reactivity by > 50% after pre-incubation with soluble JCV-VP1 (87.4% (1:60) or 82.0% (1:1620)) as compared with the reduction by soluble BKV-VP1. The pre-adsorption with soluble JCV-VP1 reduced anti-BKV reactivity by 12.6% (1:60) or 4.1% (1:1620) as compared with the reactivity without the pre-adsorption. The specificity of the anti-BKV antibody reactivity was confirmed by the reduction of anti-BKV reactivity by > 50% after pre-incubation with soluble BKV-VP1 (71.0% (1:60) or 57.0% (1:1620)) as compared with the reduction by soluble JCV-VP1. JCV: JC virus; BKV: BK virus; OD: optical density.
Epstein-Barr virus serology protocol
The antibody detection and reactivity against Epstein- Barr virus (EBV), which were studied as an internal quality control for all the sera tested, were measured by a fully automated commercial chemiluminescence microparticle ELISA (LIAISON® EBV VCA IgG assay, DiaSorin, Saluggia, Italy) as recommended by the manufacturer.
Statistical analysis
The data were analyzed using SigmaPlot 10.0 (Systat Software GmbH, Erkrath, Germany) or GraphPad Prism 5.01 (GraphPad Software, La Jolla, CA, USA). Categorical data were studied using Fisher’s exact test or Pearson’s chi square test, depending on the sample size. The 95% confidence interval (95% CI) for proportions was calculated using the modified Wald method. Quantitative data were analyzed by the non-parametric Mann-Whitney U test for two groups and by the Kruskal-Wallis test for more than two groups. Correlation coefficients (r2) were determined to calculate the quality of the fit of the quantitative results from the different ELISA formats. Cohen’s kappa test was used to assess the agreement of the two protocols in classification of sera as antibody positive or antibody negative. For the quantification of the antibody reactivity in AU, OD values of the samples were compared with a standard curve, using curve fitting of point-to-point calculation (Magellan software, Tecan, Männedorf, Switzerland). Of the two dilutions tested, the concentration resulting in OD values within the linear phase of the calibration curve were used to calculate the reactivity in AU. All of the tests were two sided, and p < 0.05 was considered to be statistically significant.
Results
Anti-JCV antibody detection in the anti-VP1 GST capture ELISA and the StratifyJCV® assay
Applying the anti-VP1 GST capture ELISA, seropositivity for the anti-JCV antibodies in patients with MS compared with the non-MS patients was lower, but the difference did not reach statistical significance in the comparable small cohort studied (53% (95% CI 46–60%) vs. 59% (95% CI 52–67%); p = 0.273). There was no gender difference in seropositivity, neither for all of the patients (male: 57% (95% CI 48–66%) vs. female: 56% (95% CI 49–62%), p = 0.813), nor for the patients with and without MS separately (Table 2). The anti-JCV seropositivity was higher in the patients 50 years and older compared with the patients younger than 30 (all patients < 30 years: 49% (95% CI 38–60%); > 49 years: 73% (58–84%); p = 0.011); Table 2). The anti-JCV antibody reactivity in AU in the seropositive patients was similar in the youngest and oldest groups (Figures 2(a) and 2(b)) and did not differ for patients with and without MS (MS: median AU 121, non-MS: median AU 115; p = 0.324).
Seropositivity for anti-JCV, anti-BKV, and anti-EBV antibodies.
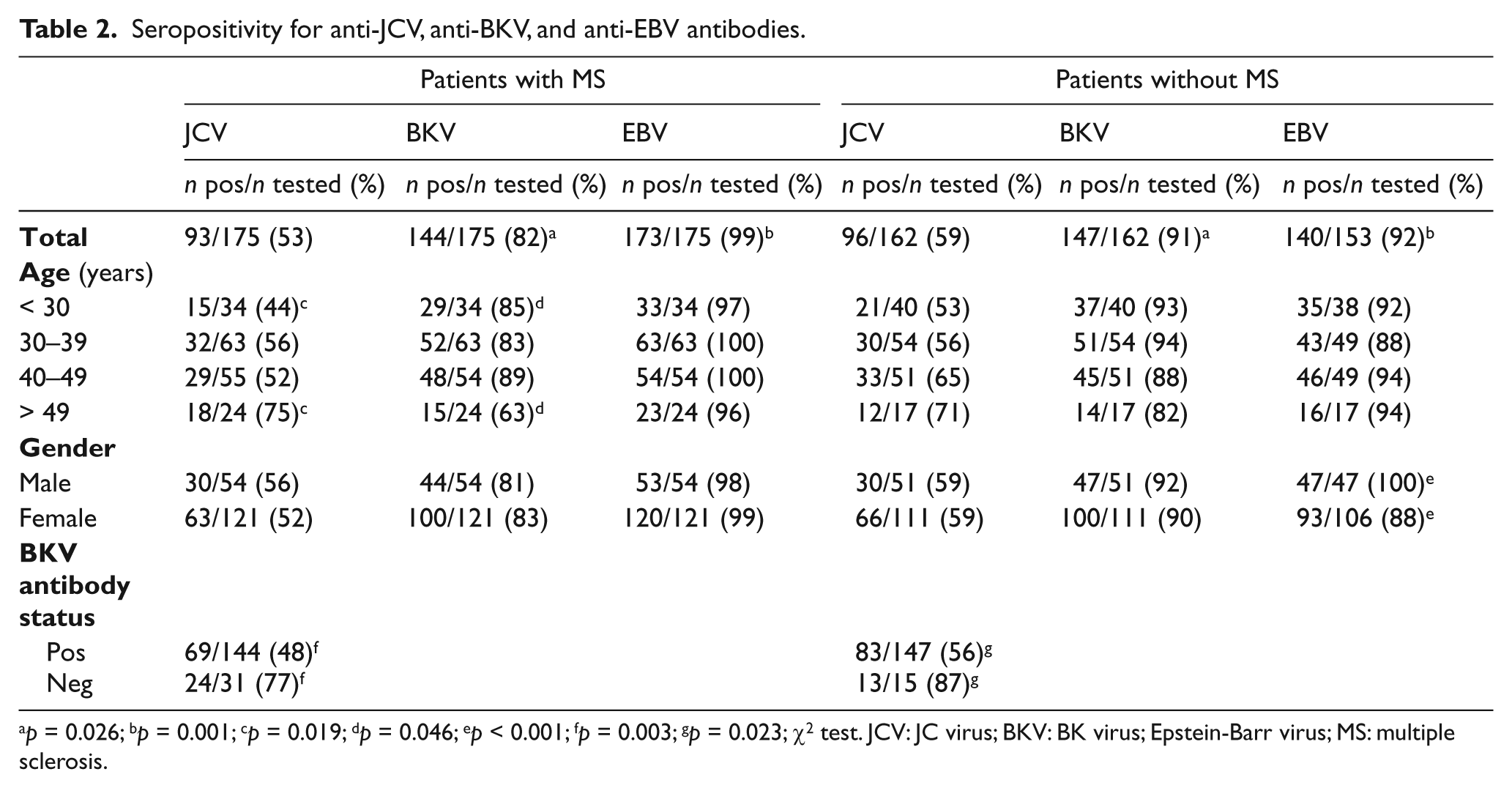
p = 0.026; bp = 0.001; cp = 0.019; dp = 0.046; ep < 0.001; fp = 0.003; gp = 0.023; χ2 test. JCV: JC virus; BKV: BK virus; Epstein-Barr virus; MS: multiple sclerosis.
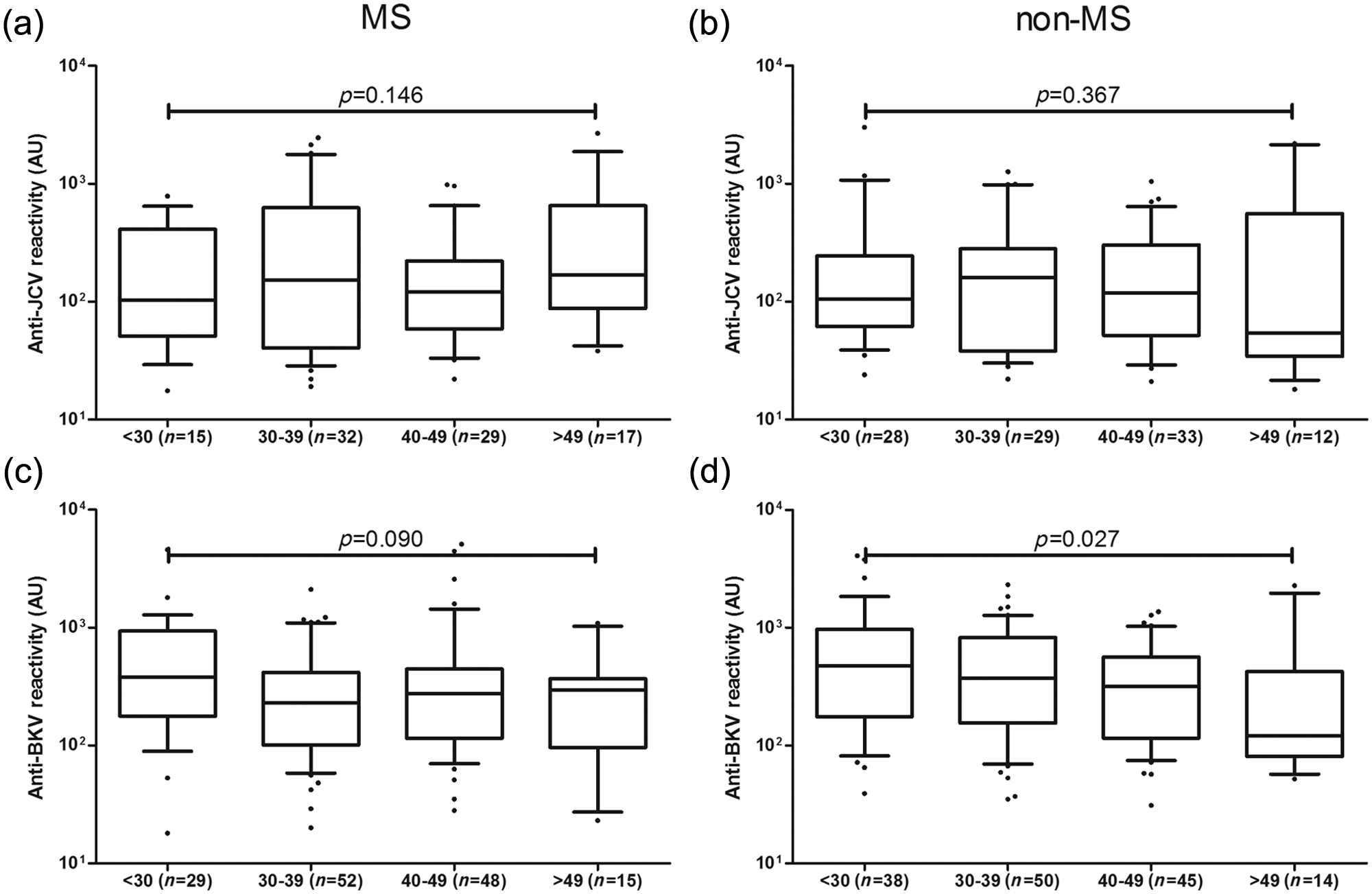
Antibody reactivity for anti-JCV and anti-BKV antibodies across different age groups. Box-whisker plots show antibody reactivity for anti-JCV and anti-BKV antibodies for four different age groups. Boxes span the interquartile range; the vertical line denotes the median, and whiskers indicate the 10th and 90th percentile. Outliers are shown as black circles. Values for anti-JCV antibodies are given in arbitrary units (AU) for patients with MS (a) and non-MS controls (b), and for the anti-BKV antibodies for patients with MS (c) and non-MS controls (d). p value: Mann-Whitney rank sum test comparing the youngest age group (< 30 years) and the oldest group (> 49 years). JCV: JC virus; BKV: BK virus; MS: multiple sclerosis.
There was a trend for a lower positivity for the anti-JCV antibodies when comparing the results from the anti-VP1 GST capture ELISA with those obtained with StratifyJCV® (StratifyJCV®: 62% (95% CI 55–69%); anti-VP1 GST capture ELISA: 53% (95% CI 46–60%); p = 0.104). The proportion of patients with agreement in the anti-JCV antibody status from both tests was 83%, and the kappa value was 0.65 (95% CI 0.54–0.76). Interestingly, a higher proportion of patients tested positive in the StratifyJCV® test only (13% (95% CI 9–19%) vs. 4% (95% CI 2–8%); p = 0.003; Figure 3(a)). A strong correlation was found between antibody reactivity in patients with the positive detection of anti-JCV antibodies in both assays (r2=0.94; p < 0.001; Figure 3(b)). The discordant serum samples for which quantitative data from StratifyJCV® were available (n=12; tested at Central Biogen laboratory, Boston) had a low anti-JCV reactivity: All of these samples demonstrated normalized OD values below 0.3 in the StratifyJCV® test, and all were below the upper cut-off point for positivity in the anti-VP1 GST ELISA (Figure 3(c)). Of all the discordant samples, 90% (27/30) tested positive for anti-BKV antibodies.
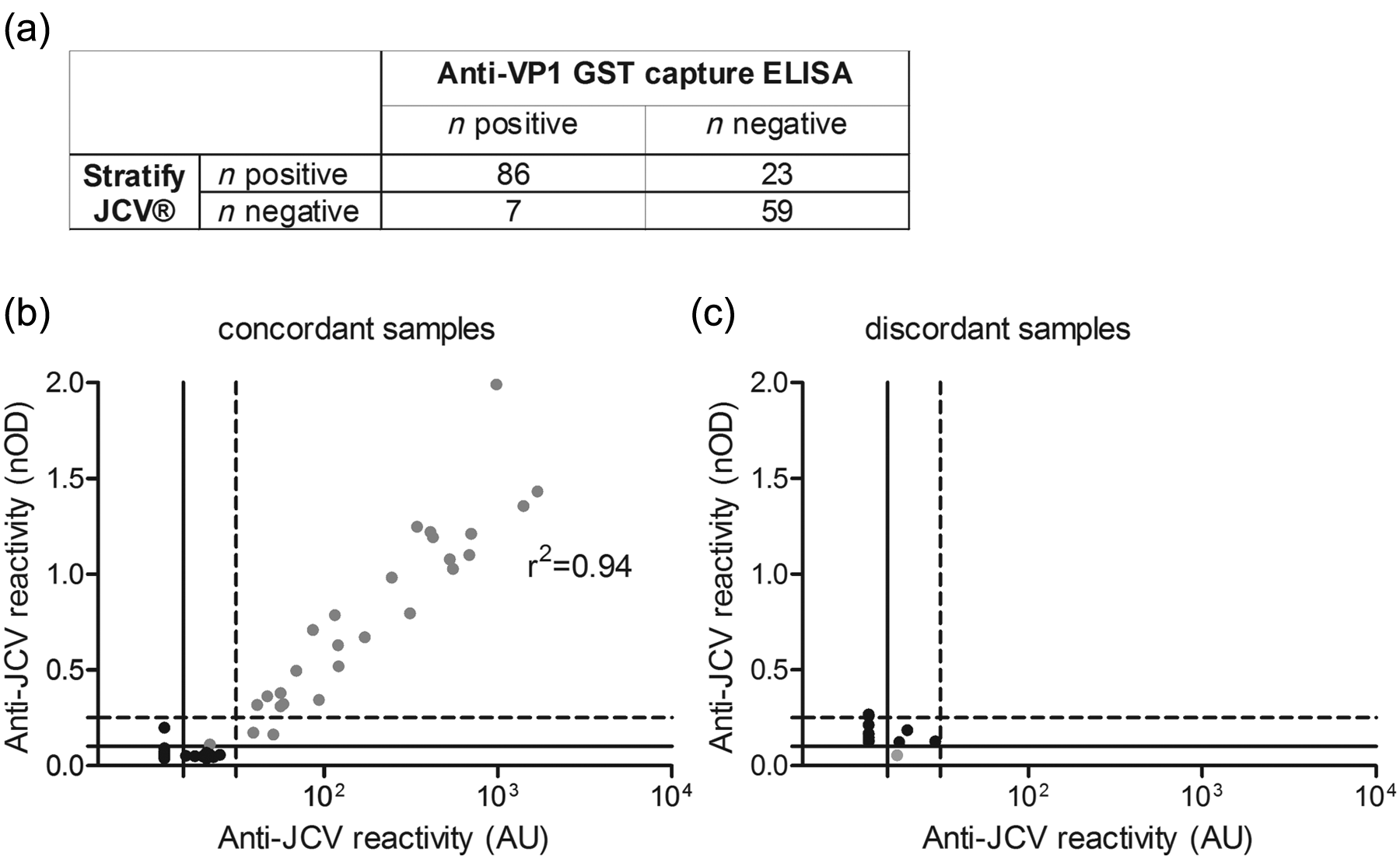
Comparison of results from Stratify JCV® and the anti-JCV GST capture ELISA. The contingency table (a) shows results as obtained with StratifyJCV® and anti-VP1 GST capture ELISA for anti-JCV antibodies in 175 patients with MS. The x-y-plots (b, c) compare anti-JCV antibody reactivity from the anti-VP1-GST ELISA (arbitrary units (AU)) and the Stratify JCV® assay (normalized optical density (nOD)). nOD-values were available only for subjects tested at the Central Biogen Idec laboratory (total 71 patients). In b, the 59/71 samples that agreed in anti-JCV antibody status are shown, and c shows the 12/71 samples that did not agree. Gray circles indicate samples that tested positive; black circles indicate samples that tested negative in the anti-VP1 GST capture ELISA. Dashed lines mark the upper cut-off, back lines the lower cut-off points for positivity. Results for samples below the lower cut-off point in the anti-VP1 GST capture ELISA were not quantified. The Spearman-correlation coefficient (r2) assessed the quality of the fit in antibody-positive patients. JCV: JC virus; GST: glutathione S-transferase; ELISA: enzyme-linked immunosorbent assay; MS: multiple sclerosis.
Anti-BKV antibody detection in the anti-VP1 GST capture ELISA
The seropositivity rate for the anti-BKV antibodies was lower in patients with MS compared with the non-MS controls (82% (95% CI 76–87%) vs. 91% (95% CI 85–94%); p = 0.024). There was no gender difference, neither for all of the patients (male: 87% (95% CI 79–92%) vs. female: 86% (95% CI 81–90%); p = 0.909) nor for the patients with or without MS separately (Table 2). We noted a lower seropositivity in the youngest patient group compared with the oldest patient group, reaching statistical significance for all patients (< 30 years: 89% (95% CI 80–95%); > 49 years: 71% (95% CI 55–82%); p = 0.012), and for the patients with MS (Table 2).
The patients 50 years and older had a lower anti-BKV antibody reactivity compared with patients younger than 30 years (all patients: median AU 167 vs. 461; p = 0.004; Figure 2). The antibody reactivity for seropositive patients with or without MS did not differ (MS: median AU 301; non-MS: median AU 363; p = 0.106).
Comparing anti-JCV and anti-BKV positivity in the anti-VP1 GST capture ELISA
Interestingly, the rate of anti-JCV antibody positivity was significantly higher among the patients who were negative for anti-BKV antibodies, which was observed both for all patients (80% (95% CI 67–90%) vs. 53% (95% CI 48–59%); p = 0.001) and for the patients with or without MS separately (Table 2). The anti-JCV and anti-BKV antibody reactivities in the patients who were positive for both anti-JCV and anti-BKV antibodies did not correlate (r2 =−0.052; p = 0.526).
Anti-EBV antibody detection
As previously reported, 23 the overall seroprevalence for antibodies against EBV was higher in the patients with MS compared with those without MS (99% (95% CI 96–100%) vs. 91% (95% CI 86–95%); p = 0.001; Table 2).
Discussion
We optimized a capture ELISA for the quantification of highly species-specific anti-JCV and anti-BKV antibody levels in MS patients based on GST-fused VP1 proteins.18–20 In contrast to the StratifyJCV® assay, in our protocol all of the sera were pre-adsorbed with soluble heterologous VP1. Similarly to the StratifyJCV® assay, we employed a second-step specificity confirmation test for all of the sera with low-level reactivity in the screening ELISA. In contrast to the StratifyJCV® protocol, in this second step we measured the percentage of reduction in antibody reactivity by soluble JCV-VP1 relative to the reduced reactivity after preincubation with soluble BKV-VP1 fusion protein. These modifications were implemented to minimize the cross-reactivity between shared epitopes of JCV-VP1 and BKV-VP1. With the help of a calibration curve of a diluted immunoglobulin (Ig)-standard, we were able to achieve the robust quantification of the anti-JCV or anti-BKV reactivity in AU (Figure e-1), with high intra- and inter-assay reproducibilities (Figure (e)-3).
When we applied this method to samples of patients with and without MS, the anti-JCV and anti-BKV antibody status and reactivity were in agreement with the published literature,5,6,16,24–26 supporting the validity of this method. Interestingly, the anti-BKV positivity was lower in the MS compared with the non-MS patients (82% vs. 91% for anti-BKV antibodies; Table 2), while for anti-JCV antibodies a similar trend did not reach statistical significance (53% vs. 59%). While a lower anti-JCV antibody positivity has been previously reported for a Swedish cohort, 27 the lower anti-BKV positivity in the patients with MS is a novel finding. Both observations are, thus far, unexplained. Based on recently presented preliminary results, genetic polymorphisms, i.e. in the human leukocyte antigen region, could be hypothesized to be relevant to MS susceptibility, and to infections with JCV and BKV. 28
Interestingly, although anti-JCV seropositivity increases with age, anti-JCV antibody reactivity remains stable.5,6,16,24–26,29 In contrast, infection with BKV is acquired early in life with high seropositivity at a young age.15,16,24–26,30 Anti-BKV antibody positivity and reactivity then mildly decline with increasing age (Figure 2). Hence, both viruses might differ in the mechanisms involved in the maintenance of the immunological memory response. A decline in the anti-BKV antibody reactivity with increasing age — due to a lower frequency of reactivation or re-exposure compared with that of JCV — is most likely linked to the decreasing positivity with age. These patients might still be infected with BKV but appear seronegative because of an anti-BKV antibody reactivity below the cut-off of the respective immunoassay used.
We observed higher anti-JCV seropositivity in BKV-seronegative individuals compared with BKV-seropositives (Table 2). The high virus species-specificity of our assay most likely contributes to this finding. The pre-adsorption of all of the sera with soluble heterologous fusion protein enables the study of responses specific for JCV or BKV and excludes the cross-reactive antibody responses against shared epitopes (Figure 1). Although previous studies suggested that the major epitopes to which antibodies are directed are those that define JCV or BKV species specificity,14–17 cross-reactive antibodies might still lead to, for example, low-reactive positivity for anti-JCV antibodies in individuals with strong anti-BKV antibody responses. Interestingly, Egli and colleagues previously noted that JCV DNA shedding in the urine was more common in patients with undetectable anti-BKV antibodies who were positive for anti-JCV antibodies only; 16 hence, cross-reactive antibodies or a poly-specific booster of the anti-JCV antibody response, e.g. by subclinical BKV reactivation, could possibly provide protection from subclinical and/or clinical JCV reactivation.
When comparing the results for the anti-JCV antibodies from the StratifyJCV® and the anti-VP1 GST capture ELISA, we noted a good agreement for the anti-JCV antibody status (kappa=0.65), and a strong correlation for antibody reactivity in positive individuals (r2=0.94, Figure 3). As such, our data generally confirm the data for anti-JCV antibodies as obtained with the StratifyJCV® test. Considering the extensive validation process for StratifyJCV® including an increasing set of prospectively collected data in pre-PML samples,5,6,8,17 we do not aim to replace the StratifyJCV® test for the purpose of PML risk stratification based on anti-JCV antibody status. In fact, our data support the validity of the approach by obtaining similar results applying a different technique. However, a slightly lower positivity was observed with the anti-VP1 GST capture ELISA (53% vs. 62%). A higher proportion of patients tested positive in the StratifyJCV® test only (13% vs. 4%), which indicates an effect of different cut-off definitions or a systematic difference in specificity. The patient samples with discordant anti-JCV antibody status exhibited low anti-JCV antibody reactivity. As 90% of the discordant samples were positive for anti-BKV antibodies, cross- reactivity with BKV might contribute to these findings. Nevertheless, due to the lack of serum standards to determine the true exposure to JCV or BKV, we cannot rule out a lower sensitivity of the anti-VP1 GST capture ELISA. In particular, the definition of the lower and higher cut-off points for positivity in two-step protocols, such as the anti-VP1 GST capture ELISA and the StratifyJCV® assay, differ. For the anti-VP1 GST capture ELISA, we determined the cut-off for positivity by analyzing the dynamic range of a human Ig-standard dilution and confirmed the results with the help of an alternative established protocol (Figure (e)-2). In contrast, StratifyJCV® used a group of patients with JCV viruria as a positive control and statistically determined the cut-off points. 5 Regardless of the method used, a proportion of patients with low-reactive positivity complicates the definition of the cut-off points. Considering the detection of higher levels of anti-JCV antibodies in pre-PML patients, 9 the significance of low-reactive antibody positivity with regard to the risk of developing PML remains unknown. As such, we hypothesize that — in addition to the infection status with JCV (yes/no) — the activity of the infection with JCV might determine the individual risk of PML. In such a concept, the negative StratifyJCV® status would still be a highly valuable tool to define a subgroup of patients with a very low risk of developing PML. However, the anti-JCV antibody-positive patients might not all share the same risk, and the assessment of the individual levels of the anti-JCV antibody reactivity as surrogate for the activity of the infection with JCV might allow further stratification, e.g. in groups with low, intermediate, or high risk. These concepts require additional validation, and an assay that reliably detects highly species-specific anti-JCV antibody reactivity.
Therefore, in future projects we aim to apply the assay presented here to larger cohorts to measure anti-JCV and anti-BKV reactivity in serum of non-PML and pre-PML samples, 10 and serum and cerebrospinal fluid (CSF) pairs in order to determine the anti-JCV antibody index in CSF. The latter is of particular interest for patients with low-level or negative detection of JCV-DNA in CSF, frequently observed in cases of natalizumab-associated PML. The overall goal would be to provide additional tools for the further stratification of the risk of developing PML in anti-JCV-positive patients, and for the earlier diagnosis of PML in a proportion of patients.
Footnotes
Conflicts of interest
CW is funded by a European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS) fellowship stipend. MP has received travel expenses for attending meetings from Johnson and Johnson. TD has received travel expenses for attending meetings from Novartis Pharma GmbH and Bayer HealthCare AG. HPH has received personal compensation for activities with Biogen Idec, Teva, Sanofi-Aventis, Novartis Pharma, Merck Serono and Bayer Schering. HW has received funding for travel and speaker honoraria from Bayer Schering Pharma, Biogen Idec/Elan Corporation, Sanofi-Aventis, Merck Serono and Teva Industries Ltd. HW has served/serves as a consultant for Merck Serono, Medac Inc, Sanofi-Aventis/Teva Pharmaceutical Industries Ltd., Biogen Idec, Bayer Schering Pharma, Novartis and Novo Nordisk; and receives research support from Bayer Schering Pharma, Biogen Idec/Elan Corporation, Sanofi-Aventis, Merck Serono and Novo Nordisk. BCK has received personal compensation for activities with Bayer Schering, Biogen Idec, Genzyme, Merck Serono, Novartis, Roche, Sanofi-Aventis Pharmaceuticals, Talecris and Teva Neuroscience. BCK has received research support from Bayer Schering, Biogen Idec, Merck Serono and Teva Neuroscience. OA has nothing to declare.
Funding
This work was supported by a local faculty grant (Forschung skommission Heinrich-Heine University Duesseldorf) to OA and a grant from the German Ministry for Education and Research (BMBF, “German Competence Network Multiple Sclerosis” (KKNMS), Natalizumab-Pharmakovigilanzstudie, 01GI1002) to BCK and HW. CW is supported by an ECTRIMS fellowship stipend. The testing of the sera using StratifyJCV® was provided free of charge by Biogen Idec per current agreement for its clinical use in patients with MS.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.