
Abstract
Background:
Treatment with natalizumab, a humanized monoclonal antibody against alpha4beta1 integrin, is associated with an increase in lymphoid progenitor cells and B cells in peripheral blood.
Objective:
The objective of this study was to examine the impact of natalizumab therapy on serum levels of total IgG, IgA and IgM in patients with multiple sclerosis (MS).
Methods:
In two independent cross-sectional patient cohorts, serum levels of IgG, IgA and IgM were compared between patients treated with natalizumab and those not receiving natalizumab. Further, serum levels of IgG, IgA and IgM before and during natalizumab treatment were compared in two longitudinal patient cohorts.
Results:
In patients treated with natalizumab, serum IgM and IgG levels were significantly lower compared with therapy naïve patients (p<0.0001). IgM levels significantly decreased after initiation of natalizumab treatment in both longitudinal patient cohorts (p<0.01). Moreover, patients treated with natalizumab showed a time-dependent decrease in IgM levels during the first 2 years of treatment.
Conclusion:
Natalizumab treatment leads to a significant decrease in serum IgM and IgG levels in patients with MS. IgM levels decrease with treatment duration during the first 2 years of treatment. These findings might support the hypothesis that natalizumab interferes with homing of B cells, possibly leading to impaired differentiation into plasma cells and subsequently disturbed immunoglobulin synthesis.
Keywords
Introduction
Very late antigen-4 (VLA-4, alpha4beta1 integrin) is an adhesion molecule expressed on all leukocytes except neutrophils. By interacting with the vascular cell adhesion molecule-1 (VCAM-1) it is involved in both rolling and firm adhesion of leukocytes on endothelial cells enabling leukocytes to transmigrate through the blood brain barrier. 1 –3 Injection of antibodies against VLA-4 prevents the development of experimental autoimmune encephalomyelitis (EAE) 4 and natalizumab, a humanized antibody against VLA-4, significantly reduces disease activity in relapsing–remitting multiple sclerosis (MS). 5 However, long term treatment with natalizumab is associated with a significant risk of the development of progressive multifocal leukencephalopathy (PML).
Besides its role in the interaction between leukocytes and endothelium VLA-4 has been studied for its ability to mediate retention of hematopoietic precursor cells in bone marrow since treatment with natalizumab induces an increase in CD34+ cells in peripheral blood. 6,7 VLA-4 also plays an essential role for the entry and retention of B cells in spleen and lymph nodes and homing of plasma cells in the bone marrow niche. 8 –10 In mice the blockade of VLA-4 and lymphocyte function associated-1 integrin (LFA-1) leads to a rapid release of B cells from the lymphoid tissue into the peripheral blood. 11 In patient s with MS treatment with natalizumab results in a significant increase of B cells in peripheral blood. 12, 13 Whether the alteration of B cell compartmentalization by natalizumab has an impact on long term immunoglobulin production has not been addressed so far. Changes in serum immunoglobulin levels during natalizumab treatment could play a role in the pathogenesis of PML as the risk of developing this disease during natalizumab therapy increases with treatment duration.
Patients and methods
Patients
Sera were obtained from patients at the Departments of Neurology of the Technische Universität München and Philipps-University of Marburg. A total of four patient groups were analysed. Two independent cohorts were used for cross-sectional studies and two for longitudinal analyses.
The cross-sectional discovery cohort consisted of nine patients with MS who were treated with natalizumab (natalizumab+, median age 42, range 26–52 years, five male and four female) and 19 patients with MS who were not treated with natalizumab (natalizumab−, median age 32 years, range 20–53 years, nine male and 10 female). Ten of these received no MS-specific medication or were on the first day of steroid treatment; eight had received intravenous or oral steroids for at least 1 day and one received interferon beta-1a. The median treatment duration of patients treated with natalizumab who were part of the discovery cohort was 70.6 weeks (range 2.1 (15 days) – 212.6 weeks (1488 days)). Treatment of these patients before natalizumab was as follows: all patients had received interferon beta; one patient was receiving glatiramer acetate; one patient was receiving azathioprine that was discontinued 72.9 weeks before sampling; one patient was receiving mitoxantrone and this was discontinued 89.1 weeks before sampling and one patient was receiving both azathioprine and mitoxantrone (azathioprine was discontinued at least 15 years before sampling and mitoxantrone was discontinued 335.3 weeks before sampling). In cases in which due to a long patient history only data on the month of initiation of natalizumab treatment or discontinuation of prior treatment was available, the 15th of the respective month was used for calculations.
The cross-sectional validation cohort consisted of 34 patients treated with natalizumab (natalizumab+, median age 31.5 years, range 21–56 years, 20 female, 14 male) and 98 therapy naïve patients with clinically isolated syndrome (CIS) or MS (median age 36 years, range 19–55, 61 female, 37 male). Samples were taken at a median of 33.1 weeks (range 4.1 (29 days) – 159.6 weeks (1117 days)) after initiation of natalizumab treatment. Of the 34 patients treated with natalizumab one received fingolimod before initiation of natalizumab therapy but had already been receiving natalizumab treatment for 21 weeks at the time of sampling. One patient received a reduced dosage of natalizumab (180 mg every 4 weeks) at the time of sampling.
Sera samples were available from 14 of the 34 patients in the cross-sectional validation series before initiation of natalizumab treatment (median 4.8 weeks before first natalizumab infusion, range 1.1 (8 days) – 40.1 (281 days) weeks) (first longitudinal series). Treatment at this time point included steroids (n=3), interferon beta (n=5), interferon beta and steroids (n=1), glatiramer acetate (n=3) or no MS-specific therapy (n=2). Four of the 14 patients had previously been treated with natalizumab (the last infusion was given at a median of 34 (range 11.1–60.1) weeks before sampling). Sera obtained at different time points before and/or during natalizumab treatment were available from 18 patients.
The second longitudinal patient cohort comprised 18 patients. Sera samples were available before as well as during natalizumab treatment for all these patients. The preceding immunomodulatory therapy (interferon beta, n=11; glatiramer acetate, n=7) was discontinued at a minimum of 1 week before the first blood sample; patients were not treated with steroids within the last 4 weeks. Samples during natalizumab treatment were taken 12–28 weeks (median 13 weeks) after treatment was initiated.
Informed consent was obtained from all patients. The study protocol was approved by the local ethics committees of the Technische Universität München and the Philipps-University of Marburg.
Methods and statistical analysis
IgG, IgA, IgM and albumin were determined by nephelometry using a Siemens BNProSpec in the cohorts from Munich and Behring Nephelometer Analyzer II (BNII) in the cohorts from Marburg (Siemens, Munich, Germany; patient cohort of Marburg), respectively. Samples of the second longitudinal cohort were measured at the Philipps-University of Marburg and all other samples were measured at the Technische Universität München. Samples of the validation series and the first longitudinal series were measured together; samples of the discovery cohort were measured separately. We did not pool the results of the longitudinal cohorts because the IgG and IgM levels measured differed between the two laboratories. In the discovery cross-sectional patient series IgG subclasses 1–4 were quantified in the serum using the human IgG Subclass Profile ELISA kit (InvitrogenTM Carlsbad, CA, USA). Serum samples were diluted 1:2500 and measured as duplicates. Concentrations of IgG subclasses were calculated from a standard curve.
Where patient serum was available during the first, second and/or third year of natalizumab treatment (n=18) absolute and relative changes in serum IgM levels were calculated from year to year. In cases where sera were obtained at two or more different time points within a year the mean values were used for calculation.
The levels of immunoglobulin classes were not normally distributed according to the D’Agostino and Pearson omnibus normality test in any of the four patient series. Therefore serum IgG, IgA, IgM and albumin levels between natalizumab treated and untreated patients as well as between patients receiving immunomodulatory treatment and therapy naïve patients were compared using the Mann Whitney U test. For the same reason, for serial comparison of serum levels before and during natalizumab treatment, Wilcoxon matched pairs test was used. Statistical analysis was performed using Prism 6 for Mac OS X (GraphPad Software, San Diego, CA, USA).
Results
In both independent cross-sectional cohorts the total serum IgG and IgM levels were significantly lower in natalizumab treated patients (n discovery cohort=9, n validation cohort=34) compared to 19 patients not treated with natalizumab (treatment included steroids, interferon beta, no therapy; Figure 1(a), p=0.0016 for IgG, p=0.0001 for IgM) or 98 therapy naïve patients, respectively (Figure 1(b), p<0.0001 for both IgG and IgM). Median serum IgG levels in natalizumab treated patients were 36.07% lower in the discovery cohort (median natalizumab+ 7.80 g/l, median natalizumab− 12.20 g/l) and 18.82% lower in the validation series (median natalizumab+ 8.41 g/l, median treatment naïve patients 10.36 g/l). The difference in IgG isotype levels between natalizumab+ and natalizumab− patients in the discovery cohort was most prominent for the IgG1 isotype (p=0.0078 for IgG1, Figure 2) while the difference in IgG2, IgG3 and IgG4 levels did not reach significance.
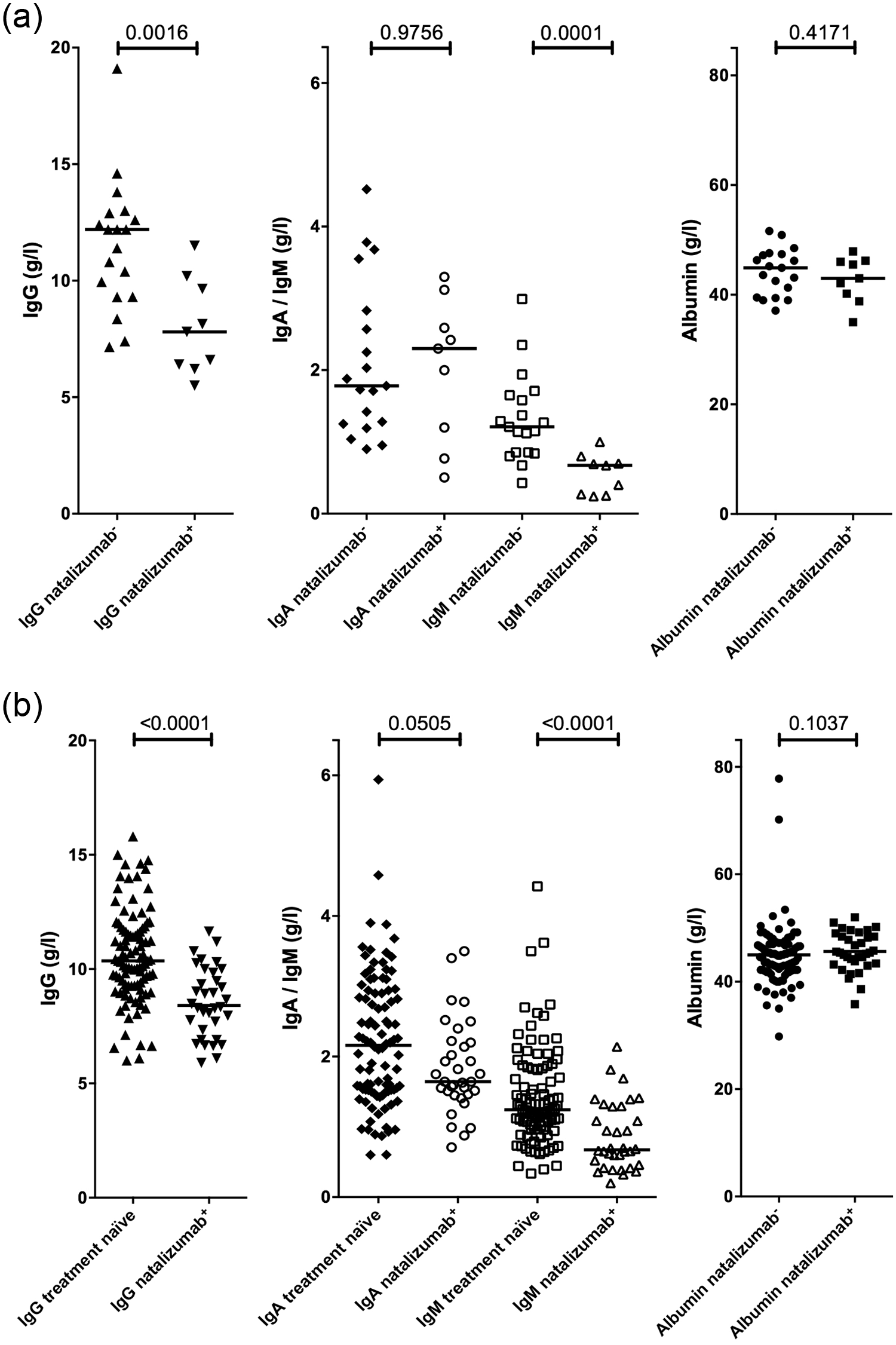
Serum IgG, IgA and IgM levels in two cross-sectional patient cohorts of natalizumab treated and untreated patients.
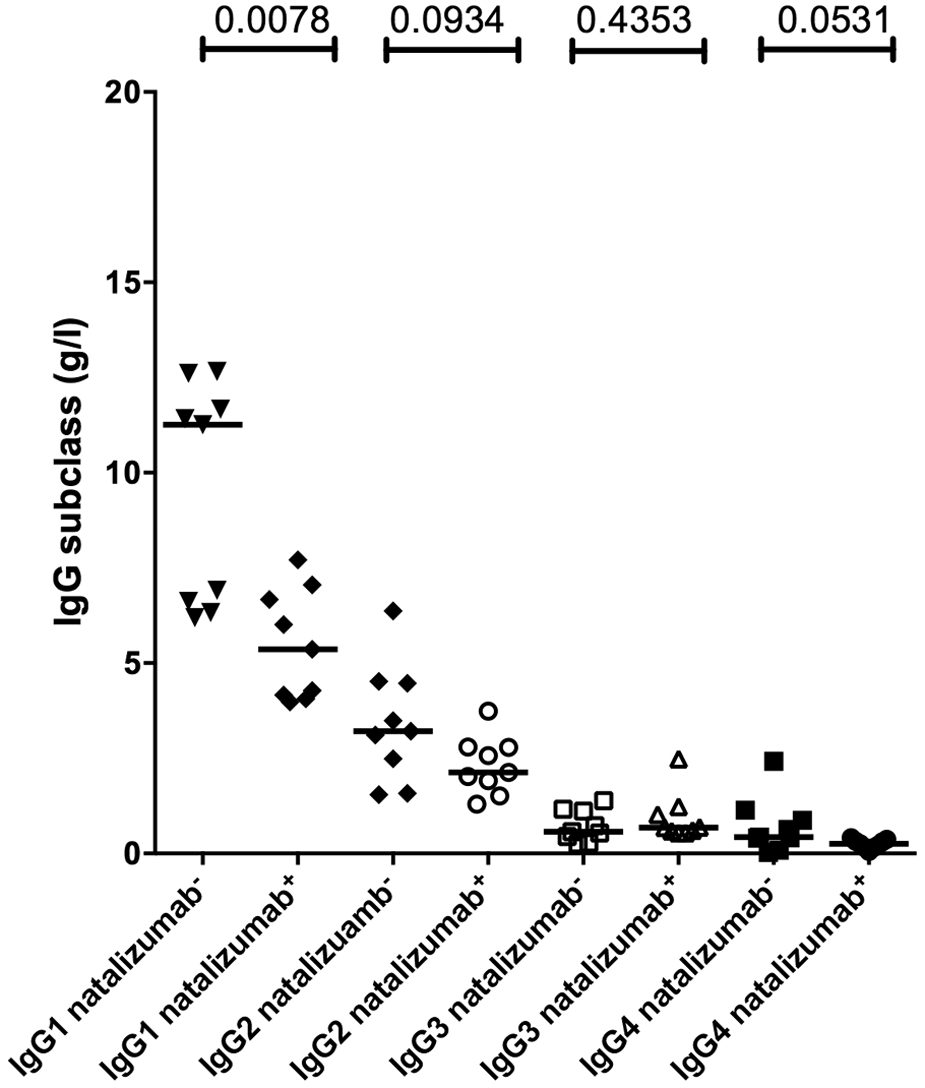
IgG subclass analysis of the discovery cohort.
Median serum IgM levels were 44.46% lower in the discovery cohort (median natalizumab+ 0.672 g/l, median natalizumab− 1.210 g/l, Figure 1(a)) and 45.98% lower in the validation series (median natalizumab+ 0.672 g/l, median treatment naïve patients 1.244 g/l, Figure 1(b)). No significant difference was found for IgA and albumin levels in both sets of patients (Figure 1).
In the two independent longitudinal patient cohorts (n first longitudinal series=14, n second longitudinal series=18) IgM levels significantly decreased after initiation of natalizumab therapy with the median of the relative reduction being by 33.94% in the first series (median before therapy 1.062 g/l, median on therapy 0.672 g/l, p=0.0033) and by 33.13% in the second series (median before therapy 1.635 g/l, on therapy 1.085 g/l, p=0.0007, Figure 3(c) and (f)).
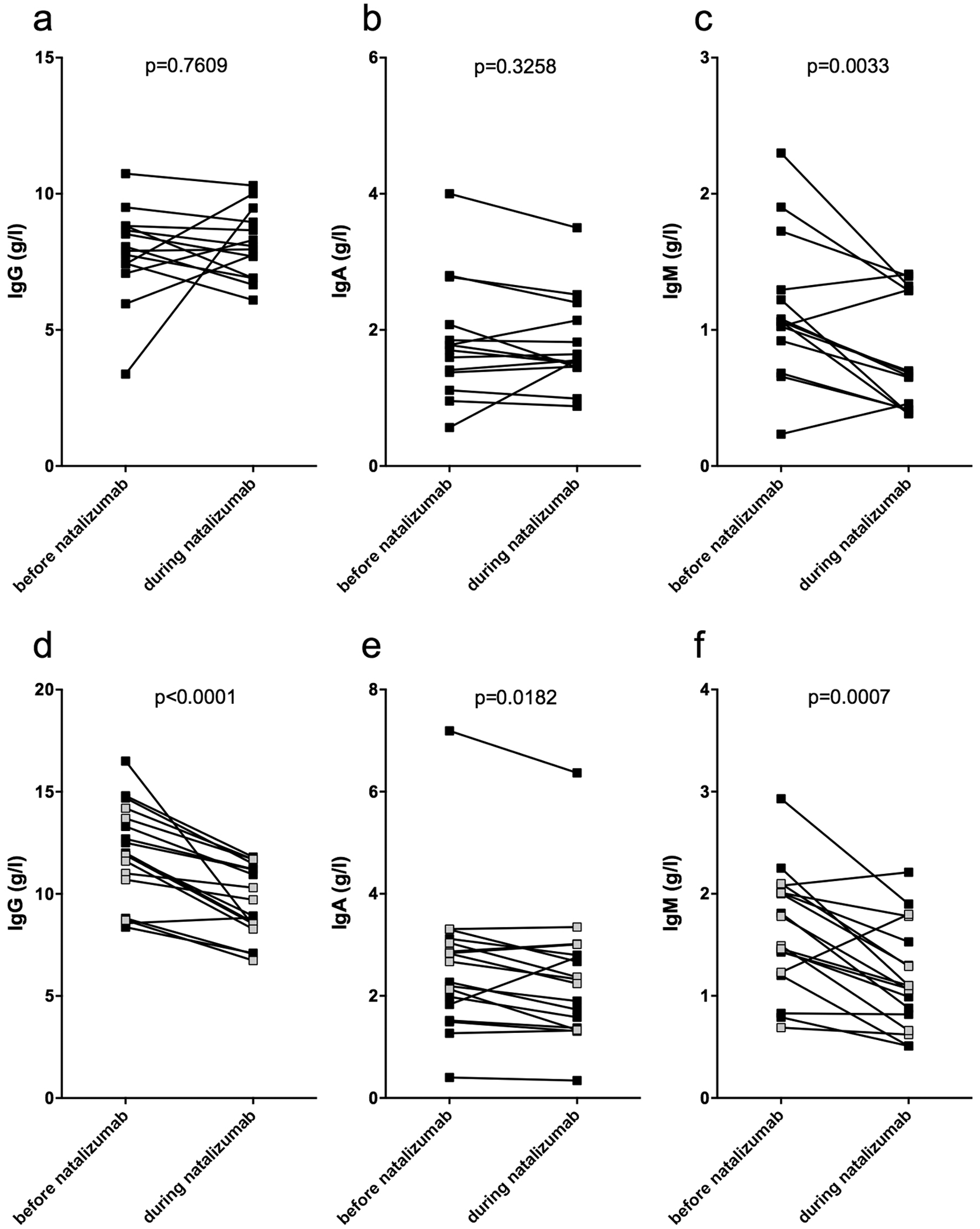
Serum IgG, IgA and IgM levels before and during natalizumab treatment.
Where patients had received steroids or immunomodulatory therapies at the time of the first sample taking (first series) their IgG and IgA levels did not decrease significantly after initiation of natalizumab therapy (Figure 3(a) and (b)). However, in untreated patients (second series) IgG and to a lesser extent IgA levels decreased (p<0.0001 for IgG, median decrease in IgG level by 18.78%; p=0.0182 for IgA, median decrease in IgA level by 12.4%, Figure 3(d) and (e)). We did not observe a significant difference in baseline IgG, IgA or IgM between patients in the second longitudinal cohort having received interferon beta and those having received glatiramer acetate before (p=0.493 for IgG, p=0.1258 for IgA, p=0.7415 for IgM).
In order to assess any impact of MS medications other than natalizumab on IgG levels these were measured in 12 patients of the first longitudinal cohort receiving steroid, interferon beta or glatiramer acetate at baseline and were compared with treatment naïve patients of the cross-sectional validation series showing a significant difference in baseline IgG but not in IgM levels between the two patient series (p<0.0001 for IgG, p=0.0716 for IgM). The IgG levels of patients receiving steroids were below the median value of the treated patients group (supplementary Figure 1) suggesting that predominantly steroid treatment might influence serum IgG but not IgM levels.
In patients where serial serum samples before and/or during natalizumab treatment were available (n=18) a decrease in IgM levels but not in IgG or IgA levels was observed over time during the first 2 years of natalizumab treatment (Figure 4). In patients where serum was available before initiation of natalizumab treatment and during the first year of treatment (n=11, day 1–365 after first dose of natalizumab) the median of the relative reduction of serum IgM levels was 31.77% during the first year compared with the level before treatment initiation (median of decrease in IgM levels 0.268 g/l, p=0.0322). In patients with sera available during the first and second year (n=13, day 366–730 after first dose) after initiation of natalizumab treatment IgM levels showed a non-significant decrease with the median of the relative reduction in IgM levels being 11.35% (median of decrease in IgM levels 0.053 g/l, p>0.05). IgM levels remained relatively stable with a non-significant increase between the second and third year (n=6, day 730–1095 after first dose, median of increase in IgM levels 0.023 g/l, p>0.05).
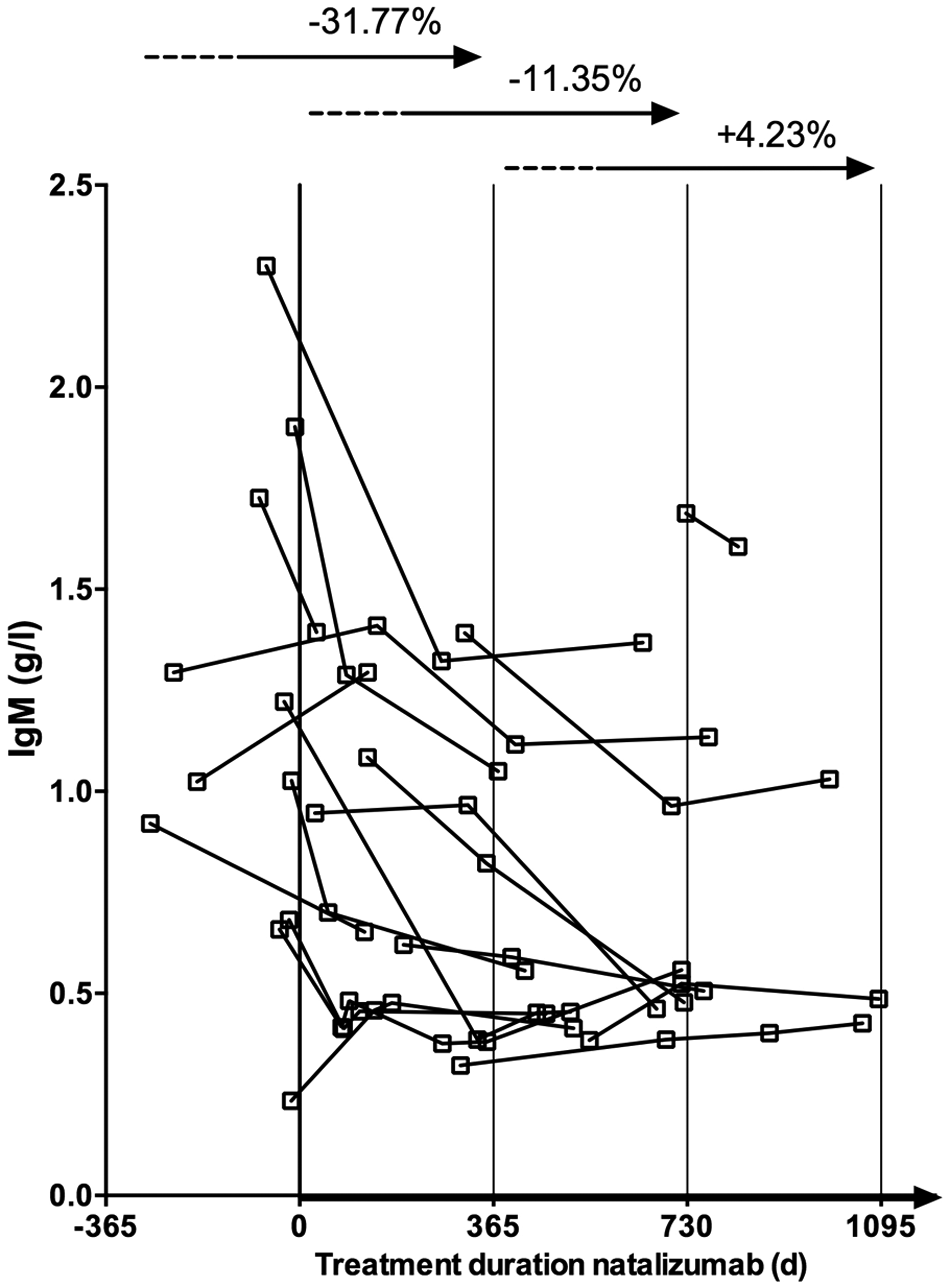
Serial analysis of serum IgM levels during natalizumab treatment.
Discussion
In this study we demonstrate that natalizumab treatment leads to a significant decrease in serum IgM and IgG levels in patients with MS. IgM levels show a time-dependent decrease during the first 2 years of natalizumab therapy.
In healthy individuals reactivated memory B cells home to secondary lymphoid tissues like spleen, peripheral lymph nodes and the mucosa associated lymphoid tissue (MALT), namely the Peyers patches of the gut. It has been shown that memory B cells express higher levels of VLA-4 compared with other mature B cells. 14 VLA-4 serves as a ligand for VCAM-1 on peripheral lymph node high endothelial venules. 15 Moreover, VLA-4 in cooperation with LFA-1 and their ligands are involved in B cell migration into the splenic white pulp. 8 In contrast, homing of naïve and memory lymphocytes to mesenteric lymph nodes and Peyers patches high endothelial venules is mainly mediated by interaction of VLA-4 with MadCAM. 1,8,15,16
Several studies have shown that individuals treated with natalizumab show a significant and sustained increase in circulating CD34+ cells in peripheral blood compared with healthy controls and untreated patients with MS 6,7 and most of the CD34+ cells were shown to be also CD38 positive identifying them as lymphoid committed progenitor cells. 6,13 During natalizumab treatment B cells also increase almost twofold in peripheral blood although it is not entirely clear which B cell subset is most strongly affected. Krumbholz and colleagues reported that in particular pre-B cells are most prominently elevated. 12 Another study found that predominantly memory- and marginal zone (MZ)-like but not naive B cells are elevated in natalizumab treated patients. 13 These findings are in line with experimental animal studies on the role of VLA-4 in B cell hemostasis.
Although we cannot provide experimental evidence why natalizumab decreases IgM and IgG serum levels it is tempting to hypothesize that the blockade of VLA-4 by natalizumab affects the formation of B cell follicles in the lymph nodesand spleen and eventually reduces plasmablast and plasma cell generation. 17,18 In addition, natalizumab might impair the VLA-4 dependent homing of plasma cells into their niches reducing the number of resident IgG and IgM producing plasma cells in the bone marrow. The fact that IgA secreting cells originate independent of VLA-4 in the MALT 19 might explain why IgA levels are only slightly affected by natalizumab treatment.
A recent study demonstrated a decrease in intrathecal IgM and to a lesser extent also IgG synthesis as well as in B cell numbers in the cerebrospinal fluid (CSF) of patients with MS showing a favorable treatment response towards natalizumab. 20 Although presumably different mechanisms play a role in B cell differentiation within the central nervous system as compared with the periphery, inhibition of B cell homing to ectopic meningeal follicles resembling peripheral lymphoid organs might contribute to this observation. 21
The IgG levels of patients receiving steroids or immunomodulatory treatment at baseline were significantly lower compared with therapy naïve patients whereas IgM levels at baseline did not differ significantly between these groups. IgG levels in patients receiving steroids were below the median of the treated patients group. This finding is in line with studies showing a decrease in serum IgG but no alteration in IgM levels during corticosteroid treatment. 22 –24 Therefore, we can neither exclude that corticosteroid treatment before initiation of natalizumab therapy might also have influence on long term IgG levels nor that the observed decrease in IgG levels during natalizumab treatment is an unspecific effect which can also be observed during steroid or immunomodulatory therapy. However, in the second longitudinal cohort where patients did not receive corticosteroids within 4 weeks before sample taking IgG levels decreased significantly after initiation of natalizumab treatment. This argues against long term effects of corticosteroid treatment on serum IgG levels. IgM levels were not significantly influenced by corticosteroid treatment and moreover showed a further time-dependent decrease within the first 2 years of natalizumab therapy.
In summary we demonstrate in two independent cross-sectional and two longitudinal sets of patients that natalizumab selectively decreases IgM and IgG levels but does not affect IgA levels to a comparable extent. The long term consequences of reduced IgM and IgG levels remain uncertain. In single patients IgG and IgM levels reach concentrations that are considered low levels and associated with increased rates of infection in patients with additional immune deficiency. 25 Besides the effects of natalizumab on the immune surveillance and the mobilization of bone marrow stem cells the reduction on IgG and IgM levels might also contribute to the risk of developing PML. 26
Footnotes
Conflict of interest
This work was supported by a grant from the German Ministry for Education and Research (BMBF, “German Competence Network Multiple Sclerosis” (KKNMS), Control-MS, 01GI0917).
Bernhard Hemmer has received invitational financial support for research activities from Bayer Health Care Pharmaceuticals, Biogen Idec, Merck Serono, Novartis, Metanomics, Protagen, and Roche and fees and honoraria for consulting from Bayer Healthcare, Biogen Idec, Genzyme, Merck Serono, Novartis, Teva Pharmaceuticals and Sanofi-Aventis.
Wolfgang H Oertel holds stocks of Roche, is a advisory board member and/or has received speaker and/or consultant honoraria from Desitin, Proteosys, Novartis, Orion Pharma, Solvay Pharmaceuticals, Synosia, Bayer-Schering, Bioprojet, Boehringer Ingelheim, Eisai (until 2007), Meda Pharmaceuticals International, Merck-Serono, Neurosearch, Schering Plough, Schwarz Pharma Neuroscience (UCB), Teva, and GlaxoSmithKline, and has received scientific grants from the German Ministry of Education and Research.
Björn Tackenberg is an advisory board member and/or has received speaker and/or consultant honoraria from Bayer Vital, Germany; Biogen Idec, Germany and USA; Merck Serono, Germany; Novartis, Germany; Sanofi Aventis, Germany; and Teva Pharma, Germany.
Achim Berthele received speaker and consulting honoraria as well as travel reimbursements from Bayer Healthcare, Biogen Idec, Merck Serono, Novartis, and Teva.
Dorothea Buck has received compensation for activities with Bayer-Schering, MerckSerono and BiogenIdec.
Rebecca C Selter, Viola Biberacher, Verena Grummel and Christian Eienbröker have nothing to disclose.
Funding
This study was funded by the German Ministry for Education and Research (BMBF, “German Competence Network Multiple Sclerosis” (KKNMS), Control-MS, 01GI0917).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.