
Abstract
Background:
Retinal nerve fiber layer (RNFL) loss occurs with multiple sclerosis and after optic neuritis. Vision or RNFL changes at presentation of optic neuritis are not predictive of outcome, but vision loss at 1 month correlates with vision deficits at 6 months. We hypothesized that RFNL thinning at 1 month would predict RNFL loss at 6 months.
Methods:
We prospectively studied the RNFL by optical coherence tomography (OCT) and scanning laser polarimetry (SLP), and determined the threshold field mean deviation, in 25 subjects with acute optic neuritis over a 6-month period. RNFL values, including the amount of thinning at 1-month, were correlated with 6-month outcome.
Results:
Baseline visual performance and RNFL values were similar for eyes grouped by 1 month RNFL thinning. Eyes with 1 month RNFL thinning had greater and significant RNFL thinning at 6 months, for all quadrants by OCT and for the nasal and inferior quadrants by SLP. RNFL thinning by OCT and SLP at 1 month correlated with 6-month OCT (r = 0.58; p = 0.006) and SLP (r = 0.59; p = 0.002) RNFL thinning, respectively.
Conclusion:
Early RNFL loss at 1 month was predictive of the RNFL thinning at 6 months, which corroborated the importance of the 1-month time point for predicting the outcome of an optic neuritis attack.
Keywords
Introduction
Analysis of the peripapillary retinal nerve fiber layer (RNFL) by optical coherence tomography (OCT) reveals that there is thinning or reduction of the average RNFL thickness after optic neuritis. RNFL loss is more prevalent in eyes with persistent visual deficits.1,2 In addition, RNFL loss occurs in patients with chronic multiple sclerosis (MS), particularly those with more neurological disability.3,4 These results are not unexpected, as Frisén and Hoyt 5 demonstrated “slit-like defects” in the peripapillary nerve fiber layer, using red-free photography in MS patients with or without prior optic neuritis, which suggested the “insidious attrition of axons.” This is further supported by reports of axonal transections in acute MS lesions. 6 We previously reported RNFL thickening or swelling at baseline and the occurrence of RNFL thinning at 1 month in a prospective observational study. 7 Furthermore, we demonstrated the utility of interocular comparison as a more sensitive criteria for detecting RNFL loss (Kupersmith M, et al. Invest Ophthalmol Vis Sci 2008; 49: E-Abstract 5389).
Although OCT is the most commonly used modality for assessing the RNFL, scanning laser polarimetry (SLP) and confocal retinal tomography (HRT) are also used to quantify the RNFL thickness and show pathologic thinning of the RNFL in glaucoma and in MS patients.9–11 In general, RNFL values are greater using OCT than SLP, but the results from both methods are comparable,12,13 particularly if enhanced corneal compensation (ECC) SLP is used.14,15 The ECC SLP improves the reliability of RNFL measurement, reducing corneal contribution to atypical retardation patterns and improving the signal to noise ratio. In a recent study, OCT and SLP (using a less sensitive corneal compensation method) showed similar losses of RNFL, in patients with MS without recent optic neuritis. 10 Here we report the value of the 1-month RNFL in predicting 6-month determinations of vision and RNFL thinning, using both time domain OCT and ECC SLP. Given the previous report noting the importance of the visual performance at 1 month in predicting vision outcome, 16 we explored whether RNFL thinning at 1 month was predictive of the structural and functional 6-month outcomes after an episode of optic neuritis.
Methods
We prospectively evaluated patients who had vision loss from acute unilateral demyelinating optic neuritis for the first time in the affected eye, with vision loss for less than 15 days. Patients were studied at presentation of acute optic neuritis (mean of 6 ± 3 days after vision loss began) and at 1, 3 and 6 months afterwards. We excluded patients with other optic nerve disorders or ophthalmic disorders that could reduce vision. Subjects could be included if they had known MS or prior optic neuritis in the fellow eye, providing the fellow eye had normal vision (≥ 20/20; ≥ 95% color plates seen; mean deviation (MD) ≥ −3.00 db) and it had average RNFL data that fell within the control 5th to 95th percentile range for OCT and SLP.
This study was conducted with New York Eye and Ear Infirmary Institutional Review Board (IRB) approval. At baseline, all subjects had monocular best corrected visual acuity (expressed in LogMAR notation; with finger counting vision to no light perception assigned a score ranging from 2–4), and threshold perimetry performed using the Humphrey Field Analyzer SITA 24–2 standard threshold strategy with stimulus size III (expressed as MD from age-matched normal subjects, in decibels (db)). Subjects with severe vision loss unable to respond to the brightest stimulus lights during threshold perimetry had their visual field scored as a MD of −35 db. Unless the patient had known MS or had a recent magnetic resonance imaging (MRI) assessment, the diagnosis of acute optic neuritis or MS was verified with a fat-suppressed gadolinium enhanced MRI and short tau inversion recovery views of the pregeniculate visual pathway and brain, during the acute stage of optic neuritis. 17
For SLP (GDx with research software for enhanced corneal compensation, Zeiss-Meditec, Dublin, CA),13,14 imaging was performed through an undilated pupil. Patients with severe visual loss who could not fixate on the internal target were asked to slowly shift their gaze until the operator could position the image of the optic nerve and macula in the center of the image. Prior to the software analysis of the RNFL thickness from the SLP image, an elliptical annulus was positioned on the image and centered on the optic disc, to permit analysis of the same peripapillary RNFL region between exams. Retardation values were determined within the annulus, with sampling of 64 circumferential wedges of peripapillary RNFL thickness. Only the SLP images that were centered on the disc, were well focused, and had quality scores ≥ 7 were analyzed. OCT (Stratus version 3, OCT 4 Software, fast RNFL protocol, Zeiss-Meditec, Dublin, CA) was used to obtain a set of three retinal scans of 3.4 mm diameter, averaged to provide the RNFL thickness at 256 points along the circumference of the circular peripapillary scan in each eye, after pupillary dilation. Only centered OCT data with signal strength scores ≥ 7 were analyzed. At baseline, we performed macula OCTs: no patient had macular edema. By using these imaging inclusion criteria, not all eyes had complete data for every point in time, for both imaging modalities. We included data for subjects with quality data: complete data for baseline, 1 and 6 months, with a normal RNFL at baseline in the patients’ unaffected fellow eyes.
We analyzed the SLP and OCT RNFL thickness, divided in four quadrants: temporal, superior, nasal and inferior. For OCT, each quadrant measurement was determined from the average of the corresponding three clock hour sectors. For SLP, the 64 RNFL data points were organized in groups of 16 points that were averaged for each quadrant measurement. We also evaluated the average RNFL thickness around the entire circumference for OCT and an ellipse for SLP. Average and quadrant RNFL thicknesses were compared with fellow eyes and with a population of normal control eyes. We demonstrated the reproducibility and stability of the average RNFL determinations, for four time points over 6 months, by time-domain OCT (5%) and the SLP (4%) on the unaffected fellow eyes, in optic neuritis.
We compared RNFL values of the affected and fellow eyes, because it has been shown that the inter-ocular difference of RNFL is quite low in normal eyes.18–20 This approach has limitations, due to the fact that it is possible that a fellow asymptomatic eye may not be completely normal in patients with acute optic neuritis or MS, and may have undergone some degree of thinning of the RNFL in the past, even without a clear history of optic neuritis. None of the fellow eye RNFL data showed thinning (Criterion 1: less than the 5th percentile RNFL thickness of control eyes for average or each quadrant RNFL values) at baseline or at 6 months.
We determined the absolute RNFL thickness measurements and the amount of calculated thinning (derived by subtracting corresponding fellow eye thickness from the affected eye) for the 1- and 6-month data. We previously showed that the inter-ocular RFNL difference of at least 10 μm (Criterion 2) can be considered a significant inter-eye asymmetry in subjects with optic neuritis. 7 This construct also concurs with data from normal eyes that suggest an inter-ocular RFNL thickness difference of less than 9μm could be a variation of normal. 20
We measured whether RNFL thinning, by Criterion 1 or 2, at 1 month was associated with worse 6-month RNFL values, RNFL thinning, visual acuity and visual field mean deviation. Pearson correlation analysis was used to determine whether the 1-month RNFL values correlated with 6-month RNFL and visual field outcomes.
Results
Of the original cohort of 40 patients described by us in a previous report of early changes in the RNFL, 7 a total of 24 patients met the inclusion criteria for the present study and had adequate optical imaging at presentation, and at 1 and 6 months. In this study, there were 5 men and 19 women with a mean age of 31.2 ± 7.3 years. Of these, 22 subjects received 3 or 4 days of intravenous therapy of 1 gr/day methylprednisolone. Five subjects had known MS, for a mean duration of 1.2 years; four were being treated with interferon or glutarimer acetate. None of the patients with MS had long-standing or secondary progressive disease, nor MRI evidence of cerebral atrophy.
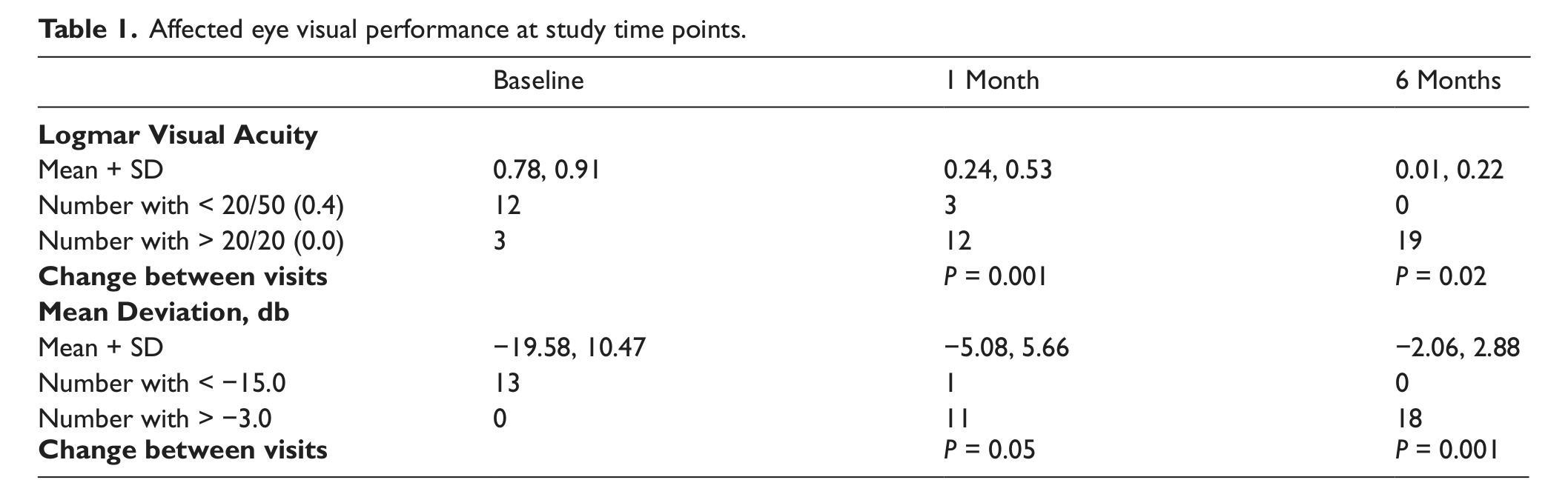
At presentation, the patients’ mean for visual acuity and mean deviation were typical of optic neuritis, with most affected eyes having moderate to severe vision loss (Table 1). No affected eyes showed thinning of the RNFL in any quadrant, by OCT or SLP. The mean RNFL values were thicker than for the fellow eyes (Figure 1). 7 The baseline SLP and OCT-measured average and individual quadrant RNFL values were similar, for eyes that were categorized at 1 month to the thinned or not thinned groups (for both criteria).
Affected eye visual performance at study time points.
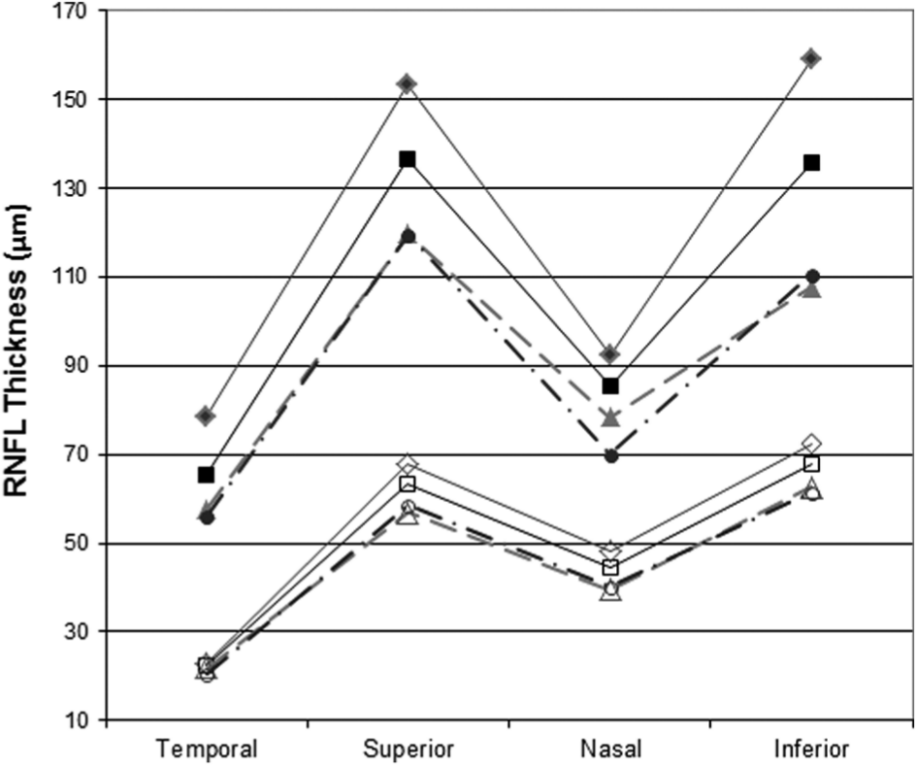
Mean RNFL values for OCT (closed symbols) and SLP (open symbols) show thinning over time (predominantly at 1 and 3 months) that is not selective for one quadrant. Baseline (diamonds), 1-month (squares), 3-month (triangles), and 6-month (circles) data are shown.
At 1 month, as expected, the patients’ vision improved in all eyes (Table 1) and the mean for RNFL thickness values across all quadrants were less thick than at presentation (Figure 1). RNFL values were below the 5th percentile in 7/20 eyes for OCT and in 6/24 eyes for SLP by Criterion 1. By Criterion 2, the RNFL was thinned based on interocular comparison in 10/20 eyes by OCT and in 11/24 eyes by SLP.
At 6 months, the mean for visual acuity and mean deviation were significantly improved, compared to at presentation and at 1 month (Table 1). Five patients had abnormal vision; only one of them had a moderate/severe deficit. By Criterion 1, at 6 months, the RNFL was thinned in 10/20 eyes (50%) by OCT and in 13/24 eyes (54%) by SLP. By Criterion 2, at 6 months, the RNFL was thinned in 14/20 eyes (70%) by OCT and in 18/24 eyes (75%) by SLP. The RNFL values for both SLP and OCT were thinner than the previous visit, for all quadrants (Figure 1).The amount of RNFL thinning at 1 month (by Criterion 1, but not Criterion 2) correlated with the amount of loss at 6 months for both OCT (r = 0.58; p = 0.006) and SLP (r = 0.59; p = 0.002) (Figure 2). The eyes with RNFL thinning at 1 month by OCT and SLP showed greater thinning across all quadrants at 6 months (Table 2). The amount of average RNFL thinning by OCT, but not SLP, at 1 month showed a trend to correlate with the MD (r = 0.40; p = 0.08) at 6 months. The average RNFL for SLP and OCT, and the number of quadrants with thinning by Criterion 2 at 1 month for OCT and SLP did not correlate with the 6-month visual acuity or visual field MD.
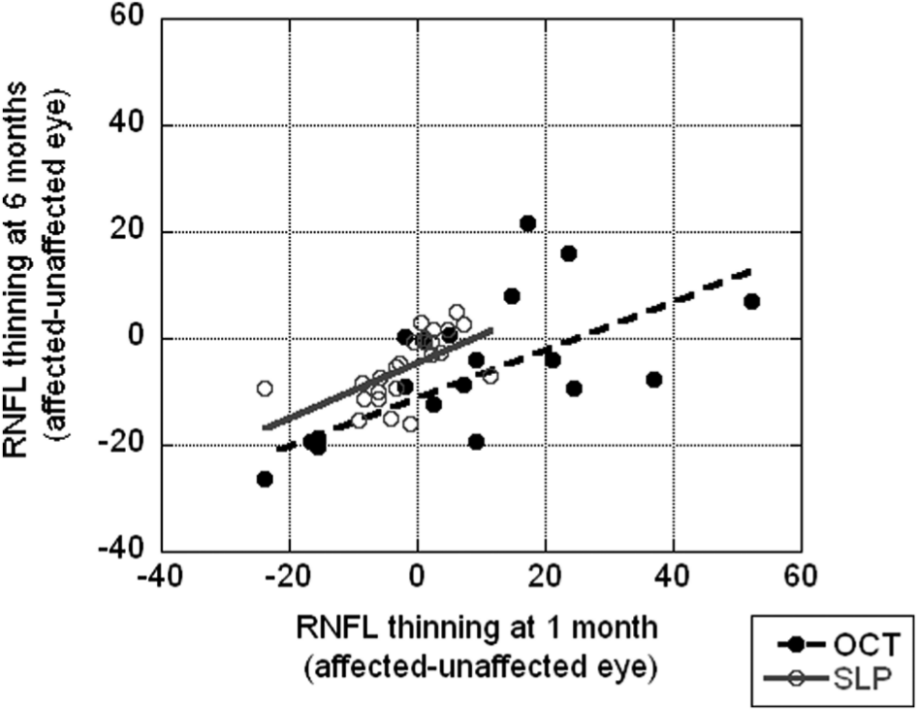
By criterion 1, the 1-month SLP and OCT measured thinning of the RNFL correlates with the 6-month SLP and OCT thinning of RNFL.
RNFL thinning (expressed as a minus value) at 6 months, based on whether the RNFL was thinned at 1 month.
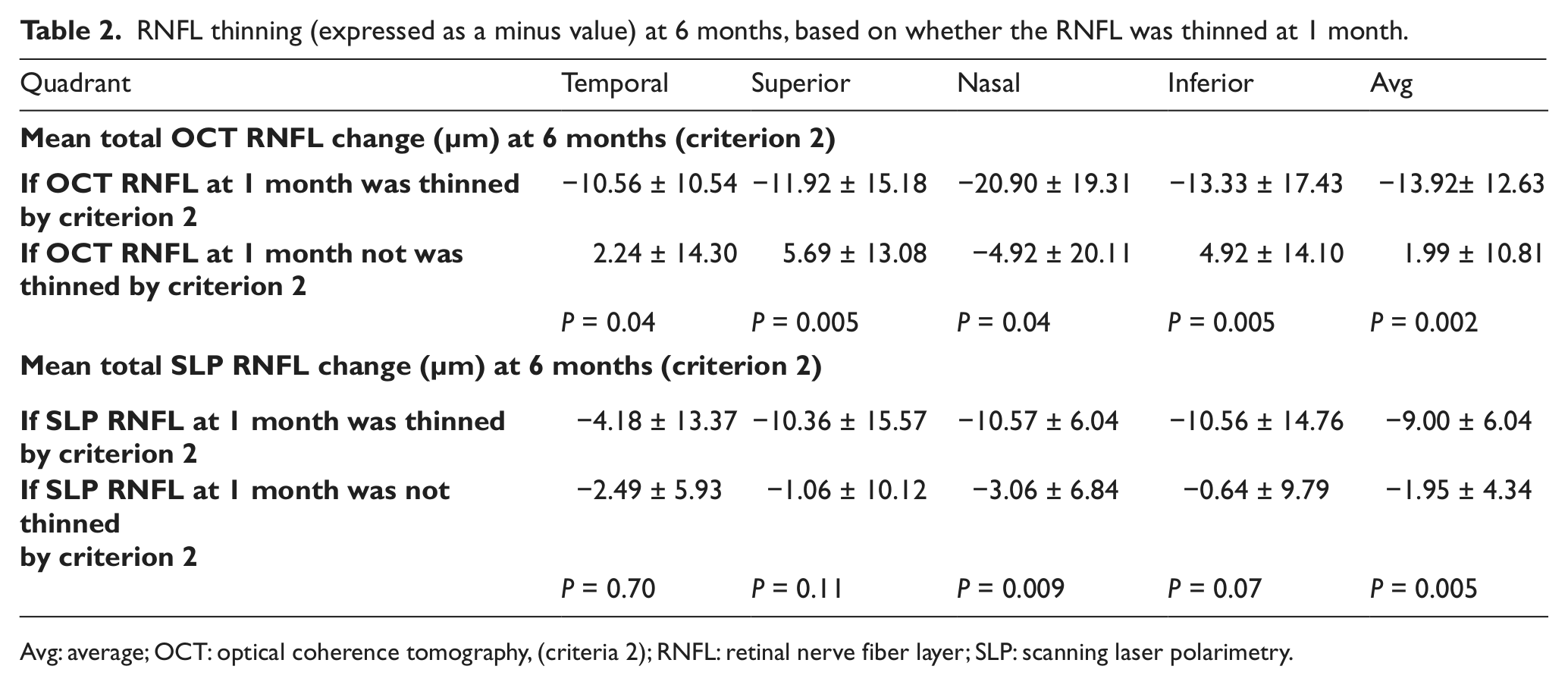
Avg: average; OCT: optical coherence tomography, (criteria 2); RNFL: retinal nerve fiber layer; SLP: scanning laser polarimetry.
The amount of average RNFL thinning at 6 months correlated with the 6-month MD for OCT (r = 0.48; p = 0.03) and with the 6-month MD (r = 0.56; p = 0.003) and visual acuity (r = −0.64; p = 0.001) for SLP. For both OCT and SLP, the average or quadrant RNFL thinning at 6 months was not significantly different between patients with MS or without an MS diagnosis (data not specifically shown) or whether the patients were being treated with corticosteroid therapy.
Discussion
In this prospective study of the RNFL in patients with acute optic neuritis, we showed there is a correlation between RNFL at 1 month and RNFL loss at 6 months. This suggested that by 1 month, extensive and permanent axonal injury had already occurred in the affected eyes, which is proportional to the loss at 6 months. This 1-month time point was in concert with the findings from the Optic Neuritis Treatment Trial (ONTT) that showed moderate/severe vision loss at 1 month predicted a visual deficit at 6 months. 15
Both OCT and SLP (with ECC) showed RNFL thinning at 6 months, confirming that SLP is comparable to OCT for evaluating nerve fiber loss in patients with demyelinating disease.10,21,22 In our study, the RNFL thinning or loss was similar across all quadrants, for OCT and SLP at 6 months. Most of the RNFL thinning shown with either SLP or OCT occurred by 3 months (data not shown except in Figure 1), with a further minor decrease at 6 months. The 3-month time point similarly showed that most vision recovery occurred in the ONTT, with mild further recovery of visual acuity (mean: 0.02 ± 0.15 LogMAR) and visual field MD (mean: −0.47 ± 2.66 db) change at 6 months.16,23
Eyes with RNFL thinning at 1 month had a greater degree of RNFL thinning at 6 months. In general, eyes with RNFL thinning at 1 month had more regional quadrants thinned by 6 months. As previously shown in the analysis of the National Eye Institute-supported ONTT, poor recovery of vision at 1 month, defined as visual acuity of 20/50 or worse, or visual field mean deviation of −15.0 db or worse, is associated with poorer vision outcome at 6 months; 16 however, it cannot be definitively determined whether the observed RNFL thinning was due to a loss of axons or whether some thinning of the remaining axons was due to a decrease in axoplasm. 6 Compared with other types of optic nerve injury, such as glaucoma and non-arteritic anterior ischemic optic neuropathy (NAION), the excellent level of vision recovery at 6 months that is typical of optic neuritis probably accounts for the lack of correlation between the 1-month SLP and OCT RNFL with the 6-month vision.
Measurements of RNFL by either OCT or SLP at 1 month were equally predictive of RNFL at 6 months. OCT and SLP measure different properties of structures in the retina, with SLP dependent on the measured birefringence. Birefringence in the retina arises from the RNFL and is due to the array of parallel cylindrical organelles, such as axonal membranes, microtubules and neurofilaments.24,25 The RNFL birefringence induces a phase shift in one of two orthogonal polarized light beams, reflected after passing through bundles of nerve fibers. This results in a delay: this slowing is termed retardance. The retardance is proportional to the RNFL thickness, so it is used in an algorithm to calculate RNFL thickness: a retardance decrease reflects RNFL thinning 26 or microtubule loss. 27 As we previously showed, 1 month after acute optic neuritis the OCT often shows persistent swelling in the RNFL, which may obscure coexistent regional thinning. 7 We anticipated that SLP would not be as confounded by coexisting edema and would show axonal injury earlier, which has been reported at presentation with NAION. 28 The loss in retardance in NAION appears to reflect changes in retinal birefringence similar to the microtubule loss that occurs after the induction of depolymerization in the experimental colchicine model27,29 or retinal ischemia; 30 however, reduced birefringence can be transient and may, in part, reflect axonal swelling at presentation in optic neuritis (Kupersmith M, et al. Invest Ophthalmol Vis Sci 2009; 50: E-Abstract 5664). In any event, the current commercially-available technology to perform SLP does not separate permanent from transient changes in birefringence in optic neuritis.
In contrast to another prospective study, 2 we found no preferential RNFL loss in the temporal quadrant as compared with other quadrants, even with our use of SLP with ECC to improve the sensitivity for demonstrating the temporal RNFL. This is in agreement with a study using SLP in 25 patients with a prior optic neuritis 8 and with a study utilizing OCT in 28 patients. 31 Our finding would appear to make sense, because there is no known immunological or inflammatory mechanism that could account for preferential injury to one region or type of axons within the optic nerve, and the breadth of the changes seen on MRI suggests that entire cross-sections of the nerve are affected acutely. 16
The 6-month RNFL thickness average and RNFL thinning, for both OCT and SLP, correlated with visual performance at the 6-month point, particularly in the mean deviation of the visual field, similar to the correlation found in glaucoma. 12 This was previously reported for OCT by Trip et al. 1 in eyes with poor recovery at least 1 year after optic neuritis, and by Costello et al 2 at 6 months; however, our results were dissimilar to studies on optic neuritis utilizing SLP that used older, less reliable methods of corneal compensation that did not show a relationship with SLP and vision. 9 Additionally, more sensitive measures of vision performance, such as contrast sensitivity16,23 or low contrast visual acuity10,32 might better correlate with thinning of the RNFL or even the retinal ganglion cell layer.
Assessing the 1-month time point for structure and function after acute optic neuritis (and possibly for some types of MS episodes) for judging the outcome of the attack may help in assessing treatment efficacy at this early time point. Certainly, any potential neuroprotective therapy would need to be initiated before 1 month. To date, the visual function and now the vision system’s structural measure, RNFL, measured at the 1-month time point, remain the only factors or “biomarkers” predictive of attack outcome for an episode of optic neuritis. However, the amount of vision loss, as measured by visual acuity (r = 0.62; p = 0.001) or mean deviation (r = 0.73; p = 0.001) appears to be a comparable or slightly more robust predictor of vision outcome at 6 months in the ONTT. 16 It is anticipated that alternative measures of structural change, such as retinal ganglion cell thickness, will not be confounded by edema or axonal swelling, and yet may show neuronal injury sooner and become earlier predictors of optic neuritis attack outcome. 33
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This work was supported by Pearle Vision Foundation, Veterans Administration (Merit Grant; Rehabilitation Division), Research to Prevent Blindness and the Pomerantz Chair in Ophthalmology.