
Abstract
Objectives:
The objective of this paper is to estimate the association between multiple sclerosis (MS) and measures of sun exposure in specific age periods in Norway and Italy.
Methods:
A total of 1660 MS patients and 3050 controls from Italy and Norway who participated in a multinational case-control study (EnvIMS) reported sun habits during childhood and adolescence.
Results:
A significant association between infrequent summer outdoor activity and increased MS risk was found in Norway and in Italy. The association was strongest between the ages of 16 and 18 years in Norway (odds ratio (OR) 1.83, 95% confidence interval (CI) 1.30–2.59), and between birth and age 5 years in Italy (OR 1.56, 95% CI 1.16–2.10). In Italy a significant association was also found during winter (OR 1.42, 95% CI 1.03–1.97). Frequent sunscreen use between birth and the age of 6 years was associated with MS in Norway (OR 1.44, 95% CI 1.08–1.93) after adjusting for outdoor activity during the same period. Red hair (OR 1.67, 95% CI 1.06–2.63) and blonde hair (OR 1.36, 95% CI 1.09–1.70) were associated with MS after adjusting for outdoor activity and sunscreen use.
Conclusion:
Converging evidence from different measures underlines the beneficial effect of sun exposure on MS risk.
Introduction
The geographical distribution of the prevalence and incidence of multiple sclerosis (MS) has generally been attributed to regional genetic and environmental differences, 1 including the level of ultraviolet radiation (UVR). 2 As sun exposure is the determining factor for vitamin D status in most populations, it has been suggested that sun exposure to some extent mediates its effect on MS risk through vitamin D. 3 Both vitamin D and sun exposure individually have immunomodulatory properties that could provide a biologically plausible explanation for their effect on autoimmune diseases such as MS.4,5
Previous studies suggest that sun exposure during the prenatal period, 6 childhood7,8 and adolescence 9 may influence the risk of developing MS. The effect of circulating vitamin D levels has mainly been studied in late adolescence,10,11 but there is evidence that vitamin D is involved both in immune development and maturation early in life. 12 Deficiency of the vitamin has also been associated with other autoimmune diseases. 13
UVR varies with season, time of day, weather conditions, altitude and latitude. 14 In Norway, with a latitude of 58–71 degrees, during the winter there is insufficient UVR to produce vitamin D for four to five months. 14 A recent study showed that the nadir vitamin D levels in the winter were 50% below the maximum summer levels and that 76% of the study population at some point were vitamin D deficient (<50 nmol/l) at this latitude. 15 Further, among 1000 adolescents from 10 different European cities, 80% had suboptimal levels (<75 nmol/l) of vitamin D. 16 The widespread insufficiency observed makes the vitamin D hypothesis attractive because of the large potential an intervention might have.
We wanted to further investigate the relation between sun exposure and MS risk in age-specific periods from birth to disease onset. The frequency of reported outdoor activities as well as sunscreen use were used as indirect measures of UVR exposure. We also wanted to study seasonal variations comparing Norway and Italy using these same measures of sun exposure.
Materials and methods
Study design
The study design and methodology has been reported elsewhere. 17 The International multicentre case-control study of Environmental Factors In Multiple Sclerosis (EnvIMS study) was carried out in well-defined geographic areas in Europe (Italy and Norway) and is ongoing in Canada, Sweden and Serbia. The aim of the study was to examine the effect of self-reported exposures to infections, sun exposure and lifestyle factors on the risk of MS and to disclose possible variations in risk between populations with differences in the disease risk using a common methodology.17,18 To assess age-specific past exposures among the participants, a novel postal self-administered questionnaire (EnvIMS-Q) was developed. It was first designed in English and then translated into different languages. Further, it was tested for reliability, cross-cultural validity and perceived difficulty of completing the questionnaire. 17
Study area
Italy and Republic of San Marino
The EnvIMS Italian sub-study involves two areas: Sardinia, situated between 38 and 41 degrees northern latitude, and the province of Ferrara, situated in northern Italy at 44 northern latitude. The cases were selected from established patient registries in each of the participating centres. The prevalence of MS has been reported to exceed 150 per 100,000 in Sardinia 19 and 120 per 100,000 in Ferrara. 20 The Republic of San Marino is situated at 43 degrees northern latitude, surrounded by Italy. It has an estimated MS prevalence of 167 per 100,000. 21 Because of its similarity and proximity to Italy it was combined with data collected in Sardinia and Ferrara for the analysis.
Norway nationwide
Norway is situated between 58 and 71 degrees northern latitude and has an estimated MS prevalence of 165 per 100,000, ranging from 106 to 246 per 100,000 in surveys from different counties. 22 EnvIMS cases were selected from the Norwegian MS registry and Biobank, Haukeland University Hospital, Bergen. 23
Study population
The current study includes participants from Italy and Norway aged 18 years or older at the time of selection. The cases were recruited from population-based MS registries and were diagnosed according to the McDonald criteria 24 with a clinical onset within 10 years prior to data collection (i.e. 1999–2008). Four times as many age and sex frequency-matched controls were randomly selected from the population registries of each region under study. Among the 1368 eligible cases in Norway invited to the study, 953 (69.7%) chose to participate, while 1717 (36.3%) of the 4728 invited controls responded and were included. The participation rate was higher in women than in men, both among the cases (72.0% and 64.6%) and controls (39.4% and 29.4%). In Italy 707 (41.8%) of the 1692 eligible cases chose to participate, while 1333 (20.8%) of the 6414 invited controls responded and were included. The participation rate was slightly higher among men than in women, both among cases (49.9% and 38.4%) and controls (23.2% and 19.8%). Population characteristics are described in Table 1.
Population characteristics in the EnvIMS study.
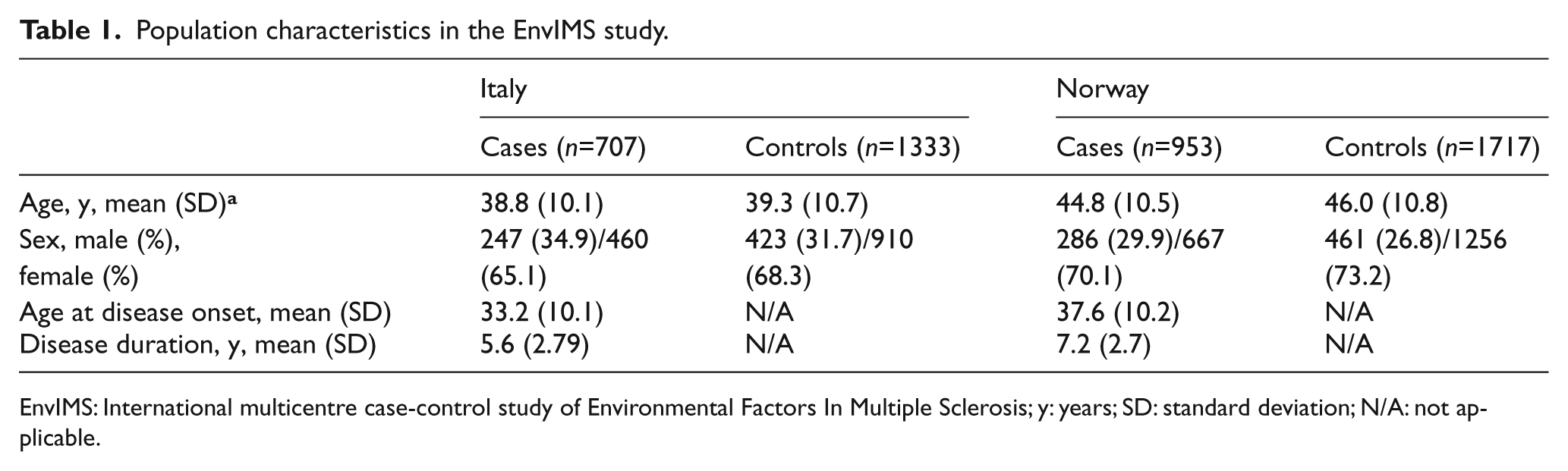
EnvIMS: International multicentre case-control study of Environmental Factors In Multiple Sclerosis; y: years; SD: standard deviation; N/A: not applicable.
Exposure
Information on outdoor activity during summer and winter in different age periods was used as a measure of sun exposure. 25 In Norway the age periods were adapted to the school system, while in Italy five-year age-intervals were used. The frequency of outdoor activity was reported on a four-point scale including ‘virtually all the time’, ‘quite often’, ‘reasonably often’ and ‘not that often’. We also included questions on sun exposure during vacation. In Norway this was specified as the number of holidays at southern latitudes, while in Italy we asked about number of hours spent daily in the sun during weekends and vacation.
The use of sunscreen is a determining factor for the amount of UVR available for cutaneous vitamin D production. 26 This factor could also modify the effect of sun exposure as measured by frequency of outdoor activity. Information on the use of sunscreen for each age category was reported as ‘Did you normally use sunscreens?’ with response categories ‘Not so often’, ‘Sometimes’, ‘Quite often’ or ‘Almost always’. In Italy the question on sun protection included sunscreen use and protective clothing.
We also included questions on other factors that could modify the effect of sun exposure such as skin colour, skin reaction to first sun exposure, and hair and eye colour. Skin colour was assessed by asking the participants to tick off the colour of the skin on their inner arm (without tanning) on a scale of skin colours ranging from 1 (fair skin) to 10 (dark skin). Skin reaction to sun exposure was reported as ‘I always burn and I never tan’, ‘Usually burn, tan less than average (with difficulty)’, ‘Sometimes mild burn, tan about average’ or ‘Rarely burn, tan more than average (with ease)’. Eye colour was reported as ‘black, brown, grey/green or blue’. The original hair colour was reported as ‘black, dark brown, light brown, blond or red’. We also included information on the participant’s education and ethnicity of both parents. The Norwegian questionnaire included the categories ‘Norwegian/European/Western, Sami, Middle East, African, Latin American and Asian’, while the Italian included different parts of Italy ‘(north, central, south, Sardinia and Sicily) and abroad’.
Statistical analysis
The association between disease and exposures was estimated as odds ratios (OR) with 95% confidence intervals (95% CIs) using logistic regression. Outdoor activity was initially treated as an ordinal variable ranging from 1 (outdoor virtually all the time) to 4 (not that often), with an OR calculated as the difference between 4 and 1. To describe the effect related to each category of variable outdoor activity, we also ran a logistic regression model including outdoor activity as a categorical variable. Skin colour, skin reaction to first sun exposure, hair and eye colour and sunscreen use were assumed to be potential modifying factors. A possible interaction between outdoor activity and these potential modifying variables was tested by including the relevant interaction term in the model. Similarly, the difference between Norway and Italy was tested by including an interaction term between country and outdoor activity in the model. All analyses were adjusted for sex and age.
All controls were assigned an index age based on the distribution of age at onset for the cases and randomly distributed to the controls. Events or reported behaviour occurring after the age at onset/index age were not considered as exposure.
Standard protocol approvals, registrations, and patient consents
EnvIMS-Q is an anonymous postal questionnaire with identical format both for cases and controls. A cover letter with the study aims and relevance, the request and instructions for participation and the investigators’ contact information, was enclosed with the questionnaire. Return of the questionnaire was considered as implied consent.
The EnvIMS study received ethics approval at each collaborating institution/health districts in Italy (Sassari, Olbia-Tempio, Nuoro, Cagliari and Province of Ferrara Ethical Committee) and Norway (n. 11, 18.12.2008; NORWAY, Regional Ethical Committee for Medical and Health Research for Western Norway).
Results
There were marked differences in the distribution of reported outdoor activity between Norway and Italy (Figure 1). During the summer as many as 9.3% of the controls from Italy reported infrequent outdoor activity in early childhood, compared to only 1.6% in Norway. Furthermore, during the winter 34.1% of the Italian controls reported infrequent outdoor activity at the same ages, compared to only 6.1% in Norway.
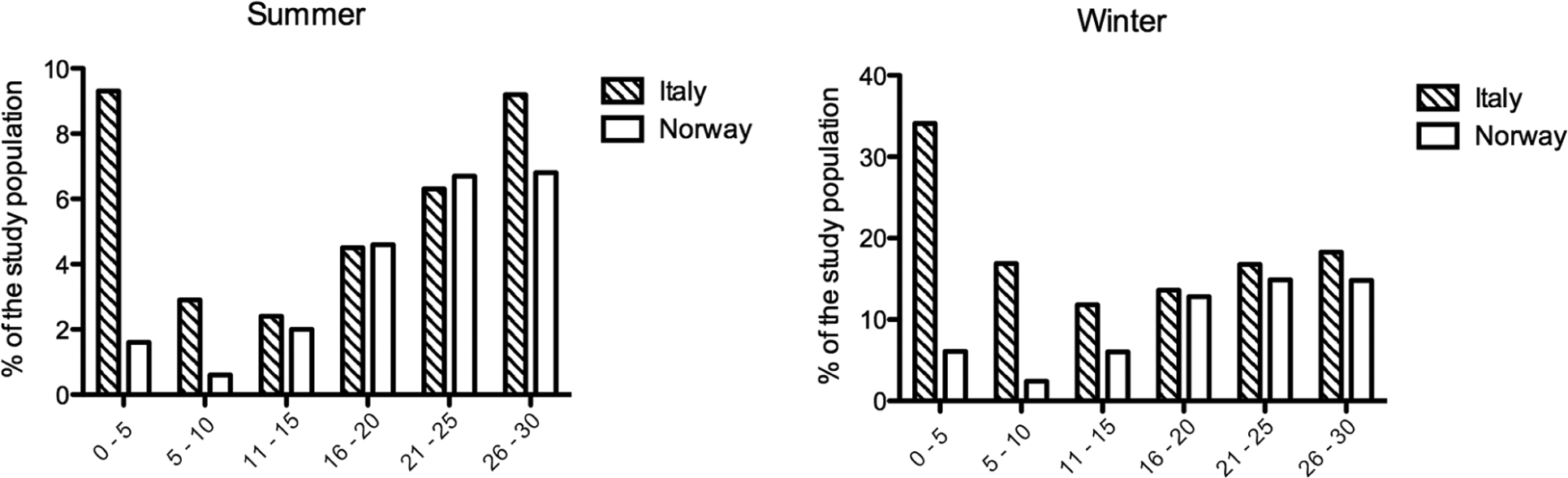
Infrequent outdoor activities in different age periods.
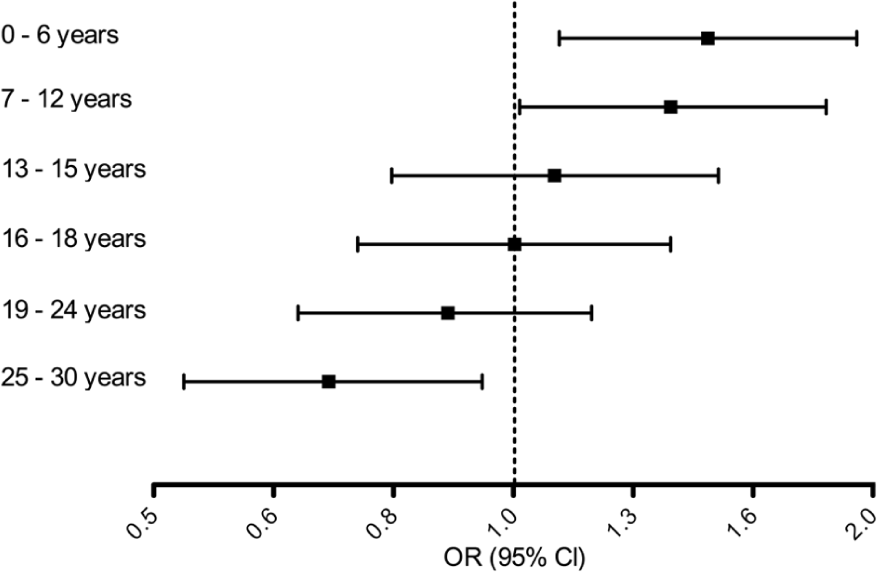
Comparing cases and controls, we found a statistically significant association between infrequent outdoor activity and an increased MS risk both in Norway and in Italy (Figure 2) for selected age ranges. The association in Norway was significant during adolescence between age 13 and 18. The association with the largest point estimate was seen for summer between age 16 and 18 years (OR 1.83, 95% CI: 1.30–2.59). Outdoor activity during winter was neither significant at this age (OR 1.27; 95% CI: 0.88–1.82) nor at any other age period. We did not find any effect of sun holiday trips to southern latitudes (data not shown) for the Norwegian study population.
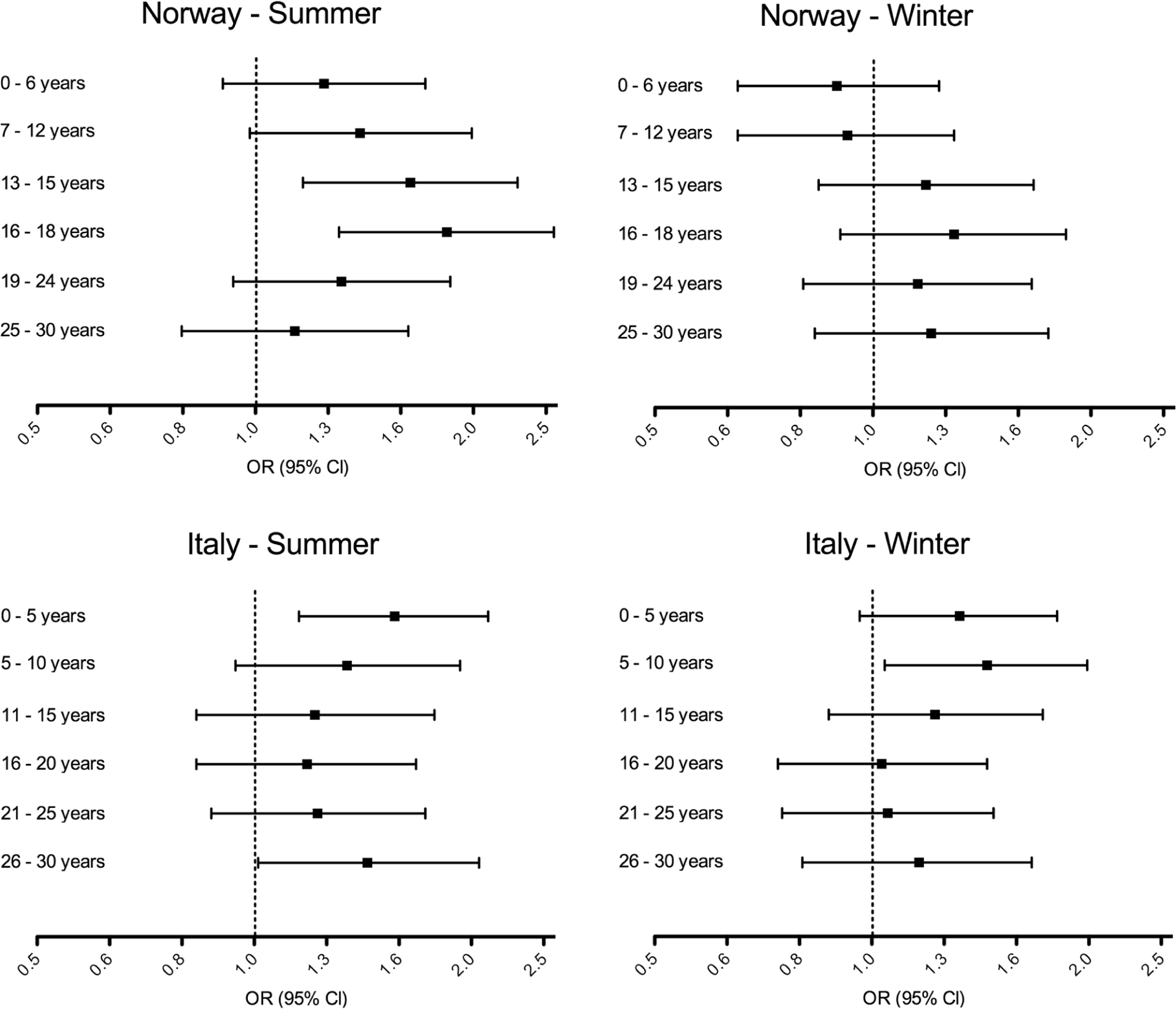
Association between outdoor activities and MS risk.
In Italy a significant association between infrequent outdoor activity in the summer and an increased MS risk was seen in early childhood, with the period from birth to the age of 5 years showing the strongest effect (OR 1.56; 95% CI: 1.16–2.10). We also found a significant association in the winter in Italy (OR 1.42; 95% CI: 1.03–1.97). Time spent in the sun during weekends and vacations was also associated with MS in Italy, with the strongest effect between age 16 and 18 (OR 1.79; 95% CI: 1.32–2.44).
A statistical test comparing Norway and Italy revealed no significant differences between summer outdoor activity and MS risk in the two countries. Further, when combining the two countries, infrequent outdoor activity was associated with an increased MS risk in all the age intervals, except the last (25–30 years). The OR ranged from 1.35 (95% CI: 1.09–1.68) in the earliest age interval to 1.51 (95% CI: 1.20–1.90) in late adolescence.
Using outdoor activity as a categorical variable and analysing the age periods with the strongest effect, the increased risk of MS seemed to be related to the groups reporting the least amount of sun exposure, particularly in Norway (Table 2). The effect of outdoor activity was only slightly attenuated by including skin colour, skin reaction to first sun exposure, hair and eye colour or sunscreen use in the model (data not shown). No significant modifying effect of any of these variables was found by testing the relevant interaction terms. The association between these variables and MS risk is shown in Table 3.
Odds ratio of multiple sclerosis in Norway and Italy by levels of sun exposure in the EnvIMS study. The table shows the results for the age periods with the strongest effect in each country (age 16–18 in Norway and age 0–5 in Italy).
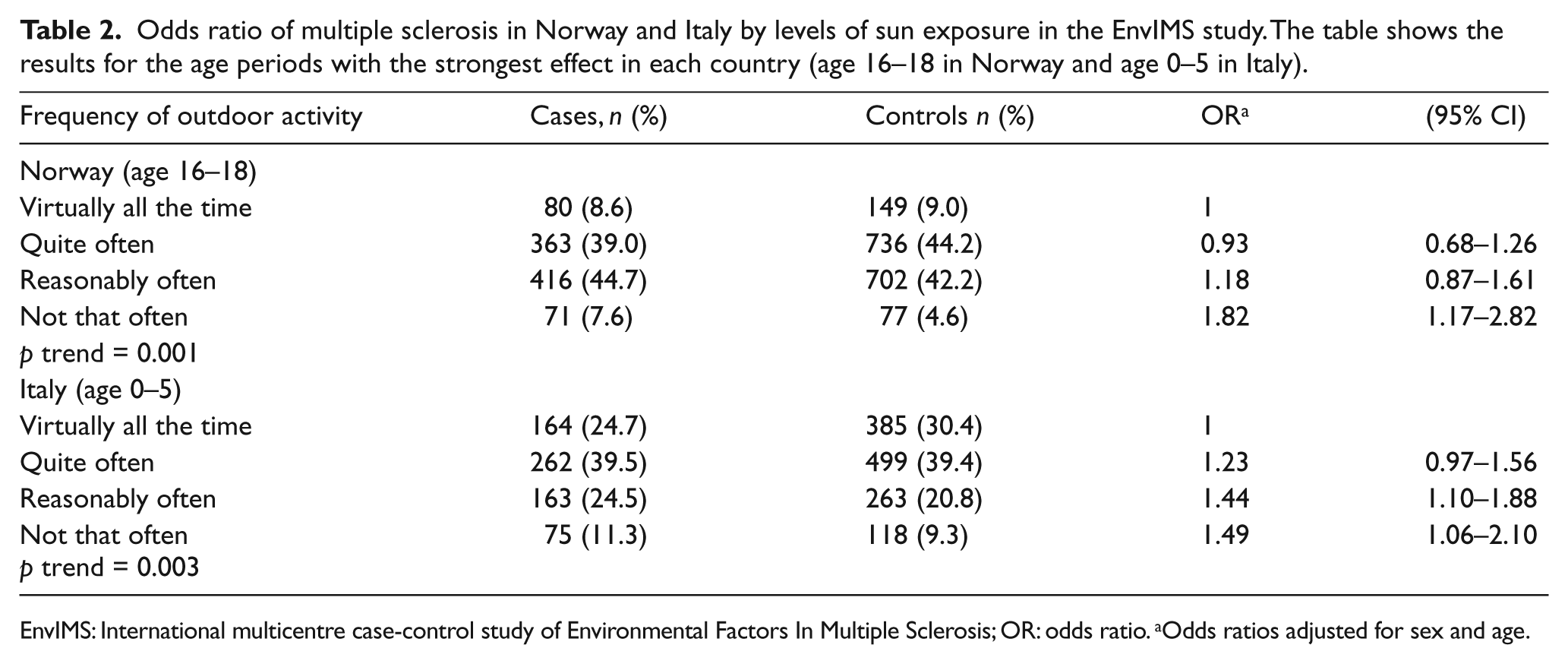
EnvIMS: International multicentre case-control study of Environmental Factors In Multiple Sclerosis; OR: odds ratio. aOdds ratios adjusted for sex and age.
The association between hair colour, skin colour, eye colour, skin reaction to sunlight and MS risk.
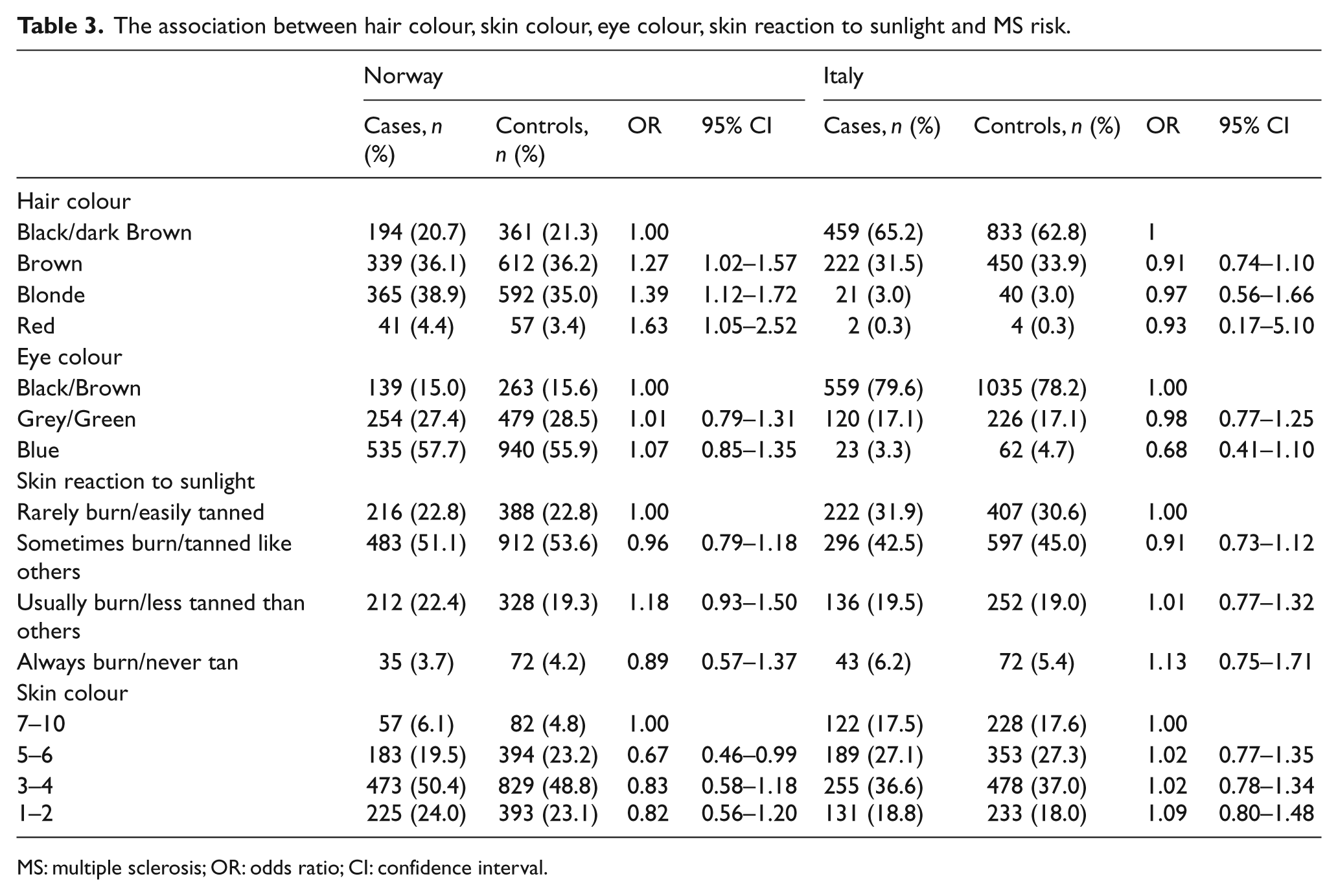
MS: multiple sclerosis; OR: odds ratio; CI: confidence interval.
In Norway the risk of MS was significantly increased for fair-haired and red-haired persons compared to persons with black hair (Table 3). We found further that those with red and blonde hair reported a more frequent sunscreen use but a similar frequency of outdoor activity compared to those with darker hair (data not shown). Still, the risk related to blonde and red hair remained similar after adjusting for sunscreen and outdoor activity (OR 1.36, 95% CI: 1.09–1.70 and OR 1.67, 95% CI: 1.06–2.63). There was little variation in hair colour among the Italian participants and no association to hair colour was found (Table 3).
In Norway we found a significant effect of sunscreen use during early childhood. Frequent use of sunscreen between birth and the age of 6 years was associated with an increased MS risk (OR 1.44 95% CI: 1.08–1.93) after adjustment for outdoor activity in the same period (Figure 3). The estimates remained similar after adjusting for skin colour (OR 1.41 95% CI: 1.06–1.89). There was also an effect of sunscreen use during age 7–12 years. No effect of sun protection was found in the Italian population.
The association between frequent sunscreen use and MS risk in Norway.
No association between education and outdoor activity was seen and only a modest association between education and use of sunscreen was found. Further, the association between outdoor activity and sunscreen use was not changed after adjusting for education (data not shown).
Discussion
In this large case-control study, both frequency of outdoor activity and sunscreen use early in life were associated with subsequent MS risk. Thus, converging evidence from different measures suggest that low sun exposure in early life increases MS risk. Frequent outdoor activity was associated with reduced risk of MS with the strongest effect seen in early childhood in Italy and in adolescence in Norway. We found significant associations both for summer and winter outdoor activity in Italy, while only for summer outdoor activity in Norway.
These observations add to previous studies showing the importance of low sun exposure on MS risk.7–9,27 The finding of winter outdoor activity being important in Italy but not in Norway corresponds to the differences in seasonal sun exposure between the two countries. In Norway there is not enough ultraviolet B rays (UVB) during winter to sustain vitamin D synthesis, while this seems to be possible to some extent in Italy. 14 In a recent study there was no observed seasonal variation in vitamin D status in an Italian study population. 28 This suggests that our findings may reflect the effect of sun exposure on vitamin D synthesis.
The age period when environmental risk factors in MS might be of importance spans from the prenatal period 6 to just prior to clinical onset. 27 We found that the effect of infrequent summer outdoor activity was strongest in early childhood in Italy and in adolescence in Norway, although there were no significant differences between the two countries. While differences in age-related susceptibility could explain the observed patterns, random variation is also likely to play a role. Overall, our results suggest that infrequent outdoor activity is associated with MS from birth throughout adolescence.
Sunscreen has been found to block vitamin D production in the skin when applied according to World Health Organisation (WHO) recommendations. 26 The association between sunscreen use and MS risk provides further evidence of sun exposure being an important environmental factor and also suggests that the effect is mediated through the skin. Even though sunscreen use is associated with increased recreational sun exposure duration, 29 which in itself could lead to a decreased MS risk, the net effect we found in early childhood was an increased risk. As the association remained after adjusting for skin colour, it is unlikely that sunscreen only is a marker for a fair skin type. However, as sun sensitivity was not objectively measured, this possibility cannot be excluded. We found the association only in early childhood, which could indicate that this is the sensitive period. However, in early childhood sunscreen is more likely to be applied by parents, which could increase the chances of proper use.
Skin phototype could also modify the effect of sun exposure, as the pigmentation of the skin both affects vitamin D production and sun tolerance. 30 However, neither the skin colour nor any of the other variables related to skin phenotype showed any modifying effect on outdoor activity on MS risk. On the other hand, we found that individuals with fair or red hair had an increased risk of MS independently of outdoor activity and sunscreen use. An increased MS risk among individuals with a red hair colour has previously been reported, and differences in sun-related behaviour and a reduced response to the anti-inflammatory alpha-melanocyte-stimulating hormone (α-MSH) were suggested as possible mechanisms for the association. 30 We observed a more frequent use of sunscreen among those with red hair, supporting behavioural differences related to lower sun tolerance for these individuals. Even if there were no observed differences in outdoor activity related to hair colour, those with a low sun tolerance could tend to avoid the sun while still being outside and therefore being less exposed to UVR. Lastly, red and fair hair colour could be predictive of those vulnerable to the disease by some other unknown mechanism including genetic factors.
The risk of recall bias is inherent in any case-control study, particularly when studying the effect of factors suspected by the cases to have played a role in the development of their disease. The low participation rate among the controls may also contribute to a selection bias and could be a limitation to the internal validity of the study. Non-response might have been associated with a low socio-economic status, which again has been associated with MS. 31 However, there was no association between outdoor activity and education among the responders, which reduces the probability of selection bias due to differences in socio-economic status. Further, the finding in our study of a general increased risk of MS associated with lack of sun exposure is consistent with previous research, which included objective measures of sun exposure such as actinic damage. 27 Further, the age-related effects reported in the present study is less likely related to recall bias, since it is unlikely that a possible differential recall between cases and controls should vary according to the age period reported. Efforts were also made to reduce the general misclassification of the reported age at exposure by adapting the age periods to the school system in the country. Where the participants could not remember the sun exposure they were encouraged to ask their parents, which likely has increased the validity of the report in childhood.
Several previous studies have shown that sun exposure plays a role in MS risk,7–9 including a study reporting a decreased risk of MS among persons with actinic damage, which is a marker of high cumulative sun exposure over time. 27 A question that remains open is whether the observed effect is mediated by sun exposure itself or by factors mediated by sun exposure such as vitamin D. The seasonal variation in the association between frequency of outdoor activity and MS risk we observed in Norway could suggest that the effect is mediated through UVB as it varies more with season than ultraviolet A rays (UVA) at high latitudes.14,32 UVB mediates vitamin D production in the skin, but also affects other biological processes that could be relevant for MS 33 and has been shown to suppress the development of experimental autoimmune encephalomyelitis independently of vitamin D synthesis. 34 Accordingly, the association between actinic damage and the first demyelinating event indicative of MS remained after adjusting for vitamin D levels. 27 Others, on the other side, have argued that this association could still be all vitamin D mediated as a single vitamin D measurement might not reflect the levels over time prior to disease. 35 A high intake of vitamin D, either through diet or supplementation, seems to influence the risk of the disease, 36 consistent with a direct role of vitamin D in MS development.
In conclusion, this large study with data from Norway and Italy provides converging evidence from different measures of the beneficial effect of sun exposure on MS risk. The association was found both in childhood and adolescence, including the period close to birth.
Footnotes
Acknowledgements
The authors wish to acknowledge Bettina Galanti, Department of Clinical and Experimental Medicine, University of Sassari, Italy (European sub-study administration and logistics), C. Monaldini, Department of Neurology, Hospital of S. Marino, San Marino (data collection), Sally Killborn, Research Institute of the McGill University Health Centre, Montreal Canada (EnvIMS-Q format, dissemination, graphics), Erin Lundy, Department of Mathematics and Statistics, McGill University (data quality assessment), Azadeh Shohoudi, Department of Mathematics and Statistics, McGill University (data quality assessment), Catherine Tansey, Research Institute of the McGill University Health Centre (project coordinator, EnvIMS-Canada), Elaina Uniat, Research Institute of the McGill University Health Centre (project coordinator Canadian EnvIMS-Q feasibility testing) and Bin Zhu, Research Institute of the McGill University Health Centre, Montreal Canada (statistical assistance).
Conflicts of interest
A.M. Landtblom has received speakers honoraria and grants from Biogen Idec, Teva, Bayer, Merck and Serono. A. Lossius has received speaker honoraria and unrestricted research grants from Novartis. K.M. Myhr has received speaker honoraria, travel support and/or unrestricted research grants from Bayer Schering, Biogen Idec, Genzyme, Sanofi Aventis, Novartis and Merck Serono. T. Holmøy has received speaker honoraria, travel support and unrestricted research grants from Sanofi Aventis, Biogen Idec, Bayer Schering, Novartis and Merck Serono. K. Bjørnevik, I. Casetta, J. Drulovic, E. Granieri, M.T. Kampman, K. Lauer, S. Magalhaes, T. Pekmezovic, M. Pugliatti, T. Riise, K. Wesnes and C. Wolfson have nothing to declare.
Funding
The study was supported by grants from the Italian MS Society/Foundation (Fondazione Italiana Sclerosi Multipla, FISM, grants n. 2007/R/14, and n. 2008/R/19 to M. Pugliatti), The Western Norway Regional Health Authority (Helse Vest) Norway (grants n. 911421/2008 to M. Pugliatti and n. 911474/2009 to K-M Myhr), The University of Bergen, Norway (2007 to T. Riise) and The Multiple Sclerosis Society of Canada (2011–2013 to C. Wolfson).