
Abstract
Background:
In a retrospective study, we have previously shown that work ability was improved after the initiation of natalizumab treatment in relapsing–remitting multiple sclerosis (RRMS). In another prospective trial (TYNERGY) the effect on MS-related fatigue was evaluated after 12 months of treatment with natalizumab. A comprehensive Capacity for Work Questionnaire (CWQ) was used to collect data regarding number of working hours and sickness absence. The predefined intention-to-treat analysis regarding work ability did not, however, show significant results.
Objectives:
The objective of this paper is to assess the amount of sick leave in RRMS before and after one year of natalizumab treatment and correlate it to fatigue and walking ability.
Methods:
This is a post-hoc analysis of the complete data from the CWQ used in the TYNERGY trial.
Results:
MS patients receiving sickness benefit before start of treatment reduced their sickness benefit by an absolute change of 33% after one year of natalizumab treatment. Younger age and improvement of walking ability correlated significantly with reduction of sick leave.
Conclusions:
This ad-hoc analysis of prospectively collected data supported our previous retrospective study and thus indicates a positive relationship between natalizumab treatment and improvement in work ability.
Keywords
Introduction
Multiple sclerosis (MS) is a chronic inflammatory disorder of the central nervous system (CNS) and leads to neuronal damage with progressive accumulation of neurologic disability over time. 1 The disease is typically diagnosed around 30 years of age, and MS is one of the major causes of reduced ability to work due to neurologic disease in the Western society.2,3 In a previous Swedish population-based study (n = 307) of MS patients aged 18–64 years, only one-third (34.5%) had no sickness benefit or disability pension, whereas 31% had a full-time sickness benefit or disability pension. 3 According to another Swedish study, MS patients with affected walking ability have about half the ability to work compared to the general population. 4 It is also well documented that increasing disability, in terms of Expanded Disability Status Scale (EDSS), correlates with an increased rate of sick leave, 3 thus it is reasonable to assume that a stable disease course enables continuous work ability. Survey data have shown that reported fatigue and mobility-related problems were the primary symptomatic factors preventing people with MS from remaining in employment.5,6
There is a notable lack of systematic studies regarding the possible influence on occupational life of the more effective immunomodulatory drugs that are available in MS since 2006. We have previously studied the effects of initiating treatment with the monoclonal antibody natalizumab (Tysabri®) on work ability in a retrospective review of data.7,8 We found that work ability increased significantly after one year of natalizumab treatment, which corresponded to an increase in average productivity by a value of approximately € 4000 per year. These data were encouraging but the retrospective design of the study with the potential for recall bias suggested that the results needed further confirmation with prospective data.
Natalizumab belongs to the new generation of biological drugs for treatment of RRMS and acts by inhibiting lymphocyte migration across the blood-brain-barrier. 9 Clinical studies have suggested that natalizumab is more effective than first-line treatments with interferon-beta and glatiramer acetate with respect to preventing relapses and inflammatory activity.9,10 The TYNERGY trial was a multicentre, open-label prospective study in the real-life setting evaluating the effects on fatigue as the primary endpoint after 12 months of treatment with natalizumab in patients with RRMS. 11 The TYNERGY trial showed a significant improvement of MS-related fatigue measured with the validated instrument Fatigue Scale for Motor and Cognitive functions (FSMC) 12 over the course of the one-year treatment in the trial.
As a part of the TYNERGY trial, work capacity was registered using the standardised multimodal questionnaire Capacity for Work Questionnaire (CWQ) 7 and constituted a secondary endpoint. The intention-to-treat (ITT) evaluation of work ability in the TYNERGY trial was predefined as the changes between the different categories of worked hours per week in 10-hour increments calculated with a generalised linear mixed model with change from baseline values as response. No significance was found and one possible explanation may be a lack of sensitivity of the statistical method used for the ITT analyses. In addition, the analyses were performed without any stratification of baseline working capacity. Therefore, we wanted to perform post-hoc in-depth analyses of the prospective data gathered with the CWQ and compare the results with our previous retrospective study that used essentially the same questionnaire. 7 We also wanted to study the relation between fatigue, walking ability and sick leave before and after one year of natalizumab treatment.
Patients and methods
Patients
From the original 162 individuals in the TYNERGY trial, our study population was restricted to those with any type of employment at the onset of the study and stable work conditions over the trial period (n = 115). The level of sickness benefit was registered before and after one year of treatment. Out of the 115 patients, 58 had a full- or part-time sickness benefit and 57 patients were working full time at their employment at the start of natalizumab treatment. The demographic characteristics before starting treatment with natalizumab for both the post-hoc population and the excluded subjects are summarised in Table 1. All data were collected between 23 March 2009 and 30 June 2011.
Baseline characteristics of the investigated cohort.

SB: sickness benefit; DMT: disease-modifying treatment; MS: multiple sclerosis; min: minimum; max: maximum; EDSS: Expanded Disability Status Scale; SD: standard deviation. The excluded population constitutes the patients excluded from the TYNERGY population because of no or unstable working condition. aPearson Chi-Square. bFisher’s exact test.
The study was approved by the institutional ethics review board at the University Hospital of Northern Sweden, Umeå.
Definitions of terms
Sick leave is defined as temporary absence from gainful employment with reimbursement from the society, denominated sickness benefit. In Sweden, a sick leave period may last for a maximum of two years and is registered by the Swedish Social Insurance Agency (SSIA). For longer or permanent incapacity to work, disability pension can be obtained from SSIA. All these types of benefits are paid as full, three-quarters, half or one-quarter benefit, depending on the extent of reduced work ability.
CWQ
The CWQ is a comprehensive inventory of occupation including employment, unemployment, parental leave, sick leave, disability pension, studies or retirement. The number of worked hours per week were categorised as 0, 1–10, 11–20, 21–30, 31–40 and over 40 hours and the amount of sickness benefit and disability pension in 25% increments from 0% to 100%. A classification of work requirements and a number of self-rated levels of physical and cognitive abilities in relation to the work requirements were also registered. A more detailed description of the questionnaire has been published previously. 7
Estimation of change in work ability
Change in sickness benefit was calculated as the net change between the value at baseline and the value after one year of natalizumab treatment in individuals with employment and stable work requirements over the one-year study period. Sickness benefit was determined as percentage (in 25% increments from 0% to 100%) of the patients’ employment. In addition, we performed separate analyses in the groups with and without sickness benefit at baseline since patients not having any sickness benefit at the start of natalizumab treatment did not change that during the course of the study and were thus uninformative regarding this parameter.
Measurements of fatigue and walking ability
To analyse the impact of changes in fatigue and walking ability on changes in obtained sickness benefit, the validated scales from the TYNERGY study were used. Fatigue was measured by the FSMC scale, which is thoroughly described elsewhere and was also the major outcome instrument in the TYNERGY trial.11,12 The FSMC total scale has a range of 20 (no fatigue) to 100 (most severe fatigue) and has cut-off values of mild (≥43), moderate (≥53) and severe (≥63) fatigue. 12 Motor fatigue and ambulation were evaluated via the 6-Minute Walk Tests (6MWT) in which the subjects are instructed to walk as fast and as far as possible during the six-minute tests to assess total distance and motor fatigue. 13 For patients terminating the test prematurely, both distance and time were recorded. 14
Statistical analyses
Statistical analysis was performed using SPSS 21. For baseline characteristics, data were analysed by descriptive statistics (number, percentage, mean and standard deviation). Differences in disease-related baseline characteristics between the post-hoc population and the excluded population were analysed with independent samples t test for parametric variables and with Pearson Chi-Square or Fisher’s exact test for the non-parametric variables. Changes of outcome variables: sickness benefit in percentage, 6MWT in metres, and fatigue in FSMC total score before (at baseline) and after one year of natalizumab treatment, were analysed by paired-samples t test. Pearson’s correlation was used for correlation between net percentage change of sickness benefit and change in walking distance in 6MWT expressed in metres and change in MS-related fatigue expressed in FSMC total score. Linear regression was performed to analyse the age-dependency regarding the net percentage change in sickness benefit and change in walking distance in 6MWT after one-year of natalizumab treatment. For Pearson’s correlation and linear regression, only the group of individuals who had some level of sickness benefit were included since no change within work ability was detected in those who worked full time at their employment at baseline. An α-level of 0.05 was selected for determining statistical significance.
Results
Sick leave was reduced after one year of natalizumab treatment
At baseline, the post-hoc population was divided into two groups based on whether they obtained any degree of sickness benefit (n = 58) or were working 100% of their employment (n = 57). Patients receiving some degree of sickness benefit at baseline decreased their percentage of sickness benefit with a net change of 33% from 57% to 24% (p < 0.001) after one year of natalizumab treatment (Figure 1). Patients working 100% of their employment at baseline retained that level throughout the study (Figure 1).
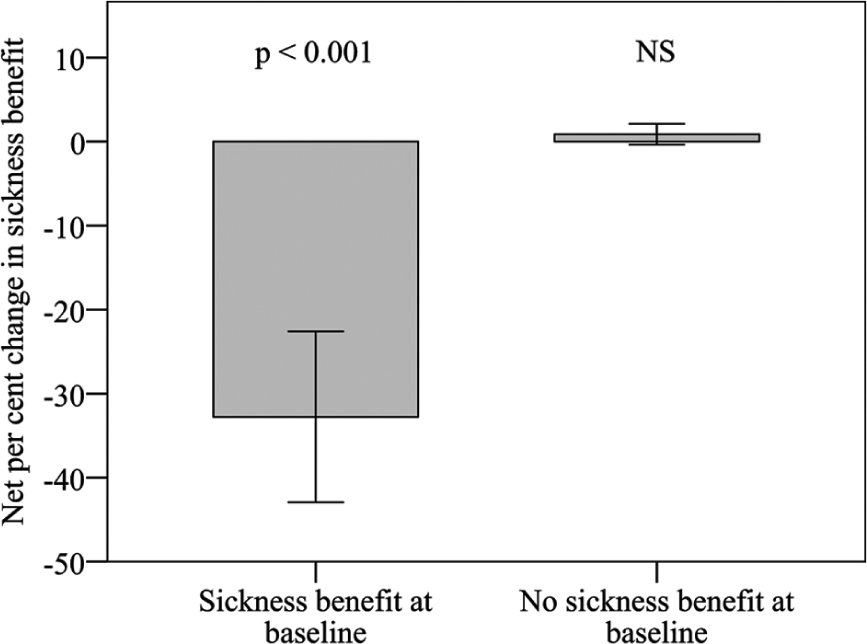
Sickness benefit as percentage of employment was reduced after the 12-month natalizumab treatment for the group with some degree of sickness benefit at baseline with a net of 33% and was stable at a zero level for the group with no sickness benefit at baseline. Error bars show 95% confidence interval.
Correlation between walking distance and sick leave
In both groups with and without sickness benefit at baseline we found a significant increase in the 6MWT after one year of treatment (Table 2). In the subset of individuals with sickness benefit at baseline (n = 58), improvement in walking distance correlated with decreased level of sickness benefit (r = 0.52, p < 0.001) (Figure 2(a)).
Summary results of 6MWT and FSMC.
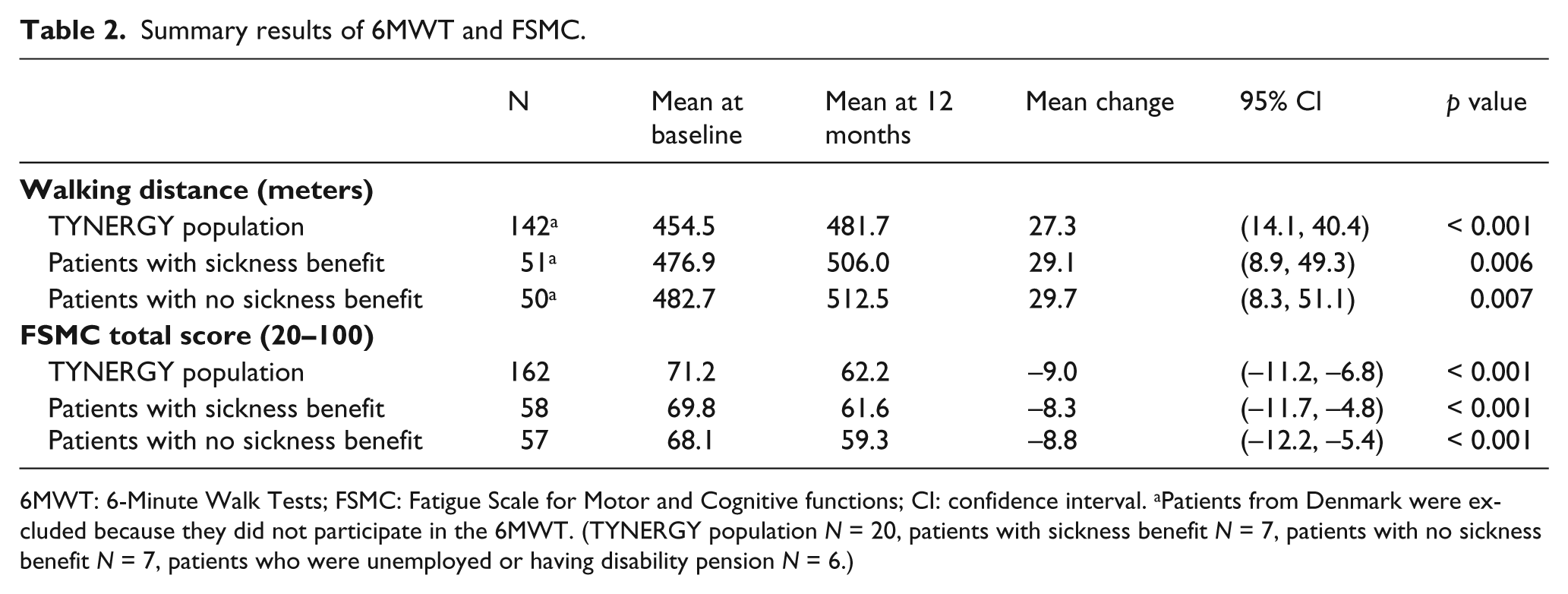
6MWT: 6-Minute Walk Tests; FSMC: Fatigue Scale for Motor and Cognitive functions; CI: confidence interval. aPatients from Denmark were excluded because they did not participate in the 6MWT. (TYNERGY population N = 20, patients with sickness benefit N = 7, patients with no sickness benefit N = 7, patients who were unemployed or having disability pension N = 6.)
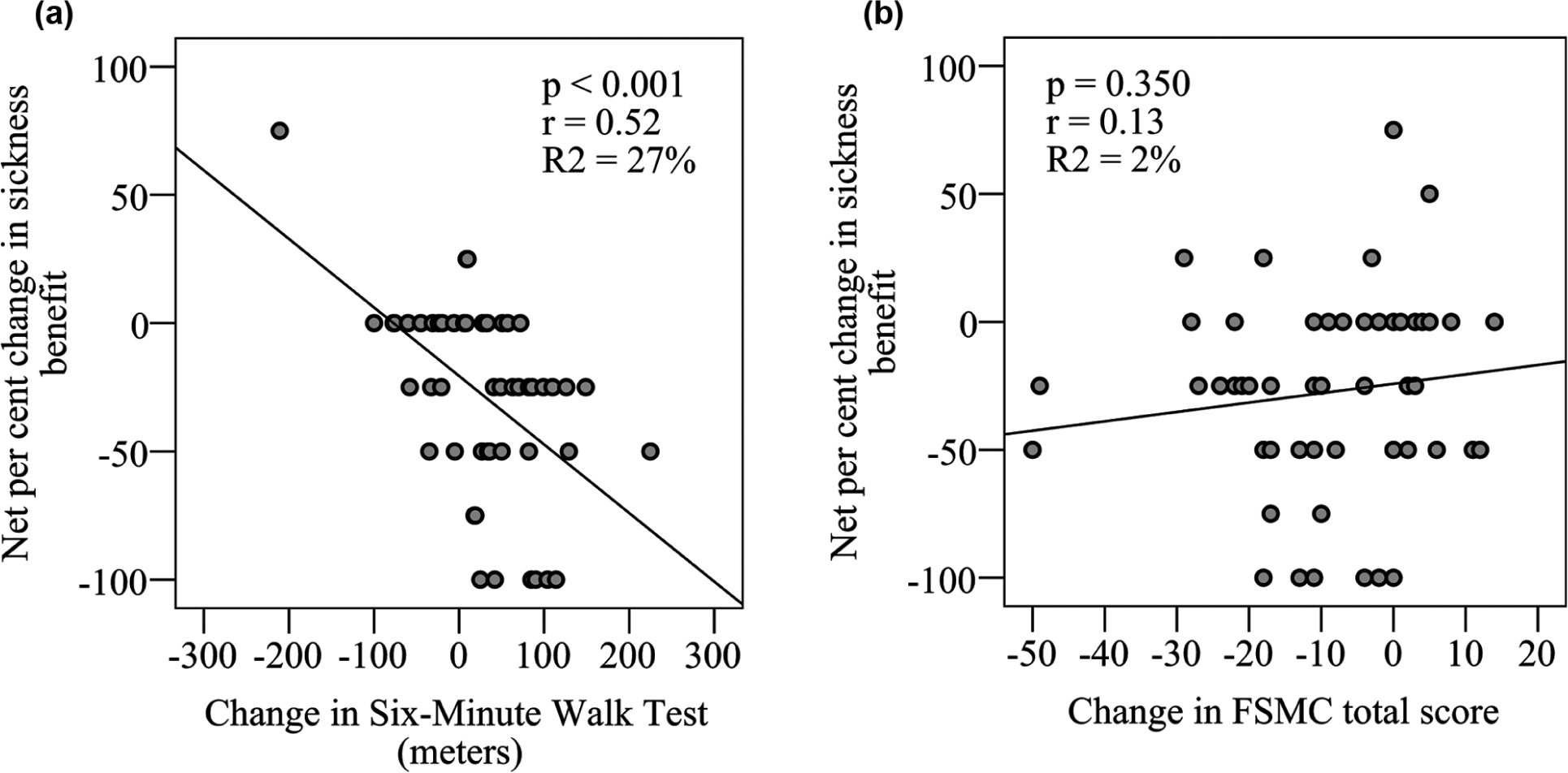
Change in sickness benefit correlated with change in walking distance (a)* but not with change in fatigue as measured with FSMC (b). Only patients with some degree of sickness benefit at baseline were included in the analyses (n = 58). Each point represents one patient.
Correlation between changes in fatigue and sick leave
Fatigue was significantly improved (p < 0.001) after one year of natalizumab treatment with a reduction of FSMC total score from a mean corresponding to severe fatigue to a mean corresponding to moderate fatigue in both groups with and without sickness benefit at baseline (Table 2). In the subset of individuals with sickness benefit at baseline (n = 58), there was no significant correlation between improvement in fatigue measured as FSMC total score and reduction in sickness benefit (Figure 2(b)).
Correlation between treatment onset and change in sick leave and walking distance
In the subset of individuals with sickness benefit at baseline (n = 58), the regression analysis in the present study showed improvement of work ability predominantly in young individuals with natalizumab treatment (p = 0.001, R2 = 19%; Figure 3(a)). Regression analysis on the change in walking distance in relation to the start of natalizumab treatment also showed the same type of relationship with age (p < 0.001, R2 = 37%; Figure 3(b)).
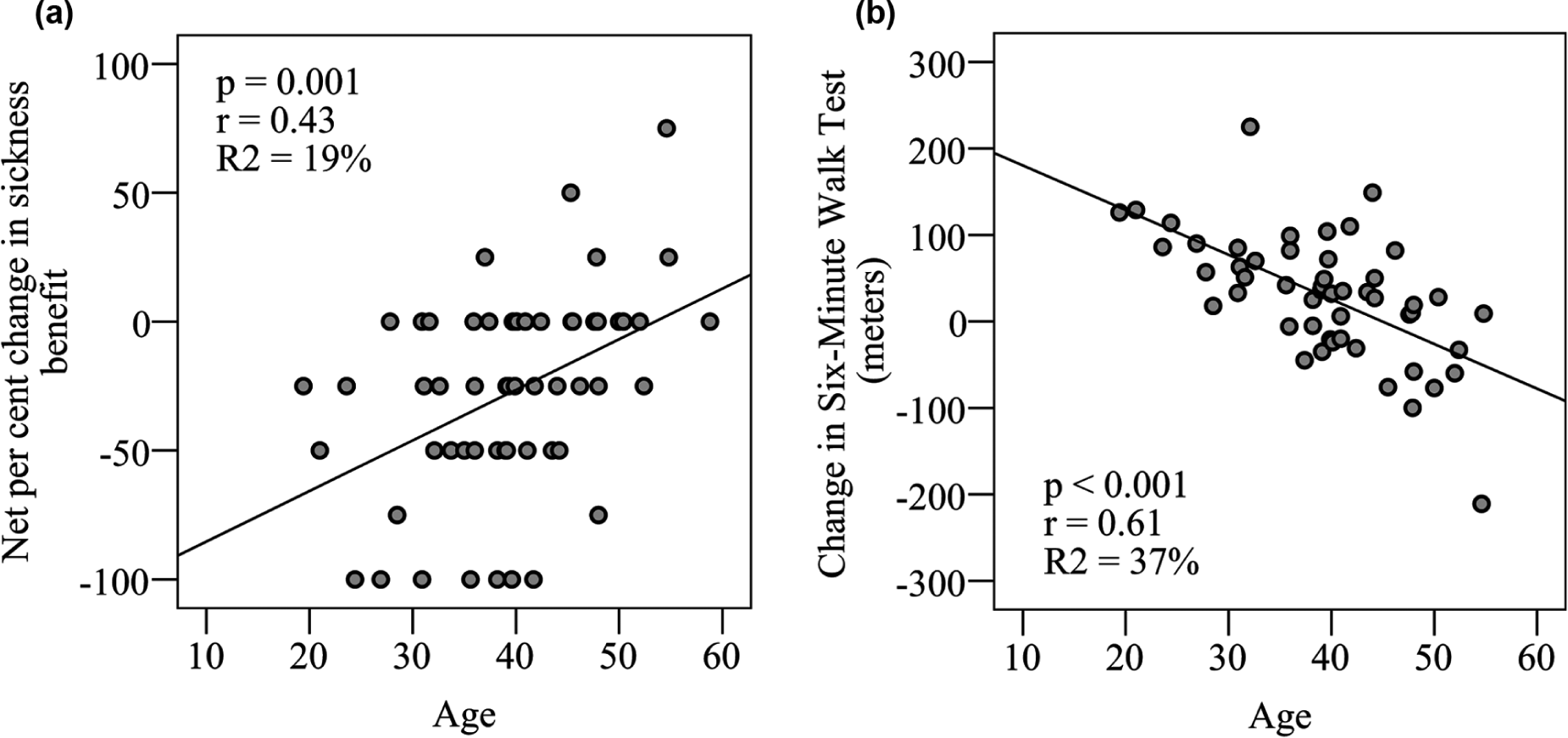
Regression analysis between age of onset of natalizumab treatment and change of sickness benefit as percentage of employment (a) and change in walking distance (b)*. Younger individuals tend to improve their work ability more than older individuals after one year of natalizumab treatment (a). Also, walking distance improves more for young individuals starting natalizumab therapy (b). Each point represents one patient.
Discussion
This study supports our previous observations that initiation of natalizumab treatment in RRMS may be associated with improved ability to work. Furthermore, this study was performed in a prospective design, eliminating the possible recall bias that could diminish the validity of our previous observations. 7 It is still not possible to draw any certain conclusions regarding causal relationships between the treatment intervention and the improved working ability since there was no control group without natalizumab treatment included in this study. Because of ethical reasons this would not have been possible and each patient thus had to serve as his or her own control. This opens a potential risk of improvement as a result of regression to the mean, which we cannot exclude to explain at least part of the findings in this study. However, we believe that the well-documented anti-inflammatory effect of natalizumab can serve as a plausible explanation for improvement of relevant symptoms that are important in the work situation, physically and mentally.
Mobility is an important factor in many different types of employment, and poor walking ability also results in a higher degree of physical fatigue during the work day that may inhibit the ability to cope with a high number of working hours. We have previously shown that walking distance as measured by the 6MWT improved significantly in the TYNERGY trial. 11 We could now document that the improvement in walking ability correlated with reduction in obtained sickness benefit. It has previously been shown that 6MWT correlates with community ambulation, which indicates relevance also for occupational activities. 15 We do not know for certain, however, to what extent our finding represents a causal relationship or just two coincidental phenomena related to a general improvement. We believe the observation is interesting and deserves further investigation.
Since the CWQ was used as a part of the TYNERGY study we could analyse possible relationships between fatigue and sick leave. Fatigue was pointed out as a factor related to decreased work ability in a recently published global survey. 5 In the present study improvement of fatigue measured with the FSMC scale did not correlate with the reduction in obtained sickness benefit. However, in our previous study using the fatigue item included in the CWQ, we found a significant correlation between improved work-related fatigue and improved work ability. 7 Although FSMC is regarded as the preferred scale to assess MS-related fatigue according to a recent systematic review, 16 it is possible that it is not optimally suited to analyse fatigue specifically related to the work situation. A reason for this may be that FSMC measures fatigue in a more general sense whereas the questions in the CWQ specifically assess fatigue related to the individual’s work situation.
One important finding in our previous retrospective study was that improvement in working ability was more pronounced in younger patients after starting treatment with natalizumab. 7 We therefore repeated this analysis with this prospectively collected data, which are thus not confounded by recall bias. We found the same age dependency in the present study with a more pronounced reduction in the sickness benefit level among younger compared with older individuals. One explanation for this finding may be that the inflammatory component in MS appears to be highest among young individuals17,18 and thus makes it plausible that a more potent inflammatory control may have a stronger effect on the overall well-being in this age group. We also performed a regression analysis between age at start of natalizumab treatment and the effect on walking ability and received the same result with a higher degree of improvement of mobility in younger individuals. Taken together, these results may indicate a greater economic gain for society from effective inflammatory control in young individuals with MS.
The predefined analysis of work ability in the TYNERGY trial did not come out as significant, which could appear as conflicting with the results in this post-hoc analysis. One reason for that may be that the statistical method used in the ITT analysis of the TYNERGY trial was inherently insensitive to analysing data of individuals with part-time employment or a part-time disability pension. In addition, the ITT population in the TYNERGY trial was not stratified in any way regarding baseline sickness benefit and therefore underestimated the possible changes in the interesting subgroup that had some degree of sickness benefit at baseline. When comparing baseline characteristics we could not see any systematic differences in disease-related parameters between the post-hoc population analysed in this study and the individuals that were excluded from the TYNERGY population. The only exception to this was EDSS that was significantly higher in the excluded group, which is easily explained by the fact that all individuals with a full-time disability pension were not part of the investigated post-hoc population according to the predefined criteria for this study. We therefore conclude that the exclusion of patients before enrolment in the present study was not a result of systematic bias that severely corrupts the obtained results.
The importance of occupational engagement is strongly anchored in the culture of the Western society. As such it also influences the quality of life and sense of well-being.6,19 Working ability is probably a robust measure of the compound physical, mental and social capacity of an individual and also unlikely contaminated by a large degree of placebo effect. Surprisingly few studies have been performed analysing the direct effects on work ability in conjunction with medical interventions. Besides being an important factor for the patients, such studies may provide valuable information for making sound health economic decisions. We would therefore encourage the pharmaceutical companies to capture this aspect when evaluating treatment effects in the pivotal phase three trials, where the most reliable results can be obtained. The experience we gained from including this parameter in the TYNERGY trial also taught us that any predefined analysis needs to be carefully considered to capture economically important information directly in the primary data analysis.
Footnotes
Conflicts of interest
Anders Svenningsson has received research support, travel grants and lecture honoraria from BiogenIdec AB, MerckSerono, BayerSchering A/G, Sanofi-Genzyme AB and Baxter AB. Anne Wickström has received research support and travel grants from BiogenIdec AB. Magnus Vrethem and Charlotte Dahle have received an unrestricted research grant from BiogenIdec AB and Novartis and lecture honoraria from Biogen Idec and MerckSerono.
Funding
This study was supported by grants from BiogenIdec Sweden AB, the Norrbacka Eugenia Stiftelse, AFA Insurance and the Swedish Association of Persons with Neurological Disabilities (NHR). Financial support was also provided through a regional agreement between Umeå University and the Västerbotten County Council on Cooperation in the Field of Medicine, Odontology and Health (ALF). The TYNERGY trial was a BiogenIdec-sponsored trial.