
Abstract

Neuromyelitis optica (NMO), also known as Devic’s disease, is a severe autoimmune inflammatory disorder of the central nervous system. NMO has long been considered as a subtype of multiple sclerosis but recent observations suggest that NMO is a different disease with humoral pathogenic mechanisms. 1 In this study we aimed to systematically analyze the epidemiology, clinical features and serology of NMO in a Caucasian population in Isfahan, Iran.
A population-based retrospective study was conducted on patients registered with diagnosis of NMO at the NMO clinic registry of Alzahra Hospital (as the only referral center for NMO patients in the province), during the time period between 5 April 2007 and 31 August 2013. Crude prevalence was calculated in living residents of the defined study region on 10 October 2013 who met the Wingerchuk diagnostic criteria for NMO. The 2010 annual population census conducted by the Iranian Central Bureau of Statistics was used as the denominator population representing the average population size of Isfahan province between 2007 and 2013.
A total of 95 patients fulfilled the NMO diagnostic criteria. The overall crude prevalence of NMO among the Caucasian population living in Isfahan province was 1.9 per 100,000 (95% confidence interval (CI): 1.6–2.3). Crude prevalence for females and males was 2.7 (95% CI: 2–3.3) and 1.2 (95% CI: 0.8–1.6) per 100,000 respectively. Initial brain MRI performed at first presentation of the disease did not fulfill multiple sclerosis (MS) diagnostic criteria for ‘Dissemination in Space’ in any of the patients; however, during the course of the disease white matter abnormalities were detected in 46 brain MRIs (40%). NMO-IgG was checked for all patients by the laboratory of Bioscientia, Ingelheim, Germany. The result was positive in 63 patients (66.3%) and negative in 32 patients (33.7%). Demographic and clinical features of patients are presented in Table 1.
Demographic and clinical features of patients.
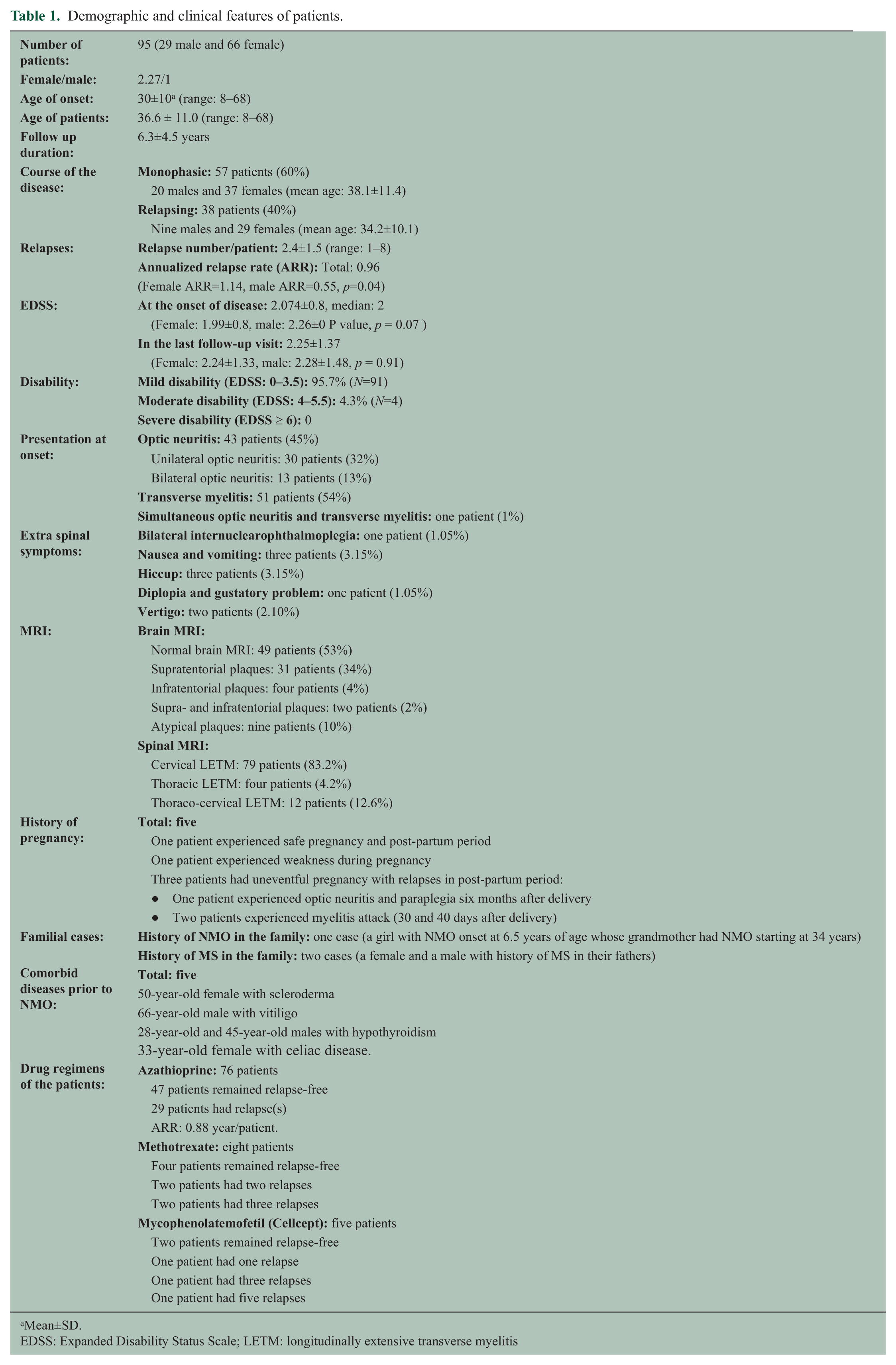
Mean±SD.
EDSS: Expanded Disability Status Scale; LETM: longitudinally extensive transverse myelitis
Reports about the prevalence of NMO in different ethnic groups suggest that the disease occurs more often in populations of African, East-Asian and Latin American descent than in other ethnic groups. 2,4,5 Results of our study (to our knowledge this is the largest case series from Western Asia) show a similar prevalence of NMO in Isfahan compared with other Caucasian populations; however, some differences existed in the clinical and demographic features of the disease in our cohort. The prevalence of NMO might be underestimated as probably many of the cases are never diagnosed and many others are misdiagnosed as MS. NMO cases in Isfahan are more likely to be monophasic and are less disabling when compared with other reported cohorts. 2 The impact of early treatment with immunosuppressive agents is not completely known, but current evidence suggests that the attack rate may be reduced by over 50% with effective immunosuppressive therapy. 3 It seems that Iranian NMO patients have a more benign course in comparison with those in Western countries. The reason for this difference is not known: earlier detection, earlier treatment with immunosuppressant agents, or differences in ethnic and geographic features might all be responsible. In our study, none of the brain MRIs met the criteria for MS at onset of the disease, although during the course of the disease white matter abnormalities were detected in 40% of brain MRIs. Hence, the first brain MRI seems more important for diagnosis of NMO since NMO patients can develop MS-like lesions in brain MRI over time. Further studies with longer follow-up will probably help confirm these findings and provide clues about the underlying reason for these differences.
Footnotes
Acknowledgements
This research is dedicated to NMO patients in Isfahan.
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.