
Abstract
Background:
There has been limited research on upper limb dysfunction in people with multiple sclerosis (PwMS).
Objective:
The objective of this paper is to study unilateral and bilateral upper limb dysfunction at different International Classification of Functioning (ICF) levels according to overall disability in PwMS.
Methods:
A total of 105 PwMS (16 with EDSS<4 (mild); 17 with EDSS 4–5.5 (moderate); 37 with EDSS 6–6.5 (severe); 35 with EDSS>6.5 (severe non-ambulant)) were recruited from two rehabilitation centers and assessed in a cross-sectional study.
Results:
The whole sample showed a diminished sensory function (median (first/third interquartile)) score of 3 (2/3) on the Monofilament Test and a reduced strength 91 (76/100) points on the Motricity Index (Body-Function level). Sensory dysfunction did not increase with higher EDSS while strength decreased from 100 (86/100) in the mild subgroups to 91 (80/100) points in the severe subgroup. All showed diminished dexterity, scoring 0.28 peg/s (0.17/0.35) on the Nine-Hole Peg Test (NHPT) (activity level). Score was better for the mild (0.38 (0.35/0.46)) peg/s compared to the severe subgroup (0.28 (0.17/0.35)). Sixty-eight percent, 44% and 75% of PwMS showed bilateral disorders in sensation, strength and dexterity, respectively. The Community Integration Questionnaire (participation level) showed a 35% reduction in home activities, even among PwMS with EDSS<4.
Conclusion:
This study showed uni-/bilateral upper limb abnormalities at all ICF levels increasing with the overall disability.
Introduction
Adequate upper limb function is essential for a person to interact within his or her environment. 1 Kister et al. 2 studied in people with multiple sclerosis (PwMS) self-reported symptom prevalence in 11 domains including upper limb function for years 0 to 30 from disease onset. For hand function they used a six-grade Likert scale; 0 (normal hand function), 1 (minimal hand disability), 2 (mild hand disability), 3 (moderate hand disability), 4 (severe hand disability), 5 (total hand disability). They showed that 8% of PwMS (N = 23,931) reported moderate (3) to total (5) hand dysfunction in the first year of the disease. Furthermore, worsening impairment was evident throughout the life span of 35% of PwMS reporting moderate (3) to total (5) impaired hand function after 30 years from the onset of the disease.
This self-reported upper limb dysfunction was confirmed by objective data reported in other studies on the characteristics of upper limb dysfunctions. 3 About 60%–75% of PwMS have impaired manual dexterity calculated as a percentage of individuals having a Nine-Hole Peg Test (NHPT) score higher than age-/sex-related norms + 1 SD. 4 Diminished dexterity is accompanied by impairments at body functions and structures levels.5–7 Some studies reported the presence of altered hand sensation, diminished arm strength 5 and tremor,8,9 while other studies found a decreased tactile sensibility, vibration and active range of motion in PwMS.10–12
Since most studies investigated primarily the presence of one or two particular impairments, it is unclear whether upper limb functional loss is associated with a single or multiple impairments. Further, it is not known whether they are already present in mildly affected individuals or present only when the overall disability is more pronounced and whether these impairments are presented unilaterally or bilaterally. Finally, the subjectively perceived impact of upper limb disorders on activities of daily living (ADL) is not well understood.
A thorough investigation of the upper limb dysfunction in MS and its underlying impairments is needed to advocate adequate treatment approaches. Insights can be gained through a comprehensive evaluation of the upper limb function using objective and subjective outcome measures at different levels of the International Classification of Functioning (ICF). Therefore, the aim of the study was to study upper limb dysfunction at different ICF levels according to overall disability and document bilateral upper limb dysfunction in PwMS.
Method
A total of 110 PwMS were screened at (REVAL – Rehabilitation Research Institute) in Belgium (n = 54) and at (Don Gnocchi Foundation) in Italy (n = 51). The two centers are specifically devoted to neurological rehabilitation in MS and are founded by local health care systems. The eligible population included all PwMS residing in the centers’ catchment areas requiring rehabilitation or follow-ups because of worsening of symptoms or check-ups. We recruited 105 people meeting the following inclusion criteria: having a confirmed MS diagnosis (by a physician or neurologist), age>18 years old, free from relapses or relapse-related treatments for one month before the study, and the ability to touch the chin at least with one hand. Individuals unable to follow test instructions (e.g. with cognitive impairment or language barrier) or having other diseases interfering with the execution of tests (e.g. depression or other psychiatric or orthopedic disorders) were excluded. All participants received information regarding the study and were included after signing the informed consent forms. The study was approved by the ethics committee of each participating center.
To verify whether upper limb impairments increase with overall disability, the sample was categorized into four disability groups according to the Expanded Disability Status Scale (EDSS): mild (1–3.5), moderate (4–5.5), severe ambulant (6–6.5) and severe non-ambulant (7–9.5).
Assessments used in the study
Using the ICF as a conceptual framework, the following assessments were administered for the right and left upper limb by a research therapist.
Body functions and structures level
Strength of the shoulder abductors, elbow flexors and pinch grip were measured by the Motricity Index (MI); 13 total score ranges from 0 (no muscle resistance) to 100 (normal strength).
A Jamar® hand-held dynamometer 14 was used to determine maximal isometric handgrip strength in three trials. Intentional tremor was assessed with Fahn’s Tremor Rating Scale (FTRS), 12 ranging from 0 (no impairment) to 4 (severe tremor).
Spasticity of shoulder adductors, elbow and wrist flexors were assessed with the Modified Ashworth Scale (MAS), 15 ranging from 0 (no spasticity) to 5 (severe spasticity).
The tactile sensitivity of the thumb was measured using the Semmes–Weinstein Monofilament Test (SWMT), 16 ranging from 1 (normal sensation) to 6 (loss of sensation).
Activity level
Manual dexterity was measured with the NHPT; 17 the mean pegs per second (pegs/sec) rate of two trials was considered. The Action Research Arm Test (ARAT) 18 was performed to rate an individual’s ability to grasp and lift objects of various sizes. It consists of 19 test items organized into Grasp, Grip, Pinch, and Gross Motor subsections. Maximum score is 57 indicating normal upper limb function. The Manual Ability Measure-36 (MAM-36) 19 was used to rate perceived manual ability on a scale ranging from 0 (impossible to complete any of activity cited) to 100 (every activity cited is accomplished without any difficulty).
Participation level
The Community Integration Questionnaire (CIQ) 20 was used to assess participation in home, social and productive activities; total score ranges from 0 to 29 representing from no to excellent community integration.
The following descriptive variables were collected from the sample (Table 1): gender; age; hand dominance determined by the Edinburgh Handedness Inventory (EHI); 21 disease duration; type of MS; EDSS determined by the neurologist; the Bohannon Standing Balance Test (BSBT): 22 upright balance ranging from 0 (unable to stand) to 6 (stand on one foot for 30 seconds); Hauser Ambulation Index (AI): 23 gait skills ranging from 0 (asymptomatic) to 9 (wheelchair bound).
Demographic and clinical characteristics of the sample.
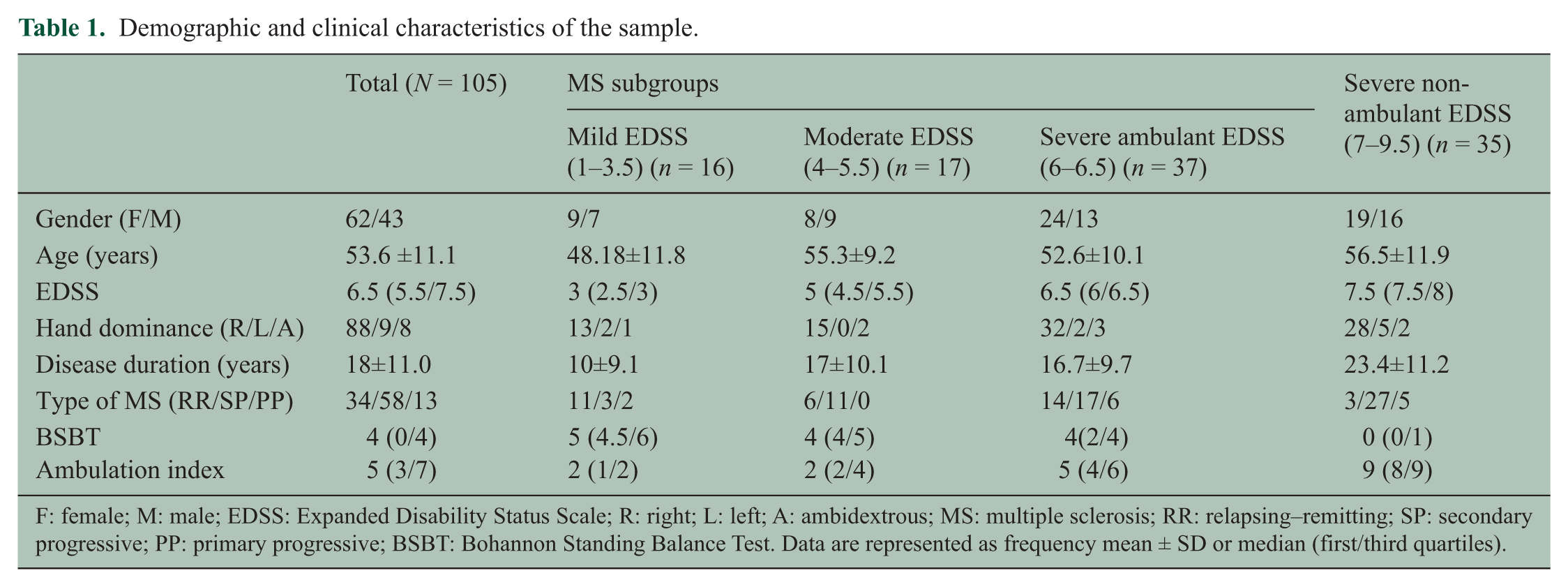
F: female; M: male; EDSS: Expanded Disability Status Scale; R: right; L: left; A: ambidextrous; MS: multiple sclerosis; RR: relapsing–remitting; SP: secondary progressive; PP: primary progressive; BSBT: Bohannon Standing Balance Test. Data are represented as frequency mean ± SD or median (first/third quartiles).
To ensure standardization between centers, an instruction booklet was used and two practice sessions in the two countries were held to minimize the differences between the two assessors. Data coming from these preliminary assessments were analyzed to verify if there were any statistically significant differences between the two centers.
Data analysis
In this exploratory, cross-sectional study, we reported results pertaining to the dominant upper limb according to the EHI. Since no statistically significant differences between centers were observed for the studied variables, no adjustments were made to correct for center.
Medians and first through third quartiles were used to describe the magnitude of upper limb disability in the whole sample and in the different EDSS subgroups. The Kruskal–Wallis Test (StatSoft 8.0) was used to assess statistically significant main effects (p ≤ 0.01) with post hoc test (corrected for multiple comparisons) to identify subgroups differences.
Percentages of unilateral and bilateral abnormal scores were used to describe upper limb disorders. For handgrip strength, Jamar and NHPT scores were considered abnormal according to normative values reported in the literature, corrected for age and gender ± 1 SD.24,25 For other ordinal scales any deviation from best score (see Table 2) was considered as abnormal.
Unilateral and bilateral involvement presented as percentages of abnormal scores in one (unilateral) or both upper limbs (bilateral) by Expanded Disability Status Scale subgroups.
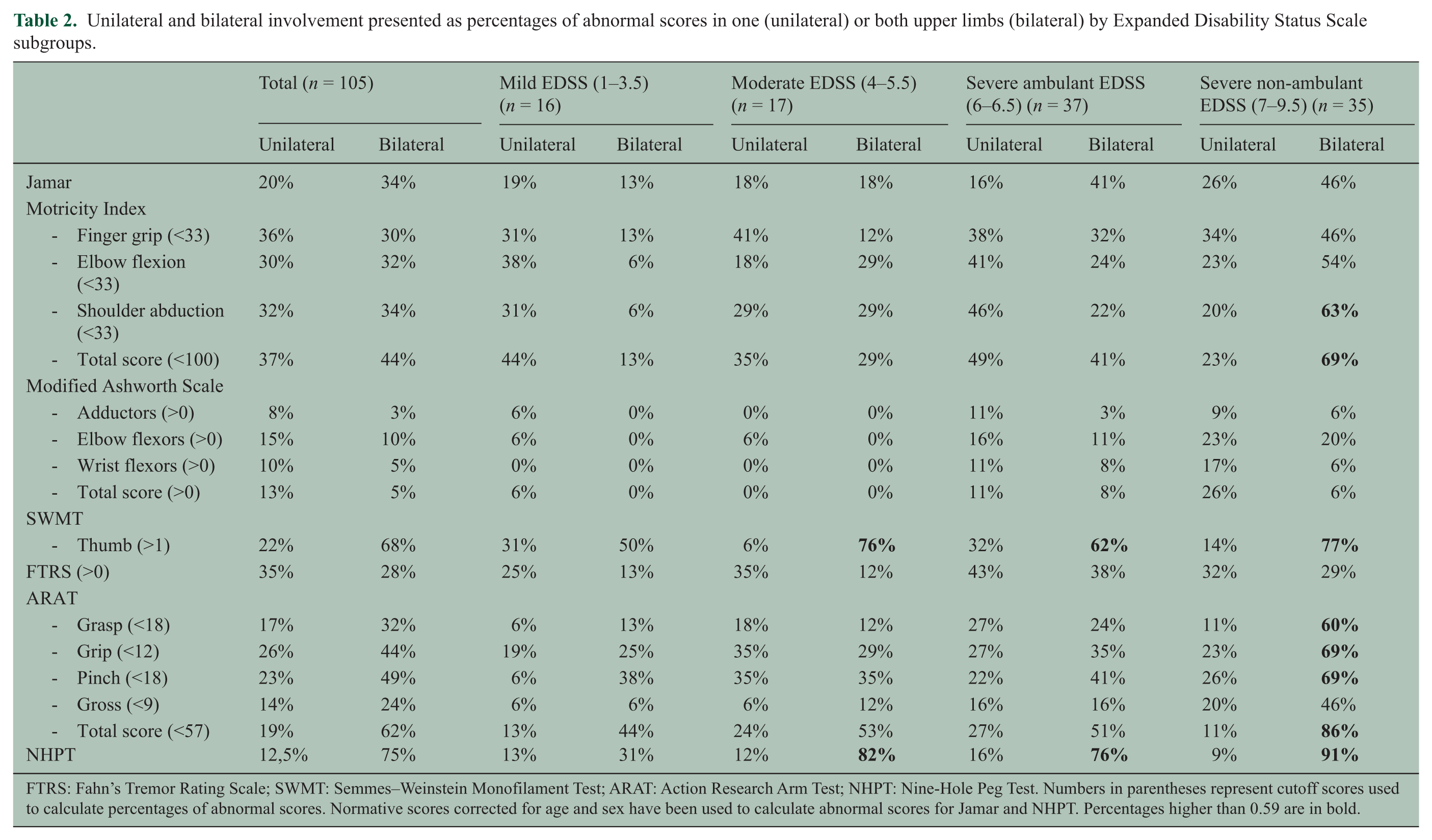
FTRS: Fahn’s Tremor Rating Scale; SWMT: Semmes–Weinstein Monofilament Test; ARAT: Action Research Arm Test; NHPT: Nine-Hole Peg Test. Numbers in parentheses represent cutoff scores used to calculate percentages of abnormal scores. Normative scores corrected for age and sex have been used to calculate abnormal scores for Jamar and NHPT. Percentages higher than 0.59 are in bold.
The CIQ subscales are reported in Figure 1 as normalized “percentage scores,” i.e. (individual’s score/maximum test score)*100, resulting in values ranging from 0 to 100.
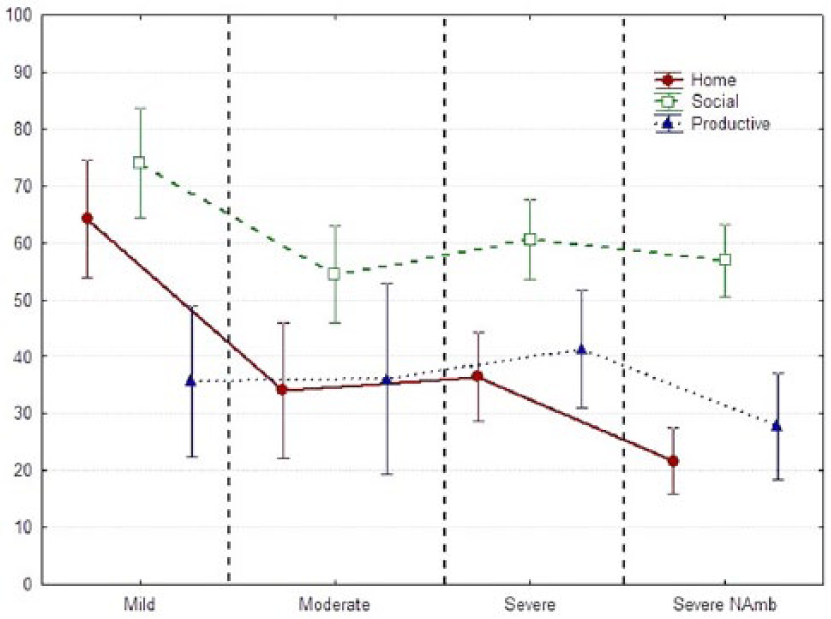
Mean (and 95% confidence intervals of mean) for Home Integration, Social Integration and Productive Activities of the Community Integration Questionnaire.
Results
Table 3 displays the median scores for each clinical variable for the whole sample and the four subgroups. On body functions and structures level, PwMS showed increased intentional tremor and impaired tactile sensitivity in the thumb with a score of 3 on the SWMT that did not change across subgroups (Table 3). Muscle weakness assessed by MI showed lower values with respect to maximum test score in the whole sample. Furthermore, MI score showed a sharp decrement in the severe non-ambulant subgroup. On activity level PwMS showed a decreased rate of peg per second (Table 3) with respect to cutoff value (around 0.5 peg/s) that was suggested to detect limitation on activity and participation level. 7 Furthermore, 38% of mildly impaired participants had abnormal NHPT scores (Table S1 in the supplementary material); furthermore, a decrease from 0.38 to 0.17 peg/s (p < 0.001) was observed in the severe non-ambulant group, of whom 97% of PwMS had impaired manual dexterity (Table S1).
Median scores (first/third quartiles) of clinical variables and p values comparing the four subgroups.
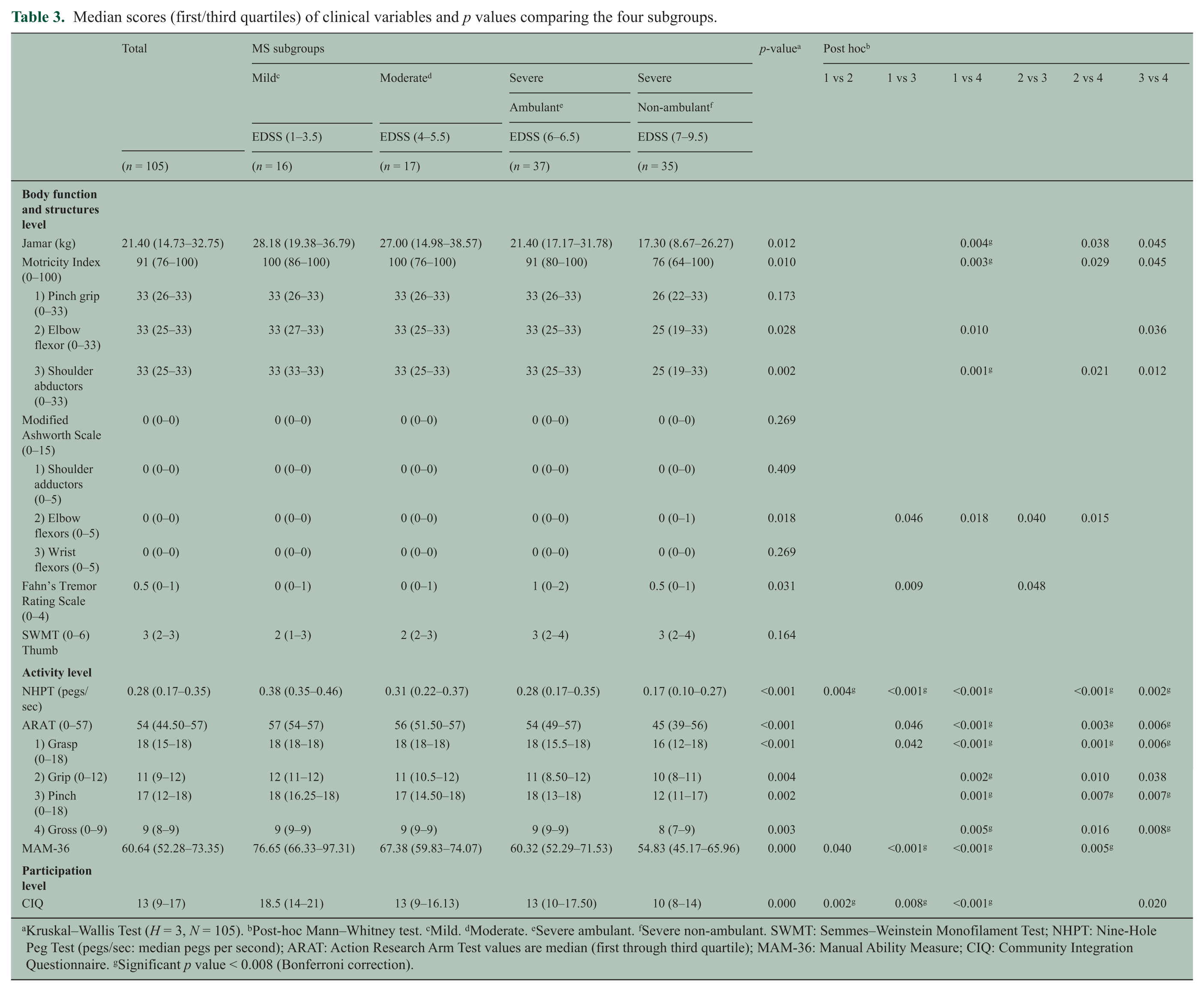
Kruskal–Wallis Test (H = 3, N = 105). bPost-hoc Mann–Whitney test. cMild. dModerate. eSevere ambulant. fSevere non-ambulant. SWMT: Semmes–Weinstein Monofilament Test; NHPT: Nine-Hole Peg Test (pegs/sec: median pegs per second); ARAT: Action Research Arm Test values are median (first through third quartile); MAM-36: Manual Ability Measure; CIQ: Community Integration Questionnaire. gSignificant p value < 0.008 (Bonferroni correction).
Bilateral involvement was highly frequent as shown in Table 2, which displays percentages of PwMS who had abnormal test scores in either one (unilateral involvement) or both (bilateral involvement) limbs. Percentages of abnormal scores were high in the severe non-ambulant group showing 91% of bilateral involvement measured by the NHPT. Normal and abnormal (unilateral and bilateral) scores are also presented in the supplementary material (Figure S1).
Further, Figure S2 (available in the supplementary material) reports percentages of participants having one or more abnormal performances in each subgroup.
Data regarding participation are depicted in Figure 1 showing the normalized CIQ percentage scores of the four subgroups. This figure illustrates the impact of MS on individuals’ home, social and productive activities.
Discussion
The aims of the present study were to document upper limb dysfunction and report unilateral and bilateral upper limb involvement on the ICF domains in PwMS with different disability levels. The results showed a wide variety of upper limb disorders at all ICF levels. At the body functions and structures level, PwMS showed impaired tactile sensitivity and reduced muscle strength. At the activity level, PwMS showed limitations in manipulating small objects even in the group with EDSS scores below 4, while PwMS with EDSS>6.5 showed limitation also in gross movements and muscle strength. Remarkably, individuals with EDSS>5.5 often had concomitant presence of disabilities in both upper limbs concerning strength (41%) and sensibility (62%) at the body functions and structures level and manual dexterity (76%) at the functional level.
PwMS showed abnormal performances at the body functions and structures level. Muscle weakness was present in all groups; MI was below the normal score for the whole group and significantly decreased in the severe subgroups compared to the mild subgroup (p < 0.01). Similar results were seen for the Jamar test especially in the severe non-ambulant group with almost a 10 kg reduction of handgrip strength (p < 0.001) compared with the mild group. This is in keeping with the results of other studies, which reported a similar level of strength impairments leading to difficulties in manipulating objects 26 and increased perception of manual impairment. 6 Furthermore, the vast majority of PwMS included in the current study had impaired sensory function and/or tremor. Sensory impairments were already present in the mild group with a median score of 3 on the SWMT indicating diminished protective sensation. In contrast to the other motor impairments, sensory impairment did not increase in the subgroups with a higher level of disability. This result, in agreement with those reported by Kister, 2 Guclu-Gunduz 5 and Sanders and Arts, 27 provides evidence of early involvement of somatosensory pathways connecting the spinal cord to upper integrative centers in PwMS. Intention tremor was present in more than 30% of the individuals having EDSS scores lower than 4, which is similar to the results reported by Alusi et al. 28 However, it is important to note that median level of tremor was around 1 on a five-point scale suggesting only mild involvement, even in the two severely affected groups. This low value could be in part due to difficulties in rating kinetic tremor due to complex ataxic movements in PwMS. Additional quantitative and ecologically designed analyses of tremor in the upper limb seem necessary to better appreciate the impact of tremor on daily activities requiring manipulation of small objects such as forks and pencils.
At the activity level, impaired manual dexterity was present in PwMS. The median score for the NHPT was 0.28 peg/s for the whole group with a sharp and statistically significant decrement (p < 0.01) in the severe non-ambulant group, compared to the mild group. Loss of manual dexterity has been shown to be associated with decreased independence in ADL 6 , 7 , 10 and is probably due to a combination of tremor, sensory and strength impairments 6 in distal segments for mildly and moderately affected individuals. Noteworthy is the fact that in severely affected individuals a perusal analysis of ARAT subtests revealed that gross movements seemed to be affected by a reduction of shoulder abductors strength. This is an important limitation probably associated with impaired mobility in wheelchair users.
The results of the MAM-36, questioning the difficulty of performing ADL independent of which arm is being used, indicated that lower than maximal scores are already present in the group of mild PwMS. As such, the MAM-36 seems to be sensitive to subtle changes not always detected with standard clinical tests performed unilaterally.
Interestingly, there is also a significant main effect of group with differences in the MAM-36 scores existing among subgroups with larger gaps (e.g. groups 1 vs. 3; see Table 3).
With respect to participation or community integration, the CIQ showed a 35% reduction in participation during home activities even in the mild group; this figure further increased to 78% in the severe non-ambulant group. This implies that the vast majority of home activities are carried out by caregivers increasing the burden on the family. Compared to home integration, social participation appears less involved with a more marked decrease between the mild and moderate groups. Further studies are warranted to understand the association between upper limb disorders with participation restriction.
Bimanual tasks such as changing clothes, performing toileting activities and washing the hands are part of everyday basic ADL requiring integrity of both arms. This is the first study documenting the high proportion of bilateral disorders in this pathology. Bilateral sensory disorders were present in more than two-thirds of the whole sample, and even half of PwMS with EDSS<4 had sensory impairments. Muscle weakness (MI) was bilaterally present in 13% of PwMS with an EDSS score<4 and steadily increased to 69% in individuals with EDSS>6.5. Similar results were obtained for manual dexterity with percentages of bilateral involvement increasing from about one-third of PwMS with EDSS<4 to almost all PwMS with EDSS>6.5. Bilateral disorders in sensation, strength and manual dexterity reduce the possibility of coping with the malfunctioning of one upper limb with the other and increases overall disability since it has been demonstrated that bimanual activities are performed more frequently in daily life than unimanual activities. 29 Note, however, that our results are influenced by the high frequency of severely involved patients having a higher level of bilateral upper limb involvement.
The present study has some limitations. First, the recruitment of participants attending rehabilitation centers probably led to an overrepresentation of problems in dexterity in all EDDS groups; moreover, sample size was small in the first two subgroups. Secondly, a more ecological and quantitative assessment of body functions and structures is needed to objectively measure tremor, trunk and proximal segments strength, force control, motor fatigue and sensory function other than tactile cues. Thirdly, visual impairment possibly affecting manual dexterity and function was not assessed.
Finally, the applied cutoff values are from a number of different studies in various populations, which can affect the result and interpretation; the inclusion of a normative sample matched for demographical characteristics may have reduced bias.
Footnotes
Acknowledgements
The authors thank the participants of this study as well as Veronik Truyens, Greet Adriaenssens, and Angelo Montesano, heads of department of the Rehabilitation and MS Center Overpelt, De MICK Rehabilitation Center Brasschaat, and Larice Lab, Don Gnocchi Foundation, respectively, for facilitation of the study. The authors highly acknowledge the physical therapists and occupational therapists: Letizia Spina, Lore Kerkhofs, and Joke Raats as well as student Nick Maesen for assistance with data collection.
Conflicts of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.