
Abstract
Background:
MS-Line! was created to provide an effective treatment for cognitive impairment in multiple sclerosis (MS) patients.
Objective:
To assess the efficacy of MS-Line!.
Methods:
A randomized, controlled, single-blind, 6-month pilot study. Patients were randomly assigned to an experimental group (cognitive rehabilitation with the programme) or to a control group (no cognitive rehabilitation). Randomization was stratified by cognitive impairment level. Cognitive assessment included: selective reminding test, 10/36 spatial recall test (10/36 SPART), symbol digit modalities test, paced auditory serial addition test, word list generation (WLG), FAS test, subtests of WAIS-III, Boston naming test (BNT), and trail making test (TMT).
Results:
Forty-three patients (22 in the experimental group, 21 in the control group) were analyzed. Covariance analysis showed significant differences in 10/36 SPART (P=0.0002), 10/36 SPART delayed recall (P=0.0021), WLG (P=0.0123), LNS (P=0.0413), BNT (P=0.0007) and TMT-A (P=0.010) scores between groups.
Conclusions:
The study showed a significant improvement related to learning and visual memory, executive functions, attention and information processing speed, and naming ability in those patients who received cognitive rehabilitation. The results suggest that MS-Line! is effective in improving cognitive impairment in MS patients.
Keywords
Introduction
Multiple sclerosis (MS) is a demyelinating disease of the central nervous system, and the second most common cause of neurological disability among young adults. 1 Cognitive impairment is a major symptom of MS that has a negative impact on patients’ quality of life, and occurs independently of the degree of physical disability.2,3
The prevalence of cognitive impairment in MS patients has been estimated at between 43% and 65%.4,5 While cognitive impairment may appear early in the disease course and tends to progress over time, 6 it is generally hidden by physical manifestations of the disease. The most common cognitive symptoms include deficits in information processing speed, memory and executive functioning.
The long gap in time between the initial diagnosis of MS and the treatment of the associated cognitive disorders, and the fact that current MS therapies for cognitive functions have not yielded positive results, shows the need to identify new approaches for the treatment and prevention of cognitive impairment. 7
MS-Line! is a cognitive rehabilitation programme designed for home use that provides an effective and freely accessible treatment for cognitive impairment, especially at the onset of the disease in the years between the initial diagnosis and the start of hospital-based neurorehabilitation.
The primary objective of the present study was to assess the efficacy of MS-Line! in MS patients. Our hypothesis was that the application of a cognitive rehabilitation programme specifically designed for cognitive impairment in MS based on the restoration of function would be an effective strategy for the improvement of cognitive function in MS patients.
Patients and methods
We performed a randomized, controlled, single-blind, 6-month pilot study conducted in the MS unit at the Dr Josep Trueta University Hospital (Spain). Two-hundred patients were randomly chosen from the database of the hospital’s MS unit using a random numbers table. All patients were sent an information sheet describing the MS-Line! project by post, together with a request to attend a briefing. Sixty-two patients attended the briefing. At the end of the meeting, patients were given an application form to participate in the MS-Line! project, and 46 patients gave their signed informed consent. The study was conducted in accordance with the principles of the Declaration of Helsinki and good clinical practice standards and was approved by the hosptial’s ethics committee.
Eligible patients were aged 20–60 years and had clinically defined MS according to the Poser criteria. 8 Patients were required to have had at least a primary education (8 years) and mild cognitive impairment as determined by the neuropsychological assessment as inclusion criteria. Severe psychiatric disorders, a history of traumatic brain injury, having taken steroids or immunosuppressor medications during the previous month, and having received other cognitive rehabilitation treatment during the previous 6 months, were exclusion criteria.
The level of cognitive impairment was assessed with the brief repeatable battery of neuropsychological tests in MS (BRB-N), 9 consisting of five tests: the selective reminding test (SRT) (which included long-term storage (SRT-LTS), consistent long-term retrieval (SRT-CLTR) and delayed recall (SRT-DR)), the 10/36 spatial recall test (10/36 SPART) (total correct responses (10/36 SPART-T) and delayed recall (10/36 SPART-DR)), the symbol digit modalities test (SDMT), the paced auditory serial addition test (PASAT) and word list generation (WLG) test. We also added the phonemic fluency (FAS) test, 10 the backward and forward digit span, block design, and letter-number sequencing (LNS) subtests of the Wechsler adult intelligence scale III (WAIS-III), 11 the Boston naming test (BNT), 12 and the trail making tests A and B (TMT-A and TMT-B). 13 Normative values were adopted in accordance with values reported by Sepulcre et al. 14 (BRB-N), Troyer 15 (FAS test), Wechsler 11 (WAIS-III), Quiñones-Ubeda et al. 16 (BNT) and Tamayo et al. 17 (TMT).
The main dependent variables were SRT-DR, 10/36 SPART-DR and the LNS as they evaluate memory and executive functions, which are the most commonly important cognitive deficits in patients with MS.
Two sequential steps were used to classify patients by the level of cognitive impairment: for each of the tests, scores were considered to be impaired if they were 1.5 SD or more below the mean of normative data; cognitive impairment was defined as: mild, between one and three impaired cognitive tests; moderate, four to seven impaired tests; and severe, eight or more impaired tests.
The percentage of patients with score improvement/no change (given that MS is a neurodegenerative disease, no change can be considered a positive outcome from a clinical viewpoint) versus worsening was calculated for each cognitive test. The following seven cognitive tests were grouped as memory tests (learning and working memory): total SRT, SRT-LTS, SRT-CLTR, SRT-DR, 10/36 SPART-T, 10/36 SPART-DR and the LNS. Subsequently, the percentage of patients with no improvement or improvement in one to two tests, improvement in three to five tests, and improvement in six or seven tests was calculated.
Participants were randomly assigned to one of the two arms in a 1:1 ratio. The randomization was stratified to avoid possible confounding variables, using the level of cognitive impairment as strata. Patients in the experimental group received two 75-minute sessions per week of cognitive rehabilitation with MS-Line! for a 6-month period. Cognitive rehabilitation sessions were performed at the Dr Josep Trueta University Hospital. Each session combined 25 minutes of written, manipulative and computer-based materials. Furthermore, patients and family members had to do a short daily cognitive exercise together at home lasting no more than 5 minutes (chosen from Soma 4, five-piece Tangram, Space Shuttle and Peg-Solitaire Hoppers).
Patients in the control group received no treatment. Investigators who performed the post-treatment cognitive assessments remained blind to the group allocation of the patients.
Written (e.g. mathematical problems, crosswords and word search puzzles), manipulative (e.g. spatial games with blocks, origami) and computer-based (e.g. logic and reasoning games, working memory games) materials included in MS-Line! were designed and developed by a multidisciplinary team consisting of software engineers, mathematicians, psychologists and linguists. All materials had different levels of difficulty, and clues to resolve the problems were provided.
Patients were considered to have adhered to MS-Line! if they had attended at least 80% of the hospital sessions and completed at least 80% of the daily exercises.
Adhesion registers were filled in by the clinicians at the hospital and family members at home.
Neurological impairment was assessed by means of the Expanded Disability Status Scale (EDSS). 18 Patients were asked to complete the hospital and anxiety depression scale (HADS),19,20 EuroQol-5D including the visual analogue scale (VAS), 21 and the multiple sclerosis impact scale (MSIS-29). 22
Statistical analysis
For each primary and secondary outcome, we computed an analysis of covariance (ANCOVA) model including the group (control versus experimental) as a fixed factor, adjusting for baseline scores of each outcome variable (covariate). We used the term ‘intergroup ANCOVA’ to evaluate treatment effects at 6 months, measured as the change from the baseline score. The term ‘intragroup ANCOVA’ refers to the evaluation of the change in the score between the baseline and the 6-month test for each treatment group independently using the MIXED procedure of the SAS system to estimate the intergroup and intragroup ANCOVA component. Comparisons of categorical data were made according to the χ2 or Fisher’s exact tests. The significance level adopted was 0.05 bilateral. Statistical analysis was performed using the SAS statistical package for Windows (version 9.1.3, SAS Institute Inc., Cary, NC, USA).
Results
Patient characteristics
Of the 46 patients who voluntarily agreed to participate in the study, two were excluded as they were already receiving cognitive rehabilitation at another centre and the third was excluded due to having changed his place of residence.
A total of 43 randomly assigned patients, 22 in the experimental group and 21 in the control group, were included in the analysis (Figure 1). During the 6-month treatment, one patient from each group withdrew (one due to a traumatic brain injury and the other due to family troubles). None were excluded due to non-compliance (Figure 1).
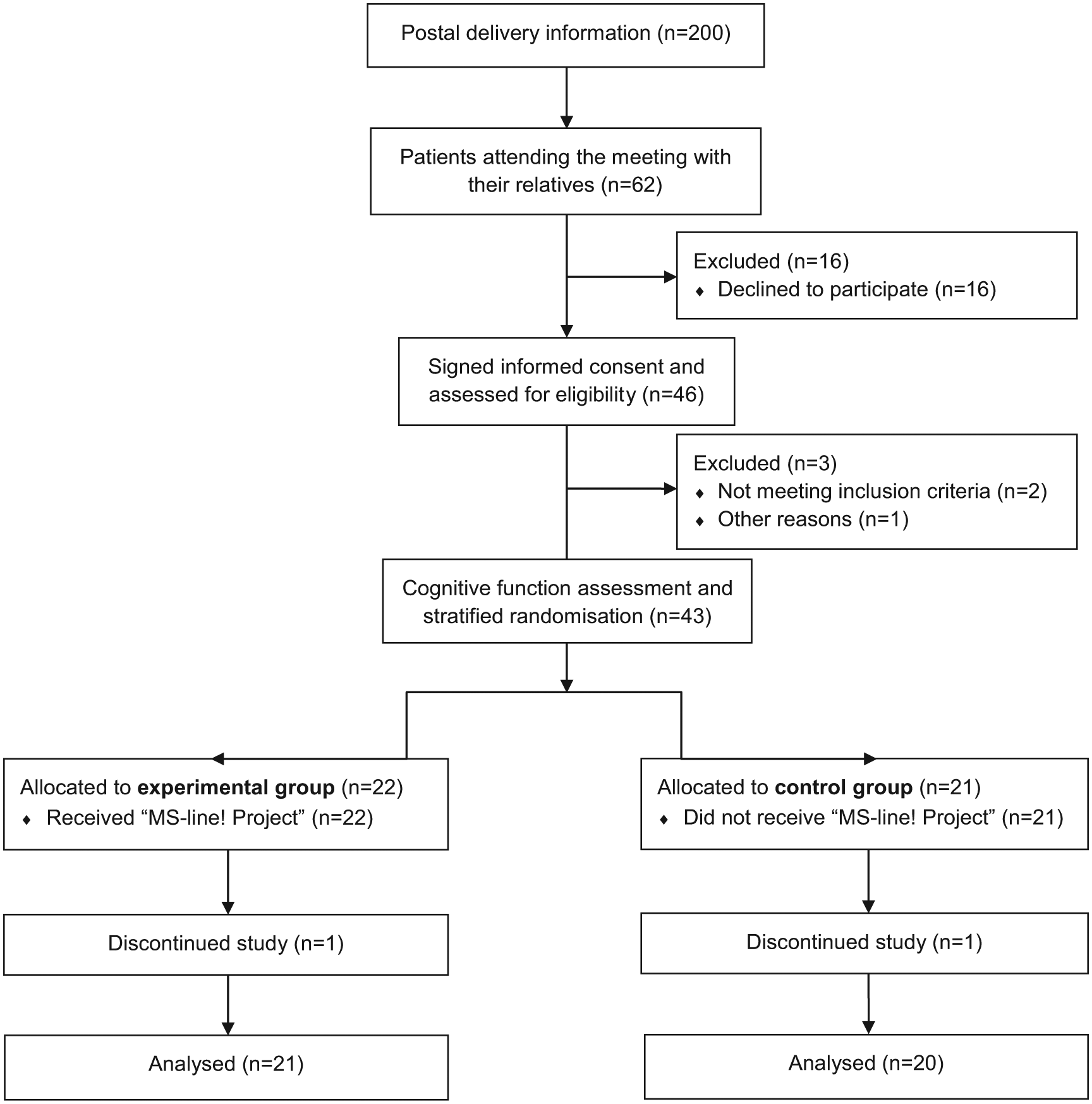
Flow chart of patients.
The demographic and baseline clinical data of the MS patients are summarized by group in Table 1. There were no significant differences in baseline characteristics between the two groups.
Baseline demographics and clinical characteristics of patients.
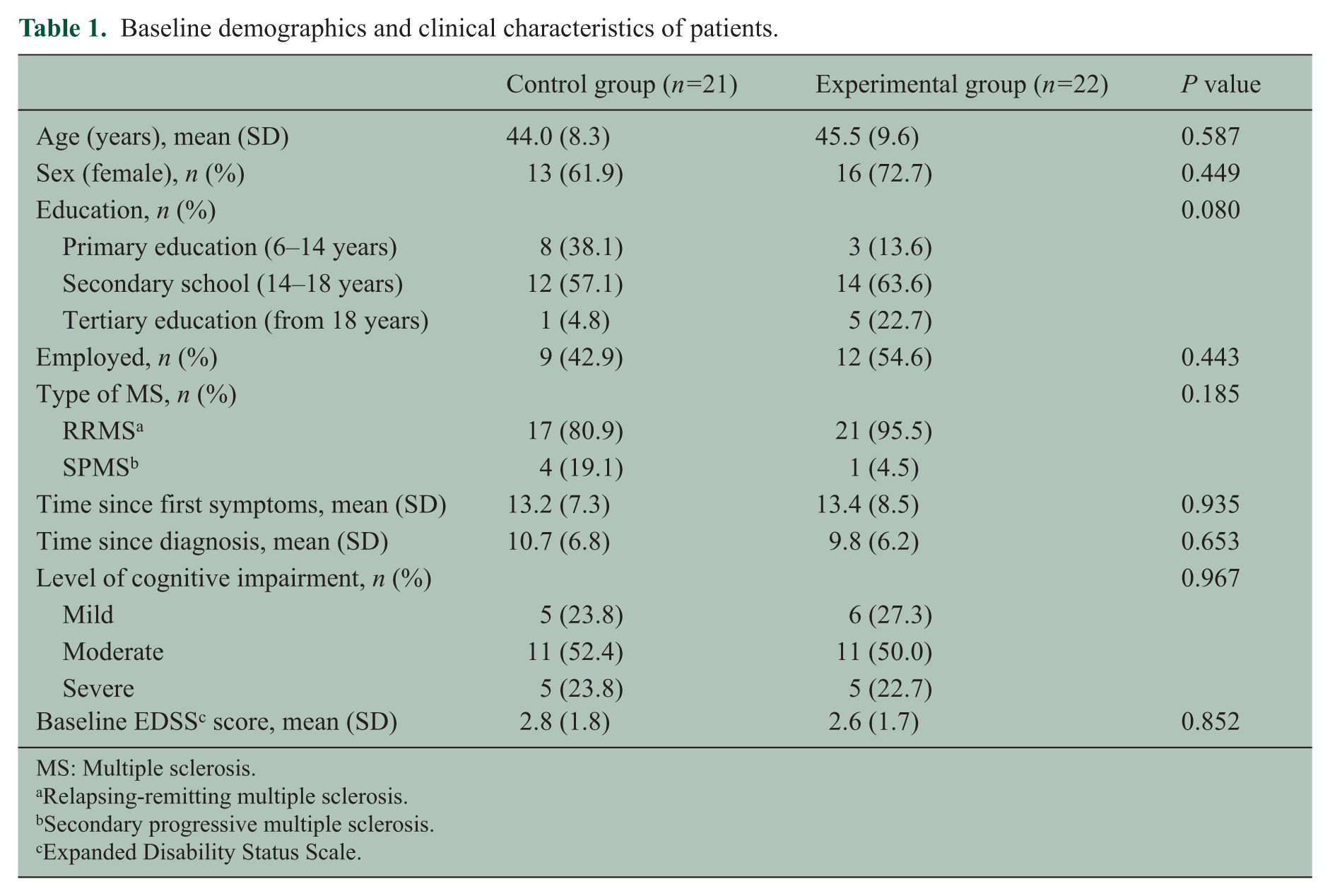
MS: Multiple sclerosis.
Relapsing-remitting multiple sclerosis.
Secondary progressive multiple sclerosis.
Expanded Disability Status Scale.
A total of 28 patients (65.1%) were treated with disease-modifying drugs at baseline without differences between the experimental and control groups. Treated patients were equally distributed by the level of cognitive impairment between the two groups (Table 2). During the study period two patients changed immunomodulating treatment: one patient changed from interferon (INF)β-1b to subcutaneous INFβ-1a due to poor tolerance, and one patient in the control group treated with subcutaneous INFβ-1a changed to natalizumab after presenting with two relapses during the study period. During the 6-month study period, two patients in the experimental group began treatment with disease-modifying drugs.
Pharmacological treatment at baseline.

Interferon.
Subcutaneous.
Intramuscular.
Cognitive function
As shown in Table 3, intergroup ANCOVA revealed significant differences in 10/36 SPART-T (P=0.0002), 10/36 SPART-DR (P=0.0021), WLG test (P=0.0123), LNS (P=0.0413), BNT (P=0.0007) and TMT-A (P=0.010) scores between the experimental and control groups.
Adjusted mean differences between the cognitive test scores of the experimental and the control group (intergroup analysis of covariance). Significant differences are marked in bold.
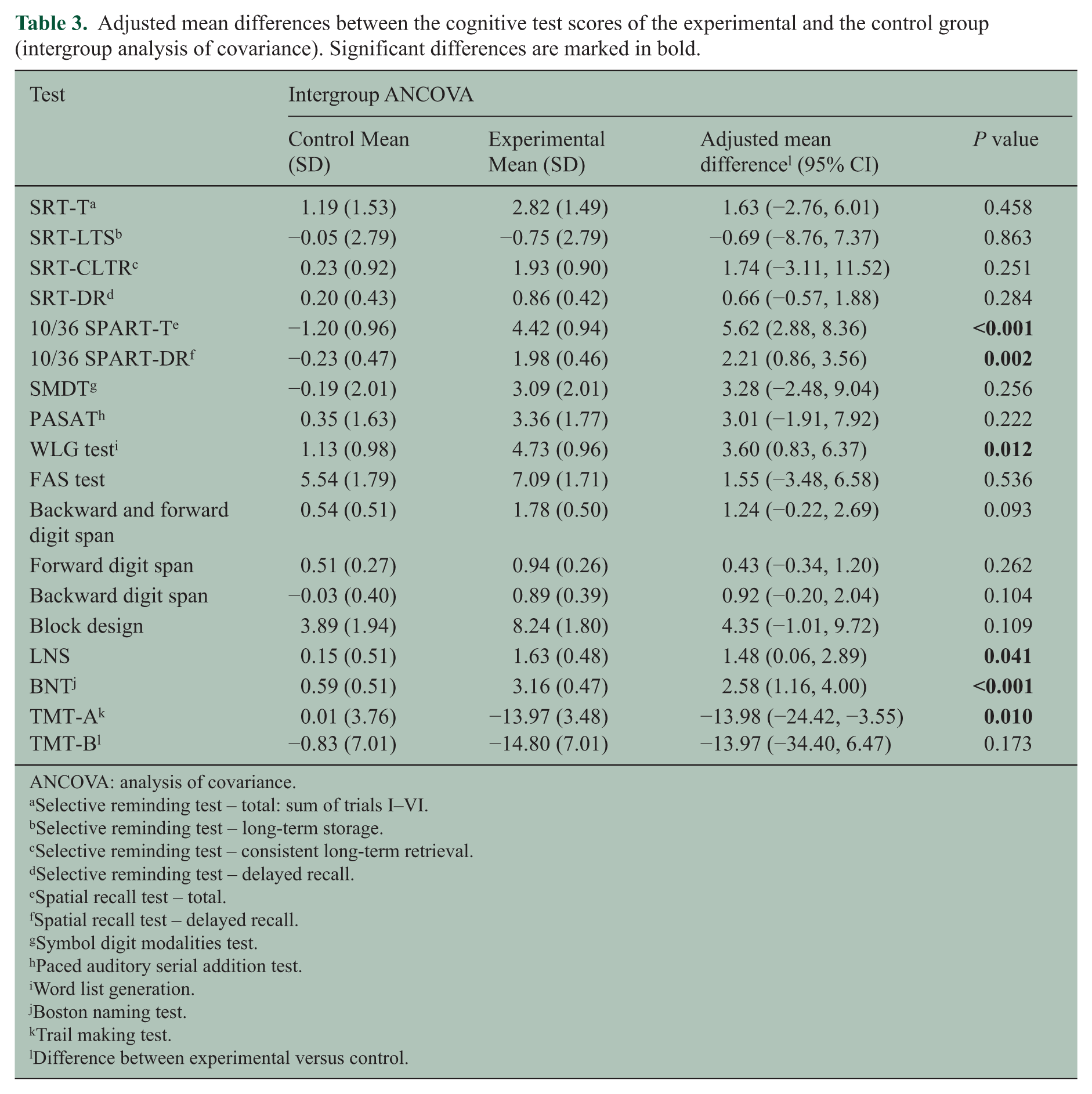
ANCOVA: analysis of covariance.
Selective reminding test – total: sum of trials I–VI.
Selective reminding test – long-term storage.
Selective reminding test – consistent long-term retrieval.
Selective reminding test – delayed recall.
Spatial recall test – total.
Spatial recall test – delayed recall.
Symbol digit modalities test.
Paced auditory serial addition test.
Word list generation.
Boston naming test.
Trail making test.
Difference between experimental versus control.
Similarly, significant differences were found between groups for the percentage of patients with score improvement/no change versus worsening in 10/36 SPART-T (P=0.0068), 10/36 SPART-DR (P=0.0268), WLG test (P=0.0452), BNT (P=0.0157) and TMT-A (P=0.0122) (see Table 5).
Intragroup ANCOVA (Table 4) showed significant final versus baseline differences in the experimental group in SRT-DR (P=0.0491), 10/36 SPART-T (P<0.0001), 10/36 SPART-DR (P=0.0001), WLG test (P<0.0001), FAS test (P=0.0002), digit span (total (P=0.0010), backward (P=0.0268) and forward digit span (P=0.0010), block design (P<0.0001) and LNS (P=0.0017) subtests of the WAIS-III, BNT (P<0.0001), 13 TMT-A (P=0.0003) and TMT-B (P=0.0437) scores. In the control group, significant differences were only found in FAS test scores (P=0.0038).
Adjusted mean differences between the cognitive test scores of the experimental and the control group (intragroup analysis of covariance). Significant differences are marked in bold.
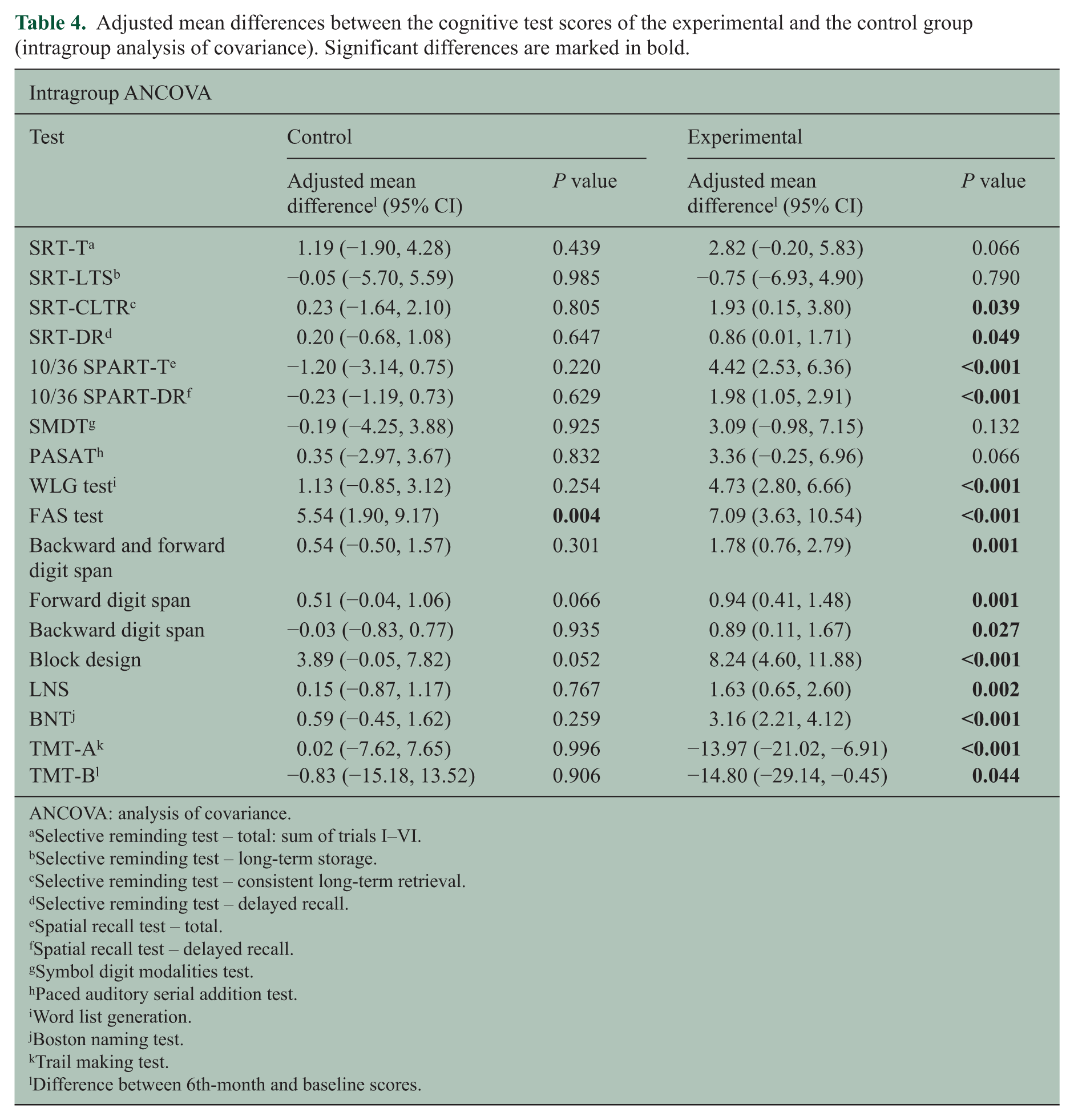
ANCOVA: analysis of covariance.
Selective reminding test – total: sum of trials I–VI.
Selective reminding test – long-term storage.
Selective reminding test – consistent long-term retrieval.
Selective reminding test – delayed recall.
Spatial recall test – total.
Spatial recall test – delayed recall.
Symbol digit modalities test.
Paced auditory serial addition test.
Word list generation.
Boston naming test.
Trail making test.
Difference between 6th-month and baseline scores.
Patients with cognitive test score improvement/no change or worsening. Significant differences are marked in bold.
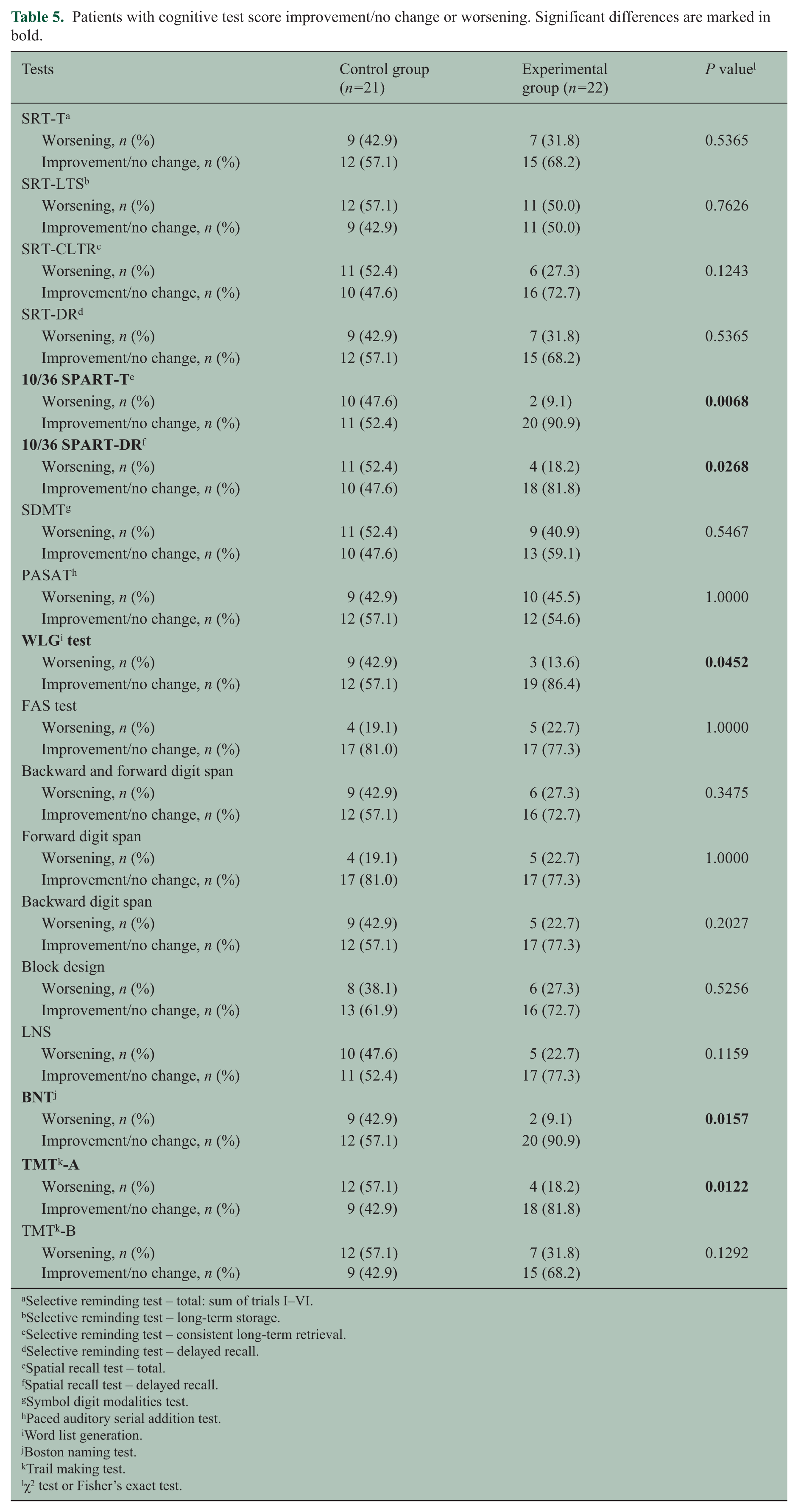
Selective reminding test – total: sum of trials I–VI.
Selective reminding test – long-term storage.
Selective reminding test – consistent long-term retrieval.
Selective reminding test – delayed recall.
Spatial recall test – total.
Spatial recall test – delayed recall.
Symbol digit modalities test.
Paced auditory serial addition test.
Word list generation.
Boston naming test.
Trail making test.
χ2 test or Fisher’s exact test.
The percentage of patients with improvement in six or seven memory tests was 57.1% in the experimental group versus 25.0% of patients in the control group (P=0.0155). Moreover, all patients included in the experimental group improved in at least three memory tests (Table 6).
Patients with improvement in memory tests.

Anxiety and depression
Intergroup covariance analysis revealed significant differences in total HADS scores between the experimental and the control group (adjusted mean difference: –3.321 (−6.368, −0.274); P=0.0335) (Tables 7 and 8). A trend towards significance was observed for both anxiety and depression subscales of HADS. In addition, intragroup ANCOVA showed significant final versus baseline differences in the experimental group either in the total HADS (P=0.0027) or in the anxiety subscale (P=0.0010) scores.
Adjusted mean differences between the experimental and the control groups’ HADS scores (ANCOVA). Statistically significant differences are marked in bold.
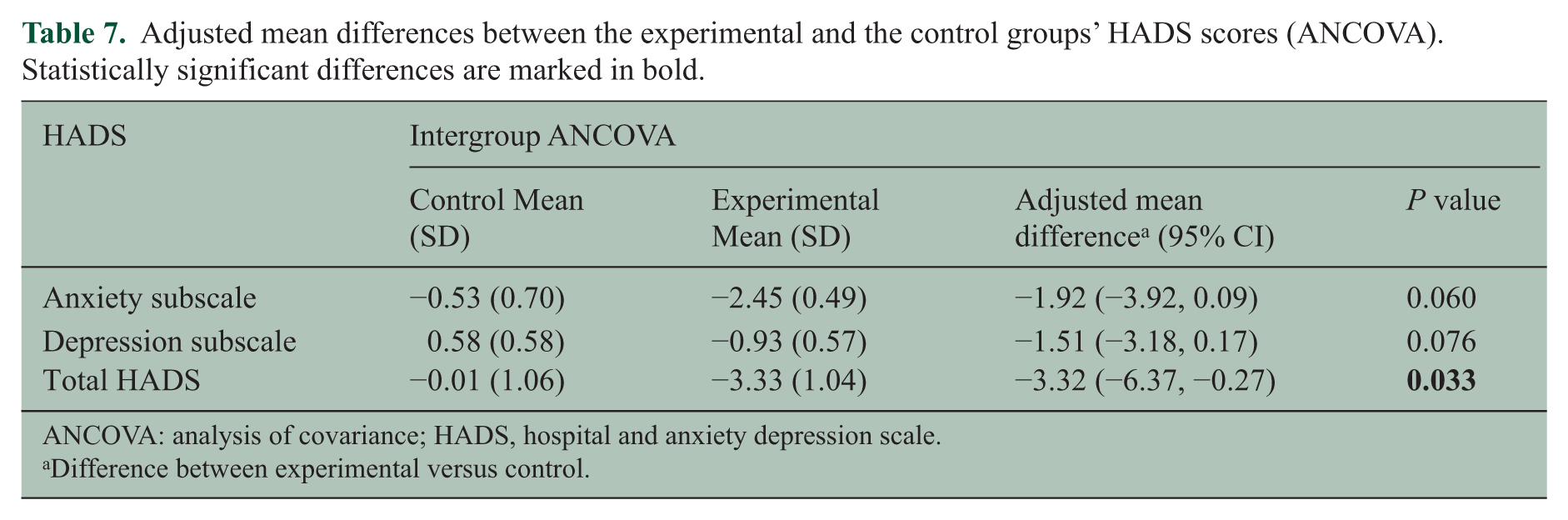
ANCOVA: analysis of covariance; HADS, hospital and anxiety depression scale.
Difference between experimental versus control.
Adjusted mean differences between the experimental and the control groups’ HADS scores (ANCOVA). Statistically significant differences are marked in bold.
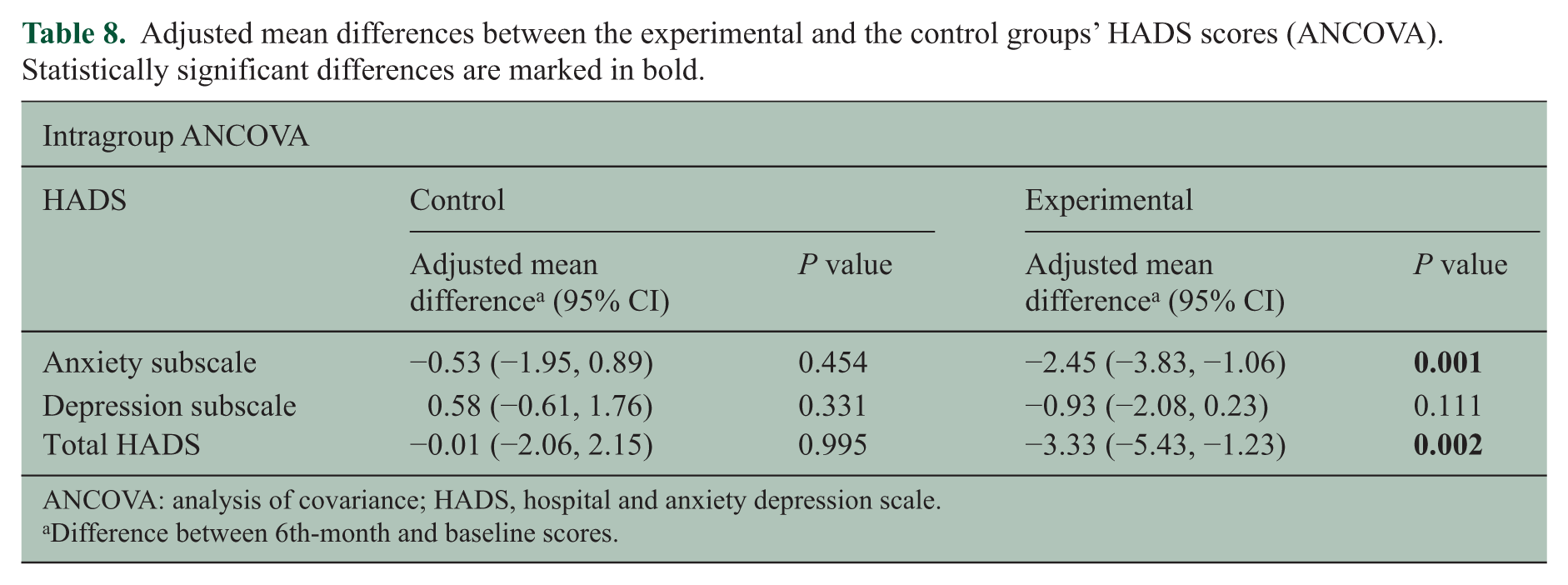
ANCOVA: analysis of covariance; HADS, hospital and anxiety depression scale.
Difference between 6th-month and baseline scores.
Quality of life
Neither intragroup nor intergroup ANCOVA showed significant differences in the VAS of EuroQol-5D or MSIS-29 total score.
Adherence to MS-Line!
The mean attendance rate at cognitive rehabilitation sessions was 84.3% and the mean completion rate of daily exercises was 83.8%. Eight out of 22 patients (36.4%) who received the cognitive rehabilitation programme were considered as adherent to MS-Line!. However, covariance analysis did not find significant differences between adherent or non-adherent patients in the six cognitive tests (10/36 SPART-T, 10/36 SPART-DR, WLG test, LNS, BNT and TMT-A) scores that previously had revealed significant differences between the experimental and control groups. Post-hoc analysis, defining adherence as having participated in at least 75% of sessions and as having completed the daily exercises, showed significant differences in the covariance analysis for 10/36 SPART-DR (P=0.0300) and a trend towards significance in the WLG test (P=0.0801) between adherent (11 patients) and non-adherent patients (11 patients).
Discussion
We have performed a prospective controlled study to assess the efficacy of the MS-Line! cognitive rehabilitation programme in MS patients. ANCOVA reveals that after cognitive rehabilitation, patients who received treatment improved in six out of the 18 (33%) cognitive tests used in the study. This improvement was found to relate to learning and visual memory, executive functions, attention and information processing speed, and naming ability. In the intragroup analysis, the experimental group had better results in 13 out of the 18 (72%) cognitive tests. On the other hand, the control group performed at significantly higher levels in only one of the 18 tests evaluated (6%): the FAS test (P<0.01). These results suggest that MS-Line! works effectively although other possible explanations should be considered. The results may have been influenced by practice effects on neuropsychological test per-formance, which would help to explain the slight improvement found in the control group with the FAS test. However, we did include a control group in order to examine treatment efficacy beyond this practice effect, and a battery of neuropsychological tests clearly showed that this treatment effect did indeed exist. In order to avoid the regression to the mean phenomenon, in addition to using a control group that was similar to the experimental group in terms of clinical and neuropsychological baseline variables, an ANCOVA approach was used that explicitly models the influence of the pre-test scores on the post-test scores by the inclusion of a term for regression towards the mean in the model. 23 It is also possible that the results were influenced by an extra effort being made by patients as they knew they were members of the experimental group.
Although it is not easy to establish the percentage of variability of each of these factors in the final outcome, the influence of the practice effect is unlikely to exceed 5–10% of the total variability in the experimental group as this was the improvement found in the control group. The contribution of other factors, such as the real effect of treatment or the feeling of belonging to one group or the other, are impossible to discern with the model that we have used. This methodology could be improved by incorporating an active control group that would be required to perform unrelated tasks at the hospital.
The real effect of treatment and the specificity of cognitive rehabilitation is a controversial area. Although it seems reasonable to suppose that programmes designed specifically to treat functions affected by MS will perform better than programmes applied more broadly to a variety of neurological diseases, this cannot be verified as no specific programmes have been available until now. The closest we have to such a study is Solari et al., 24 who found similar levels of improvement between patients following a function-specific training programme (attention and memory exercises) and those following a non-specific rehabilitation programme (visual constructive and visual memory skills). However, the REHACOM programme they used was not specifically developed for MS patients. The same situation occurs with other more recent studies that have been published, which are all methodologically solid, allowing treatment differences to be detected after treatment, but that use programmes that rehabilitate functions independently of the neurological aetiology. 25 Different strategies have also been published for improving memory in patients with MS. 26 These behavioural approaches appear so effective that changes in cerebral activity measured by functional magnetic resonance imaging are still observed at 6 months. 27
Our present results are consistent with previous studies performed by Brissart et al. 28 and Shatil et al., 29 who both used general cognitive rehabilitation programmes (Procog-SEP and CogniFit Personal Coach). Patients participating in Brissart’s 6-month study showed improvement in verbal and visuospatial memory, verbal fluency and in their responses to conflicting orders after treatment, but the absence of a control group makes one cautious when interpreting the results. In our case, patients were not found to improve in verbal memory, possibly due to the fact that most of the material used for memory stimulation used visual afferent rather than auditory pathways. In both Brissart et al. 28 and the present study, patients improved in semantic but not in phonemic fluency.
In Shatil et al., 29 the experimental group showed a significant improvement in comparison with the control group in three memory-based cognitive abilities (general memory, visual and verbal working memory), speed of information recall and focused attention.
In contrast with the studies of Brissart et al. and Shatil et al., our patients not only improved in memory functions but also in information processing speed, executive functions and naming ability.
Although it is not possible to attribute these improved results to specific methodological differences, the greater number of sessions, the increasing difficulty of the tasks, the three types of materials included in the programme, and the use of materials specifically designed for cognitive deterioration in MS are all likely to have contributed.
With regard to the assessment of anxiety and depression, Jønsson et al., 30 Mendoza et al., 31 Brenk et al. 32 and Mattioli et al. 33 observed improvements in affectivity after periods of cognitive rehabilitation (the first three studies used the Beck depression inventory, whereas the last used the Montgomery–Asberg depression rating scale) and in the case of Jønsson et al. 30 this improvement continued at 6 months. In our study sample, we found a clinical improvement of the anxiety symptoms using the HADS from 7.5 (probable disorder) to 5.1 (no disorder) points in the experimental group. This clinically significant difference had an effect on the trend towards significance found in the ANCOVA between groups (P=0.0604). There were also significant differences between groups in the total HADS score (P<0.05). No clinically significant differences were found in depressive symptoms as none of the groups had baseline scores suggestive of a depressive disorder. However, the results showed a trend towards significance between the experimental and control groups (P=0.0765).
Recently, in analyzing the effects of a 13-week neuropsychological rehabilitation programme on cognition in MS patients, Mäntynen et al. 34 failed to find improvements in cognitive function but did find reduced perceived cognitive deficits measured with the perceived deficits questionnaire 35 in their experimental group. In our study, on the other hand, no improvement in quality of life was detected using the EuroQol-5D and MSIS-29 questionnaires, possibly as a result of poor instrument selection as neither of these two questionnaires studies cognitive functions in depth.
One of our main concerns in designing the cognitive rehabilitation programme was to promote adherence by making the materials attractive. Our success in this endeavour will be determined by the level of adherence once the programme is used by patients at home without the supervision of a clinician, but the 80% mean completion rate of the daily home-based exercises found during the trial is a promising result. Adherence may also be enforced by the involvement of family members in the treatment, and by the fact that clues are supplied, so creating a positive psychological climate for patients to find solutions for themselves.
While the fact that the mean time from diagnosis was 10 years might be considered a limitation given that the objective of MS-Line! is to promote cognitive rehabilitation in the early years of the disease, we do not consider this to be a major concern as our patients had a mean EDSS of 2.7, and 38 out of the 43 patients were in the relapsing-remitting phase. However, it should be noted that Shatil et al. 29 found that older and more deteriorated MS patients are more adherent than younger patients in carrying out cognitive rehabilitation therapy at home. A second limitation could be that there may be a self-selecting bias. However, it must also be borne in mind that this was a pilot study and that a multicentre study with a larger sample size and an improved methodology will be required to validate our initial findings.
To the best of our knowledge, MS-Line! is the first general cognitive rehabilitation programme developed specifically taking into account the cognitive profile of MS patients. By going beyond other programmes in providing written, manipulative and computer-based materials rather than just two-dimensional computer-based exercises and games, cognitive domains other than the purely sensorial afferent pathways are reinforced through visual spatial, visual constructive, manipulative and motor skill training.
In conclusion, the study finds a significant improvement in information processing speed, attention, learning and visual memory, naming ability and executive functions. Furthermore, a tendency towards significance is found in tests that evaluate verbal memory and planning ability as well as manipulative praxis. These promising results suggest a clear tendency to the efficacy of MS-Line! in counteracting the main cognitive deficits associated with MS.
Footnotes
Acknowledgements
The authors wish to thank Xavier Núñez from TFS and Maria Buxó from IDIBGI for their assistance with the statistical analysis, Sonsoles García Rodicio for her advice in the methodological design of the study and for her critical reading of the manuscript, and Andrew J Hughes for language editing.
Conflict of interest
The authors declare that there is no conflict of interest with any financial organization regarding the material discussed in the manuscript.
Funding
Financial support was provided by Biogen Idec, Merck Serono, Bayer Healthcare, Teva Pharmaceutical Industries, ‘La Caixa’ (Spain), Fundación Obra Social Caja Madrid (Spain) and Acadèmia de Ciències Mèdiques i de la Salut de Catalunya i de Balears (Spain).