
Abstract
Background:
The pathophysiology of multiple sclerosis (MS) tremor is uncertain with limited phenotypical studies available.
Objective:
To investigate whether dystonia contributes to MS tremor and its severity.
Methods:
MS patients (n = 54) with and without disabling uni- or bilateral upper limb tremor were recruited (39 limbs per group). We rated tremor severity, writing and Archimedes spiral drawing; cerebellar dysfunction (SARA score); the Global Dystonia Scale (GDS) for proximal and distal upper limbs, dystonic posturing, mirror movements, geste antagoniste, and writer’s cramp.
Results:
Geste antagoniste, mirror dystonia, and dystonic posturing were more frequent and severe (p < 0.001) and dystonia scores were correlated with tremor severity in tremor compared to non-tremor patients. A 1-unit increase in distal dystonia predicted a 0.52-Bain unit (95% confidence interval (CI) 0.08–0.97), p = 0.022) increase in tremor severity and a 1-unit (95% CI 0.48–1.6, p = 0.001) increase in drawing scores. A 1-unit increase in proximal dystonia predicted 0.93-Bain unit increase (95% CI 0.45–1.41, p < 0.001) in tremor severity and 1.5-units (95% CI 0.62–2.41, p = 0.002) increase in the drawing score. Cerebellar function in the tremor limb and tremor severity was correlated (p < 0.001).
Conclusions:
Upper limb dystonia is common in MS tremor suggesting that MS tremor pathophysiology involves cerebello-pallido-thalamo-cortical network dysfunction.
Introduction
Tremor, which can affect up to two-thirds of multiple sclerosis (MS) patients, 1 is associated with higher Expanded Disability Status Scale (EDSS) scores. 2 Recently, clinical studies demonstrated that action tremor, attributed to cerebellar disease, is the most common MS tremor type. 1 The classical view of MS tremor as purely of cerebellar origin is, however, in doubt, with studies of tremor pathogenesis in animals and the surgical targeting of the thalamic nuclei in the treatment of MS tremor highlighting interactions between the cerebellum, cortex, basal ganglia, and thalamus.3–5
We recently demonstrated that targeted onabotulinumtoxin A, a drug commonly used for focal dystonia, 6 reduces upper limb tremor severity in MS patients.1,7 This finding, together with empiric clinical observation, raises the possibility that dystonia contributes to tremor in MS.
The purpose of this study was to investigate the presence of upper limb dystonia and its contribution to tremor occurrence and severity in MS. We therefore recorded the presence and severity of dystonia in well-matched MS patients with and without tremor.
Methodology
Participants
Twenty-seven relapsing–remitting and secondary progressive MS patients with disabling upper limb tremor,8,9 aged between 18 and 70 years, were recruited from two tertiary hospital MS clinics from 2010 to 2012. In the control group, 27 MS patients without tremor were matched for age, sex, EDSS, and disease duration. When bilateral tremor was present, both limbs were assessed independently in the tremor case and matched control. Patients were excluded if they were on tremor-suppressing medication or if they had experienced a MS relapse in the preceding 3 months. Participants were required to have near normal upper limb strength (Medical Research Council (MRC) score >4/5). 10
Standard protocol approvals, registrations, and patient consents
This study was conducted in accordance with the Declaration of Helsinki and participants provided voluntary, written consent to protocols approved by the human research ethics committees of the participating hospitals. Authorizations have been obtained for disclosure of recognizable persons in videos.
Assessments
Multiple sclerosis disease course
MS disease subtype and disease duration were determined from clinical history. Two qualified raters determined the EDSS on all participants. 2 Sensory examinations were rated using the Kurtzke Functional Score for Sensation. 2 Strength was assessed using the MRC rating system. 10
Tremor assessments
Tremor was clinically defined according to published guidelines. 11 Tremor severity was rated using the Bain tremor rating score, previously validated for MS tremor.12,13 Overall tremor severity, writing a standardized sentence, and drawing an Archimedes spiral on a pre-drawn pattern with the dominant hand, was rated from 0 (no tremor) to 10 (extremely severe tremor).
Tremor severity was rated after assessing tremor components in detail with participants sitting comfortably in a chair. The rest component was scored with the arms in the patient’s lap. Postural tremor was assessed in two positions. Firstly, with the arms outstretched, hands pronated, and fingers spread and secondly, in the bat wing position (shoulders abducted to 90°, elbows flexed, and fingers almost touching below the nose). Kinetic tremor was measured during the transit phase of the finger-nose test and intention tremor as the subject’s index finger approached a target placed at the limit of reach. Each component of the examination lasted at least 10 s.
Cerebellar assessment
Ataxia was assessed using the Scale for the Assessment and Rating of Ataxia (SARA) in the absence of a validated MS-specific ataxia scale. 14 This scale has been validated for use in spinocerebellar ataxias, and provides a comprehensive assessment of cerebellar function. Limb assessments include measurements of dysmetria, intention tremor, and heel-shin testing. Each limb is scored separately before obtaining a total score.
Dystonia assessments
Dystonia is a movement disorder characterized by sustained or intermittent muscle contractions causing abnormal, often repetitive, movements, postures, or both. 15 Motor phenomenology includes alleviating maneuvers (geste antagoniste) that are simple movements directed to the affected body region to correct the abnormal posture. Mirror movements (or mirror dystonia) are unilateral postures or movements that are similar to a dystonic feature that can be elicited, usually in the more severely affected side, when contralateral movements are performed.
Upper limb dystonia was assessed with the patient sitting and the arms outstretched. The patient was instructed to alternately open and close, and then to pronate and supinate the hands. The rater also observed for abnormal posturing or movements of the affected limb whilst the patient performed tasks such as writing, drawing and drinking with both limbs. Lower limb dystonia was assessed with the patient sitting in a chair (feet resting on the ground and with the legs extended 90 degrees) and also whilst walking. The overall presence and severity of dystonia was assessed with the Unified Dystonia Rating Scale (UDRS). 16 The Global Dystonia Scale (GDS) was applied to rate dystonia in the shoulder and proximal arm and distal arm and hand only. The GDS rate dystonia from 0 (no dystonia) to 10 (severe dystonia). In addition, the presence of dystonic posturing, mirror movements and geste antagoniste was documented and rated for severity on a five-point scale from 0 (none) to 4 (severe).
Functional tasks
Writing and drawing was scored using the Bain tremor score. The writing assessment required the patient to write a sentence with the dominant hand. The drawing task was completed by asking participants to draw an Archimedes spiral on a pre-drawn pattern, using their dominant hand. In addition, participants were asked to draw straight lines between bars with each hand. These assessments were photocopied, renumbered, and blindly rated by an independent movement disorder expert. Additional motor tasks included drinking from a cup with each hand and pouring water from one cup to another. Tremor whilst drinking from a full cup, using each hand, was assessed on a five-point scale (0 = none; 1 = mild; 2 = moderate; 3 = marked; 4 = severe). The CRST (Combined Rating Score for Tremor) was used to rate pouring performance with each hand. The nine-hole peg test was included as a test of upper limb dexterity, 17 with the better of two trials recorded.
Video assessments and blinded ratings
A standardized video assessment was completed for each par-ticipant. On study completion, the videos were renumbered, shuffled and presented to an independent, blinded rater who rated both tremor and dystonia severity. When bilateral limb tremor was present, the blinded rater was instructed to independently rate both limbs of the patient and their control using separate rating forms to maintain limb independence. Ten randomly selected videos were rated twice, 3 months apart, to determine intra-rater reliability.
Statistics
Categorical variables were summarized using frequency and percentage. Continuous variables were all skewed and therefore summarized using median and interquartile range (IQR). Uni-variate associations between tremor severity, EDSS, dystonia and SARA scores were tested using non-parametric Spearman’s rank correlations.
Differences in outcome (tremor severity scores, cerebellar function, dystonia and functional tasks) between cases and controls were assessed using a Wilcoxon signed-rank test for continuous outcomes and a McNemar chi test for categorical outcomes. Associations between dystonia score and tremor severity for cases were investigated using univariable and multivariable quantile median regression where disease duration and EDSS were the controlling covariates. Quantile regression was used because the Bain score distribution was skewed. A link test was used to assess each model for specification error whilst a He and Zhu omnibus goodness of fit test was used to assess the overall fit of the adjusted quantile regression models. The effect of tremor severity (Bain score) on multiple sclerosis disability (EDSS) in tremor cases was investigated using multivariable linear regression controlling for age and disease duration. Intra-rater reliability was assessed through generation of reliability coefficients.
All reported p-values are two-tailed and for all analyses p < 0.05 was considered significant. All analyses were performed using Stata version 12 (StataCorp, College Station, Texas).
Results
Demographic data and tremor characteristics
Twelve patients had bilateral upper limb tremor resulting in a total of 39 upper limbs in each group. There were no differences in baseline characteristics between the groups (see Table 1).
Demographic data of MS tremor cases compared to disease-matched non-tremor controls.
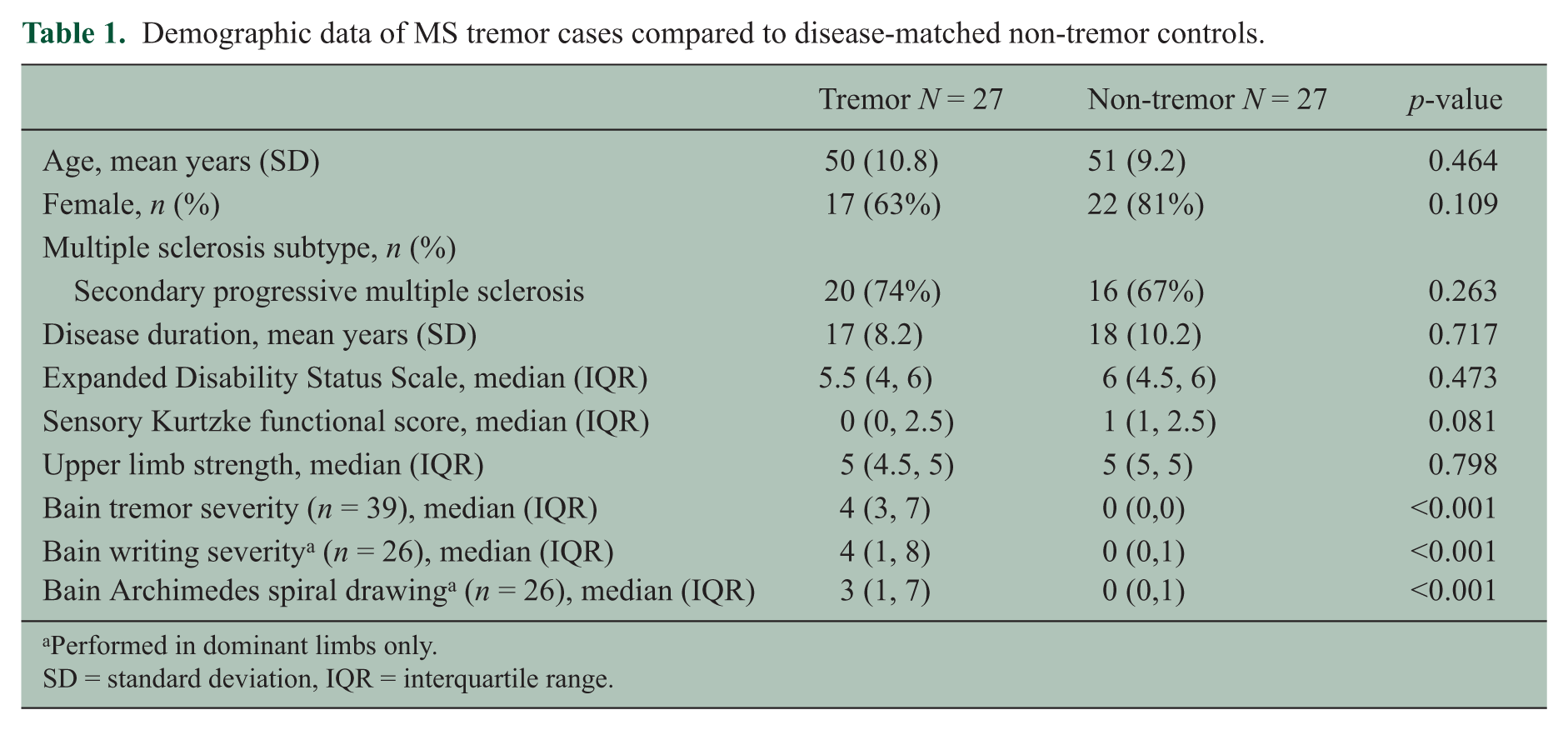
Performed in dominant limbs only.
SD = standard deviation, IQR = interquartile range.
The average latency from first symptoms of MS to the onset of tremor was 10.7 (standard deviation (SD) 8.7) years. Head and neck tremor was observed in 15 (56%) of patients and the trunk was involved in 13 (48%) cases. Median upper limb tremor severity was moderate with a Bain score of 4 (IQR 3.7). Of the 39 tremor limbs, 13 (33%) were classified as severe (Bain score = 8 (IQR 7,9), 10 (26%) as moderate (Bain score = 5 (IQR 4,5.5), and 16 (41%) as mild (Bain score = 2 (IQR 2,3). Leg tremor was present unilaterally in three (11%) patients and bilaterally in 12 (44%) patients. All leg tremors were postural/kinetic or observed during heel-shin testing.
Performance in functional tasks, such as the CRST drawing score, was worse in tremor patients (2 (1,4)) than in controls (0 (0,0)). Pouring scores were also worse in tremor (2 (1,4)) than non-tremor patients (0 (0,0). Not surprisingly, tremor patients (2 (1,4)) performed less well when drinking from a cup than controls (0 (0,0) and nine-hole peg test times were also longer in tremor patients (mean 63.5 seconds (SD 50)) than in controls (23.2 seconds (SD 5.2). The p-value for all above comparisons was p < 0.001.
Dystonia in MS patients with and without tremor
The presence and severity of dystonia was compared between tremor and non-tremor patients (Table 2). All dystonia scales were significantly worse (p < 0.001) in patients with tremor than those without. In the tremor patients, GDS scores for distal dystonia (median 3 (IQR 2,5)) were higher than for proximal dystonia (median 1 (0,3)). Dystonic features such as geste antagoniste and mirror dystonia were more frequent and more severe in tremor patients than in non-tremor controls (see video 1). Dystonic posturing, although almost universally present in the tremor cohort, was also observed in 46% of the non-tremor group (p < 0.001). However, dystonic posturing in non-tremor patients was very mild (median 0 (IQR 0,1)) compared to that in tremor patients (2 (2,3)), p < 0.001.
The presence and severity of dystonia in MS patients with tremor compared to those without tremor.
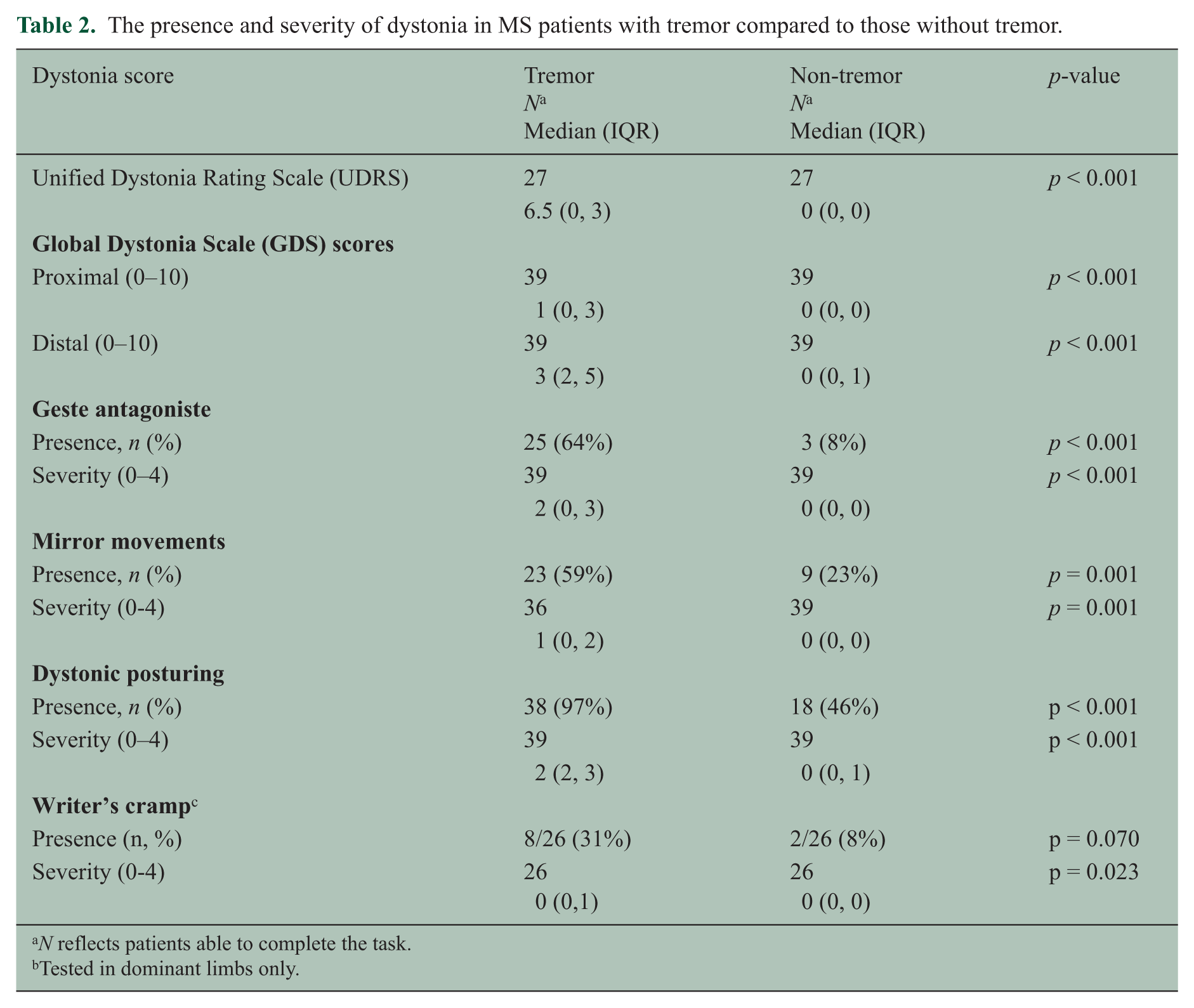
N reflects patients able to complete the task.
Tested in dominant limbs only.
Correlation between severity of tremor, dystonia, and cerebellar dysfunction
We tested the correlations between three tremor severity scores, dystonia, and cerebellar rating scores. As shown in Table 3, both proximal (r = 0.419, p = 0.008) and distal (r = 0.493, p = 0.001) GDS scores correlated with Bain Tremor severity score. Distal, but not proximal GDS scores were correlated with the Bain Archimedes spiral drawing score (p < 0.001) and the Bain writing score (p = 0.020). In assessment of correlation between tremor and cerebellar scores, the total SARA score did not correlate with the tremor severity scores. However, Bain tremor severity scores significantly correlated with cerebellar ataxia scores (finger-chase test, nose-finger test, fast alternating movement test) pertaining to the tremor-affected limb (p < 0.001).
Relationship between dystonia and cerebellar dysfunction and Bain tremor severity scores.
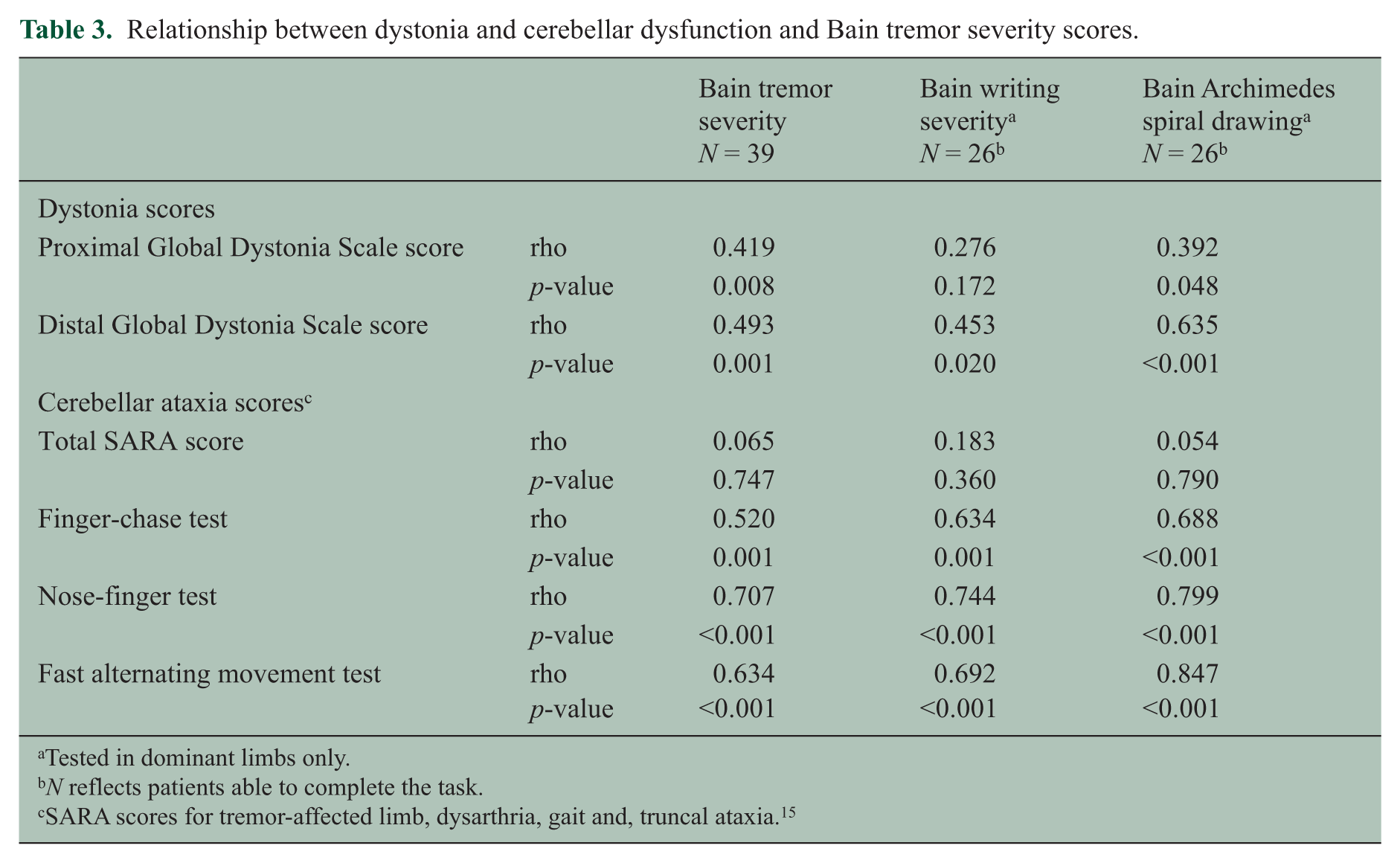
Tested in dominant limbs only.
N reflects patients able to complete the task.
SARA scores for tremor-affected limb, dysarthria, gait and, truncal ataxia. 15
The relationship between dystonia severity (distal or proximal GDS score, modeled separately) and tremor severity (Bain score) was further assessed by quantile median regression controlling for disease duration and EDSS. In a multi-variable model, a 1-unit increase in distal GDS was associated with a 0.52-unit (95% confidence interval (CI) 0.08–0.97), p = 0.022) increase in Bain tremor severity score. In a further model, a trend for worse distal dystonia to increase the Bain writing score severity by 0.8-units was found (95% CI −0.07 to 1.6, p = 0.070). Furthermore, a higher distal GDS score significantly predicted an increase of 1-unit in the Bain Archimedes spiral score (95% CI 0.48–1.6, p = 0.001).
Using the same multi-variable model but assessing proximal rather than distal GDS scores, proximal GDS scores were associated with a 0.93-unit increase (95% CI 0.45–1.41, p < 0.001) in Bain tremor severity score after controlling for EDSS and disease duration. A trend for proximal dystonia to independently worsen writing ability (as assessed using Bain writing score severity) by 0.99-units (95% CI 0.00–1.99), p = 0.050) was found. The severity of proximal dystonia was significantly associated with a 1.5-unit (95% CI 0.62–2.41, p = 0.002) increase in Bain Archimedes spiral score.
The effect of tremor severity on MS disability
The effect of tremor severity on MS disability (EDSS) was investigated using linear regression corrected for age and disease duration. In tremor cases, Bain severity score independently predicted EDSS in cases with a 1-point increase in Bain score correlating with a mean 0.25 unit increase in EDSS (95% CI 0.10–0.39, p = 0.002).
Intra-rater reliability
Intra-rater reliability was substantial to almost-perfect for all scores (see Table e-1).
Discussion
Our major novel finding is the association between MS upper limb tremor and dystonia, given the widespread assumption that MS upper limb tremor is a cerebellar ataxia syndrome. Dystonia was more frequent and severe in tremor patients compared to disease-matched non-tremor controls. Tremor patients were more likely to exhibit dystonic features such as geste antagoniste or mirror dystonia, while dystonic posturing occurred almost universally in this group. Dystonia was moderate in most tremor cases, with the severity and location of dystonia predicting a 0.5–1.5 point increase in Bain scores for tremor, writing and drawing impairment. Dystonia severity correlated with tremor severity in the in the tremor-affected limb independently of EDSS and disease duration, indicating a unique link between the two movement disorders. Upper limb cerebellar impairment scores also correlated with tremor severity, suggesting that a combination of cerebellar dysfunction and dystonia, especially distal upper limb dystonia, is the likely cause of most MS upper limb tremor.
Our study is the first to describe dystonic features associated with upper limb MS tremor. Although Alusi et al.’s work described dystonic head tilt with head tremor, 1 there was no examination for dystonia in other tremor-affected body areas. The most well described MS related dystonia is thought to be paroxysmal dystonia (or tonic spasms) hypothesized to be caused by spreading ephaptic activation of axons within a lesion at any level in a motor pathway. 18 Other focal dystonias are thought to be rare in MS, with occasional case reports of spasmodic torticollis,1,19 focal dystonia,3,20 blepharospasm, 21 hemidystonia, 22 and writer’s cramp, 23 mostly corresponding to acute inflammatory lesions. A few cases of generalized dystonia in MS have been published with plaques in the basal ganglia implicated. 24
In patients without MS, association of tremor and dystonia can be confusing and the term “dystonic tremor” has been inconsistently applied in the literature. 15 Currently, the descriptor dystonic tremor is reserved for the coexistence of tremor and dystonia in the same body segment. 11 Dystonic tremor is further characterized by directionality, with the increasing amplitude in one particular direction, and by the null point phenomenon, resulting in diminished or absent tremor in certain limb positions. Our data therefore indicate that the tremor of MS may be regarded as dystonic or having dystonic features.
The association of MS tremor with both cerebellar dysfunction and dystonia is informative on a pathophysiological level and points to injury within the cerebello-pallido-thalamo-cortical tract and/or dysfunction in the feedforward cortico-cerebellar loops. Onabotulinumtoxin A has peripheral and central mechanisms of action, and likely improves tremor and dystonia through modulation of these networks. 25 Peripherally, onabotulinumtoxin A decreases excitability of muscle spindles, reflex loop function and increased long latency stretch reflexes.5,26,27 Peripheral input is relayed to the nucleus ventralis intermedius before being integrated by the primary motor cortex, 28 which then provides modulation to the motor network through feedforward loops. 29 In dystonia, onabotulinumtoxin A has an effect on central motor network modulation through the pallido-thalamic tract and its outflow to the motor areas involved.30,31 The lack of clinical weakness from onabotulinumtoxin A injection despite tremor reduction in the majority of treated patients would support this proposed central mechanism.7,32 Imaging work by Feys et al. demonstrated a relationship between the lesion load in the contralateral pons and MS tremor severity. 33 These findings suggest that tremor-related lesions in the pons may affect the ascending projections via the cerebello-thalamic pathway and/or descending pathways, such as the rubro-olivary and cortico-olivary tracts, which can all be modulated by the central actions of onabotulinumtoxin A.
The results of our study add significantly to the current literature on MS tremor phenomenology. As reported, 1 MS causes predominantly upper limb action tremor (postural, kinetic, and intention tremors). In our cohort, other body parts were frequently involved, particularly the head and neck. Lower limb tremor was less commonly seen, and when present, was predominantly postural in nature, which differentiates it from leg clonus, a condition that worsens with passive activation of stretch reflexes. Tremor is mostly a feature of secondary progressive MS and a median latency of 10 years from diagnosis to the onset of the tremor was observed. In addition, the tremor spread so that it often involved more body areas over time. Most patients in this study had moderate tremor but one-third of tremors were severe or very severe (Bain score ⩾7). Furthermore, clinical signs of cerebellar dysfunction, considered to be a predictor of worse prognosis, 34 were more pronounced in patients with tremor than those without, demonstrating the complexity of this movement disorder. More severe tremor resulted in higher EDSS scores independently of age and disease duration, consistent with published reports. 1
There are limitations to our clinically focused study. We were not able to accurately quantify the relative contribution of cerebellar dysfunction and dystonia to MS tremor. EMG techniques may be helpful in the future to further delineate the importance of these components in the generation of MS tremor. 35 Ratings were done based on video recordings with high intra-rater reliability (see Table e-1), but direct assessments may provide additional clinical insights. Detailed neuro-imaging, delineating possible demyelinating lesions in the basal ganglia, would also be important in future studies. Patients in this cohort were selected to have disabling tremor, hence the findings in this study may not be generalizable to MS patients with milder tremor.
The results of this study demonstrate the importance of recognizing dystonia as part of the complex movement disorder that results in symptomatic MS-related tremor. The view that MS tremor is synonymous with intention tremor due to injury in a single neuroanatomical site, the cerebellum, is overly simplistic and also limits the treatment options. Our description of dystonic features in upper limb tremor generates a theoretical framework to explain the effectiveness of onabotulinumtoxin A for this disabling symptom. It should generate the impetus for additional phenomenological and imaging studies to further define the neuroanatomical networks involved in multiple sclerosis tremor generation and give rise to novel and replicative therapeutic studies.
Footnotes
Conflict of interest
Dr A van der Walt has received travel support from Novartis Australia and speaker’s honoraria from Biogen Idec. She receives a post-doctoral fellowship from the Melbourne Brain Centre at RMH, University of Melbourne. She is an investigator on National MS Society (USA) Project Grant (RG4211A4/2).
Dr K Buzzard has received post-doctoral fellowship support from Genzyme and has received speaker’s honoraria from Novartis and conference travel support from Sanofi Aventis and Biogen Idec.
Dr S Sung has received unrestricted grant support from Pfizer Australia and Allergan Australia.
Dr T Spelman has received travel support from Biogen Idec Australia.
Dr M Marriott has served on scientific advisory boards for Bayer Australia. He has received travel support from Biogen Idec, Merck Serono, and Novartis.
Dr Kolbe has received travel support from Merck Serono. Has received an MS Research Australia postdoctoral fellowship. He is an investigator on National MS Society (USA) Project Grant (RG4211A4/2).
A/Prof Helmut Butzkueven has served on scientific advisory boards for Biogen Idec, Novartis, and Sanofi-Aventis and has received conference travel support from Novartis, Biogen Idec and Sanofi Aventis. He serves on steering committees for trials conducted by Merck Serono, Biogen Idec, and Novartis. Prof Butzkueven has received research support from Merck Serono, Novartis, and Biogen Idec in his capacity as honorary chair of the MSBase Foundation. He is on the editorial board of Multiple Sclerosis International. He is the recipient of a National Health and Medical Research Council (NHMRC) Career Development Award (628856), NHMRC Project Grants (566513, 628799, and 1009757), NHMRC Centre of Excellence Award (1001216), an Australian Research Council Linkage Grant (LP110100473) and National MS Society (USA) Project Grants (RG3850A3/1 and RG4211A4/2).
Dr Andrew Evans has received honoraria from Novartis for giving presentations, and providing consultancy services. He has participation in scientific advisory board meetings for Novartis, UCB pharma, Allergan, and Boehringer Ingelheim. He has received conference travel support from Boehringer Ingelheim.
Dr van der Walt contributed to the design and study conceptualization. She was one of the examining neurologists, and assisted with data analysis and interpretation. She drafted the manuscript.
Dr Buzzard was an examining neurologist and assisted with data interpretation. She assisted with drafting the manuscript.
Dr Sung contributed to data collection by acting as the blinded independent rater. He assisted with the drafting and revision of the manuscript.
Dr Tim Spelman assisted with data analysis and interpretation. He assisted with the drafting and revision of the manuscript.
Dr Scott Kolbe contributed to the design and study conceptualization. He assisted with the drafting and revision of the manuscript.
Dr Mark Marriott contributed to the data analyses and the drafting and revision of the manuscript.
A/Prof Butzkueven contributed to the design and study conceptualization. He assisted with data analysis and interpretation as well as with drafting and revising the manuscript.
Dr Andrew Evans contributed to the design and study conceptualization. He acted as an examining neurologist, and assisted with data analysis and interpretation. He assisted with drafting the manuscript.
Funding
This work was supported by the Box Hill MS Research Fund.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.