
Abstract
Aim:
We examined the combined effect of having multiple key risk factors and the interactions between the key risk factors of multiple sclerosis (MS).
Methods:
We performed an incident case-control study including cases with a first clinical diagnosis of central nervous system demyelination (FCD) and population-based controls.
Results:
Compared to those without any risk factors, those with one, two, three, and four or five risk factors had increased odds of being an FCD case of 2.12 (95% confidence interval (CI), 1.11–4.03), 4.31 (95% CI, 2.24–8.31), 7.96 (95% CI, 3.84–16.49), and 21.24 (95% CI, 5.48–82.40), respectively. Only HLA-DR15 and history of infectious mononucleosis interacted significantly on the additive scale (Synergy index, 3.78; p = 0.03). The five key risk factors jointly accounted for 63.8% (95% CI, 43.9–91.4) of FCD onset. High anti-EBNA IgG was another important contributor.
Conclusions:
A high proportion of FCD onset can be explained by the currently known risk factors, with HLA-DR15, ever smoking and low cumulative sun exposure explaining most. We identified a significant interaction between HLA-DR15 and history of IM in predicting an FCD of CNS demyelination, which together with previous observations suggests that this is a true interaction.
Keywords
Introduction
Multiple sclerosis (MS) is a multi-factorial disorder caused by the interplay of genetic and environmental factors. A number of risk factors are now known, including human leucocyte antigen (HLA)-DRB1*1501-DQB1*0602 (HLA-DR15),1,2 high anti-Epstein-Barr virus nuclear antigen (anti-EBNA) immunoglobulin (Ig)G levels3,4 and history of infectious mononucleosis (IM). 5 HLA-A*02:01 (HLA-A2) has been demonstrated to have an independent protective effect on MS, and there is now substantial evidence that low personal sun exposure and low circulating vitamin D (25-hydroxyvitamin D (25(OH)D)) levels are associated with an increased risk of MS. 6 We recently showed that 25(OH)D level and cumulative sun exposure, measured by actinic damage of the skin, were independent predictors of risk. 7 A large number of studies, including prospective studies,8–11 have found modest positive associations between smoking and MS. 12
Given that no single factor leads to the development of MS, the joint action of, or interactions between, these factors is likely to be important and informs our understanding of potential causal pathways. While some studies have looked at interactions between two or three factors,13,14 none have had the capability of examining interactions between all key MS risk factors. It is also important to know which prevention efforts are most worthwhile, taking into account the interactions between the multiple risk factors. Here, using an incident case-control study including cases with a first clinical diagnosis of central nervous system (CNS) demyelination (FCD), we examined the interactions between the key MS risk factors on disease risk and the joint impact of the risk factors on FCD as well as the relative importance of each factor.
Methods
The Ausimmune Study is a multi-centre case-control study in four regions of Australia: Brisbane city (latitude 27 degrees South), Newcastle city and surrounds (33 degrees South), Geelong city and the Western Districts of Victoria (37 degrees South) and the island of Tasmania (43 degrees South). 15 Detail is provided in a previous publication on the study in relation to the design and bias. 15
Participants
Participants were aged 18–61 years and resident within a study region between 1 November 2003 and 31 December 2006. Cases had an incident FCD within the study period, including true first demyelinating events (FDEs) (defined as a single, first, episode of demyelination as per international consensus criteria 16 ), primary progressive multiple sclerosis (PPMS), and possible subsequent events, where the historical first event had not previously been clinically diagnosed. Cases were notified of the study by medical specialists and a study neurologist confirmed the date and symptomatology of the FDE and conducted a full neurological examination. Annually case clinical information was reviewed by the study neurologist group to assess eligibility as FDE, FCD or PPMS. Of 311 eligible cases, 282 (91%) agreed to participate, including those presenting with a classic FDE (n = 216), a first diagnosis of PPMS (n = 18) and those in whom, in retrospect, there had been a previous, undiagnosed, probable FDE (n = 48).
Controls were randomly selected from the Australian Electoral Roll (compulsory registration for citizens ⩾18 years) and matched to cases (2:1) on age (within two years), sex and study region. Of 1118 controls initially selected, 937 were successfully contacted (84%) and 558 participated in the study (60% of those contacted).
The Ausimmune Study was approved by nine regional human research ethics committees. All participants gave written informed consent.
Measurements
We collected self-report data on history of IM (‘have you ever had glandular fever?’), smoking history, and highest education level. Silicone skin casts were used to objectively measure cumulative past sun exposure. 17 They were made on the dorsum of both hands as previously described, 17 photographed and graded on a scale from 1 to 6, representing minimal to severe actinic skin damage. Skin reflectance on the buttock (non-sun-exposed site) was measured using a hand-held spectrophotometer (Minolta 2500d) to estimate cutaneous melanin density. 17
Most participants provided a blood sample (94%). Serum aliquots (1 ml) were stored at −80°C and analysed at study completion. Concentration of 25(OH)D was measured using liquid chromatography tandem mass spectrometry, with a high inter-batch agreement for duplicate samples (n = 39 pairs, intraclass correlation = 0.89). The genotyping for HLA-DR15 (single-nucleotide polymorphism (SNP) rs9271366) was performed by the SNPline method (KBiosciences, Hoddesdon Herts, UK). HLA-DR15 was measured using proxy SNP rs9271366. The genotyping for HLA-A2 (SNP rs2844821 on Illumina Custom MS Chip) was performed by the Hussman Institute for Human Genomics, University of Miami (USA) on 218 cases and 405 controls. Anti-EBNA IgG antibody titres were measured only on n = 206 cases, n = 217 controls, using an immunofluorescence assay. 18
Data analysis
Conditional logistic regression was used to account for the matched study design. 19 To allow for seasonal effects of 25(OH)D level on disease onset, we fitted region-specific sine and cosine curves 20 to the individual data points of 25(OH)D level and used these curves to project 25(OH)D levels of the controls to the blood collection date of the matched case. All key factors were coded as dichotomised factors to obtain odds ratios (ORs) >1: HLA-DR15 SNP rs9271355 (GG or AG vs AA), HLA-A2 SNP rs2844821 (AA vs AG), ever had IM (yes vs no), high anti-EBNA IgG (⩾160 vs <160), low 25(OH)D levels at FCD onset (<50 nmol/l vs ⩾50 nmol/l), and ever smoked (yes vs no). To assess interaction on the multiplicative scale, we included a product term in the logistic model. To examine interaction on an additive scale, we used the Synergy Index (SI), because it is the only additive interaction parameter where the parameter does not vary across strata, allowing adjustment for confounders. 21 Confidence intervals (CIs) and p values for measures of additive interaction were obtained using a first-order linear approximation (delta method). 22 We calculated the population attributable fraction (PAF) of FCD due to the combination of multiple risk factors by summing category-specific attributable fractions (estimated from the prevalence in the cases and OR for disease) for each combination of risk factors using methods described elsewhere. 23 CIs were calculated using Jackknife delete-a-group, with groups based on the matched design. 24 To estimate the relative importance of each risk factor, we summed the category-specific fractions of those categories where the factor of interest was present.
Results
Around three-quarters of our participants were female and the mean age was 39 years (Table 1). In unadjusted analysis, HLA-DR15 was the strongest risk factor of FCD, followed by high anti-EBNA IgG titres. Table 2 shows a multifactorial model including all key risk factors. Because anti-EBNA IgG was measured on only a subset of participants, an additional column is provided limiting the sample to those with anti-EBNA IgG measured before adding in anti-EBNA IgG as a key variable in the model. A multivariable model including HLA-A2 showed no independent association (OR 1.09 (0.66–1.79)). We therefore did not carry HLA-A2 through in subsequent analyses.
Characteristics of cases and controls and associations between risk factors and first clinical diagnosis of CNS demyelination in the Ausimmune Study.
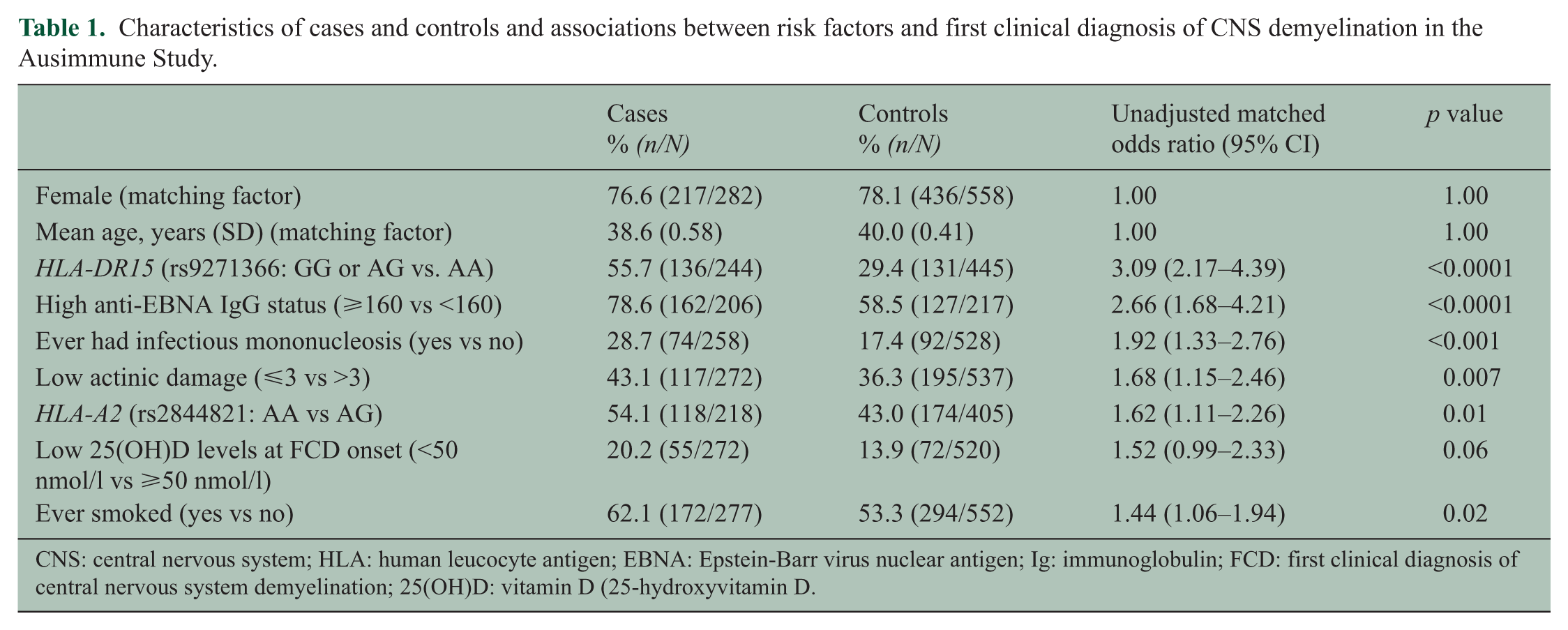
CNS: central nervous system; HLA: human leucocyte antigen; EBNA: Epstein-Barr virus nuclear antigen; Ig: immunoglobulin; FCD: first clinical diagnosis of central nervous system demyelination; 25(OH)D: vitamin D (25-hydroxyvitamin D.
Multivariable model (without interactions) of risk factors for first clinical diagnosis of CNS demyelination in the Ausimmune Study.
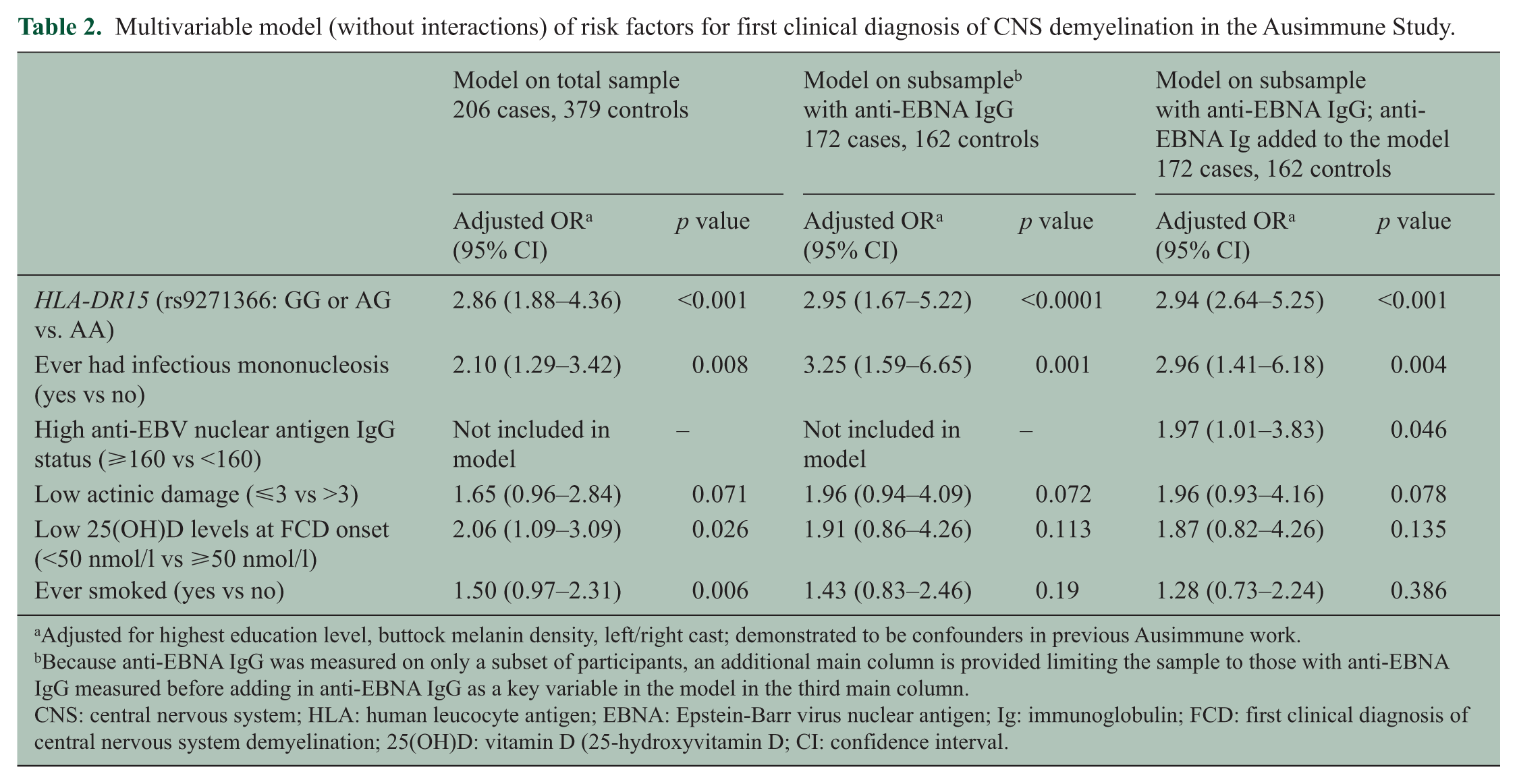
Adjusted for highest education level, buttock melanin density, left/right cast; demonstrated to be confounders in previous Ausimmune work.
Because anti-EBNA IgG was measured on only a subset of participants, an additional main column is provided limiting the sample to those with anti-EBNA IgG measured before adding in anti-EBNA IgG as a key variable in the model in the third main column.
CNS: central nervous system; HLA: human leucocyte antigen; EBNA: Epstein-Barr virus nuclear antigen; Ig: immunoglobulin; FCD: first clinical diagnosis of central nervous system demyelination; 25(OH)D: vitamin D (25-hydroxyvitamin D; CI: confidence interval.
Cumulative risk model
For every additional risk factor added to the model, the odds of disease roughly doubled (Table 3). Those people with four or five risk factors had odds that were more than 20 times higher compared to those without any risk factors. The results were similar when we limited to classic FDE cases (one risk factor, OR 1.98 (0.94–4.14), two risk factors, OR 4.25 (2.00–9.01), three risk factors, OR 7.01 (3.03–16.23), four or five risk factors, OR 20.52 (4.52–93.02).
An average estimate of relative risk of first clinical diagnosis of CNS demyelination for increasing number of risk factors.
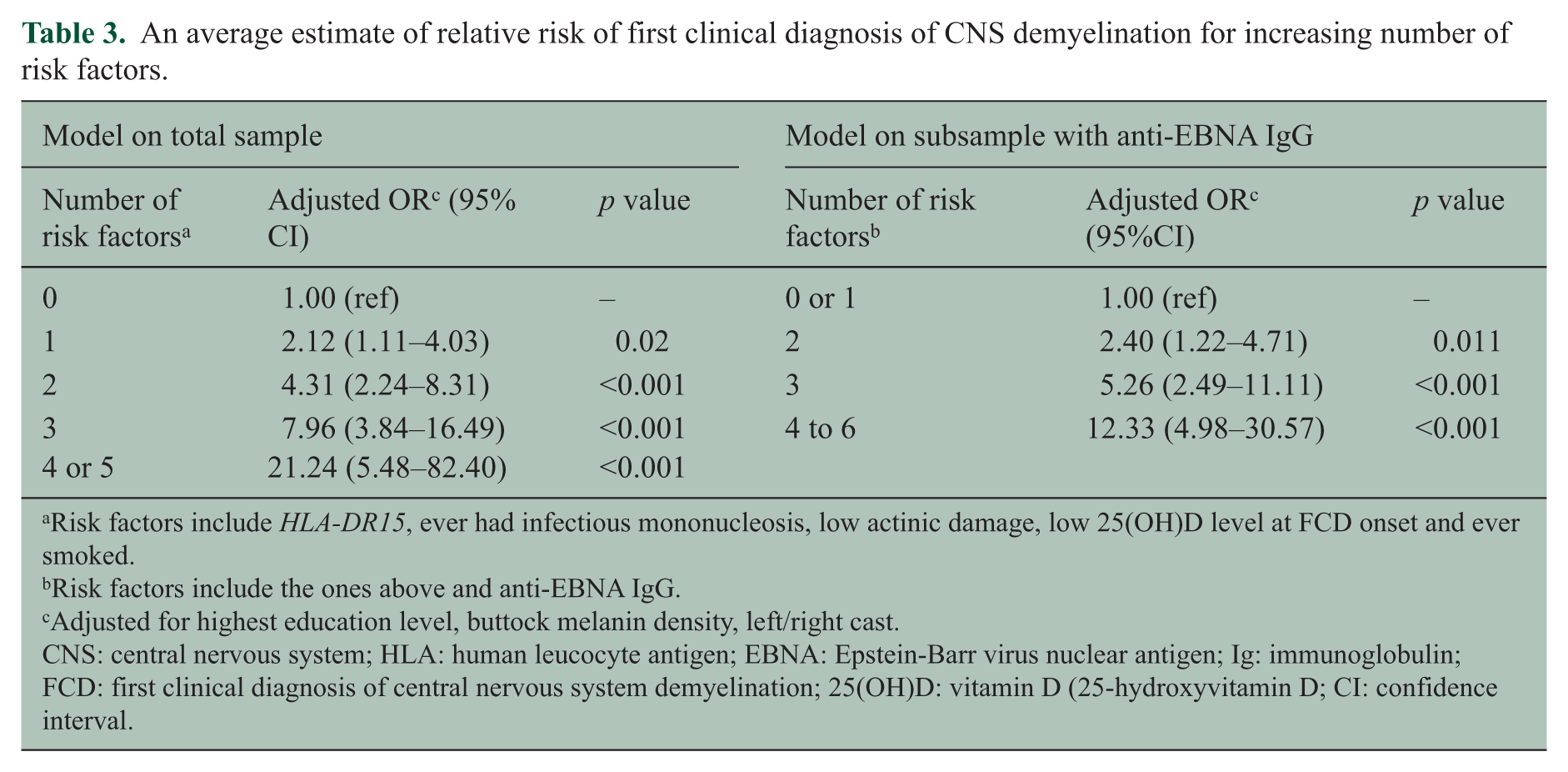
Risk factors include HLA-DR15, ever had infectious mononucleosis, low actinic damage, low 25(OH)D level at FCD onset and ever smoked.
Risk factors include the ones above and anti-EBNA IgG.
Adjusted for highest education level, buttock melanin density, left/right cast.
CNS: central nervous system; HLA: human leucocyte antigen; EBNA: Epstein-Barr virus nuclear antigen; Ig: immunoglobulin; FCD: first clinical diagnosis of central nervous system demyelination; 25(OH)D: vitamin D (25-hydroxyvitamin D; CI: confidence interval.
Interactions on the additive and multiplicative scale
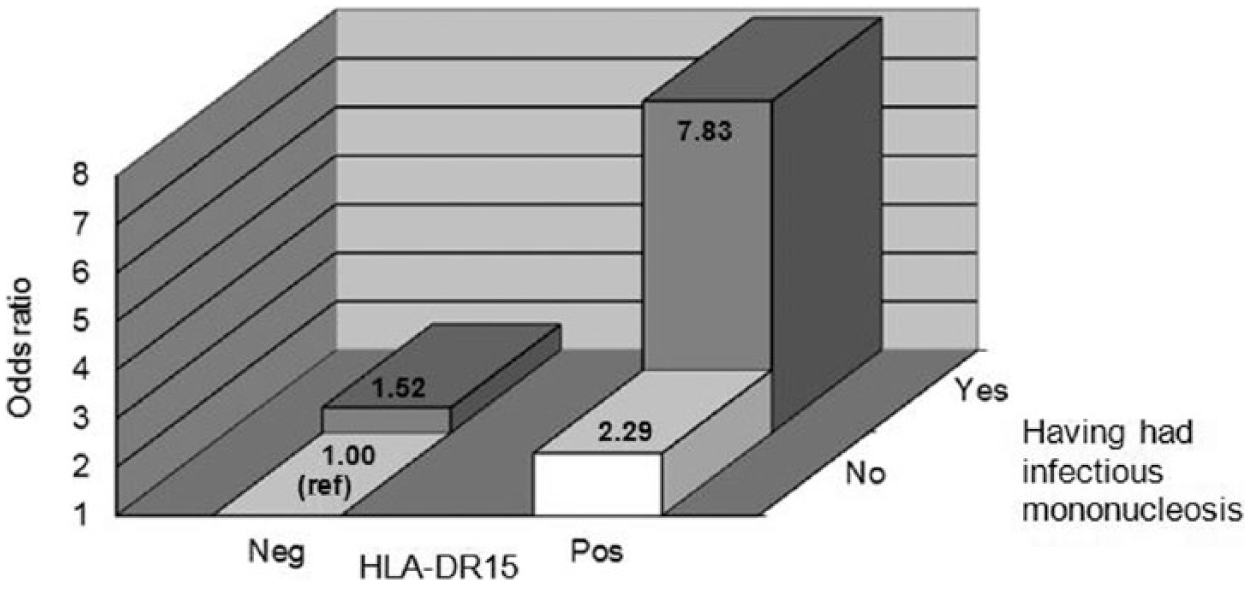
Table 4 shows all pairwise interactions between the key risk factors. We found a significant interaction on the additive scale (Figure 1). The combined effect of having both the HLA-DR15 genotype and a history of IM (OR, 7.83; 95% CI, 3.60–17.08) was higher than expected based on the effect of having had IM in the absence of HLA-DR15 (OR, 1.52; 95% CI, 0.79–2.94)) and the effect of HLA-DR15 in the absence of IM (OR, 2.29; 95% CI, 1.37–3.81) (SI, 3.78; p = 0.03). Expressed as stratified data, we found that the effect of HLA-DR15 was stronger among those with a history of IM (OR, 4.94; 95% CI, 2.16–11.29) compared to those without a history of IM (OR, 2.46; 95% CI, 1.58–3.86). There was some evidence for an interaction on the additive scale between HLA-DR15 and having ever smoked, and HLA-DR15 and low 25(OH)D levels at the time of FCD onset but these were not significant (Table 4). There were no significant interactions on the multiplicative scale.
Examination of interaction on the multiplicative and additive scale between different risk factors.
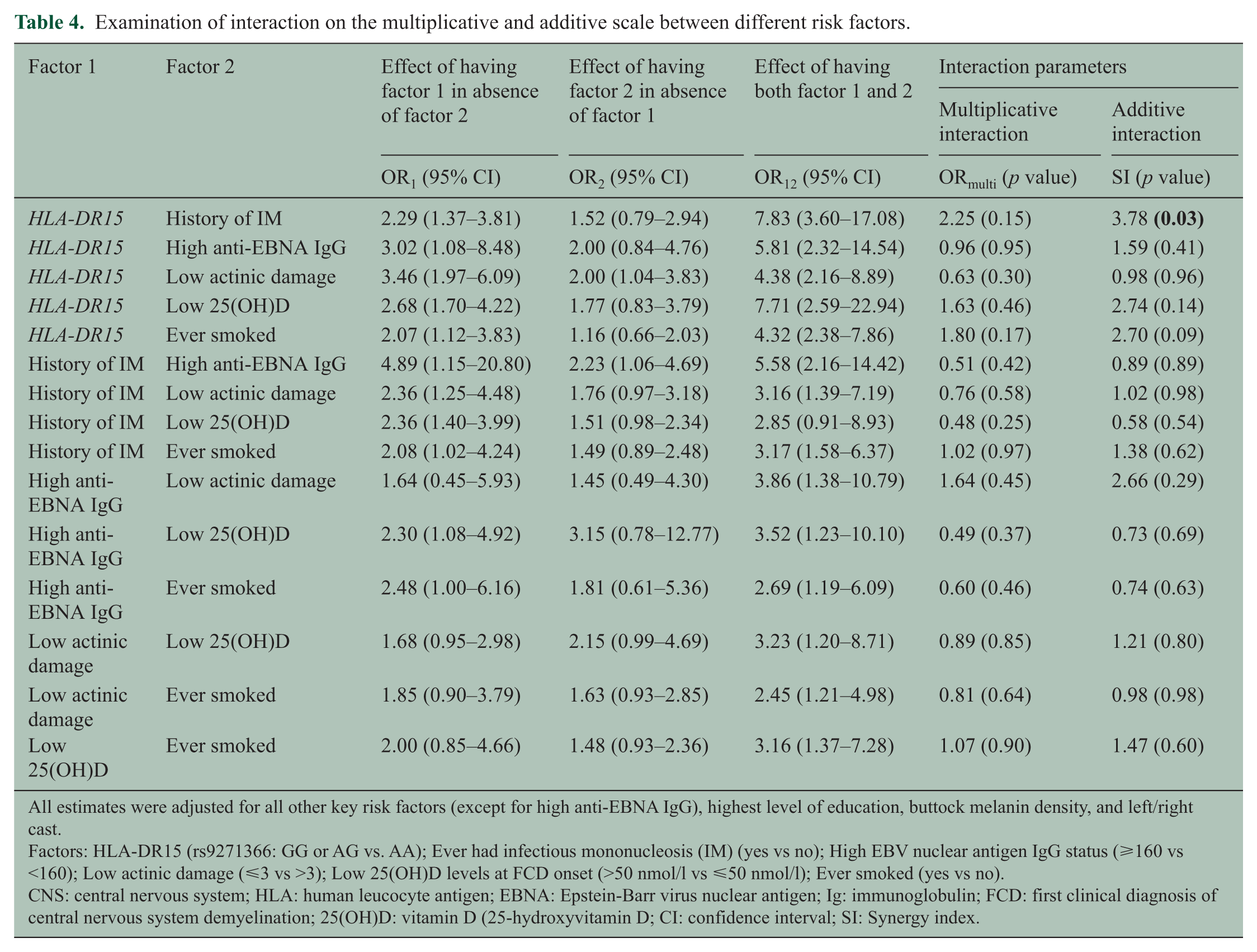
All estimates were adjusted for all other key risk factors (except for high anti-EBNA IgG), highest level of education, buttock melanin density, and left/right cast.
Factors: HLA-DR15 (rs9271366: GG or AG vs. AA); Ever had infectious mononucleosis (IM) (yes vs no); High EBV nuclear antigen IgG status (⩾160 vs <160); Low actinic damage (⩽3 vs >3); Low 25(OH)D levels at FCD onset (>50 nmol/l vs ⩽50 nmol/l); Ever smoked (yes vs no).
CNS: central nervous system; HLA: human leucocyte antigen; EBNA: Epstein-Barr virus nuclear antigen; Ig: immunoglobulin; FCD: first clinical diagnosis of central nervous system demyelination; 25(OH)D: vitamin D (25-hydroxyvitamin D; CI: confidence interval; SI: Synergy index.
Odds ratios for FCD for different combinations of HLA-DR15 and infectious mononucleosis.
We next examined the three interactions separately for males and females and adjusted the model for females for parity, because we previously identified this to be a strong confounder in females. 25 The interaction between HLA-DR15 and IM was present only for females (females: ORmulti = 5.25 (p = 0.02); SI = 11.04 (p = 0.02); males: ORmulti 0.25 (p = 0.29); SI = 0.45(p = 0.43)). The magnitude of effect of the interaction for females increased further when we adjusted for parity (ORmulti = 6.26 (p = 0.01); SI = 13.92 (p = 0.02). The interactions between HLA-DR15 and having ever smoked and between HLA-DR15 and 25(OH)D levels at FCD onset did not differ by sex (p > 0.8 for difference in effect, assessed on the multiplicative scale), and adjustment for parity in females did not materially change the parameters of interaction (data not shown).
Joint impact of the risk factors on MS and the relative importance of each factor
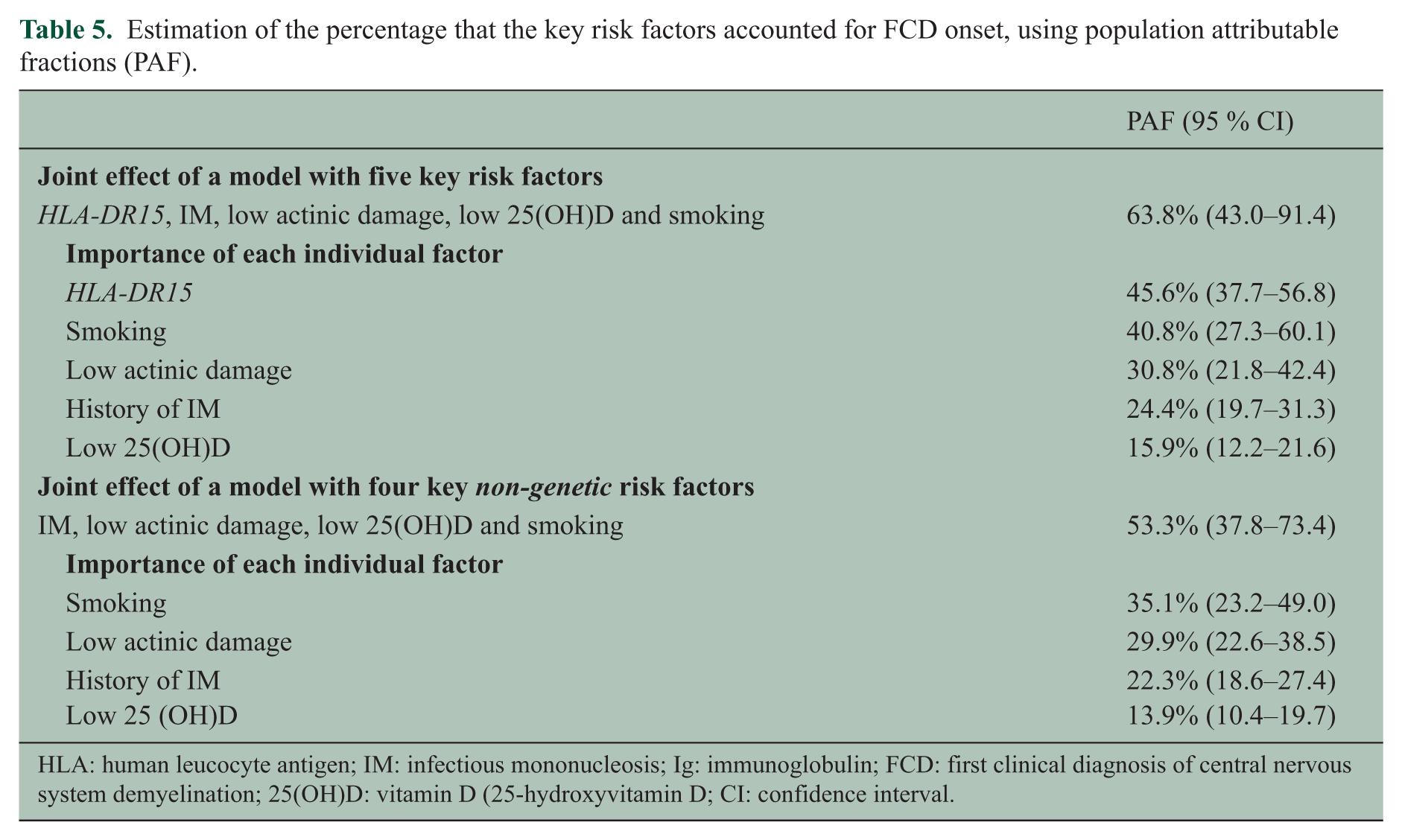
We estimated the PAF jointly for the five risk factors (HLA-DR15, IM, low actinic damage, low 25(OH)D at FCD onset and smoking), which takes any mode of interaction into account, and found that these factors accounted for 63.8% of FCD onset (Table 5). The results were similar when we limited to classic FDE cases (summary PAF 59.1%, HLA-DR15 41.6%, smoking 36.0%, low actinic damage 29.7%, history of IM 22.4%, and low 25(OH)D 16.9%). When we limited to the four non-genetic factors (IM, low actinic damage, low 25(OH)D at FCD onset and smoking), the summary PAF was 53.3%. To rank the importance of each factor, we summed the category-specific attributable fractions where the factor of interest was present. We found that HLA-DR15 contributed most, followed by smoking and low actinic damage (Table 5). The estimated summary PAF for just low actinic damage and low 25(OH)D at onset was 24.1% (95% CI, 13.9–36.1). The subsample was too small for running models with all risk factors including high anti-EBNA IgG. However, based on the overall high prevalence of this separate risk factor (78.6%) and an OR of 1.97, the individual PAF, excluding any joint actions, was 38.6% (95% CI, 10.1–66.2), suggesting that high anti-EBNA IgG also makes an important contribution to and would further increase the summary PAF.
Estimation of the percentage that the key risk factors accounted for FCD onset, using population attributable fractions (PAF).
HLA: human leucocyte antigen; IM: infectious mononucleosis; Ig: immunoglobulin; FCD: first clinical diagnosis of central nervous system demyelination; 25(OH)D: vitamin D (25-hydroxyvitamin D; CI: confidence interval.
Discussion
This study examines the joint impact of the key risk factors on disease, the relative importance of each factor and the effect of all pairwise interactions between these MS risk factors on the risk of an FCD of CNS demyelination, including a number of interactions that have not been previously examined. The five key risk factors jointly contributed to 63.8% of FCD onset, with HLA-DR15, ever smoking and lifetime sun exposure (measured by actinic damage) contributing most and high anti-EBNA IgG also likely to make a significant contribution. Every additional risk factor roughly doubles the odds of disease, and those people with four or five risk factors had odds that were more than 20 times higher than those without any risk factors. We identified a significant interaction on the additive scale between HLA-DR15 and a history of IM. We did not observe any significant interactions on the multiplicative scale.
Strengths of this multicentre study include the population-based design, recruitment of a large number of incident cases from regions spanning a wide latitude range, the examination of a broad spectrum of environmental factors, and the inclusion of objective and validated measured factors. We assessed a number of interactions that have not been previously reported, including interactions between low sun exposure and 25(OH)D levels at FCD onset with other leading factors such as IM or smoking, as well as the interaction between IM and smoking. Generally, larger sample sizes are needed to detect interactions compared to main effects. As studies are generally powered for main effects, this might lead to false-negative associations. Sometimes only ‘exciting’ significant interaction findings are reported out of a range of secondary analyses, resulting in publication bias. Therefore, the systematic approach of examining all key interactions is a strength. Despite the use of objective and validated measures, it is likely there is some measurement error in the use of proxy measures to indicate, for example, life course vitamin D status so the true summary PAF is likely to be higher than 63.8%. PAF estimates are based on the prevalence of exposures and these may differ for other populations. FCD cases included people with a classic FDE (76.6%), people with PPMS (6.4%) and people with a previous undiagnosed FDE (17.0%). Our key findings were similar when limited to classic FDE cases.
The significant interaction on the additive scale between HLA-DR15 and IM is in line with reports from two previous case-control studies,26–28 and a case-only study. 29 Putting the evidence critically together, and using stringent criteria as suggested by Boffetta and colleagues, 30 including the evidence on the main and interaction effects (replication, protection from bias, plausibility), suggests that at this stage there is moderate evidence for a true interaction. We did not observe an interaction between HLA-DR15 and anti-EBNA IgG levels, in line with two other studies,14,31 although one study identified interaction on the additive scale. 32 We also found no interaction between anti-EBNA IgG levels and history of IM, in line with results from the Tasmanian MS case-control study. 6 Interestingly, additive interactions have been found between HLA-DR15 and IgG reactivity to specific anti-EBNA1 domains (amino acid 385–420). 27 Having higher levels of antibodies to these anti-EBNA1 domains has been shown to be a stronger risk factor for MS than higher levels of EBNA1 IgG.27,33 Moreover, a recent genomewide association study identified SNPs located in the genes HLA-DRB1 and HLA-DQB1 that were significantly associated with anti-EBNA IgG levels, providing further support for a true interaction between HLA-DR15 and anti-EBNA IgG. 34 HLA class II molecules may play a role in viral penetration of B cells by serving as cofactors for EBV infection of B cells. A further or alternative role could be in T cell control of EBV-infected B cells, because HLA class II genes are involved in the presentation of viral antigens to T cells. 34
No other clear interactions between risk factors were evident, although some might have been significant in a larger dataset, such as the interaction between HLA-DR15 and having ever smoked, or low 25(OH)D.
Importantly, the five key risk factors jointly contributed to 63.8% of FCD, or said differently, if we were to be able to eliminate all five risk factors, we would theoretically reduce the FCD (and probably MS) incidence by 63.8%. More than 53.3% was due to non-genetic factors, indicating that prevention efforts directed towards these environmental factors could have a substantial impact. In order to ascertain which prevention efforts would be most worthwhile, we examined which factors were most important. We found that HLA-DR15, ever smoking and low cumulative sun exposure contributed most, largely due to the higher prevalence of these factors. Thus, our data suggest that reducing smoking rates and creating a smoke-free generation 35 will have substantial pay-offs for MS. Prevention efforts aimed at providing optimal vitamin D over the life course are being discussed. Our data indicate that improving 25(OH)D levels immediately before FCD onset may be less important than improving 25(OH)D over the longer term, given that low actinic damage is a marker of lower cumulative sun exposure and probably 25(OH)D status over a long period. Optimising sun exposure and vitamin D during the life course could have an important impact at the population level, because these two factors accounted for a quarter of FCD onset. We previously found that both low 25(OH)D levels at FCD onset and low actinic damage were independently predictive of FCD risk. However, we could not distinguish whether actinic damage reflects 25(OH)D impacting at different ages or whether there is an independent benefit of ultraviolet ray (UVR) exposure. If the latter, then prevention efforts aimed at optimising vitamin D alone may have less impact, and reversing the trends of decreasing time spent outside in younger cohorts 36 may be more important (while balancing the risks of sun exposure). We could not include anti-EBNA IgG levels in the same model, but reducing the prevalence of high anti-EBNA IgG levels is also likely to have a large impact given its high prevalence. If we were able to add this as an additional factor in our model, it was likely to increase the summary population attributable fraction well beyond 63.8%. In the future, vaccination or immune boosting may be effective in controlling EBV infections and reducing anti-EBNA IgG levels. 37
In conclusion, we identified a significant interaction between HLA-DR15 and history of IM in predicting an FCD of CNS demyelination, which together with previous observations suggests that this is likely to be a true interaction. A high proportion of FCD onset can be explained by the currently known MS risk factors, with HLA-DR15, ever smoking and low cumulative sun exposure explaining most, and high anti-EBNA IgG also likely making a high contribution. Optimising sun exposure and vitamin D during the life course could have an important impact at the population level.
Footnotes
Conflict of interest
None declared.
Funding
This work was supported by the Australian Research Council (Future Fellowship 100100511), the National Health and Medical Research Council of Australia, the Australian Research Council, Multiple Sclerosis Research Australia, the Royal Australasian College of Physicians, MS Research Australia, the United States National Multiple Sclerosis Society, the Poola Foundation, the Health Research Council of New Zealand, the MS Society of Tasmania, Bayer Schering Pharma, and Biogen Idec Inc.