
Abstract
Background:
Fingolimod modulates sphingosine-1-phosphate receptors that are also found in cardiovascular tissue.
Objective:
To investigate the effects of fingolimod on cardiac autonomic regulation prospectively.
Methods:
Twenty-seven relapsing–remitting multiple sclerosis patients underwent 24-hour electrocardiogram recording before, at the first day of fingolimod treatment (1d) and after three months of continuous dosing (3mo). The time interval between two consecutive R-peaks (RR-interval) was measured. Cardiac autonomic regulation was assessed by the various parameters of heart rate variability. Parasympathetic stimulation prolongs the RR-interval and increases heart rate variability while the effects of sympathetic stimulation are mainly the opposite. The low frequency/high frequency ratio reflects sympathovagal balance.
Results:
From baseline to 1d, a prolongation of the RR-interval (P<0.001), an increase in the values of various heart rate variability parameters (P<0.05 to P<0.001) and a decrease in the low frequency/high frequency ratio (P<0.05) were demonstrated. At 3mo, although the RR-interval remained longer (P<0.01), the values of various heart rate variability parameters were lower (P<0.01 to P<0.001) as compared to baseline. At 3mo, the low frequency/high frequency ratio (P<0.05) was higher in men than in women although no such difference was found at baseline or at 1d.
Conclusions:
After an initial increase in parasympathetic regulation, continuous fingolimod dosing shifts cardiac autonomic regulation towards sympathetic predominance, especially in men. Careful follow-up of fingolimod-treated relapsing–remitting multiple sclerosis patients is warranted as sympathetic predominance associates generally with impaired outcome.
ClinicalTrials.cov: NCT01704183
Introduction
Fingolimod is an increasingly prescribed disease modifying treatment for relapsing–remitting multiple sclerosis (RRMS).1,2 The therapeutic effects of fingolimod are mediated by the modulation of sphingosine-1-phosphate (S1P) receptors on lymphoid and neural structures.3–6 In addition, the S1P receptors are found in the cardiovascular system.7–9
The initial cardiovascular effects of fingolimod through S1P1 receptor modulation resemble that of muscarine M2 receptor activation by the parasympathetic nervous system.7,8 The initiation of fingolimod dosing triggers a decrease in heart rate and blood pressure due to initial S1P1 receptor agonism. 10 Continuous dosing with fingolimod, on the other hand, results in the downregulation of S1P1 receptors, a subsequent shift in the S1P receptor profile and an increase in blood pressure. 10 The effects of the altered S1P receptor profile on cardiac autonomic regulation, however, are not fully described.
Cardiac autonomic regulation can be non-invasively assessed by heart rate variability (HRV). 11 Heart rate varies with every heartbeat and HRV quantifies these fluctuations mathematically. In brief, parasympathetic stimulation results in increased HRV whereas sympathetic stimulation is associated with a decrease in HRV. Of note, decreased HRV is an established risk factor for subsequent cardiac events, malignant arrhythmias and even sudden cardiac death.12–14
In this study, we assessed HRV before the initiation of fingolimod, at the first day of fingolimod treatment and after three months of continuous dosing with fingolimod to evaluate the effects of fingolimod on cardiac autonomic regulation in patients with RRMS.
Materials and methods
Before participating in the study, each patient gave written informed consent after full explanation of the purpose, nature and risk of all procedures used. The study was carried out in accordance with the Declaration of Helsinki (2008) of the World Medical Association and the local ethics committee approved the study protocol.
Study population
The study population consisted of 27 patients (16 women and 11 men) with RRMS who were considered eligible for fingolimod treatment on a clinical basis. 15 Fingolimod was selected according to the accepted drug label set by the European Medicines Agency and was prescribed as a second-line immunomodulative treatment for RRMS either due to lack of effect or significant side effects for agents in the first line. Fingolimod treatment was initiated in the hospital before 10.00 a.m. Before discharge, all patients were subsequently followed for at least six hours, or as long as heart rate started to recover. None of the patients needed overnight observation in the hospital.
Patients were 43 ± 11 years of age, the diagnosis of RRMS was set 10 ± 7 years before the study and the Expanded Disability Status Scale (EDSS) was 3.4 ± 1.8 on average at baseline. Five patients (19%) had one or more of the following comorbidities: two patients (7%) had type 1 diabetes mellitus with insulin treatment, three patients (11%) were adequately treated with hormonal substitution for hypothyreosis, one patient (4%) had asthma and one patient (4%) had optimally treated hypertension combined with Raynaud phenomenon. No changes in medication other than the initiation of fingolimod were performed. Previous immunomodulative treatment for RRMS was discontinued at least a day before fingolimod initiation if shifted from interferon-1b or glatirameracetate and at least two months before if shifted from natalitsumab.
A total of 24 (89%) patients completed three months’ follow-up as one patient discontinued fingolimod due to pregnancy plan, another dropped out as he moved to another hospital district and one patient was lost to suicide after discharge.
Study protocol
The patients underwent 24-hour ambulatory electrocardiogram (ECG) recording 20 ± 16 days before fingolimod treatment (baseline), at the day of fingolimod initiation (1d) and after three months (88 ± 7 days) of fingolimod treatment (3mo). The neurological disability related to RRMS was assessed by EDSS for each patient at baseline. The study was registered at ClinicalTrials.gov (NCT01704183).
Acquisition of ECG signal
Twenty-four-hour ambulatory ECG recordings were performed using Schiller Medilog AR12plus recorders (Schiller Medilog, Schiller AG, Switzerland) with a sampling frequency of 250 Hz. Three bipolar ECG leads (modified chest lead V5, modified chest lead V1 and modified aVF) were used. Digital ECG recordings were read to the Darwin Holter analysis system (Schiller Medilog) and they were exported in MIT format for further analyses. Normal daily living was allowed during ambulatory ECG recordings with the exception of six hours in-hospital observation required by drug label at 1d.
Analysis of HRV
The values for different HRV measures were calculated according to the recommendations 11 and using the WinCPRS software (Absolute Aliens Oy, Turku, Finland). For the assessment of HRV in the time domain, the standard deviation of all RR-intervals (SDNN), the percentage of normal RR-interval with duration more than 50 months different from the previous normal RR-interval (pNN50) and the root mean square of successive differences in RR-interval (rMSSD) were measured. Frequency domain analysis of HRV was performed with fast Fourier transformation. The power spectrum of RR-interval variability was divided into very low frequency (VLF) (0.005–0.04 Hz), low frequency (LF) (0.04–0.15 Hz) and high frequency (HF) (0.15–0.40 Hz) bands. The integrals under the power spectral density functions were measured and expressed as absolute units (equal to area under the curves for the spectral densities) and as normalised units by dividing the power of LF (LFnu) and HF (HFnu) components by the total power, from which the <0.04 Hz spectral component had been subtracted and multiplying by 100. In addition, the ratio of the LF power band and HF power band (LF/HF ratio) was calculated.
Physiological correlates of HRV
Most HRV measures have an inverse relation to heart rate and thus HRV tends to be higher with lower HR (longer RR-interval) and vice versa. 16 High HRV associates with higher cardiac parasympathetic regulation and low HRV indicates lower cardiac parasympathetic regulation. 11 The physiological mechanisms underlying the various components of HRV differ from each other. In the time domain, parasympathetic activation is typically reflected by an increase in pNN50 and rMSSD variables of HRV. In the frequency domain, parasympathetic activity is the major contributor of the HF component of HRV. 17 Both parasympathetic and sympathetic components of autonomic nervous systems influence the LF component of HRV. The LFnu component is considered mainly to reflect sympathetic and the HFnu component to be a marker of parasympathetic cardiac autonomic regulation.17,18 Correspondingly, the LF/HF ratio indicates sympathovagal balance of cardiac autonomic regulation. 11
Statistical analyses
The normal distribution of variables was verified by the Kolmogorov–Smirnov test. In the case of non-normal distribution, logarithmic (ln) transformation was applied for statistical testing. Results are expressed as mean ± standard deviation (SD) unless otherwise indicated. The one-way analysis of variance (ANOVA) was applied to verify significant differences in measurements between baseline, 1d and 3mo overall. Thereafter, a paired t-test was applied to test the significances of differences between two specific time points. To test the significances of differences between the groups, an independent samples t-test was used for continuous variables. All analyses were conducted at the two-tailed level and a P-value <0.05 was considered statistically significant. All statistical analyses were performed using IBM SPSS statistics (version 19, 1989–2010; SPSS Inc., Chicago, USA).
Results
Cardiac autonomic regulation on the first day of fingolimod treatment
The average RR-interval was longer at 1d as compared to baseline (P<0.001) (Table 1, Figure 1). Correspondingly, SDNN (P<0.05) (Figure 2) and VLF (P<0.05) as well as HRV variables mirroring cardiac parasympathetic regulation (pNN50, P<0.001; rMSSD, P<0.01 and HFnu, P<0.01) were higher at 1d as compared to baseline (Table 1). Accordingly, HRV variables reflecting cardiac sympathetic regulation (LFnu, P<0.05) and sympathovagal balance (LF/HF ratio, P<0.01) were significantly lower at 1d than at baseline (Table 1).
Heart rate variability before fingolimod initiation (baseline), at the day of fingolimod initiation and after three months of fingolimod treatment.
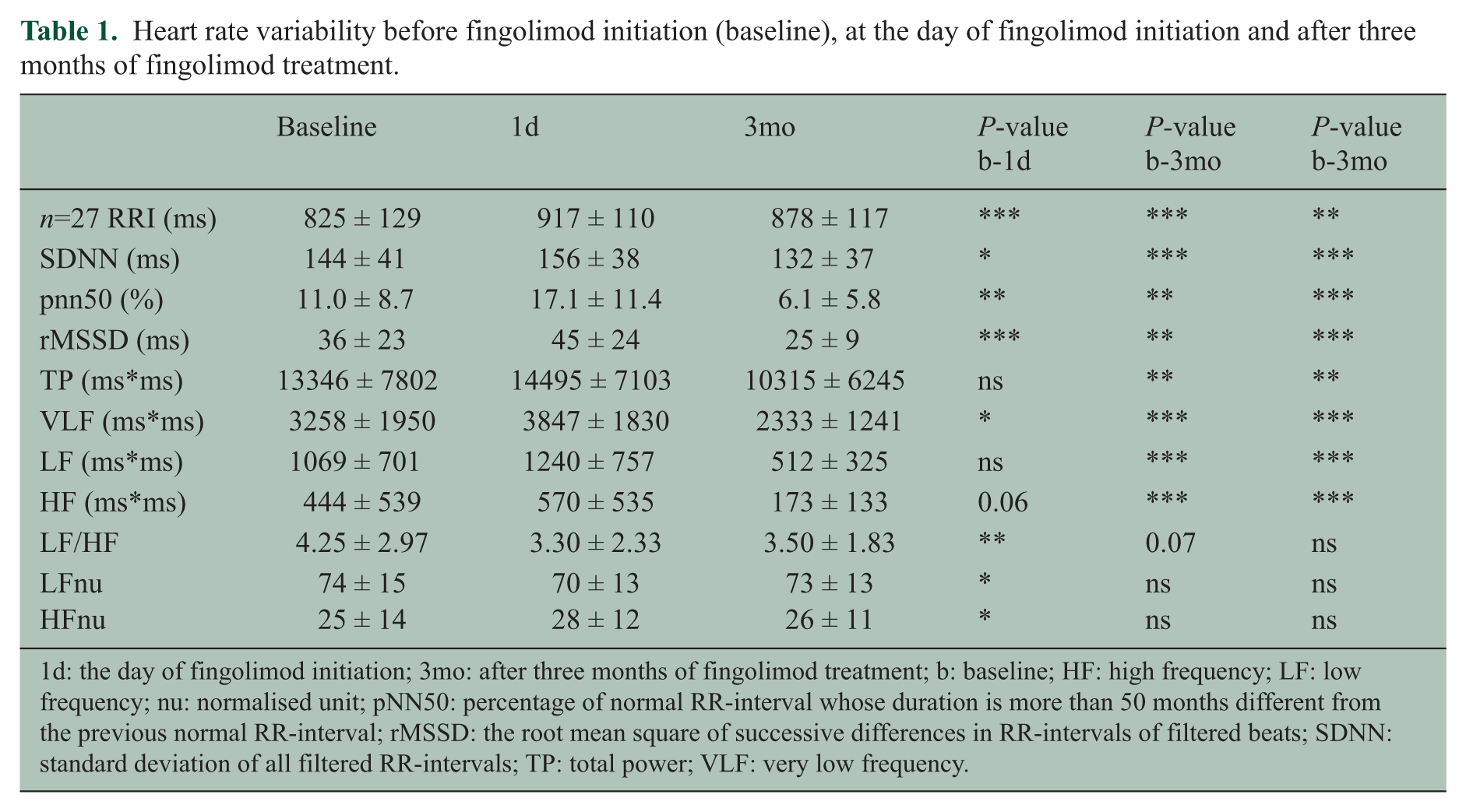
1d: the day of fingolimod initiation; 3mo: after three months of fingolimod treatment; b: baseline; HF: high frequency; LF: low frequency; nu: normalised unit; pNN50: percentage of normal RR-interval whose duration is more than 50 months different from the previous normal RR-interval; rMSSD: the root mean square of successive differences in RR-intervals of filtered beats; SDNN: standard deviation of all filtered RR-intervals; TP: total power; VLF: very low frequency.
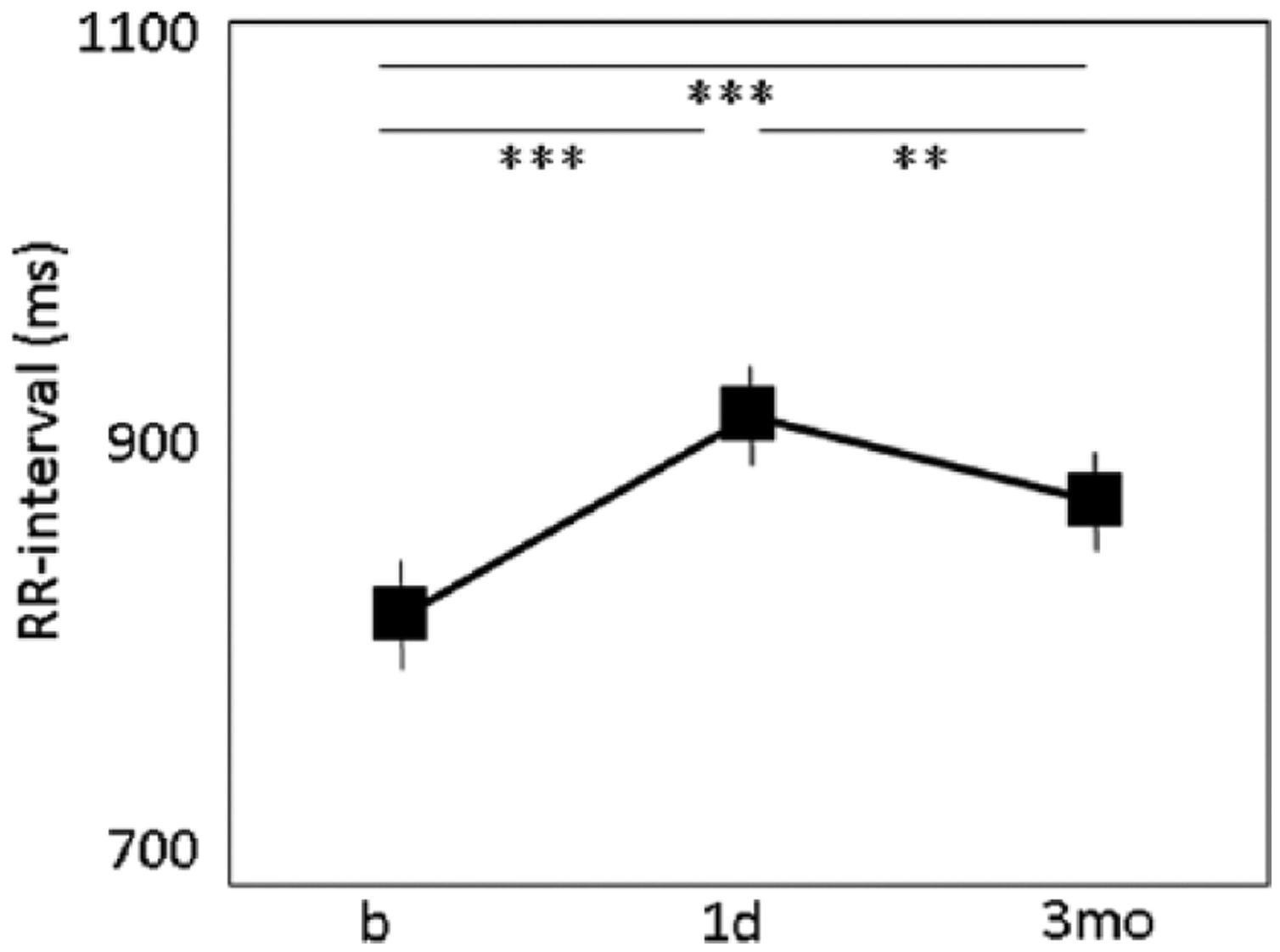
The time interval between two consecutive R-peaks (RR-interval) at baseline (b), at the first day of fingolimod treatment (1d) and after three months of continuous dosing with fingolimod (3mo). Values are expressed as mean ± SEM. Significances: **P<0.01 and ***P<0.001.
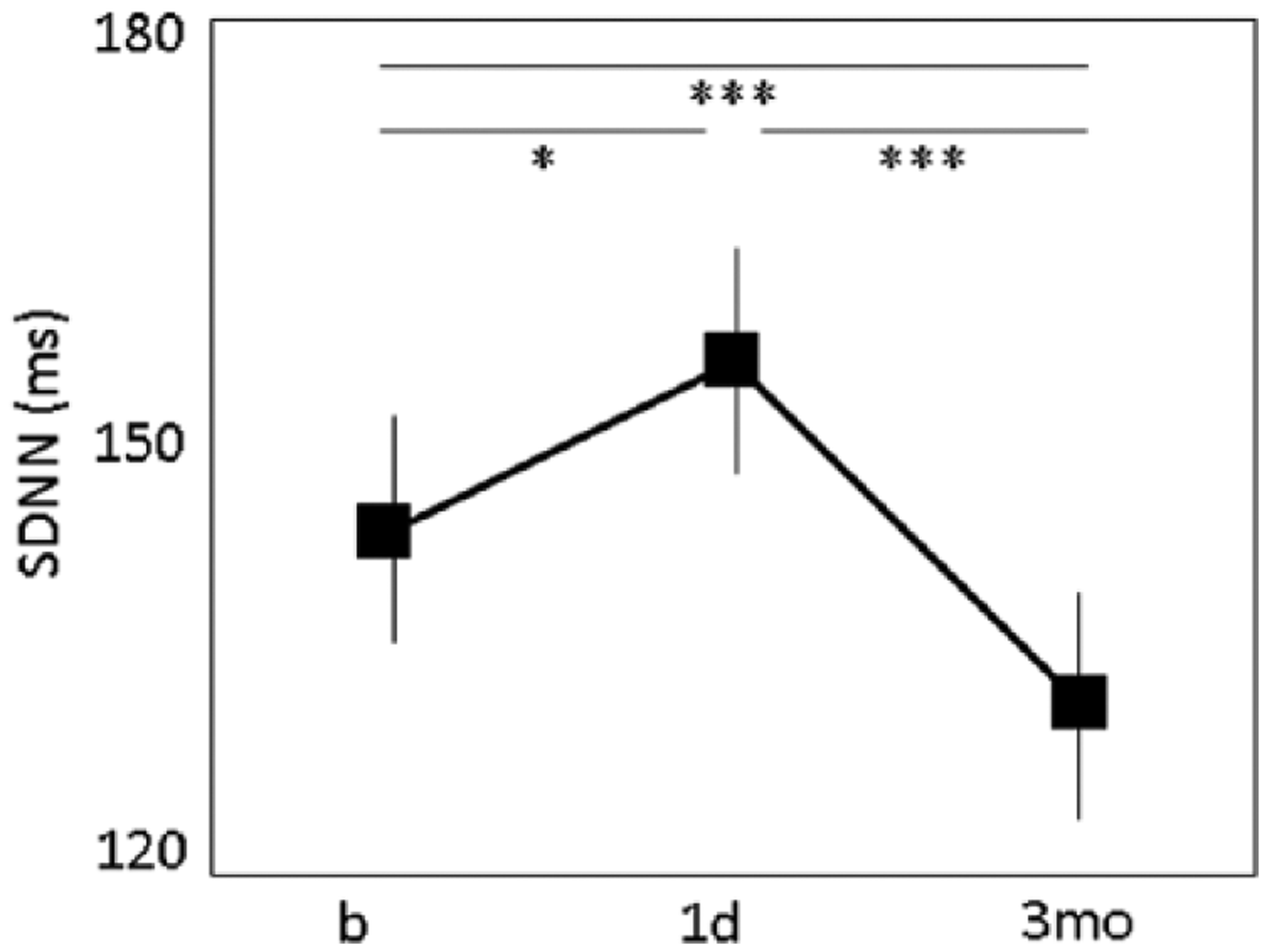
The standard deviation for all filtered RR-intervals (SDNN) at baseline (b) at the first day of fingolimod treatment (1d) and after three months of continuous dosing with fingolimod (3mo). Values are expressed as mean ± SEM. Significances: *P<0.05 and ***P<0.001.
Cardiac autonomic regulation after three months of fingolimod treatment
The average RR-interval was still longer at 3mo than at baseline (P<0.001), but shorter as compared to 1d (P<0.01) (Table 1, Figure 1). Surprisingly, SDNN (P<0.01) (Figure 2), total power (P<0.01), VLF (P<0.001), LF (P<0.001) as well as HRV measures mirroring cardiac parasympathetic regulation (pNN50, P<0.01; rMSSD, P<0.01; HF, P<0.001) were lower at 3mo as compared to baseline (Table 1).
Cardiac autonomic regulation between genders during three months of fingolimod treatment
Men and women were similar with respect to age (43.9 ± 7.5 years vs 42.4 ± 13.5 years), EDSS (3.3 ± 1.4 vs 3.5 ± 2.1), RRMS disease duration (8.9 ± 6.4 years vs 12.4 ± 7.0 years), systolic blood pressure (133 ± 12 mmHg vs 133 ± 11 mmHg) and diastolic blood pressure (82 ± 6 mmHg vs 83 ± 13 mmHg) at baseline, respectively.
The average RR-interval was similar between men and women at baseline (866 ± 155 ms and 798 ± 103 ms), 1d (947 ± 119 ms vs 898 ± 103 ms) and 3mo (890 ± 132 ms vs 869 ± 109 ms), respectively.
There were no differences in HRV measures between genders at baseline or 1d. However, at 3mo HRV measures mirroring cardiac parasympathetic regulation such as pNN50 (3.43 ± 3.34% vs 8.03 ± 3.43%; P<0.05) and HFnu (20 ± 8 vs 30 ± 12; P<0.05) were significantly lower in men than in women. Correspondingly, at 3mo HRV measures mirroring cardiac sympathetic regulation (LFnu 79 ± 9 vs 68 ± 13; P<0.05) and sympathovagal balance (LF/HF ratio 4.6 ± 2.1 vs 2.7 ± 1.2; P<0.05) were higher in men as compared to women.
Discussion
We showed that fingolimod therapy influences cardiac autonomic regulation in patients with RRMS. We found increased HRV after the first dose of fingolimod whereas a decrease in HRV was seen after three months of continuous dosing with fingolimod. In addition, fingolimod seemed to elicit gender-dependent alterations in HRV.
The previously reported initial cardiac effects of fingolimod through S1P1 receptor agonism resemble that of muscarine M2 receptor activation by the parasympathetic nervous system.7,8 Consequently, the initiation of fingolimod results in slowing of the heart rate, slowing of atrioventricular conduction and prolongation of the myocardial refractory period, all suggestive of increased cardiac parasympathetic regulation.19,20 In this study, we demonstrated that S1P receptor modulation by fingolimod increases HRV and particularly its parasympathetic components in patients with RRMS. This finding further emphasises the initial vagomimetic effects of fingolimod.
Interestingly, at three months HRV and its parasympathetic components were lower as compared to baseline. As is known, continuous dosing with fingolimod results in the downregulation of S1P1 receptors and a subsequent shift in the S1P receptor profile towards predominance of S1P2 and S1P3 receptors. 10 An altered S1P receptor profile has been suggested to be responsible for the increase in blood pressure via arterial vasoconstriction during long-term fingolimod treatment.21–23 Accordingly, the shift in the S1P receptor profile may also explain the withdrawal of parasympathetic activation and the shift of cardiac autonomic regulation towards sympathetic predominance during the continuous dosing of fingolimod.
Unexpectedly, in our study the decrease in HRV indicative of increased cardiac sympathetic regulation at three months was accompanied by a prolonged RR-interval (equal to lower heart rate and increased parasympathetic regulation). Usually, the decrease in HRV tends to associate with a shorter RR-interval (lower heart rate) and vice versa. 16 Our finding reinforces the established concept that HRV provides additional information regarding cardiac autonomic regulation and cannot be considered as a surrogate for heart rate. 24 Indeed, our study indicates that in spite of the partial recovery of the RR-interval, the physiology of heart beat regulation becomes fundamentally influenced by fingolimod.
Although fingolimod has been considered to be well tolerated in eligible RRMS patients certain precautions remain for patient selection due to cardiac safety concerns.25,26 Correspondingly, the long-term effects of enhanced cardiac sympathetic regulation associated with fingolimod treatment are not known, especially when the fingolimod-treated RRMS patients get older and the risk of cardiovascular diseases increases. Decreased HRV, suggestive of enhanced sympathetic regulation, predicts an increased risk of subsequent cardiac events in the general population. 14 In addition, decreased HRV is an established risk factor for malignant arrhythmias and sudden cardiac death, particularly in post-infarction patients.12,13 Whether HRV has prognostic value also in RMMS patients treated with fingolimod is beyond the scope of this study.
Gender-dependent differences in HRV have previously been reported in healthy subjects although the reason for this has not been fully established.27,28 In our study, HRV demonstrated higher parasympathetic cardiac autonomic regulation among women as compared to men at three months, although the RR-interval remained similar between the genders during the study. This suggests that continuous dosing with fingolimod results in a different balance of cardiac autonomic regulation between the genders.
All the patients were followed for at least six hours after the first dose of fingolimod according to the safety instructions of the accepted drug label. None of the patients needed overnight observation in the hospital. Although patients were ambulatory, physical inactivity during the in-hospital period might have resulted in increased parasympathetic components of HRV at the day of fingolimod initiation. However, ECG at baseline and at three months was undertaken out of hospital during normal daily activities. A relatively small sample size and the lack of a control group are also recognised but each patient served as her/his own control during the follow-up. We consider that these limitations do not significantly confound the interpretation of results.
Conclusion
The initiation of fingolimod results in enhanced cardiac parasympathetic regulation in the short term, whereas continuous dosing with fingolimod shifts cardiac autonomic regulation towards sympathetic predominance, particularly in men. In general, the sympathetic predominance of cardiac regulation is associated with impaired outcome. Whether this is also true in RMMS patients warrants careful follow-up of these patients.
Footnotes
Conflict of interest
SS has been congress representative of Mikkeli Central Hospital and is sponsored by industry (BiogenIdec, Boehringer Ingelheim, Genzyme, GlaxoSmithKline, Novartis, OrionPharma, Sanofi, TEVA) and is a speaker in symposiums sponsored by industry (BiogenIdec, Novartis, TEVA).
PH has been congress representative of Kuopio University Hospital and is sponsored by industry (Medtronic, TEVA, Genzyme), and is a national and local investigator in studies sponsored by industry (Sanofi Aventis, Biogen).
JEKH has been congress representative of Kuopio University Hospital and is sponsored by industry (Biosense Webster, Medtronic, St Jude Medical, Boehringer Ingelheim, MSD), is a national and local investigator in studies sponsored by industry (Astra Zeneca, Medtronic, St Jude Medical, Biosense Webster, Boehringer Ingelheim), is a speaker in symposium sponsored by industry (Cardiome AG, MSD, Astra Zeneca) and is a member of advisory boards of industry (Pfizer, Lilly, MSD, Astra Zeneca, Bayer, BMS).
TL, TML and TT report no conflicts of interest.
Funding
This work was supported by the government (grant number 12178).