
Abstract
Background:
Onset of multiple sclerosis (MS) is typically in early adulthood. The impact, if any, of menopause on the MS course is unknown. Our objective was to determine whether menopause is associated with changes in MS severity in a longitudinal clinical cohort.
Methods:
Responses from an ongoing reproductive questionnaire deployed in all active female CLIMB observational study participants with a diagnosis of clinically isolated syndrome (CIS) or MS were analyzed when the response rate was 60%. Reproductive data were linked with clinical severity measures that were prospectively collected every six months, including our primary measure, the Expanded Disability Status Scale (EDSS).
Results:
Over one-half of the respondents (368 of 724 women) were postmenopausal. Median age at natural menopause was 51.5 years. In our primary analysis of 124 women who were followed longitudinally (mean duration 10.4 years) through their menopausal transition (natural or surgical), menopause represented an inflection point in their EDSS changes (difference of 0.076 units; 95% CI 0.010–0.14; p = 0.024). These findings were not explained by vitamin D levels, nor changes in treatment or smoking status over this period. There was no effect of hormone replacement therapy (HRT) exposure, but HRT use was low.
Conclusions:
We observed a possible worsening of MS disability after menopause. Larger cohorts are required to assess any HRT effects.
Keywords
Introduction
There is emerging evidence of an impact of menopausal status on neurologic decline, both in healthy women and in women with neurologic diseases.1–3 Studies of menopause, and in particular of the sudden declines in estradiol occurring with early bilateral oophorectomy, have highlighted an increased risk for cognitive deterioration and dementia, including Alzheimer Disease. 4
In multiple sclerosis (MS), a disease characterized by both a neuroinflammatory and a neurodegenerative component, there is an age-related increase in disability and conversion to a progressive course, observed around the age of 45. 5 While many factors may contribute to this phenomenon, there are important gender differences in MS risk and course. 6 Men often have a more progressive and aggressive MS course, but in individuals with disease onset after age 50 there is a narrowing of gender differences in the disease course, 7 invoking a role for gender-specific changes 8 around this time, such as reproductive aging.
Investigating the potential impact of menopause in MS is of high relevance, as the onset of MS is typically during the reproductive years; hence, most women will undergo the potentially modulatory menopausal window after MS onset. Previous approaches to assessing the impact of menopause in MS include:
Comparison of male and female disability and brain atrophy in individuals, prior to and after the age of 50 9 ;
Reports of the association between early, surgical menopause-based patient-reported disability scores in an online research platform cohort 10 ; and
Patient assessments of menopausal impact on MS symptoms (40–54% of women reported symptom worsening, in two small cross-sectional studies,11,12 but not in a larger one 13 ).
In this study, we hypothesized that menopause accelerates the accumulation of disease burden in women with MS. Because known gender differences in disease course, as well as age-related changes, could obscure the impact of gender-specific changes in trajectory, 8 we chose not to compare women to men, as was previously done. 9 Instead, we examined the impact of menopause on individual women’s MS course, in a well-characterized cohort of women followed longitudinally with serial examinations through their menopausal transition.
Materials and methods
Study design
We performed a retrospective analysis of the impact of reported menopausal status on prospectively collected measures of MS course.
Subjects
The Comprehensive Longitudinal Investigation of MS at the Brigham and Women’s Hospital (CLIMB) study was initiated in the year 2000, and has enrolled 2098 patients who were cared for at the Partners MS Center (www.climbstudy.org). Patients underwent standardized clinical exams, magnetic resonance imaging (MRI) and blood collection. Female subjects completed a one-time epidemiologic questionnaire, including reproductive history (Table 1). We selected women aged ⩾ 18, who met the 2005 McDonald diagnostic criteria for MS 14 or clinically isolated syndrome (CIS).
Demographic and menopause characteristics of study subjects. a
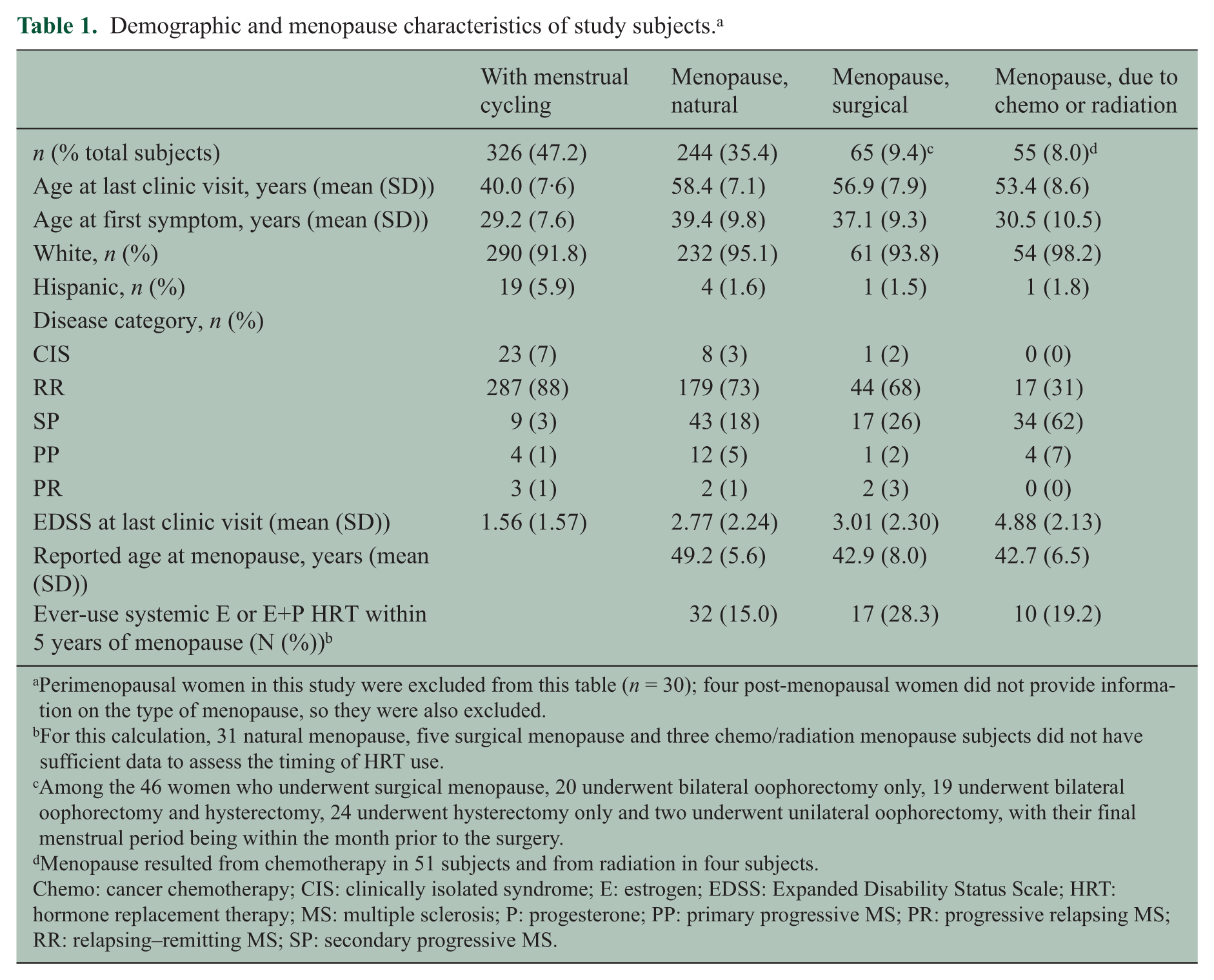
Perimenopausal women in this study were excluded from this table (n = 30); four post-menopausal women did not provide information on the type of menopause, so they were also excluded.
For this calculation, 31 natural menopause, five surgical menopause and three chemo/radiation menopause subjects did not have sufficient data to assess the timing of HRT use.
Among the 46 women who underwent surgical menopause, 20 underwent bilateral oophorectomy only, 19 underwent bilateral oophorectomy and hysterectomy, 24 underwent hysterectomy only and two underwent unilateral oophorectomy, with their final menstrual period being within the month prior to the surgery.
Menopause resulted from chemotherapy in 51 subjects and from radiation in four subjects.
Chemo: cancer chemotherapy; CIS: clinically isolated syndrome; E: estrogen; EDSS: Expanded Disability Status Scale; HRT: hormone replacement therapy; MS: multiple sclerosis; P: progesterone; PP: primary progressive MS; PR: progressive relapsing MS; RR: relapsing–remitting MS; SP: secondary progressive MS.
Reproductive survey
The reproductive questions were piloted in 140 female subjects (data not included in the current analyses) and then modified for clarity. The revised survey (Supplementary Table 1) was then deployed through a phased combination of modalities, depending on whether the subjects were previous or new enrollees in CLIMB (Supplementary Figure 1 has the launch, mailer and clinic-based phases). Subjects could respond on paper or via a secure website; also, 13 subjects responded by telephone or in person.
The responses to the revised questionnaire received by 20 June 2014 were analyzed (these were 60% of the total eligible cohort of 1210). We verified the ambiguous or unusual responses (e.g. menopausal age outside the typical parameters of 42–58 years old), by both reviewing the longitudinal medical record and re-contacting subjects if necessary.
Reproductive variables
Menopausal status was categorized as still cycling, perimenopausal (last menses in the 3–12 months prior to survey) or postmenopausal (either no menses in the prior 12 months, or loss of menses due to surgical intervention). Menopausal type was categorized as resulting from natural physiology, surgical intervention (hysterectomy and/or bilateral oophorectomy), or chemotherapy or radiation. In postmenopausal women, the menopausal type was considered natural if menses continued after unilateral oophorectomy and surgical if they ceased (n = 2). Date was defined as the last menstrual period beyond which no menses occurred for 1 year (natural), or was associated with the date of surgery (surgical), according to the Stages of Reproductive Aging Workshop + 10 guidelines. 15 Hormone replacement therapy (HRT) use was categorized dichotomously for type (estrogen and/or progestogens versus other types (black cohosh, testosterone, etc.), administration (systemic (patch + oral) versus local (gel, cream and ring)) and the timing of initiation (whether initiated within five years of menopause 16 ).
To validate patient reports, we first reviewed surveys from a randomly selected subset of 20 subjects receiving primary and gynecological care at our hospital against the medical record, and found a concordance of 100% for menopause status, 90% (two were within one year) for year, 100% for menopause type and 100% for systemic HRT ever usage.
Outcomes
The primary outcome measure was the Expanded Disability Status Scale (EDSS), 17 scored prospectively by MS clinicians every six months. The secondary outcomes included:
The EDSS Functional Systems scores;
The Timed 25-Foot Walk (T25FW) 18 (with any subject unable to walk or with a walk time > 50 seconds classified as ‘50’); as well as
Patient-reported outcomes (PRO) measures, completed biennially by a subset of CLIMB subjects enrolled in the Quality of Life (QOL) subgroup (n = 262): Short-Form-36 (SF-36) of the General Health Survey of the Medical Outcomes Study, 19 Modified Fatigue Impact Scale (MFIS) 20 and Center for Epidemiological Studies of Depression (CES-D). 21
Ethics statement
Ethical approval for this study was obtained from the Partners Healthcare Human Research Committee Institutional Review Board.
Statistical analysis
We compared respondents’ demographic and disease characteristics at the most recent clinical visit to those of non-respondents, using two sample t-tests and chi-square tests. We characterized menopausal features using descriptive statistics and compared the demographic and menopausal characteristics according to menopausal type, using t-tests and Fisher’s exact tests. Because natural menopause is reported to occur at an earlier age in epilepsy, another neurologic disease affecting young individuals, 22 we estimated the age at natural menopause. We used a Kaplan-Meier curve. The cycling or perimenopausal subjects were censored at the date of the questionnaire; the surgery and chemotherapy/radiation-induced menopausal subjects were censored at their date of menopause. We preferred censoring subjects with surgical and chemotherapy/radiation-induced menopause over a competing risk analysis, since they would have gone through natural menopause after the date of induced menopause, if other interventions had not been required.
In our primary assessment of the impact of menopause on MS disease severity, we used an inflection point analysis examining longitudinal changes in EDSS in women followed through their menopausal transition. This pre-specified primary model examines within-subject changes. Using only subjects who had at least one EDSS score before and after their date of menopause (n = 124), we assessed whether menopause represented an inflection point in a subject’s disease trajectory, by performing a linear spline mixed effects model with a change in the slope at the time of menopause.
The random effects in this model were a random intercept, slope and change in slope after menopause, and an unstructured covariance matrix among the random effects was assumed. 23 The time scale for this analysis was in years. We further separated subjects into a natural menopause group (n = 101), a surgical menopause group (n = 23), and a surgical menopause subset who had undergone bilateral oophorectomy (n = 11); and the same model was refit. We excluded women reporting menopause induced by chemotherapy (because aggressive MS disease may result in chemotherapy use and subsequent menopause, confounding the effect of menopause on disease severity 24 ) and by radiation (which would give potentially altered ovarian physiology). To ensure that the results were robust to the assumptions of linear mixed models, we refit the models using a mixed ordinal logistic regression model. In secondary analyses, we used the same approaches for each EDSS Functional Systems score and each of the PROs.
To assess potential confounders, we performed additional variations on this primary model. First, to assess the impact of vitamin D level, subjects with a vitamin D measurement within two years of menopause (n = 37) were identified, and the seasonally adjusted vitamin D level was added as a fixed effect to the inflection point analysis. Second, to assess the impact of smoking or MS disease modifying therapy (DMT), we restricted the model to subjects who did not change smoking status (n = 115) nor DMT type (n = 22) during the follow-up period. Finally, we performed an exploratory analysis to assess whether HRT protects against disease worsening after menopause by including a main effect for HRT use (systemic estrogens and/or progestogens, given within five years of menopause versus never used); and interaction between HRT use and the post-menopausal change in slope, with the interaction term serving as the focus of the analysis.
To further distinguish the effects of menopause from the effects of aging, we examined longitudinal changes in women aged 35–45 who were either cycling (n = 225) or had undergone surgical menopause (n = 26, including 10 with bilateral oophorectomy). In these subjects, we included a linear effect for age, as well as a quadratic effect of age to allow EDSS changes to accelerate with normal aging. We added a change in the linear term at the onset of menopause in the women who experienced surgical menopause, corresponding to a change in the slope of the quadratic effect after the onset of menopause.
Statistical analyses were performed using the software program R version 3.0.2. (www.r-project.org).
Results
Respondent characteristics
A total of 724 subjects returned questionnaires within the study time frame, out of the 1210 subjects who received the questionnaire, for a response rate of 60%. Respondents were older at survey completion, but did not differ in other demographic characteristics nor, importantly, in EDSS or disease type, from the non-respondents (p > 0.10; Supplementary Table 2).
Menopausal characteristics
Over one-half of respondents were post-menopausal (50.8%). Menopause was natural in 67.0% of the post-menopausal respondents. The median age at natural menopause was 51.5 years (95% CI 50.8, 52.4) (Figure 2). Women with surgical menopause reported a younger average menopausal age than women with natural menopause (42.9 versus 49.2 years, p < 0.001) and higher rates of HRT use (28.3% versus 15.0%, p = 0.02).
Changes in MS course at menopause
In our primary inflection point analysis, we assessed whether the rate of disability accumulation changes after menopause, in 124 subjects (characteristics summarized in Supplementary Table 3) followed through the menopausal transition, for a mean of 10.4 years (SD = 2.5; range 1.5–17.0). The mean (SD) duration of follow-up pre-menopause was 5.4 (3.3) years, and the mean (SD) duration of follow-up post-menopause was 5.1 (3.1) years. The rate of EDSS change increased from 0.051 units per year before menopause, to 0.13 units per year after menopause (difference of 0.076 units; 95% CI 0.010, 0.14; p = 0.024) (Figure 1). A similar effect was observed in the natural and surgical menopause groups, but the effect was not statistically significant in any of the groups, potentially due to the reduced sample size. In the natural menopause group, the estimated increase in slope was 0.055 units (95% CI − 0.016, 0.126; p = 0.13); in the surgical menopause group, the estimated increase in the slope was 0.17 units (95% CI − 0.037, 0.37; p = 0.11). Similar results were observed in the mixed effects ordinal logistic regression model. When we assessed the individual EDSS Functional Systems, we only found a significant inflection point for the visual function (p = 0.048, Table 2) but this was not significant after adjustment for multiple comparisons (Bonferroni correction: p = 0.05/8). Additionally, there was no significant inflection point for the T25FW (p = 0.26), or any PRO (Supplementary Table 4).
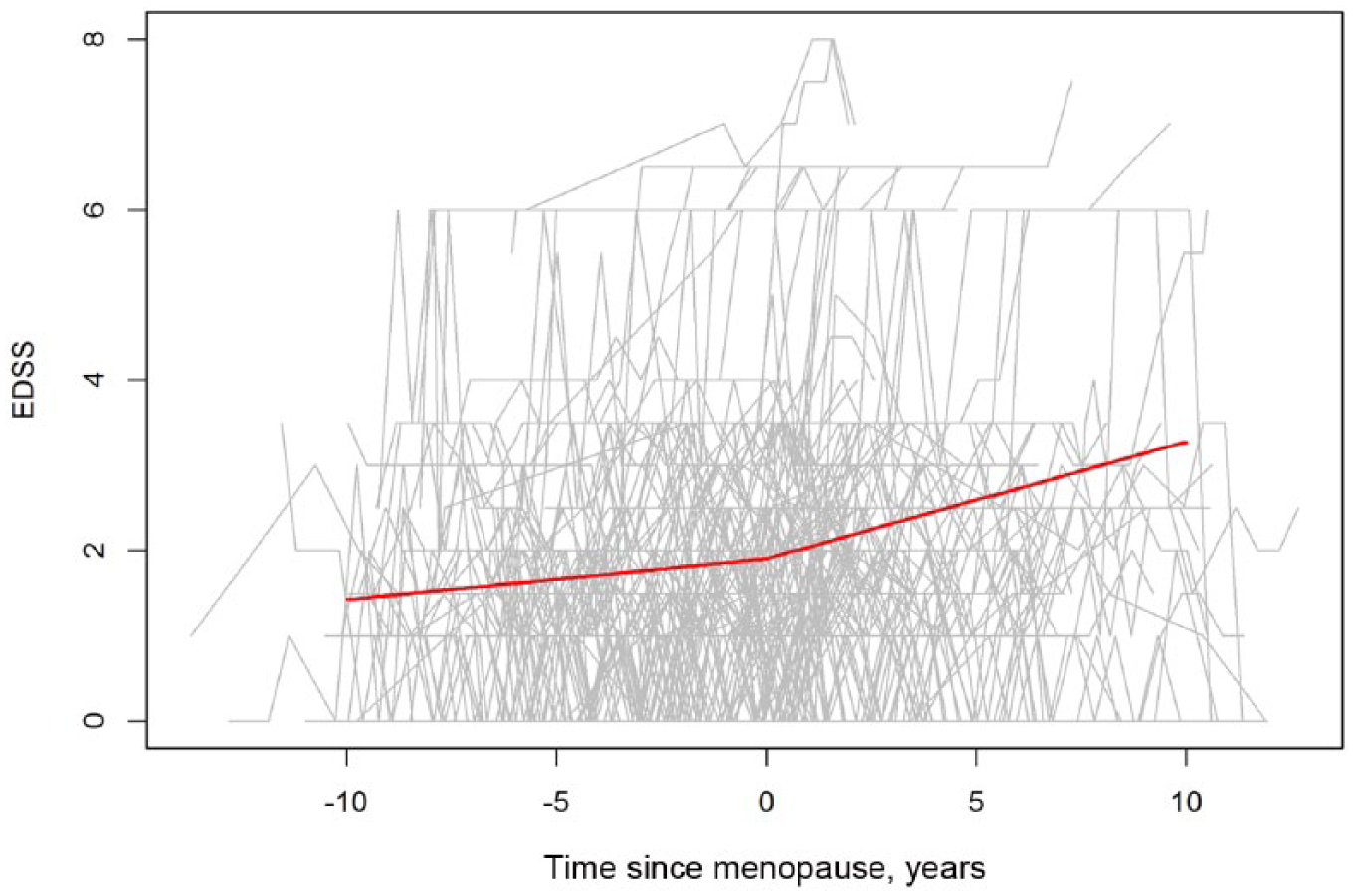
EDSS score trajectory for each subject is provided (gray lines). The thick solid line reflects the estimated population line. Only subjects with observations before and after the onset of menopause were included (n = 124).
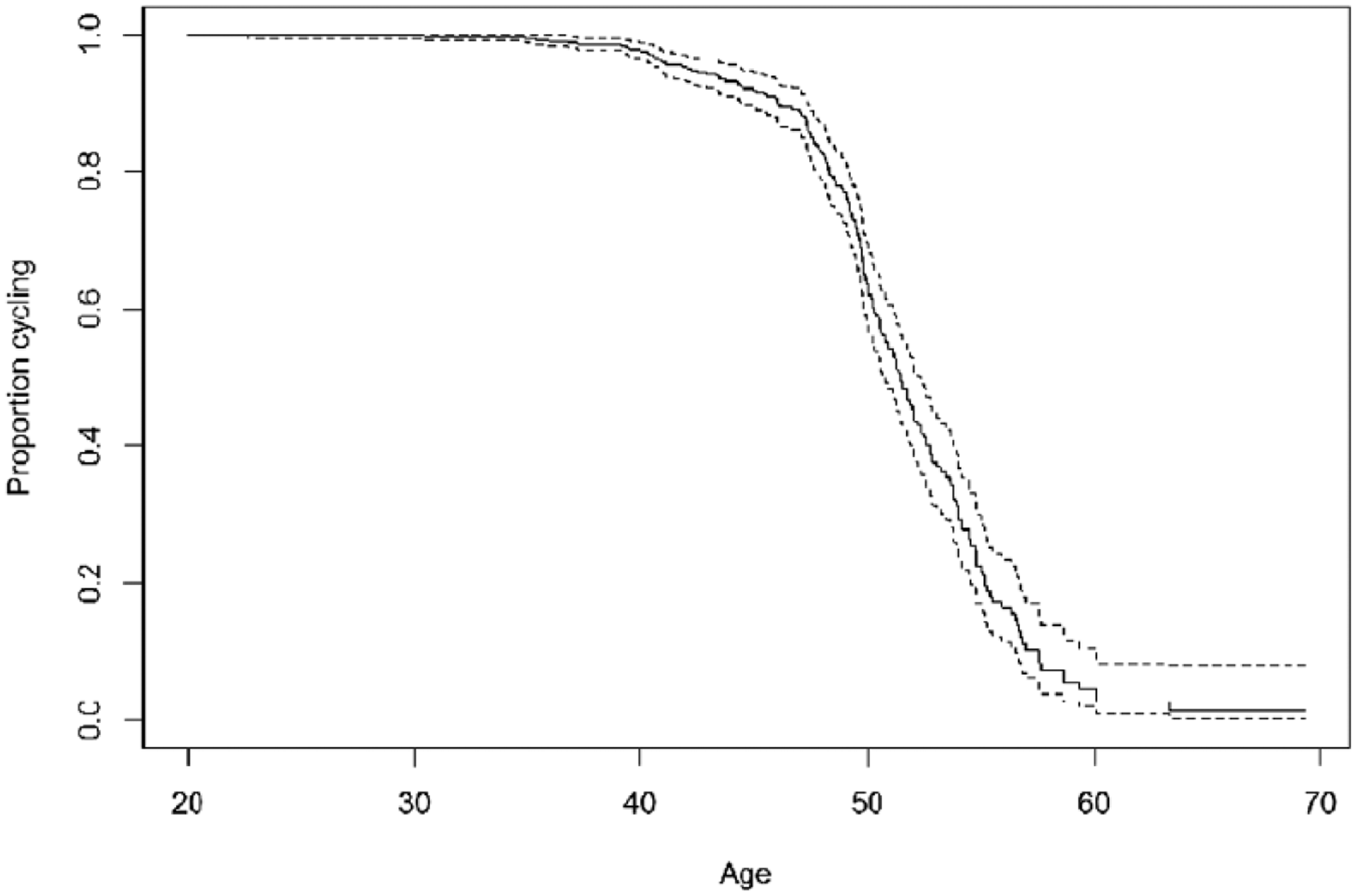
Distribution of Age at Natural Menopause in a large clinical cohort of women with MS.
Inflection point analysis for functional systems scores, in women followed longitudinally through their natural or surgical menopause (n = 124).
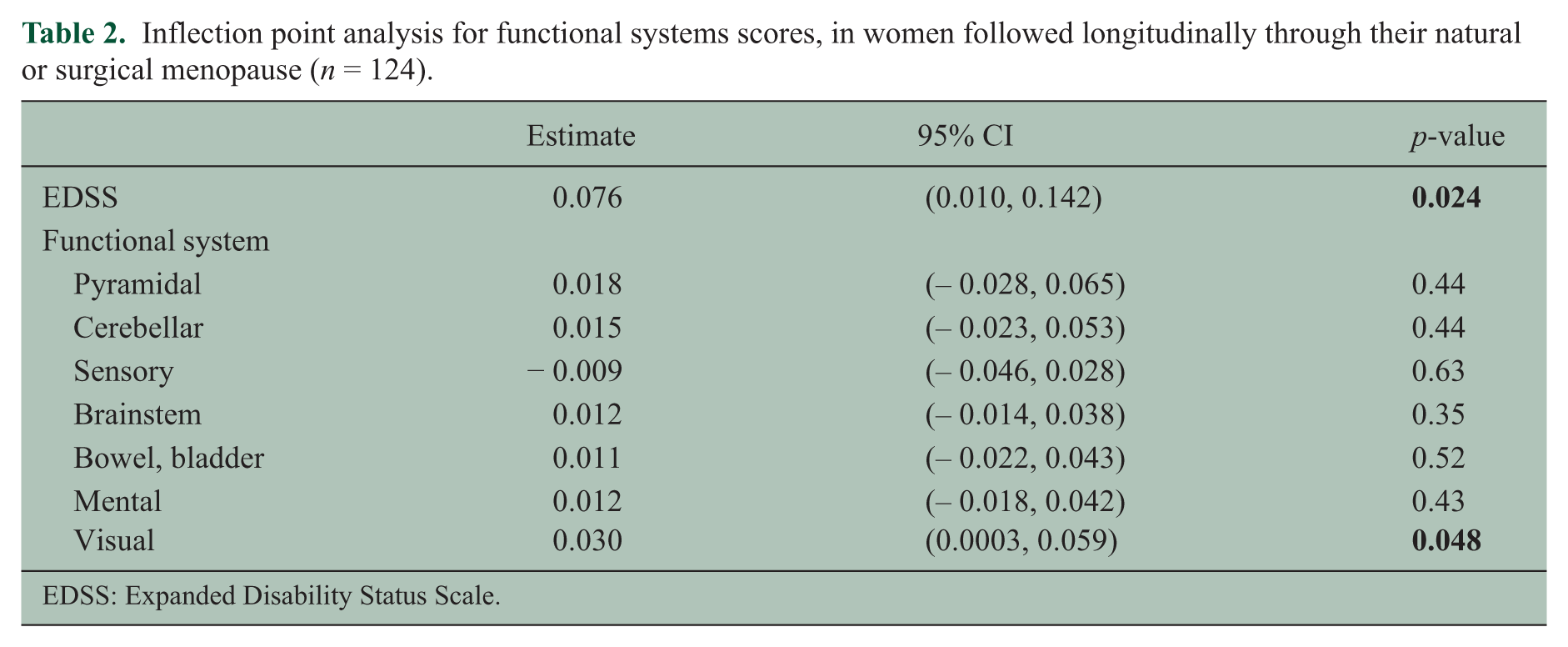
EDSS: Expanded Disability Status Scale.
To explore potential confounders, we performed modifications to this model. First, using seasonally adjusted vitamin D levels did not significantly alter the conclusions of our analysis, but the inflection point was not statistically significant in the subset of subjects with a vitamin D measurement. When we restricted our analysis to subgroups of subjects with consistent smoking status or DMT status, the change in slope was still observed (Smoking: n = 115; change in slope = 0.093 units; 95% CI 0.02, 0.16; p = 0.011and for DMT status: n = 22; change in slope = 0.083 units; 95% CI − 0.03, 0.19; p = 0.15). The interaction term between HRT use and change in EDSS slope at menopause was not significant (p = 0.38).
We then sought to further distinguish the effects of natural aging from those of loss of ovarian function, and restricted our analysis to younger women (aged 35–45) who were either cycling (n = 225) or had undergone surgical menopause (n = 26). In this group, the indications for surgical intervention included one borderline mucinous ovarian tumor, but they were mostly benign (fibroids (n = 10), endometriosis (n = 3), benign ovarian growths (n = 3), family history of malignancy (n = 3), dysfunctional uterine bleeding (n = 2) and other (n = 2)); i.e. most indications were not related to systemic illnesses that might confound our results. Similar to our primary analysis, we found that menopause led to a change in the EDSS trajectory after menopause: The change in the linear term of the model after menopause was 0.12 (95% CI 0.010, 0.24; p = 0.034). Tempering this result, we found that the removal of one subject whose EDSS increased significantly after menopause resulted in a p-value of 0.38.
Discussion
In this study, we assessed the impact of menopause on disease severity in a well-described clinic-based cohort and in our primary analysis involving 124 women followed for a mean of 10.4 years, through their menopausal transition. We noted that the standard clinical severity outcome, EDSS, seemed to change more rapidly after menopause.
To our knowledge, no other studies have examined longitudinal changes in objective clinical severity associated with menopause. We previously reported that in MS onset after the age of 50, women’s disease trajectories are more similar to those of men, than in individuals with onset of MS prior to 50; we postulated that the effect of turning 50 (and perhaps menopause) might contribute to a more rapid decline in women, thereafter. 7 Here, while we found a significant inflection point in EDSS scores, we did not note significant changes in individual Functional Systems scores, which is consistent with previous models of sustained clinical progression. 25 The fact that we found similar findings in women who underwent surgical menopause, which occurs earlier than natural menopause, suggested that our findings cannot entirely be attributed to known age-related accumulation of disability, to similar ages at natural menopause and at transition to SPMS, or to accumulation of co-morbidities in women’s later years. Notably, in our sub-analysis of younger women, we observed a significant result, but this result may have been driven by one subject, who experienced dramatic MS worsening after surgical menopause.
While our primary analysis findings were statistically significant, the effect of menopause was modest (about one EDSS point over 10 years). If menopause does lead to even a minor acceleration of disability accumulation in MS, a potential mechanistic effect (and hence, opening up a therapeutic window of opportunity), could be attributed to the loss of the neuroprotection afforded by estradiol, as its levels decline after menopause. Thus, estradiol may provide protection against neurodegeneration, as has been noted in animal models of MS. 26 In healthy women, declines in estradiol at menopause (particularly the sudden declines after surgical menopause) have been linked with longitudinal cognitive decline, 4 which continue to be magnified even into the later years; 27 and hormonal therapies initiated within a perimenopausal window appear to be protective.4,17 Neuroimaging studies might help substantiate neurodegenerative changes.
Because the timing of the CLIMB study (started in 2000) largely coincided with declines in HRT use following the publication of the Women’s Health Initiative results, 28 few of our prospectively followed subjects were treated with HRT. A longer observation period and a larger sample size are required to determine whether or not HRT has neuroprotective effects.
With respect to other hormonal changes associated with menopause, postmenopausal weight gain is typically gradual; and in our CLIMB cohort, higher body mass index (BMI) was not associated with longitudinal worsening in EDSS scores (unpublished data). In the current study, we did not observe an association between vitamin D levels and post-menopausal EDSS changes. Vitamin D levels are commonly assessed at the time of menopause for bone health considerations, with post-menopausal vitamin D levels linked to supplementation. 29 During the observation period of this study, low vitamin D levels also became linked with adverse MS outcomes. 30 For both these reasons, if anything, vitamin D supplementation at the time of menopause would have mitigated our observations on subsequent MS course.
An alternative explanation for our findings could be that menopause does not influence MS, but affects organs that are affected by MS, such as the bladder. We did not find evidence of an effect of menopause on any one individual Functional Systems score, including bladder/bowel scores. While perimenopausal symptoms (e.g. hot flashes or sleep loss) could certainly contribute to worsening function, because these typically start prior to the final menstrual period, 16 they would have contributed to both the pre- and post-menopausal cohorts’ disease severity.
Menopause has been associated with patient-reported worsening of symptoms in 40–54% of women in two small cross-sectional studies,11,12 but not in a larger one. 13 In our prior analysis of menopause outcomes in an on-line MS cohort, surgical menopause was associated with higher cross-sectional patient-reported disability scores, using the MS Rating Scale (MSRS). 10 The MSRS has previously shown reasonable correlations with the EDSS; 31 but in areas other than ambulation, it may be more sensitive than the EDSS to patients’ perceptions of function. In the current study, objective clinical severity was observed to worsen in the post-menopausal subjects, even though PROs did not. It is not clear whether we were underpowered to detect an inflection point in PROs, whether the PROs used in this study were insensitive to changes at menopause, or whether other components of QOL could actually improve with menopause, obscuring an effect of post-menopausal MS changes on PROs.
Our second observation was that the median age of natural menopause of 51.5 years in our cohort was broadly similar to the mean age of natural menopause in Western populations (51 years). 32 This raises the possibility that MS may not adversely impact long-term gonadal function, as is observed in epilepsy, another chronic neurologic disease affecting young individuals. 32
The menopausal transition involves a series of stages of hormonal fluctuations and symptomatic changes 16 ; and longitudinal follow-up is required, because menopause can occur over a wide range of ages. The strengths of this study included the use of a detailed questionnaire, and inclusion of disease severity scores (EDSS and PRO) collected prospectively by clinicians and patients blinded to study hypotheses. Additionally, the spline analysis permitted an assessment of the change in disease trajectory at the time of menopause, regardless of disease type and duration, or other prognostic factors in MS (e.g. DMT use or smoking).
An underlying limitation is the biases inherent in patient-reported data. The CLIMB study provided several opportunities for data validation, including verifying reported reproductive histories with medical records, in a random sample, when possible. Similar mean ages of our subjects at survey response and at natural menopause may also partially mitigate recall biases. Second, even though our response rate of 60% was comparable or greater to other large MS-based reproductive questionnaires (45%) 33 and surveys, 34 the older average age of respondents does raise the possibility of responder biases. Importantly, respondents did not differ from non-respondents in terms of disease type or EDSS.
A third limitation is that by categorizing women undergoing hysterectomy but with preserved ovaries as post-menopausal, we may have attenuated the association between menopause and/or surgical menopause, and MS outcomes. Additionally, the exclusion of subjects with chemotherapy-induced menopause limited our ability to determine whether menopause impacts disease course, in patients for whom chemotherapy may have been prescribed for aggressive disease.
Caution must be taken when generalizing the results of this study to other cohorts. Because many CLIMB subjects enroll at or shortly after first presentation to the MS Center, and because of prescribing patterns in a specialized MS clinic, the subjects in this study may have a lower overall burden of disability than subjects in population-based settings. It is not clear whether this feature affected our sensitivity to detect an even larger inflection point in EDSS at menopause, or limited our ability to detect even greater effects in populations with more disease burden. Lastly, we did not assess the effects of race, education or other variables, which may be considerations for future studies.
Given an aging population and a median age of individuals currently living with MS that is very close to menopausal age, potentially modifiable changes occurring at menopause might impact the trajectory of many patients with MS. In addition to validating our findings in additional cohorts, the potential impact of HRT should be further investigated.
Footnotes
Acknowledgements
The authors are grateful to the patients participating in the CLIMB study who contributed their data and time to this project. The authors wish to thank the following colleagues at the Brigham and Women’s Hospital: Emily Greeke and Grace Little for their administration of the questionnaires, Mariann Polgar-Turcsanyi for her role in managing the Partners MS Center research database, as well as Nafiseh Alsharif and Taylor Saraceno for their research assistance.
Conflict of interest
Authors R Bove and A Musallam report no conflicts of interest; BC Healy has received research support from Merck Serono and Novartis; BI Glanz has received research support from Merck Serono; PL De Jager has received research support and speaker honoraria from Biogen-Idec and consultation fees from Teva Neuroscience. T Chitnis has served as a consultant for Biogen-Idec, Sanofi Aventis, Novartis and Alexion; and she has received grant support from Merck-Serono and Novartis for unrelated activities.
Funding statement
This work was supported by the National Multiple Sclerosis Society (grant number RG-4256A4/2 to TC), the National Multiple Sclerosis Society/American Brain Foundation (Clinician Scientist Award FAN 1761-A-1 to RB) and the NIH (grant number 5K12HD051959-09 BIRCWH Scholar Award to RB).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.