
Abstract
Background:
Only limited data are available on whether glatiramer acetate exposure during pregnancy has an effect on perinatal outcome.
Objective:
To determine the effect of glatiramer acetate exposure during pregnancy on pregnancy outcomes in women with multiple sclerosis.
Methods:
We compared the outcome of pregnancies of women with multiple sclerosis exposed to glatiramer acetate with pregnancies unexposed to disease-modifying therapies. Women were enrolled into the German Multiple Sclerosis and Pregnancy registry. A standardized questionnaire was administered during pregnancy and postpartum. Detailed information on course of multiple sclerosis and pregnancy, concomitant medications, labor, delivery, and outcome of pregnancy was obtained.
Results:
We collected data on 246 multiple sclerosis pregnancies, 151 exposed to glatiramer acetate and 95 unexposed to disease-modifying therapies during pregnancy. Three (2.2%) congenital anomalies occurred in the exposed and 6 (6.7%) in the control group. We did not observe an increase in other adverse pregnancy or delivery outcomes including spontaneous abortions, preterm birth, Cesarean sections, or reduced birth weight in the exposed group.
Conclusion:
Our data provide further evidence that glatiramer acetate exposure during the first trimester of pregnancy appears safe and without teratogenic effect. These findings provide important additive knowledge to better counsel women with multiple sclerosis in planning a pregnancy.
Keywords
Introduction
Many patients with multiple sclerosis (MS) start early in the course of the disease with various disease-modifying therapies (DMTs), as early relapse prevention is thought to have favorable effect on the course of the disease.1–4
Young women with MS are not discouraged from getting pregnant but they are advised to discontinue DMTs prior to conceiving due to unknown safety of early pregnancy exposure. 5
Only limited data are available on whether glatiramer acetate (GLAT) exposure during pregnancy is safe.6–13 A systematic review identified 97 GLAT-exposed pregnancies from eight studies and found no safety signals on the outcome of pregnancy, labor, or delivery. The authors considered the results as not compelling due to small sample size. 5 Teva Pharma, the GLAT manufacturing company, had never published their post-marketing pregnancies in a scientific manuscript but reported on a conference abstract no adverse pregnancy outcomes. 13 All available published studies are limited by a small sample size.
Therefore, the objective of this prospective cohort study was to determine safety of GLAT exposure during early pregnancy on fetal outcome in comparison to women with MS unexposed to any DMTs during pregnancy.
Methods
Participants
A total of 246 pregnant women with relapsing remitting MS 14 who voluntarily enrolled in the nationwide German Multiple Sclerosis and Pregnancy registry (Deutschsprachiges Multiple Sklerose und Kinderwunsch Register (DMSKW)) during pregnancy between 2008 and 2013 were collected. Enrollment was possible at any time point during pregnancy. Women responded to advertisements or were actively recruited by their treating clinicians or MS nurses. The details of the registry established in 2006 are published elsewhere. 15 The registry is supported by industry funding, but the sponsors have no role in the registry design, data collection, analyses, or dissemination of results. The registry is approved by the local institutional review board of the Ruhr University Bochum (314108) and all women gave their written informed consent.
Data collection
Women are contacted after study entry, each remaining trimester of pregnancy, the first 6 weeks and months 3 and 6 postpartum to complete a structured, interviewer-administered questionnaire by phone or in-person during visits to our outpatient clinic. During pregnancy, a detailed history of MS (diagnosis, disease activity, treatments) and reproductive history are obtained along with exposure to other toxins as alcohol, tobacco, or recreational drugs. Follow-up interviews obtained information on the state of pregnancy, any alteration in pregnancy status, type of delivery, outcome of pregnancy, medication, and wellbeing of the child.
Definition of exposures
GLAT-exposed pregnancies were defined as last injection administered after the last menstrual period (LMP). A pregnancy was considered unexposed to DMTs if (1) the last injection of GLAT or interferon-beta was administered any time before the LMP, (2) the last infusion of natalizumab was given more than 3 months before the LMP, (3) the last dosage of fingolimod was given more than 2 months before the LMP, (4) if the last infusion of rituximab was given more than 4 months before the LMP, (5) the last dosage of azathioprine was given any time before the LMP, or (6) the woman had never been treated with DMTs. All definitions of exposure are based on five half-life times of the molecule. 16
Maternal smoking status was defined as smoking (in any trimester yes/no). The body mass index (BMI) from the expectant mothers’ record of prenatal and natal care at the beginning of pregnancy was defined as the weight in kilograms divided by the square of the height in meters (kg/m2). Steroid exposure during first trimester (yes/no) and any steroid use during any trimester of pregnancy (yes/no) were obtained.
Definition of outcomes
The primary outcome was defined as live birth with one or more congenital anomalies (CAs). CA was specified as a defect in organogenesis, major CA as structural defects of the body and/or organs that impair viability and require intervention. Minor CA was defined as small structural developmental disturbances that do not impair viability and do not need to be treated. 17 CAs were rated and classified in accordance with the guidelines of EUROCAT (European surveillance of CAs) 18 by a teratologist (A.Q.W.). Other outcomes were defined as follows: spontaneous abortion: fetal loss before 22 completed gestational weeks (gw); 19 fetal death: fetal loss 22 gw or fetal weight of >500 g; 19 early neonatal death: death of the newborn occurring during the first 7 days of life (0–6 days); 20 and preterm delivery: live birth less than 37 completed gw. 21 Elective abortion and ectopic pregnancies were also documented. Birth weight and birth length of the newborns were analyzed as reported in the expectant mothers’ record of prenatal and natal care. For any adverse outcome in the newborns, the treating pediatrician was contacted to verify the medical problem.
Statistical analysis
Means and standard deviation (SD) for the descriptive statistics were compared using the two-sided t-test if the continuous variables were normally distributed. In case of non-normality distributed continuous variables, the Wilcoxon rank sum test was used and chi square/Fisher test to assess differences between categorical variables.
We used multivariate logistic regression to estimate the crude odds ratio (OR) with 95% confidence intervals (CIs) to compare GLAT-exposed pregnancies to non-DMT-exposed pregnancies for binary outcomes and linear regression to compare birth weights and length of full-term newborns among the two groups.
We also assessed propensity score (PS) adjusted logistic regression, as a method of observational studies to account for bias in a choice of treatment or behavior (in our case being exposed to GLAT) in a non-randomized setting. 22 We controlled for sufficient overlap in the PSs between GLAT-exposed and unexposed women. PS quintiles were then used in the logistic regression model.
We considered the following potential confounders in the multivariate model for all outcomes: age at conception, disease duration, BMI, smoking during pregnancy (yes/no), relapse 23 during pregnancy (yes/no), steroid use during any trimester of pregnancy due to MS relapses (yes/no), steroid use during first trimester (yes/no), gw of entry into the cohort (categorized around the median), and preterm birth (yes/no) for the outcome C-section. If a covariate demonstrated an association with both the exposure and outcome (p < 0.2) it was considered as a confounder. A two-sided p-value of <0.05 was defined as statistically significant. All statistical analyses were conducted using SAS version 9.2 (SAS Institute, Cary, NC).
Results
Study sample
We collected data on 246 pregnancies of women with MS exposed to GLAT (n = 151) or without DMT exposure during pregnancy (n = 95) from January 2008 to December 2013. No woman was lost to follow-up.
A total of 151 pregnancies were exposed to GLAT during pregnancy with a median duration of 31.0 (range = 0–154) days. The vast majority (n = 148) of GLAT-exposed women stopped treatment during the first pregnancy trimester; only 3 women stopped GLAT during the second trimester.
We included 95 non-DMT-exposed pregnancies as a control group. We did not observe significant differences in basic demographics between the two groups (Table 1). Women exposed to GLAT joined the cohort earlier then unexposed women. A total of 67 (70.5%) women in the control group were treated with DMT prior to pregnancy, but had stopped treatment in advance to pregnancy. Most (n = 39; 41.1%) were treated with interferon-beta, 17 (17.9%) with GLAT, 7 (7.4%) with natalizumab, 2 (2.1%) with fingolimod, 1 (1.1%) with rituximab, and 1 (1.1%) with azathioprine prior to pregnancy. A total of 28 (29.5%) women never received an MS treatment.
Characteristics of the study sample.
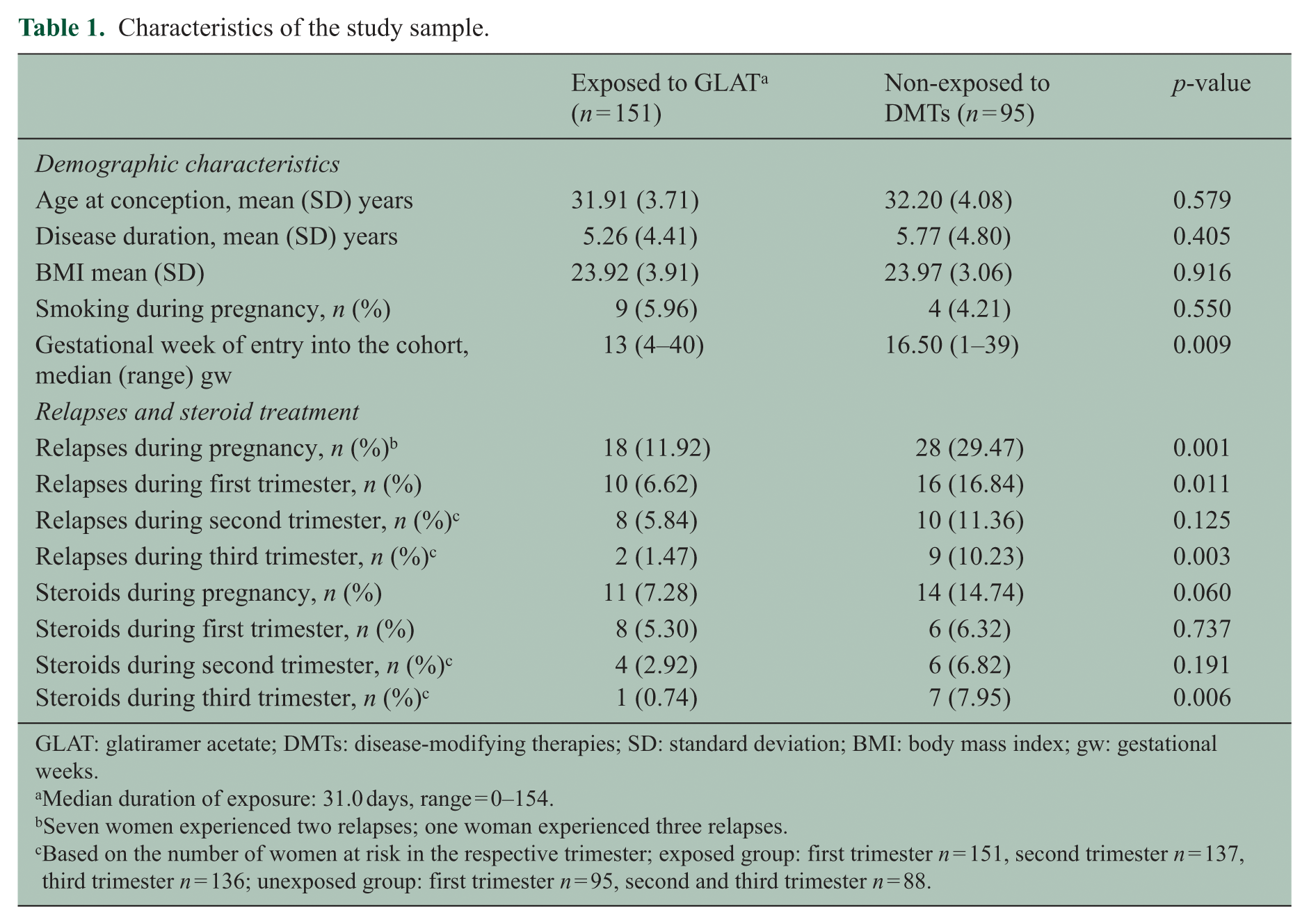
GLAT: glatiramer acetate; DMTs: disease-modifying therapies; SD: standard deviation; BMI: body mass index; gw: gestational weeks.
Median duration of exposure: 31.0 days, range = 0–154.
Seven women experienced two relapses; one woman experienced three relapses.
Based on the number of women at risk in the respective trimester; exposed group: first trimester n = 151, second trimester n = 137, third trimester n = 136; unexposed group: first trimester n = 95, second and third trimester n = 88.
A total of 46 women (18.7%) experienced at least one relapse during pregnancy (Table 1). Women unexposed to DMTs at the onset of pregnancy had significantly more relapses and more corticosteroid treatments during pregnancy than women with early pregnancy exposure to GLAT especially in the first and third trimesters (Table 1).
Pregnancy outcomes after GLAT exposure
We observed 224 live births, 136 exposed to GLAT and 88 in the non-DMT-exposed group. Details of the pregnancy and delivery outcomes are presented in Figure 1. A total of 19 out of 22 pregnancies not resulting in live births were spontaneous abortions in the first trimester.
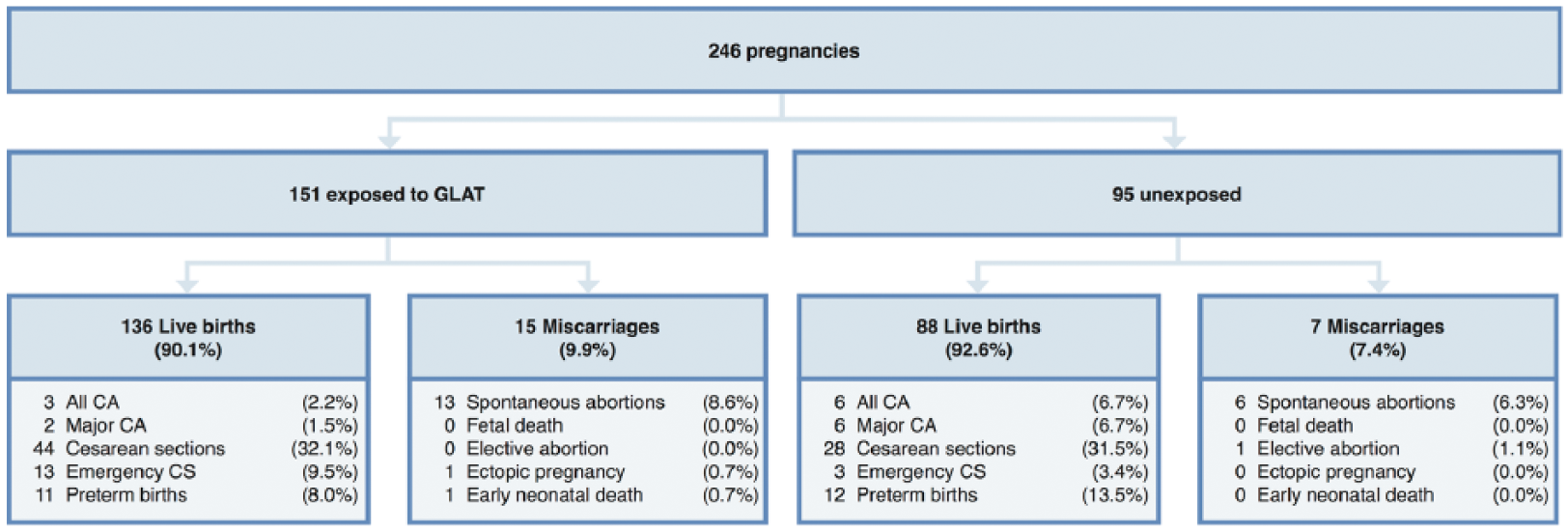
Outcomes of GLAT-exposed and non-DMT-exposed pregnancies.
The single GLAT-exposed early neonatal death was born in 24th gw due to a maternal infection and survived for only 30 minutes. The mother received GLAT for 8 months prior to pregnancy, stopped treatment in the second gw, and was not exposed to other substances during pregnancy.
The probability of a live birth was equal in both groups (Table 2).
Crude ORs and PSs of pregnancy outcomes.
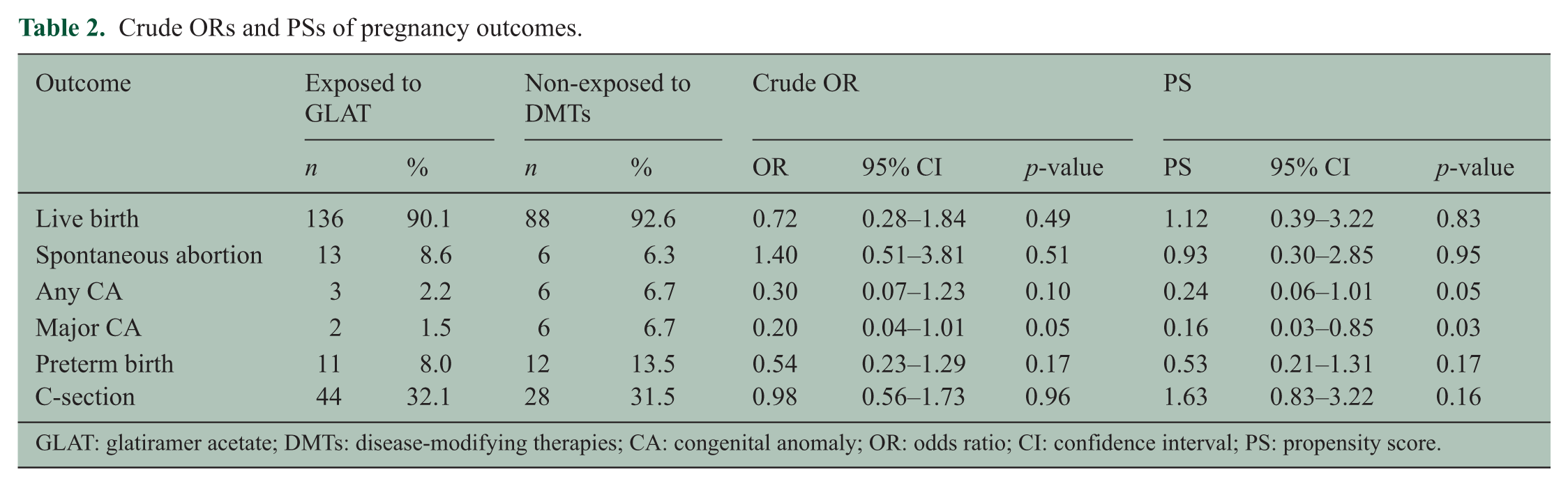
GLAT: glatiramer acetate; DMTs: disease-modifying therapies; CA: congenital anomaly; OR: odds ratio; CI: confidence interval; PS: propensity score.
Early pregnancy exposure to GLAT was not associated with an increased risk of spontaneous abortion (after adjusting for gw of entry in the cohort), any or major CAs, or with preterm delivery (Table 2).
Most women delivered naturally in both groups. In nine cases the use of vacuum extractors and in two cases of forceps was needed. GLAT exposure did not affect the mode of delivery so the delivery via C-section was similar between GLAT-exposed women compared with controls (Table 2).
Mean gw at birth was 38.7 ± 2.7 with no difference between the groups. Mean birth weight including all pregnancies was 3250.3 ± 689.7 g in pregnancies exposed to GLAT and 3195.0 ± 679.7 g in unexposed pregnancies. Mean birth length was 50.7 ± 4.5 cm in the GLAT-exposed and 50.4 ± 3.9 cm in unexposed pregnancies. No differences regarding mean birth weight (p = 0.56) and mean birth length (p = 0.64) were observed between the two groups.
Fetal abnormalities
Nine (4.0%) infants were born with CA (eight major and one minor) in our cohort with no specific pattern, three (2.2%) in the exposed and six (6.7%) in the unexposed group (Figure 1). In the GLAT-exposed group, one infant was born with patent foramen ovale (minor CA), one with renal duplication, and one with pyloric stenosis. Five infants of the DMT-unexposed women were born with CA of non-genetic origin: two with an atrial septal defect (ASD), two with hip dysplasia, one with dysmelia of the tibia and fibula of the right leg. One newborn was diagnosed with Wolf Hirschhorn syndrome (aberration of chromosome 4 with ventricular septal defect, ocular hypertelorism, and dysplastic ears).
All newborns with CA in the exposed group were born full-term, GLAT-treatment was stopped in the first trimester, and no other drug exposures were reported during pregnancy.
In the DMT-unexposed group, both newborns with ASD were born premature in 30th and 36th gw, respectively. The mother of the first newborn had never received any DMT treatment and was not exposed to other toxins during pregnancy. The mother of the second newborn had received GLAT for 4 years and stopped treatment before LMP. She was exposed to intravenous immunoglobulins due to a relapse in the first trimester and to intravenous steroids in the 14th gw.
One mother of the two term-born infants with hip dysplasia was treated with interferon-beta and stopped treatment before LMP. The other mother had stopped GLAT before LMP and received intravenous steroids in the 12th and in the 31st gw.
The newborn with dysmelia of the tibia and fibula was born full-term in the 41st gw. The mother had received interferon-beta but stopped treatment before LMP. In the 24th gw, she received betamethasone due to an imminent premature birth.
The newborn with Wolf Hirschhorn syndrome was born full-term in the 40th week. The mother had received interferon-beta and stopped treatment before LMP. She received oral steroids in the third trimester due to a relapse.
In all cases of CA, we could not identify other risk factors (smoking, alcohol, drug abuse, family history of CA) that could have affected the outcome of the pregnancy.
Discussion
In this prospective cohort with 151 GLAT-exposed pregnancies, we did not observe a negative impact on several major pregnancy outcomes in women exposed to GLAT in early pregnancy compared to women with MS without DMT exposure during pregnancy. This is the second largest study of the safety of GLAT exposure during early pregnancy, the largest besides the manufacturers’ post-marketing surveillance report. 13
In a systematic review, Lu et al. identified in total 97 GLAT-exposed pregnancies from eight studies5,6,11,12,24–28 without any increased risk for lower birth weight, congenital abnormalities, preterm birth, or spontaneous abortion. A potential increased risk for shorter birth length could not be ruled out. 5 Post-marketing studies with 245 GLAT-exposed pregnancies, a smaller recently published study (n = 17), a Brazilian study (n = 41), and our own previous studies (n = 41) did not reveal an increased risk for CA or other neonatal complications related to the drug.7–9,13 Only in the Brazilian study, the mean birth length of newborns with exposure to GLAT was statistically smaller, 9 a finding not supported by our data.
The prevalence of major CA in the GLAT-exposed group was in line with the expected proportion (2%–4%) from the general population 17 although the control group had slightly more major CAs than expected. This is most likely due to the relatively small number of pregnancies in the control group. Other possible explanations are the higher number of pregnancy relapses and high-dose corticosteroid-exposed pregnancies in the control group than the GLAT-exposed group.
The finding that GLAT exposure during early pregnancy is not associated with adverse pregnancy outcomes is consistent with its pharmacokinetic characteristics. The placental barrier is permeable for lipophilic and small substances with a molecular weight between 600 and 800 Da. It is not permeable for large heterogeneous mixture of polypeptides like GLAT (molecular weight of 5000–9000 Da). 29 Therefore, our results of a lacking adverse effect of GLAT during early pregnancy exposure are biologically plausible as it is very unlikely that GLAT passes the placental barrier.
Women without GLAT exposure during pregnancy experienced significantly more relapses during pregnancy and therefore received more corticosteroids during pregnancy than GLAT-exposed women. This was also observed by the Italian group 7 and is a plausible explanation for relapses that occurred during the first trimester. But GLAT exposure is not a likely explanation for why fewer women had relapses during the third trimester, as a continuing effect after withdrawal of a DMT is unlikely. Another explanation could be a higher disease activity in the DMT-unexposed group.
Since the vast majority of the women included in our study had stopped treatment during the first trimester we cannot draw any conclusions about the safety of GLAT exposure beyond that point of time. A small case series did not report on an elevated risk of negative pregnancy outcomes in women with high former disease activity who were treated with GLAT throughout pregnancy. 28
Like most pregnancy registries, our study has several limitations. Through the structure of our registry we cannot exclude a certain selection bias as many women contact us by themselves. This also may explain the relatively high percentage of exposed pregnancies compared to other cohorts.6,7 However, this should not affect the magnitude of effect of the investigated pregnancy outcomes. All women joined the registry during pregnancy, leading to a likely underestimation of spontaneous abortions. Our sample size, although relatively large for GLAT exposure during pregnancy, is adequate to detect a three-fold increase in major CA (assuming 4%; power 80%, two-sided p = 0.05).
Our cohort has several strengths. The German Multiple Sclerosis and Pregnancy registry is a modern cohort of women, mainly treated for the underlying disease, making it suitable to investigate drug effects on pregnancy outcomes. Thus, we are able to compare our data with unexposed but diseased controls from the same source population to exclude any potential impact of the disease itself. All data included in this analysis were collected prospectively which makes over-reporting and recall bias unlikely. 30 Our two groups were very similar in general characteristics and possible confounders for adverse pregnancy outcomes. Furthermore, none of our patients started GLAT accidentally while already being pregnant, therefore immortal time bias, a common problem in pregnancy registries is not relevant. 31
In conclusion, our results provide further reassurance that early pregnancy exposure to GLAT appears safe. This information is important to women with MS who desire children and the neurologists who counsel them.
Footnotes
Acknowledgements
The authors thank the patients for their voluntary participation and the German multiple sclerosis (MS) society (Deutsche Multiple Sklerose Gesellschaft (DMSG)) as well as all referring neurologists and MS nurses for their support.
Conflicts of interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: S Herbstritt, M Rockhoff, and A Queisser-Wahrendorf report no disclosures. A Langer-Gould is the site principal investigator for two industry-sponsored randomized clinical trials (Biogen Idec and Roche). A Haghikia is supported by the German Research Council (Deutsche Forschungsgemeinschaft—DFG). R Gold has received payments for consultancy from Biogen and Teva; speaker honoraria and research grants from Biogen Idec Germany, Teva, Sanofi-Aventis, Novartis, Bayer Healthcare, and Merck Serono. K Hellwig is supported by the German Research Council (Deutsche Forschungsgemeinschaft—DFG) and has received speaker honoraria from Biogen Idec, Teva Sanofi-Aventis, Novartis, Bayer Healthcare, and Merck Serono.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The German Multiple Sclerosis and Pregnancy registry was partly supported by Bayer Healthcare, Biogen Idec Germany, Merck Serono, Novartis Pharma, Teva Pharma, and Sanofi-Aventis Genzyme Pharmaceuticals.