
Abstract
Background:
In Europe, there exists considerable variability in access to care and treatment for multiple sclerosis (MS).
Objectives:
To improve this situation, we identified key issues payers should take into account when making decisions on access to care and treatment for MS. We also give an overview of the different dimensions determining total MS burden and discuss why it is key to integrate the patient’s perspective in estimating this burden.
Results:
The total burden of MS relates to three dimensions: clinical, humanistic and economic. Although the clinical burden is extensively studied, crucial information is still missing about MS pathophysiology, how MS-related symptoms will develop during the disease course and which patients will progress more rapidly. With regard to the humanistic burden, information on patient-reported quality of life systematically collected in clinical trials for registration purposes is still scarce. Early engagement between pharmaceutical companies, the European Medicines Agency and health technology agencies to prospectively identify key evidence needs for the regulatory and reimbursement processes is required as a first step towards more equal access to care and treatment in MS in Europe. Patients’ expectations regarding treatment outcomes should be better researched and integrated into decision-making and patients should be counselled in this process.
Keywords
Introduction
Multiple sclerosis (MS) is a common neurological disorder. In many countries, it is the leading cause of non-traumatic disability in young adults. Given the plethora of symptoms experienced by MS patients and the unpredictable and progressive character of the disease, MS profoundly affects the patient’s quality of life (QoL) from the moment of diagnosis, until the end of their life.1,2 Moreover, it is estimated that within a decade 3 or perhaps even as soon as (on average) three years after diagnosis, half of the MS patients become unemployed 4 and may depend on a disability pension or on their family and friends for the rest of their life. As such, MS is associated with a high burden for patients, their caregivers and families and society as a whole.1,2
Although no cure or preventive measures for MS exist, early diagnosis in combination with timely access to appropriate care (physio/rehabilitation therapy, respite care, home-care, multi-disciplinary team management, etc.) and targeted treatment with disease-modifying drugs (DMDs) provide multiple benefits to MS patients. MS patients will keep a better QoL, are able to remain more active in their family lives and in the workforce, and maintain a higher degree of social participation, self-esteem and economic independence. Unfortunately, people with MS across the different European countries face wide variation in access to care and treatment (as shown by the MS Barometer 2013 survey of the European Multiple Sclerosis Platform (EMSP)) as well as barriers to employment and reimbursement of costs. 4
In order to better meet the patients’ needs in the real-world situation, good communication and collaboration between the different stakeholders involved in MS is essential. This includes MS patients, their caregivers, policy makers, healthcare professionals, researchers, industry, regulators and payers. Therefore, two Pan-European MS Multi-stakeholder Colloquia were organised on 23–24 May 2014 5 and 15–16 May 2015 6 in Brussels to enhance cross-talk and collaboration between several stakeholders: patients, healthcare professionals, regulators and payers. The programme of the first 2014 Colloquium developed by the chair and scientific committee aimed at prioritising actions needed to improve the quality of and access to care. After introductory presentations of experts from the different stakeholder platforms, the audience was asked to pick, from a list of potential calls to action, those which deserved in their opinion highest priority. The outcome of the polling was used as input for further discussions with the speakers, a group of panel members and the audience, which formed the basis for the development of 10 integrated Calls to Action. 7 At the second 2015 Colloquium, guidance propositions/recommendations for the Calls to Action prepared by four working groups prior to the Colloquium were presented and discussed, focussing on how accelerating adoption of innovation can lead to better care in MS.
In this review, we will provide a summary of the content of the presentations and the outcome of the discussions related to the payer’s perspective. The total burden associated with MS, not only from a clinical but also from a humanistic and economic perspective, was first explored. In addition, it was discussed and explored whether and how the patient’s perspective could be better integrated in taking decisions on access to care and treatment.
What is the total burden of MS?
To evaluate the total burden of MS, three dimensions should be taken into account: the clinical, humanistic and economic dimensions. Moreover, the total burden of MS relates not only to patients but also to their caregivers and society in general.
Clinical burden
Epidemiology
In 2013, the estimated number of people living with MS worldwide was 2.3 million with a global median prevalence of 33 per 100,000.8,9 The disease is usually diagnosed during early adulthood (with a peak incidence around 30 years), making it the leading cause of non-traumatic disability in young people. While MS is present in all regions of the world, its prevalence varies greatly, being highest in North America and Europe (140 and 108 per 100,000, respectively) and lowest in Sub-Saharan Africa and East Asia, at 2.1 and 2.2 per 100,000, respectively.8,9 Moreover, prevalence also varies considerably within regions and according to latitude and is expected to further increase in the future. MS is at least twice as common among women than in men. 8 The reason(s) for this observed variability is not understood and requires more research.
Symptoms
Clinically, MS is characterised by multiple signs and symptoms of neurological dysfunction, including gait and mobility impairment, spasticity, visual and sensory disturbances, bladder and bowel problems, pain, sexual disturbances, fatigue, cognitive deterioration and depression.2,9 The Atlas of MS is an extensive worldwide survey of the epidemiology of MS and the global availability and accessibility of resources for people with MS, performed by the Multiple Sclerosis International Federation (MSIF). The 2013 data revealed sensory (40%) and motor (39%) symptoms as the most common, and pain (15%) and cognitive issues (10%) as the least common symptoms (Figure 1).8,9 Although the range of MS-related symptoms is thoroughly described, individual patients’ experience of MS is highly variable and it remains largely unknown how the different symptoms occur and develop during the course of the disease.
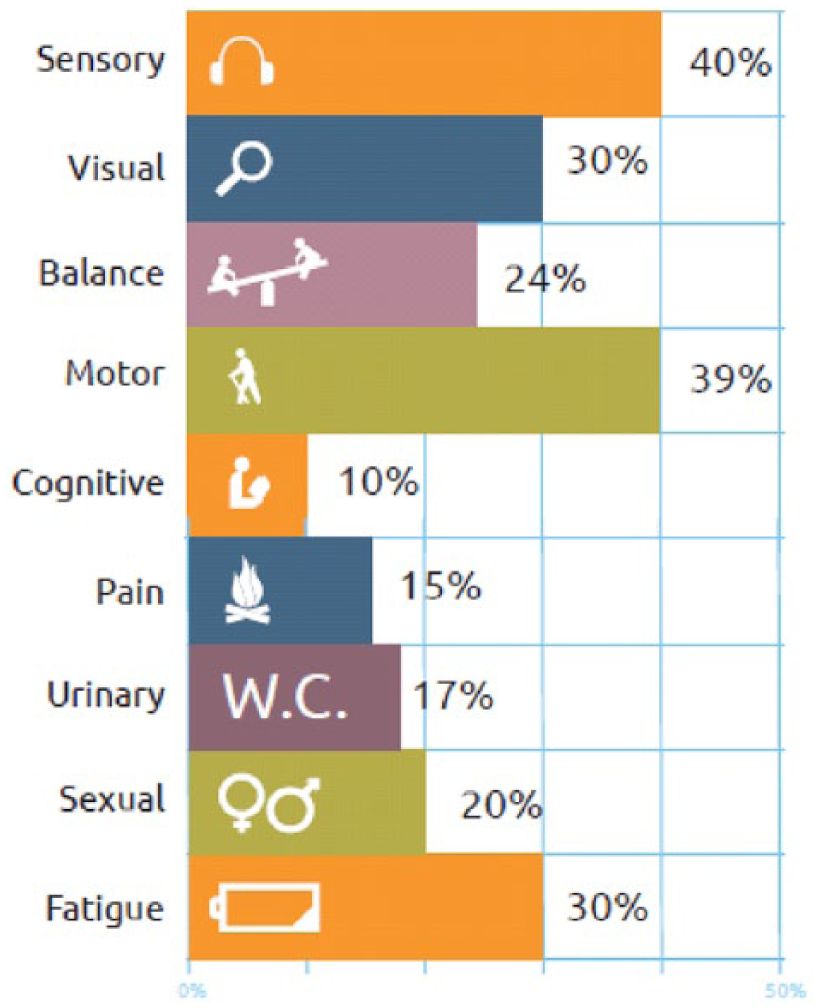
Most common presenting MS symptoms. 8
Natural course of relapsing-remitting multiple sclerosis
In all, 85% of patients with MS have a biphasic disease course. 2 The first phase, relapsing-remitting multiple sclerosis (RRMS), is characterised by recurring episodes of neurological symptoms, persisting for at least 24 hours, followed by complete or partial recovery. 1 Most of the patients with RRMS will develop secondary progressive multiple sclerosis (SPMS), characterised by a steady irreversible neurological decline with a reduced frequency or absence of relapses.1,10 In all, 10% of patients with MS is diagnosed with primary progressive multiple sclerosis (PPMS) and 5% with progressive relapsing multiple sclerosis (PRMS).8,9,11
The rate of disability progression is highly variable. Although several demographic (late age at onset, male gender) and clinical (high number of relapses in first 2 years from onset and incomplete recovery from first relapse) prognostic markers have been identified, 9 it remains very difficult to predict the disease course in the individual patient at disease onset.
Pathophysiology
It was long thought that disability progression in MS patients resulted from the accumulation of residual disability after serial relapses. So, redu-cing relapse rate in RRMS patients was and still is frequently used as the primary endpoint in clinical trials studying DMDs. Nowadays, accumulating evidence suggests that the pathophysiological mechanism underlying relapses is at least partially different from those responsible for disability progression.12–15 While relapses are believed to result from focal inflammation and demyelination causing white matter lesions, disability progression seems to be mainly driven by chronic oxidative stress leading to neurodegeneration and diffuse, progressive brain damage (Figure 2).11,16 As treatment for progressive MS is currently lacking, future research should aim not only at reducing relapses but also at reducing brain atrophy for delaying disability progression in both RRMS and progressive MS patients.
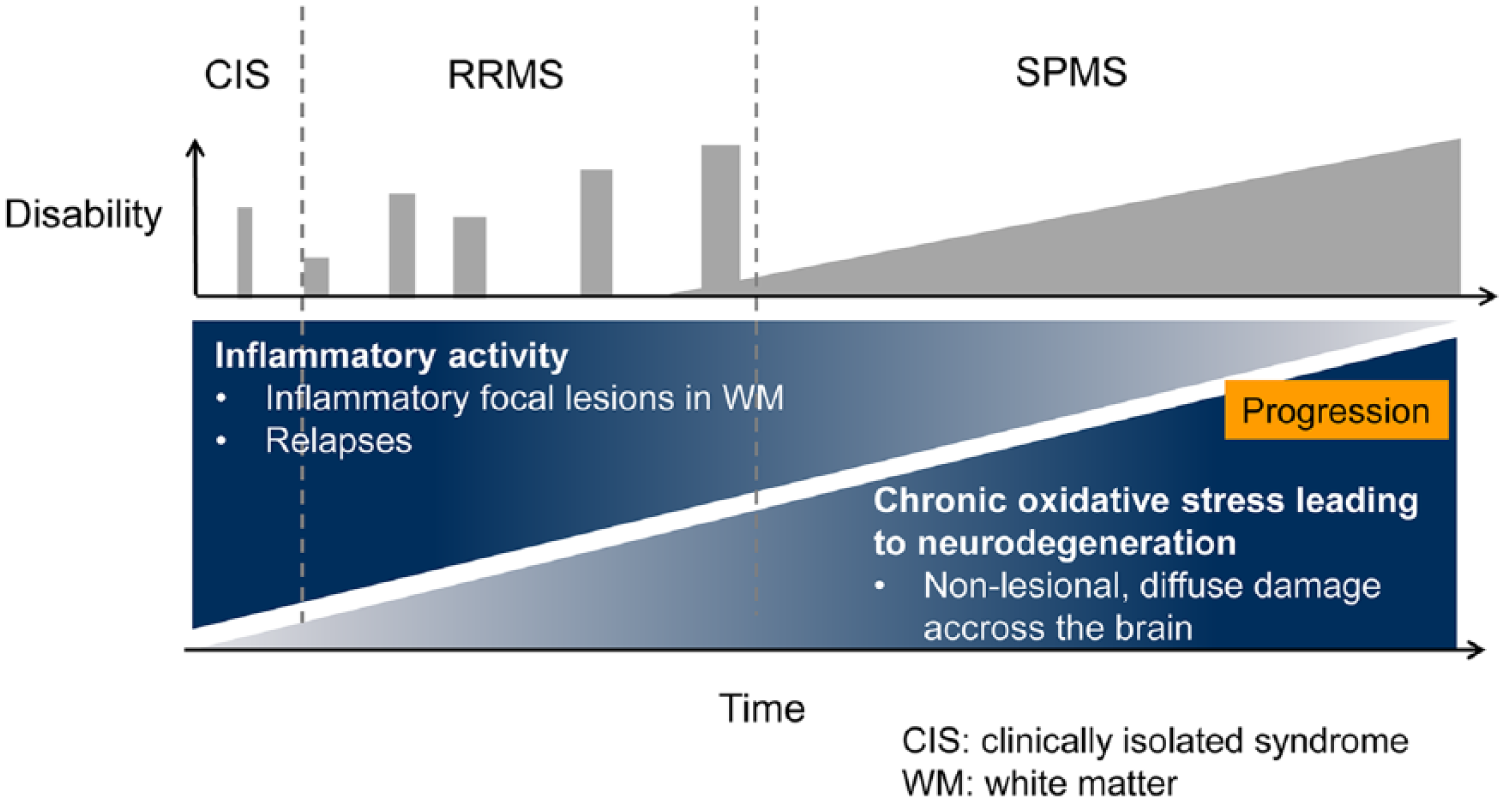
Natural course and pathophysiology of MS. 16
Although the clinical burden of MS is extensively studied, essential information, especially from long-term, well-established studies also focusing on disability progression, is still unknown.
Humanistic burden
As MS is a chronic progressive disease, the plethora of symptoms associated with the disease1,2 will inevitably lead to an increasing level of disability, with impairments in activities of daily living (ADL) and increasing dependence on family and friends. As such, MS has a considerable impact on the QoL of both patients and caregivers, especially because it is most frequently diagnosed in young adults still developing their professional career, social and family status. 2 Furthermore, the unpredictable course of MS leaves individuals with big concerns about their future.
Preference-based valuations of Health-Related Quality of Life (HRQoL) using generic instruments such as the EuroQoL 5 domains (EQ-5D) or the Short-Form 6 domains (SF-6D) are generally being used for health technology assessment (HTA), informing the allocation of resources across different conditions. These valuations (known as utilities) anchor HRQoL between 1 (perfect health) and 0 (absence of life or dead). Different studies have shown that HRQoL in MS patients is reduced compared to the healthy population,17–21 and in many cases, compared with other brain disorders (including stroke, dementia, Parkinson and epilepsy) 22 and chronic conditions such as chronic ischaemic heart disease (IHD) and non-insulin dependent diabetes (NIDM). Even mildly to moderately disabled MS patients (Expanded Disability Status Scale (EDSS) = 3) have a similar or lower HRQoL utility value (0.56–6.5)17,18 than patients with chronic IHD (0.64) 19 or NIDM (0.67). 19 MS disease progression (as measured by the EDSS) has been identified as strong predictor of HRQoL, 18 with a reduction in the utility value with increasing loss of mobility (Figure 3 and Table 1). 18 A US study in around 3,500 MS patients from the NARCOMS registry has also shown larger decrements in EQ-5D utility at earlier mobility impairment stages, as measured with the Patient Determined Disease Steps questionnaire. 20 A systematic literature review by Naci et al. 3 in 2010 including 18 studies evaluating the correlation between disability and health utility confirmed this as well.
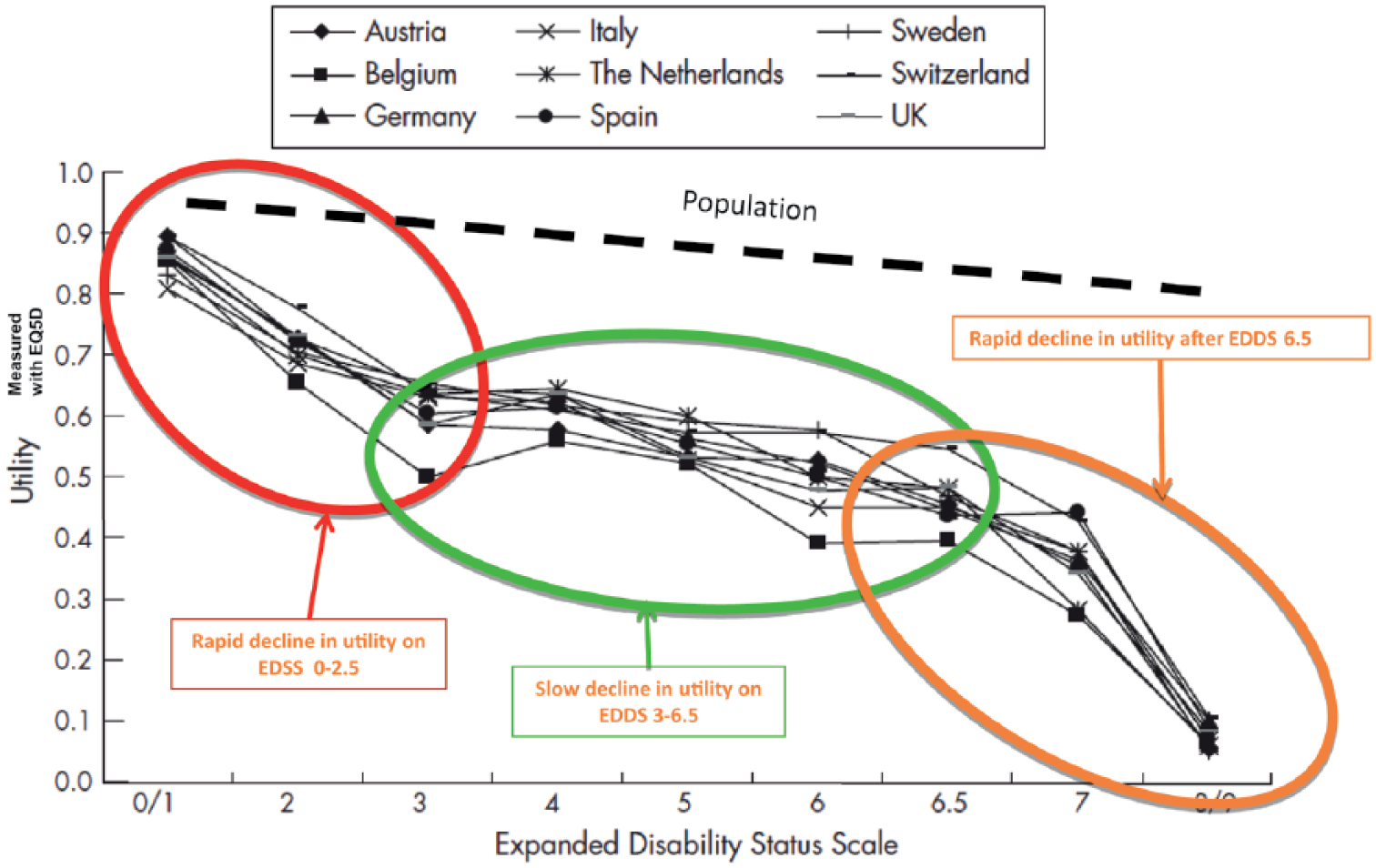
Non-linear relationship between utility and disability progression. Utility scores are calculated with the original EQ-D5 in all countries to obtain comparable values. 18
Relationship between disability (EDSS) and EQ-5D utility.
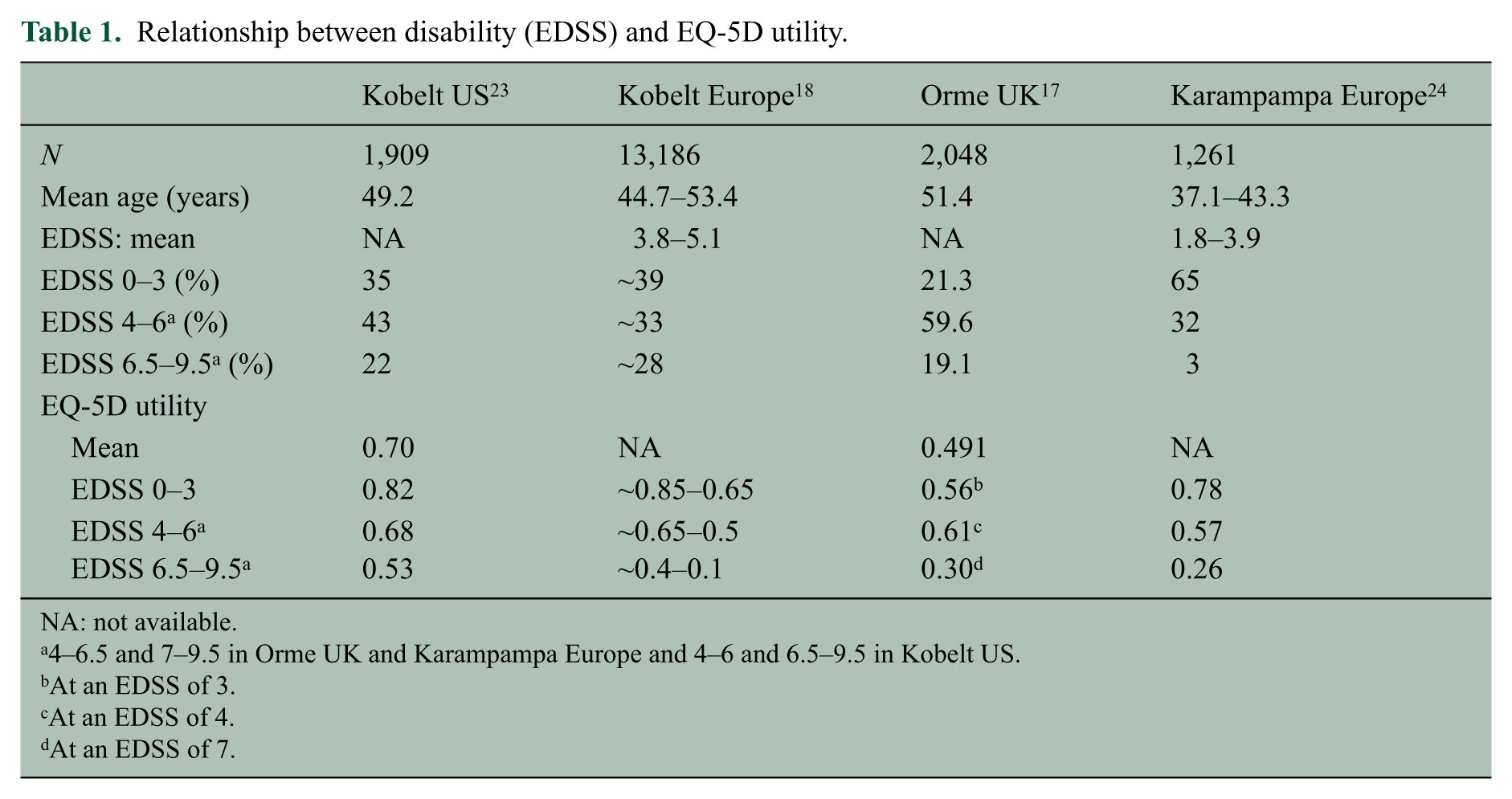
NA: not available.
4–6.5 and 7–9.5 in Orme UK and Karampampa Europe and 4–6 and 6.5–9.5 in Kobelt US.
At an EDSS of 3.
At an EDSS of 4.
At an EDSS of 7.
Not only disability status, but also other MS symptoms have been shown to affect physical, mental and social aspects of the patient’s QoL, 21 with depression identified as one of the strongest predictors of QoL in patients with MS.25,26 With a lifetime prevalence of almost 50%, depression is very common among MS patients. 27 Several studies have observed a strong correlation between MS severity (measured by the EDSS) and depression.28,29 Depression may also be associated with DMD therapy, e.g. interferons.27,30,31 Treatment with inter-ferons may therefore be an important confounding factor in the assessment of MS-related QoL and vice versa. Besides symptoms and disease-related factors, also several socio-demographic and psychosocial factors, such as age, employment status, education level and religiosity have been shown to predict QoL impairment in MS.24,32–34
Despite the increased awareness of the importance of patient-reported QoL, the number of clinical trials including such measurements for registration purposes is still very limited. Furthermore, it is important to include different patient-reported outcome measures. Generic instruments (such as the EQ-5D and SF-6D) capture broad domains of health status, facilitating the comparison of healthcare programmes across disparate clinical outcomes, while MS-specific instruments (such as the Multiple Sclerosis International Quality of Life questionnaire (MusiQoL)) measure symptoms specific to MS.
Economic burden
The substantial impact of MS on the patient and his QoL also has socio-economic consequences. MS typically strikes patients during their peak productive ages and can significantly affect the patient’s physical and/or cognitive ability. Therefore, it often leads to loss of productivity due to sick leave (absenteeism) from work, reduced productivity while at work (presenteeism), early retirement and informal care from family and friends. 20 When evaluating the total economic burden of MS, a distinction is made between direct, indirect and intangible costs. Direct costs represent resources consumed by MS-related interventions including medical costs (e.g. DMDs) and non-medical costs (e.g. disability-related home modifications). Indirect costs relate to productivity losses. Intangible costs relate to the value of lost health, including pain, anxiety, the ability to perform ADL and/or social functioning, often measured and valued through the utility approach.
Total costs for MS have been shown to increase with increasing disease severity/disability.3,35 However, this linear relationship is not observed when direct and indirect costs are evaluated separately.24,35 While direct medical costs dominate the overall costs in patients with low levels of disability, indirect costs outweigh the direct costs in severely disabled patients (Figure 4).24,35 An analysis of work capacity in people with MS of working age in a series of cost of illness studies in 10 countries showed that employment rates declined with increasing disability in a similar way in all countries, generally starting at an EDSS 3–4. 18 As an example, in the French part involving over 1,000 patients below the official retirement age at the time (60 years), only 60% were working at an EDSS 3–4 and only 25–30% at an EDSS 6–7. This compares to a normal workforce participation of 80–90% in the population aged 25–54 years. 36 More or less similar data have been published for Germany. 37
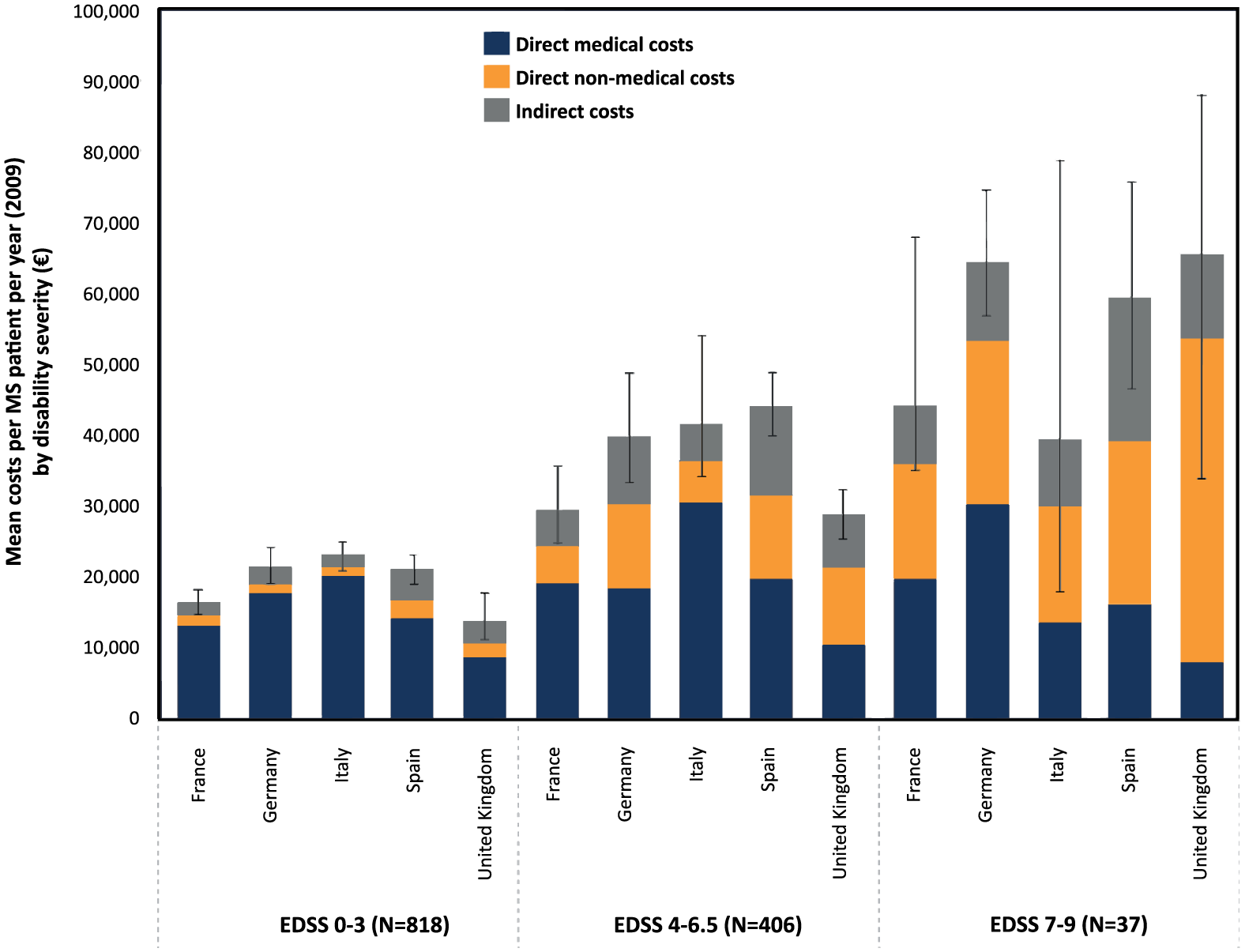
Direct and indirect costs of MS according to disability status. Mean cost per patient per year among 1,261 patients from five European countries with MS. Direct medical costs comprise inpatient and outpatient care, consultations, investigations, MS treatments, prescribed medications and over-the-counter medications. Direct non-medical costs comprise investments/modifications, professional care (paid) and informal care (unpaid). Indirect costs are related to sick leave and retirement due to MS. 24
In chronic progressive diseases, disease duration may also serve as a proxy to observe how unemployment rates increase with disease duration. 38 At 5 and 20 years after disease onset, the probability of remaining without early retirement was 70% and 22% for MS patients compared to 97% and 86% for age-matched controls, respectively. 38 Moreover, those patients with MS who are still able to work often need to reduce their workload or change the type of work. Interestingly, the relative contribution of sick leave and early retirement is the greatest in patients with moderate disability, as more patients are at working age in this group than in the severely disabled patient group.20,23 Therefore, early drug and non-drug interventions which delay disability progression may help to reduce the cost burden. 3
A large amount of data on the cost of MS is available from countries across the world, but the general picture may still be confusing, as comparisons of costs are not straightforward. 3 Costs are a function of resource consumption and prices and both are different in different countries. Thus, while resource consumption, e.g. the rate of hospitalisation or consultations, the use of DMDs or the support for disabled people can indeed be compared (provided studies use the same methodology and are performed during the same time period), it is pointless to compare the resulting costs. Therefore, caution is needed when interpreting/comparing different study results. Despite the number of available studies, with the recent approval of many new DMDs, there is a need for a new, well-designed economic burden study across Europe. Such a study, using a similar set-up as the study performed in 2005, 18 is currently being carried out for the EMSP in 16 European countries involving thousands of patients.
The general methodology for performing this type of cost-of-illness studies is well developed, 39 but often not appropriately applied. Convenience samples, small or biased populations, incomplete data, inadequate costing methods, timing and incorrect assumptions are some of the issues frequently found. Studies are often performed by non-specialists, e.g clinicians with insufficient awareness of economic methodology and results are thus often incomplete or outright meaningless. One solution to improve the quality of the studies could be to develop multi-disciplinary guidelines for non-specialists on how to perform both cost of illness and economic evaluation studies, specifically in MS. A second necessity is to ensure better communication of such studies.
Finally, it is important to ensure that the patients’ point of view on the disease burden is included. The polling at the first Colloquium highlighted a clear need for a consensus on how patients interpret the ‘burden’ from MS, as well as a need for research determining the most important treatment outcomes from the patients’ perspective, including their interpretation of ‘value for money’.
How should the patient’s perspective be integrated in HTA and access to care and treatment?
Marketing authorisation of new treatments in Europe is centrally arranged by the European Medicines Agency’s (EMA) Committee for Medicinal Products for Human Use (CHMP), which is responsible for the approval of effective and safe medicines in the European Union (EU). The CHMP decision is based on the benefit/risk assessment of the efficacy and safety data submitted for a particular treatment by the applicant. 40 For comparative reasons, the primary efficacy outcome data for RRMS are typically based on annualised relapse rates over a time period of 2 years, whereas the main benefit of DMDs lies in their potential to delay the progression of disability. Although the marketing authorisation decision is made on the European level, HTA and subsequent reimbursement/pricing decisions of payers are currently made at the national or regional level. In these decisions, the long-term cost-effectiveness of the new treatment together with the relative burden of the illness, the quality of the evidence and the affordable healthcare budget within the country or region are major determinants. These national and regional processes, as well as the economic wealth of the countries, result in substantial variability in treatment access between different European countries and regions, particularly for chronic diseases such as MS (Figure 5). 41
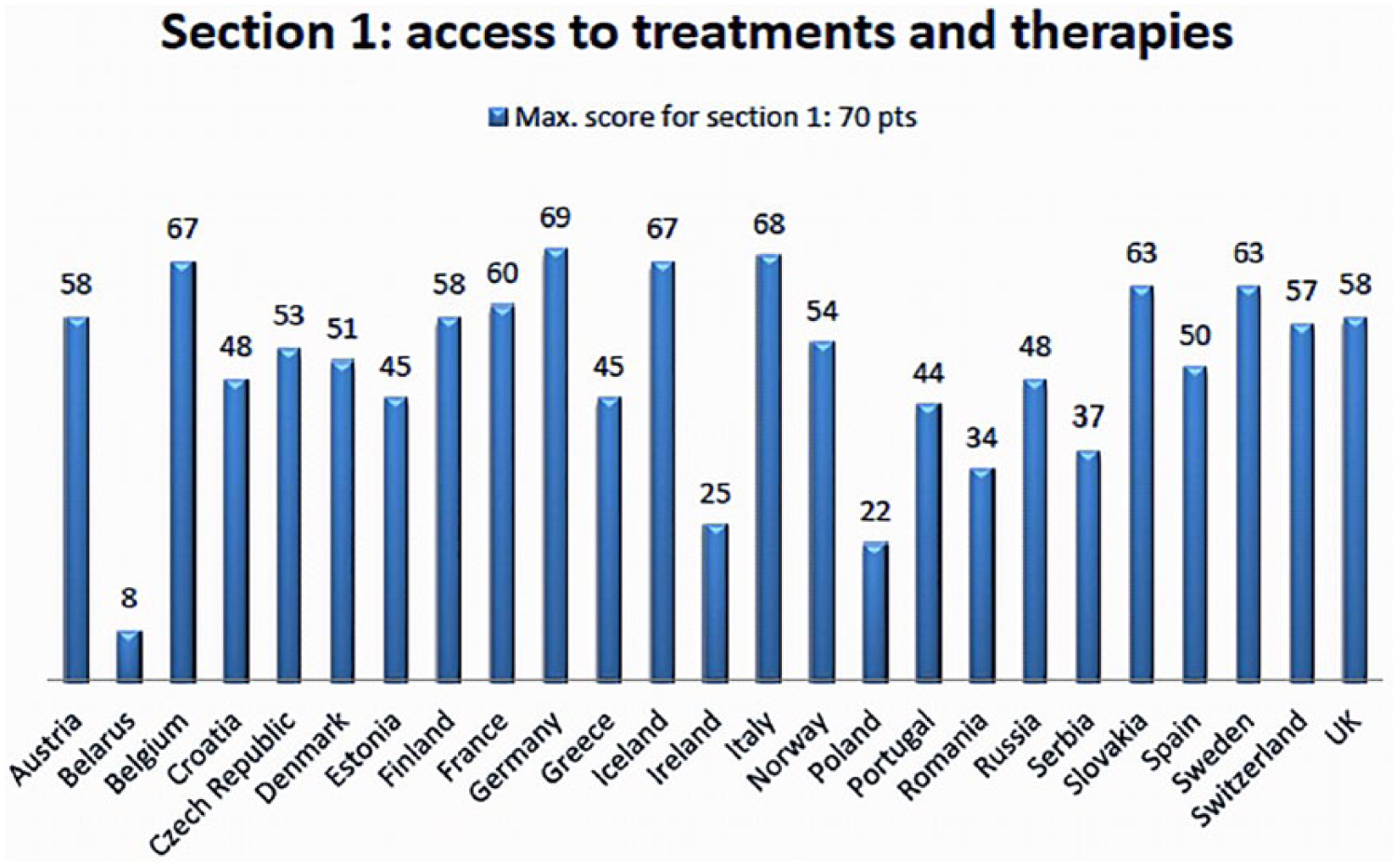
Widespread inequalities in access to MS therapy across Europe. 41
An example of HTA and treatment access decisions is described for the United Kingdom. In August 1999, the Department of Health and National Assembly for Wales asked the National Institute for Health and Clinical Excellence (NICE) to appraise interferon-β (IFN-β: Avonex® (Biogen), Betaferon® (Schering), Rebif® 22 and 44 µg (Serono)) and glatiramer acetate (GA: Copaxone® (Teva)) for MS. Although randomised controlled trials had shown clinical efficacy and safety of each drug in the short-term (usually 2 years) marketing authorisation trials, none of the MS treatments was recommended by NICE. 42 While treatment for MS has been shown to reduce temporary disability due to relapses, the major economic benefit of DMDs lies in the future, when progression to more severe disease/disability is delayed or prevented. As clinical trials are too short to provide full evidence of the benefits of DMDs, modelling has become the accepted standard for economic evaluation in MS. 43 These models combine epidemiological data on the natural history of the disease, consumption of healthcare, QoL related to disease severity and data on the effectiveness of treatments to change the disease course. 18 The assumptions relating to the long-term costs and benefits of DMDs applied in the different modelling studies resulted in huge variability in cost-effectiveness calculations, ranging from £10,000 to £3 million per quality-adjusted life year (QALY) in published studies, being £42,000 to £98,000 per QALY in the NICE HTA. 43 Bearing in mind these cost-effectiveness ratios, NICE concluded that IFN-β and GA were not cost-effective and gave a negative recommendation. This was appealed by different organisations and resulted in the initiation of the ‘Risk-Sharing Scheme’ in February 2002. This allowed the prescribing of the four MS treatments according to the guidelines of the Association of British Neurologists, leading to a 10-year follow-up study able to assess the critical uncertainties emphasised by NICE. If any individual product failed to show benefits as assumed, the subsequent price to the National Health Service would need to be reduced to restore cost-effectiveness to a benchmark of £36,000 per QALY evaluated over a 20-year horizon. 44 The results after 6 years of follow-up of over 4,000 RRMS patients treated with either GA or IFN-β included in the UK Risk-Sharing Scheme (2002–2005), which were modelled using continuous Markov and multilevel models with data derived (during 1980–1996) from the Canadian British Colombia untreated natural history cohort of almost 900 patients, were recently published. 45 The primary outcomes were the progression ratio (treated vs untreated) measured for both the EDSS score and the utility. The observed EDSS progression rate for treated patients was less than that for untreated controls, that is, 75.8% for the Markov and 60.0% for the multilevel model or, respectively, a 24.2% and 40.0% relative reduction in EDSS progression versus untreated controls. Utility ratios were also consistent with cost-effectiveness (58.5% for the Markov and 57.1% for the multilevel model). The authors conclude that GA and IFN-β as a group alter the natural history of RRMS in the real-life setting and, if sustained in the 10-year analysis, the magnitude of the treatment effect observed will be consistent with the pre-defined NICE cost-effectiveness target of £36,000 (US$61,000, Є45,000) per QALY over 20 years.
The importance of the issues outlined above came also out of the polling results at the first Colloquium. Having long-term data at the patient level publicly-accessible for the purpose of comparison with historical cohorts was ranked as first key action to be addressed. The need for a consensus or at least an open discussion between patients, clinicians, HTA and payers on appropriate modelling for long-term effects was considered the second key priority. Early engagement between pharmaceutical industries, the EMA and HTA agencies to prospectively identify key evidence needs for the regulatory and reimbursement processes was also considered important. As mentioned at the second Colloquium, the European Commission is funding since 2010 increased communication between CHMP/EMA and the European Network for HTA (EUnetHTA), a network of government-appointed organisations from EU Member States, the European Economic Area and accession countries and a large number of relevant regional agencies and non-for-profit organisations that produce or contribute to HTA in Europe (http://www.ema.europa.eu/ema/index.jsp?curl=pages/partners_and_networks/general/general_content_000476.jsp&). As part of this, they are currently trying to initiate early dialogue and provide parallel scientific advice on development plans for new medicines, as outlined in the ‘Best Practice guidance for Pilot EMA HTA Parallel Scientific Advice procedures’ document. As a result, the European Public Assessment Report template of the CHMP/EMA has been improved to support rapid relative efficacy assessment (REA) by HTA bodies. 46 In addition, they are working together on the development of scientific and methodological guidelines to facilitate clinical-trial design that can generate (patient-reported outcome (PRO)) data relevant for both benefit–risk and relative effectiveness assessments. At the first Colloquium, the key action to be taken was the empowerment and involvement of MS patients in the decision-making processes. People affected by MS are best placed to represent themselves and their needs, especially because physicians’ concerns and treatment expectations may differ substantially from patients’ preferences. 47 In addition, patients’ preferences might also differ from the opinion of the other involved stakeholders, who finally take decisions which have substantial impact on the patient’s daily life. Therefore, more research should be devoted to determine patients’ perspectives/expectations from treatment outcomes and to the development of tools/methods to measure PROs. In 2009, a web survey among 651 MS patients in the United States revealed delaying disability progression as most important treatment preference. 48 Furthermore, safety concerns, such as risk for progressive multifocal leukoencephalopathy, liver failure and leukaemia, were deemed more important for patients than reducing relapse rate. 48 The EMA has recently accepted to include patients’ opinion on regular stages. There are also several initiatives underway to improve patient consultation and participation in treatment access decisions. However, this will only be successful if patients (or the general public) are well-informed about all aspects of MS and the EMA and HTA processes so they can understand and contribute effectively to decision-making.
Conclusion
Given the current economic situation, the ageing population in most European countries and pressure on healthcare budgets, payers face today tough decision-making for providing access to care and treatment, especially for chronic diseases such as MS.
In order to make appropriate decisions on disease budget allocations, payers should capture the total burden of MS relative to other diseases. Therefore, it is important to identify all factors influencing the burden of the disease, including clinical, humanistic and socio-economic parameters and standardise the methods for doing so.
The principle of equality demands that all people with MS, regardless of where they live in Europe, get access to early diagnosis, appropriate treatments, rehabilitation, interdisciplinary resources and specialists, comprehensive information and palliative care. In order to do so, the whole MS community (including patients, caregivers, pharmaceutical companies, policy makers, healthcare professionals, researchers and payers) should work together (irrespective of their individual stakes) and improve the processes related to decisions on market authorisation, HTA and access to treatments for MS. Furthermore, the patient’s perspectives/expectations should become the key contributor to the decision-making process, as it is the patient who ultimately decides about treatment success or failure.
Footnotes
Acknowledgements
The authors would like to thank Ismar Healthcare, Lier, Belgium for providing assistance with the writing of the manuscript based on the content of the presentations given at the Colloquia and the outcome of the related discussions and voting polls.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Ralf Gold received honoraria or consultation fees from Baxter, Bayer Schering, Biogen Idec, CLB Behring, Genzyme, Merck Serono, Novartis, Talecris, Teva and Wyeth. His department received grant support from Bayer Schering, Biogen Idec, Genzyme, Merck Serono, Novartis and Teva. Mondher Toumi has no potential conflicts of interest to report. Bianca Meesen is a Managing Director of Ismar Healthcare who received support from Teva Pharmaceuticals Europe for facilitating the organisation of the colloquium and proving writing assistance. Emer Fogarty has no potential conflicts of interest to report.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by Teva Pharmaceuticals Europe.