
Abstract
Introduction:
In order to estimate the value of interventions in multiple sclerosis (MS) – where lifetime costs and outcomes cannot be observed – outcome data have to be combined with costs. This requires that cost data be regularly updated.
Objectives and methods:
This study is part of a cross-sectional retrospective study in 16 countries collecting data on resource consumption and work capacity, health-related quality of life (HRQoL) and prevalent symptoms for patients with MS. Descriptive analyses are presented by level of severity, from the societal perspective, in EUR 2015.
Results:
A total of 1010 patients (mean age = 45 years) participated in Italy. In total, 94% were below retirement age, and of these, 56% were employed. Employment was related to disability, and MS affected productivity at work in 77% of the patients. Overall, 96% and 65% of the patients experienced fatigue and cognitive difficulties as a problem, respectively. Mean utility and total annual costs were 0.735 and €22,900 at Expanded Disability Status Scale (EDSS) of 0–3, 0.534 and €40,100 at EDSS of 4–6.5, and 0.135 and €53,300 at EDSS of 7–9. The mean cost of a relapse was estimated to be €2600.
Conclusion:
This study illustrates the burden of MS on Italian patients and provides current data on MS that are important for the development of health policies.
Introduction
Economic studies in health care play a less important role in decision-making in health care in Italy than in some other European countries. Nevertheless, since 1997, in order for a new drug to obtain its price and reimbursement, the negotiation between authorities and the pharmaceutical industry must include, among other, an economic evaluation in addition to an estimate of the impact on the domestic market in terms of public pharmaceutical expenditure and the effects on the national economy (employment and investments). 1 Physicians are aware of the importance of such data for policy, 2 and a considerable number of studies on the cost of multiple sclerosis (MS) have been published in the past decades.3–8
The availability of disease-modifying treatments (DMTs) has led to changes in patient management and more focus on earlier and better diagnosis, including new diagnostic criteria.9–11 One of the consequences in this regard is that the recorded prevalence of the disease is quite different from that estimated two or three decades ago.12,13 A recent review of prevalence estimates of MS in Italy over the last 40 years reported a large variation by region, with 130 patients per 100,000 population in Lazio, 188/100,000 in Tuscany and 176/100,000 and 299/100,000 in Sicily and Sardinia, respectively. 14 With diagnosis possible already after a clinically isolated event, 10 one must also expect a different distribution of the type of MS and the severity of the disease than 10 years ago: a larger proportion of patients with relapsing-remitting disease and thus of patients in the early stages of the disease with less disability.
Therefore, it is important to update the information on the burden of MS, and this study is part of a European-wide effort in 16 countries, endorsed by the European Platform of MS Societies (EMSP) and carried out with the support of national MS societies. 15 It uses a similar methodology as the last European survey in 2005 that also included Italy.4,16
Materials and methods
The detailed methodology for this European survey is published separately. 16 We therefore only provide a short summary of the general methods and issues specific to Italy.
Data
This study aimed to estimate the costs of all health care and other resource utilisation related to MS: hospitalisation, rehabilitation, consultations, diagnostic procedures and tests, medication, community care, family support and production losses (sick leave, early retirement and invalidity). In addition, information on major symptoms such as fatigue and cognitive difficulties, health-related quality of life (HRQoL) as well as self-assessed disability using descriptions based on the Expanded Disability Status Scale (EDSS) was collected.
Data were collected with a standard questionnaire, at a single point in time, for a retrospective period of time. The latter was varied depending on the question in order to minimise recall bias: 1 month for use of drugs, community services and family help; 3 months for hospitalisation, consultations, tests, sick leave and relapses; and 12 months for major investments. Resource utilisation is reported for these time periods, while cost calculations are annualised.
Disease information (type of MS, disability (EDSS), HRQoL, utility (EuroQol five-dimensions (EQ-5D) 17 ), symptoms (fatigue and cognitive difficulties) and the effect of MS on work related to the current day or week. For comparability across countries, 15 utilities are estimated with the original value set developed in the United Kingdom. 18 This tariff is generally used in studies in Italy. However, Scalone et al. 19 established an Italian tariff applying the same methodology as used for the UK tariff with individuals from the general population, and therefore, we also present utilities established with this local tariff.
The handling of missing data for the cost calculation is explained in more detail in the paper describing the methods. 16 For resource use, we present actual answers without any imputation for missing answers. Also, no imputations are made for missing information on disease status, symptoms and HRQoL.
Costs
Costs are calculated in the societal perspective, including all costs regardless of who ultimately is responsible for them. Patient co-payments and patients’ out-of-pocket expenses are thus included.
The cost of a relapse is calculated as the difference in quarterly costs between patients with or without a relapse and an EDSS score of 0–6; patients who were unsure were excluded from the estimation. Invalidity, early retirement and DMT costs are not considered in the calculation as these are unlikely to be affected within 3 months. Unit costs for the individual resources were taken from public sources and described in the paper on the study methodology, 16 and results are reported in EUR 2015.
Patients
The objective was to include a sample where all levels of disease severity (defined by EDSS) were represented in sufficient numbers to permit analysis, rather than a prevalence sample. This allows highlighting how costs and HRQoL change as the disease progresses and provides the necessary data for cost-effectiveness analysis of treatments that are expected to change the course of the disease. Mean results may thus not be representative and should neither be extrapolated directly to national costs nor be compared directly to the results in earlier studies. We therefore report results by disease severity groups only (mild MS, EDSS = 0–3; moderate MS, EDSS = 4–6.5; and severe MS, EDSS = 7–9).
Data collection
In anonymous surveys, it is difficult to include a fully representative patient population, and changes in the management of MS, in particular earlier diagnosis, have increased this challenge. In addition, participation will depend heavily on the methods used for the survey: collecting data in MS centres tends to overestimate the number of patients with early but severe disease and on treatment with DMTs; 20 collecting data from members of patient organisations may lead to the opposite. Internet surveys will bias towards younger patients with better education, while postal mailing may bias towards older patients.
The Italian participants in the study presented here were all people in contact with the Italian Multiple Sclerosis Association (AISM). The data were collected during spring and summer 2015. AISM invited 4000 individuals to participate in the survey with a web mailing list regularly used to distribute information. This sample of online users from the AISM is typically rather young (mean age = 43.5 years). To also include older patients with more advanced disability, 200 patients were contacted personally by staff from the regional offices of AISM and their answers collected on paper.
Results
A total of 1010 evaluable responses were received. All patients invited by mail answered electronically (80%), while the 200 patients contacted directly completed paper questionnaires. The geographical distribution of respondents represented well the proportion of inhabitants of the different regions, with, however, a slight overrepresentation in Sardinia and Tuscany and an underrepresentation in Campania and Sicily. 21 Table 1 provides details on demographics, employment and disease.
Demographic and disease information.
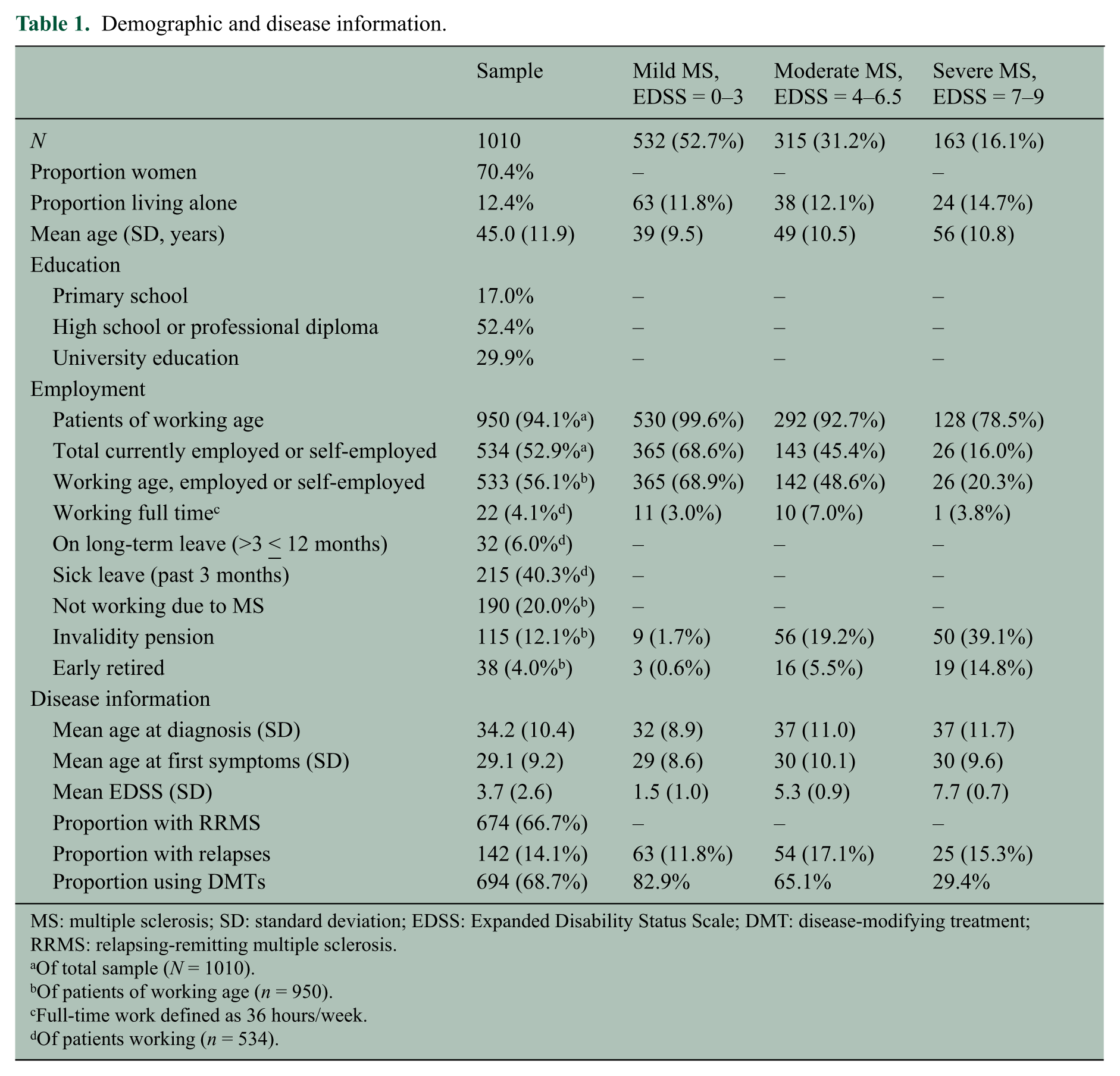
MS: multiple sclerosis; SD: standard deviation; EDSS: Expanded Disability Status Scale; DMT: disease-modifying treatment; RRMS: relapsing-remitting multiple sclerosis.
Of total sample (N = 1010).
Of patients of working age (n = 950).
Full-time work defined as 36 hours/week.
Of patients working (n = 534).
Demographics and employment
The age of respondents in Italy ranged from 19 to 84 years (mean = 45 years, median = 44 years and standard deviation (SD) = 12.0 years). Women represented 70% of the sample; 87% lived with their family and only three patients lived in a nursing home at the time of the survey. Education levels in our sample were considerably higher than in the general population of that age, as would be expected in this mostly online survey: 17% of patients had basic education, 52% had a secondary or a professional degree and 30% a university degree. This compares to 36% of the population with primary education, 47% with upper secondary education and 19% with tertiary education in 2015. 22
The majority of patients in the sample were below retirement age (defined as effective retirement age, 60.5 years for women and 61.1 years for men 23 ): 950 patients (94%). Of these, 533 patients (56%) were employed or self-employed. One patient above retirement age also worked, bringing this group to 534 patients (or 53% of the full sample), with a mean age of 46.6 years. This compares to an employment rate of 60.5% in the general population aged 20–64 years in 2015. 24 However, 96% of employed patients worked part-time, on average 23 hours/week; 84% of these did so due to MS, confirming indeed the effect of MS not only on employment but also on working time. In addition, 6% of employed patients were on long-term absence, while short-term sick leave during the past 3 months was reported by 215 patients (23%), with a mean duration of 12 days.
Employment decreased rapidly with advancing disease, as shown in Figure 1. Of non-employed patients below retirement age, 20% indicated MS as the reason for leaving the workforce.
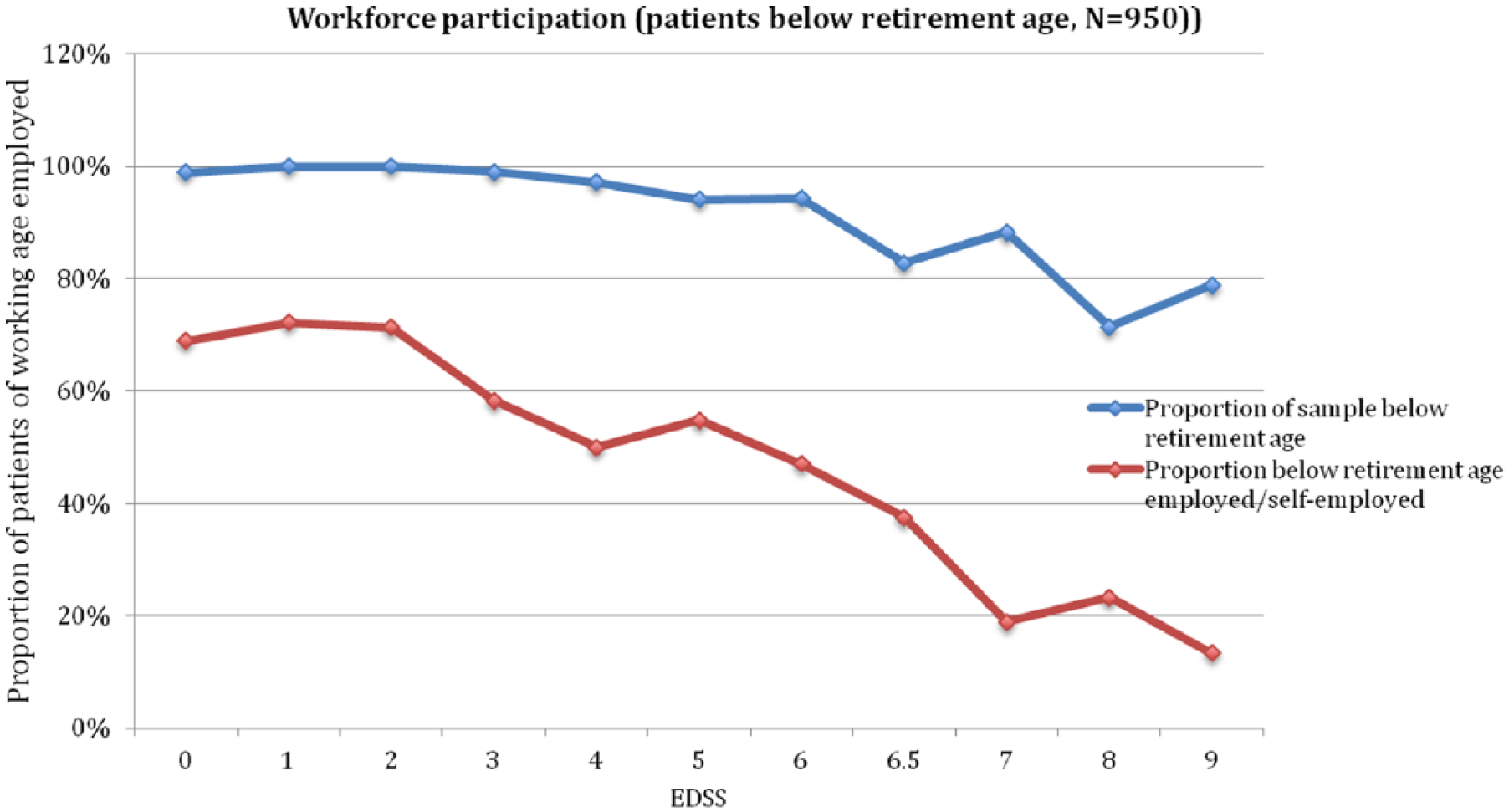
Employment by disease severity.
Most employed patients felt that MS affected their productivity at work (77%), and only 12% indicated that they had no problems related to work, while 10.5% had not answered this question. The severity of the effect covered the entire visual analogue scale (VAS) range from 0 to 10, with a mean of 3.6 (SD = 2.6; Figure 2). Fatigue was considered the most bothersome symptom (78%), followed by cognitive difficulties (30%), low mood (27%), mobility (23%) and pain (17%).
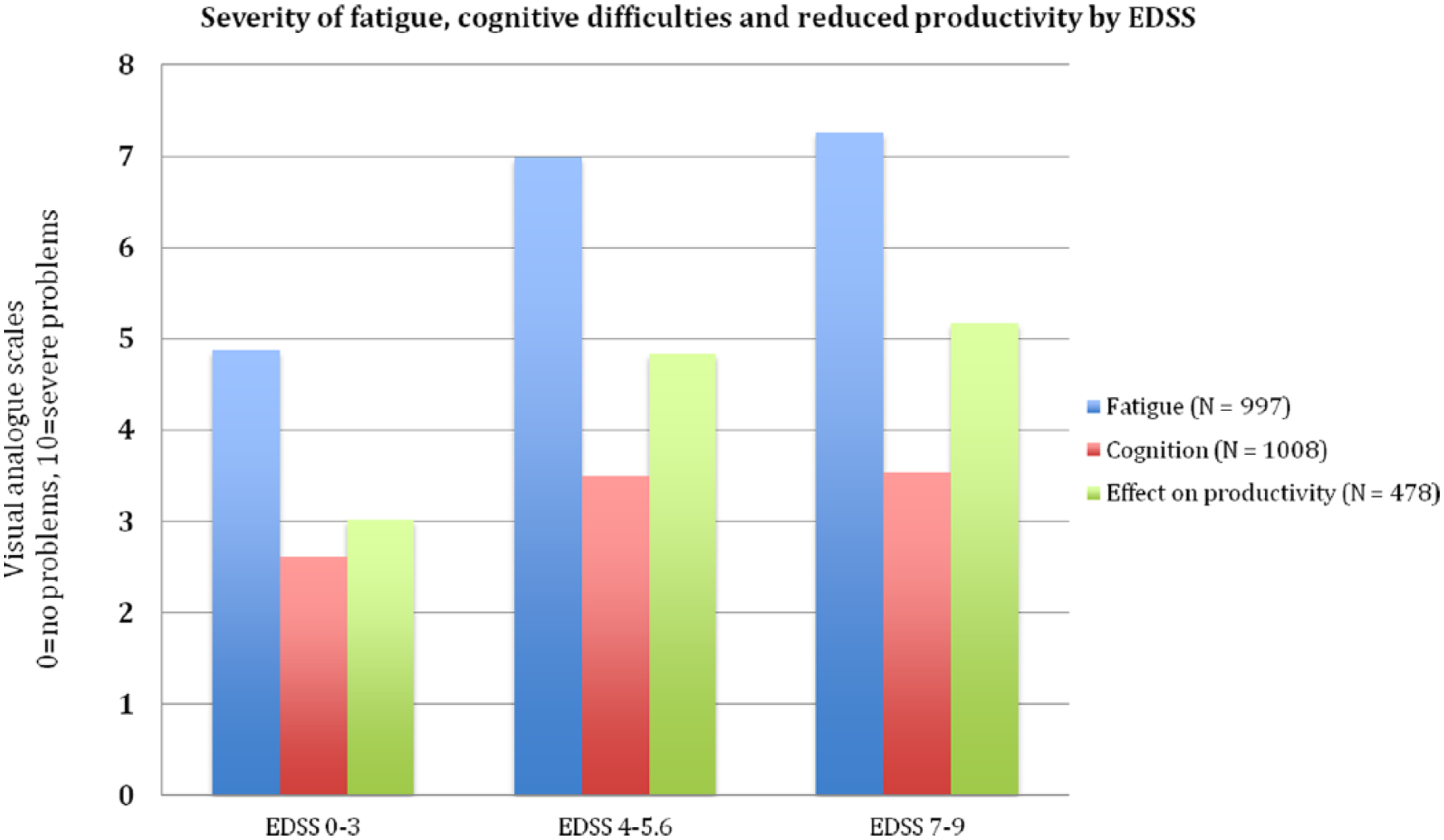
Fatigue, cognitive difficulties and effect of MS on productivity at work.
Disease characteristics
Data on disease characteristics are summarised in Table 1. As a consequence of mean age of the Italian sample, the mean EDSS was low (3.7, SD = 2.6) and the group with early or mild disease was very large. The mild group represented 53% of the sample, the moderate group 31% and the severe group 16%. However, the number of patients at each EDSS score exceeded 50 with the exception of EDSS 9 with 19 patients only.
Similarly, a majority of patients (67%) had relapsing-remitting multiple sclerosis (RRMS), while 20% had secondary progressive multiple sclerosis (SPMS) and 12% had primary progressive multiple sclerosis (PPMS), with 1% missing. Considering this group with recent diagnoses, the proportion of PPMS is probably higher than seen in recent studies 25 and suggests, as we found in previous studies, that patients were insecure in their answers regarding the type of disease. We therefore did not include the disease course in our analyses and focussed on EDSS levels instead. Nevertheless, the high proportion of RRMS and young age may partly explain that DMTs were used by 69 of the sample, with usage declining with higher EDSS levels, as expected (Table 1). Among users, 31% were on their first DMT treatment; first-generation DMTs were used by 64% of users (Table 2).
Type of DMTs used (N = 694).
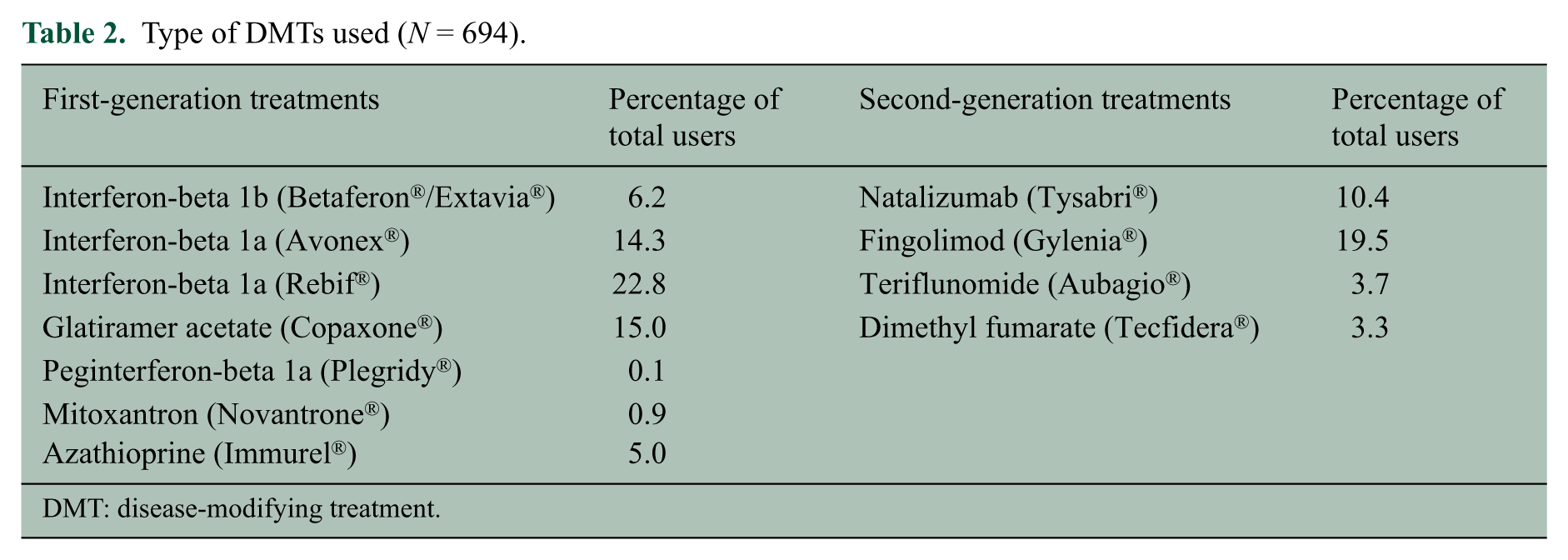
DMT: disease-modifying treatment.
Relapses in the preceding 3 months were reported by 142 patients (14%), of which half occurred in the past month (Table 1). However, 189 patients (19%) were unsure whether they had a relapse or not, and we assumed that the answer was no. Thus, the mean relapse rate over a 3-month period was estimated at 0.2 (SD = 0.5). Corticosteroids were administered to 62% of the patients with relapses, most often as infusion.
Symptoms and HRQoL
Fatigue and cognitive difficulties were an issue for the majority of patients, and both were related to disease severity (Figure 2). Fatigue was present in 96% of the patients (1% missing). The mean VAS score was 5.9 (SD = 2.6) for the whole sample, 4.9 for patients with mild disease, 7.0 for patients in the moderate group and 7.3 for patients in the severe group. Cognitive difficulties were present in 65% of all patients. The mean VAS score in this group was 4.6 (SD = 2.1) overall, 4.1 in the mild, 5.1 in the moderate and 5.5 in the severe group. For the full study sample (assigning 0 to the group with no problems), the mean score was 3.7 (SD = 2.8), with scores of 2.6 in the mild and 3.5 in the moderate and severe groups.
All five domains of HRQoL included in the EQ-5D 18 represented problems for a large proportion of patients: pain/discomfort for 73%, usual activities for 67%, mobility for 60%, anxiety/depression for 59% and self-care for 32%. Both the severity and the affected domains changed with advancing disease. Self-care was unaffected in patients with mild disease but declined very rapidly with advancing disease, with <10% without difficulties in the severe disease group; mobility, pain and usual activities presented problems for almost all patients already with moderate disease; most noticeably, however, anxiety/depression was present in about 60% of the patients at all levels of disease severity (Figure 3).
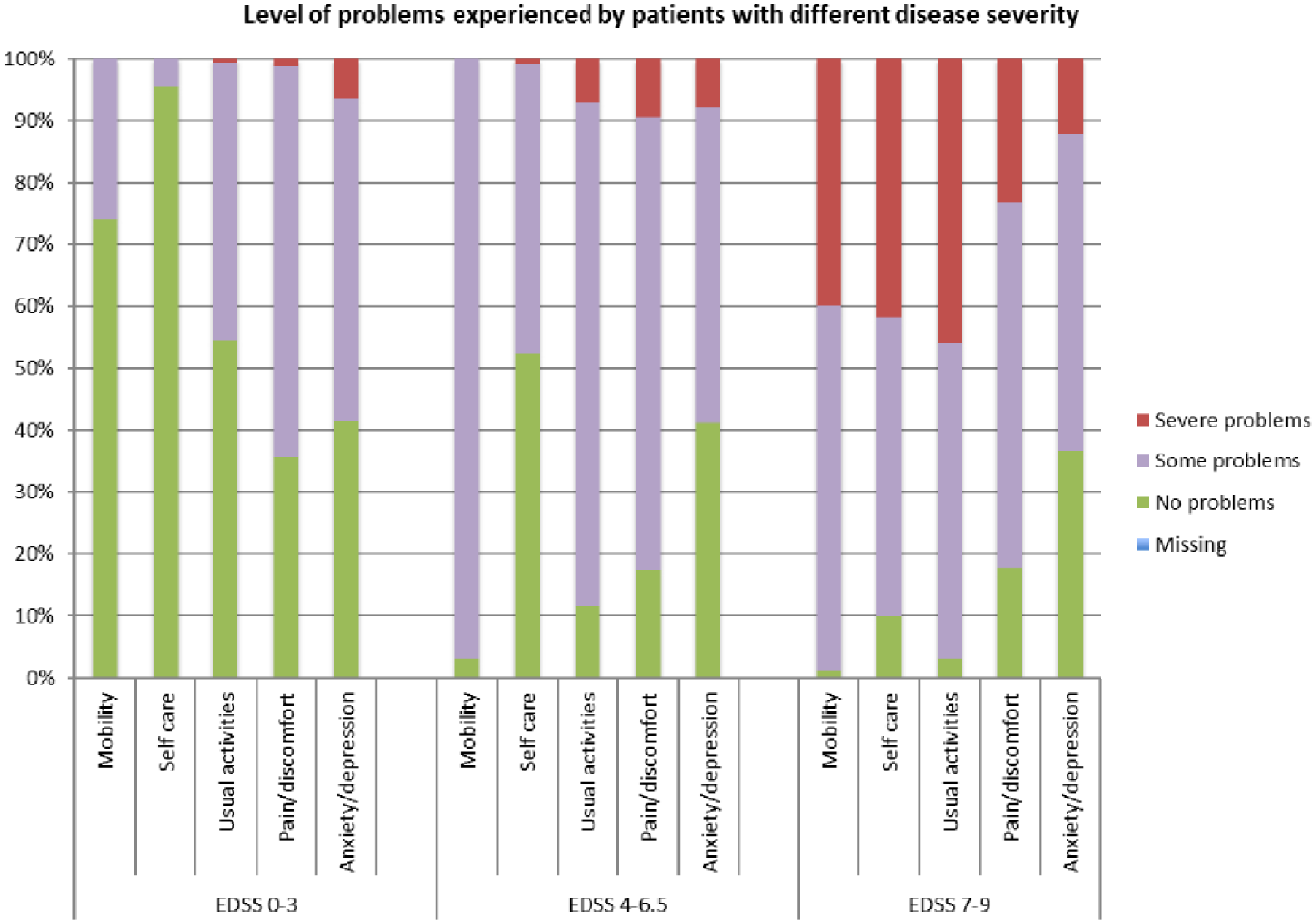
Problems in different domains of QoL (EQ-5D; N=1010).
Utility
Utility scores declined with increasing disability (EDSS; Figure 4). Mean utility in this specific sample of patients was 0.575 and 0.744 using the UK and Italian value sets, respectively. The scores with the UK value set are very similar to those found in a recent study with a similar patient population. 8
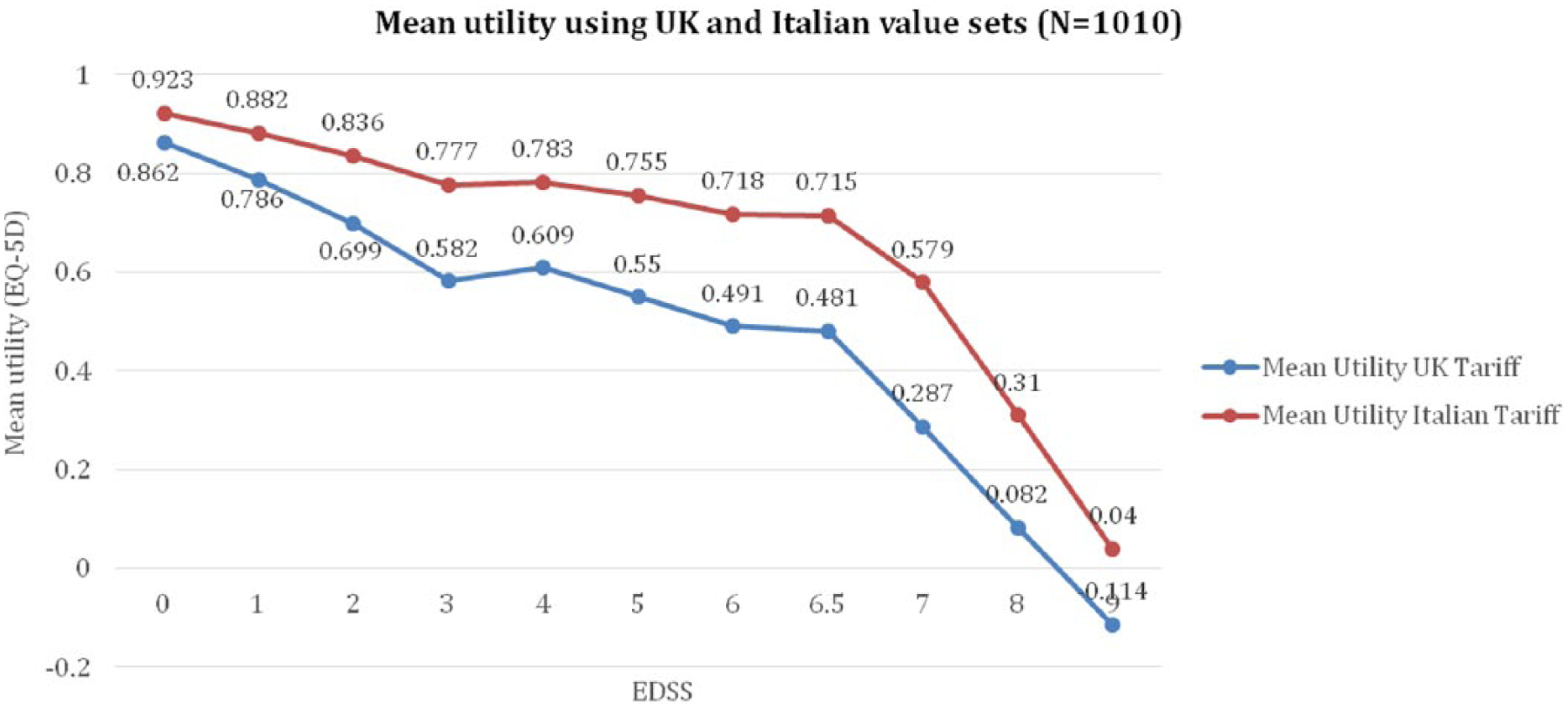
Utility by EDSS (N=1010).
Resource utilisation
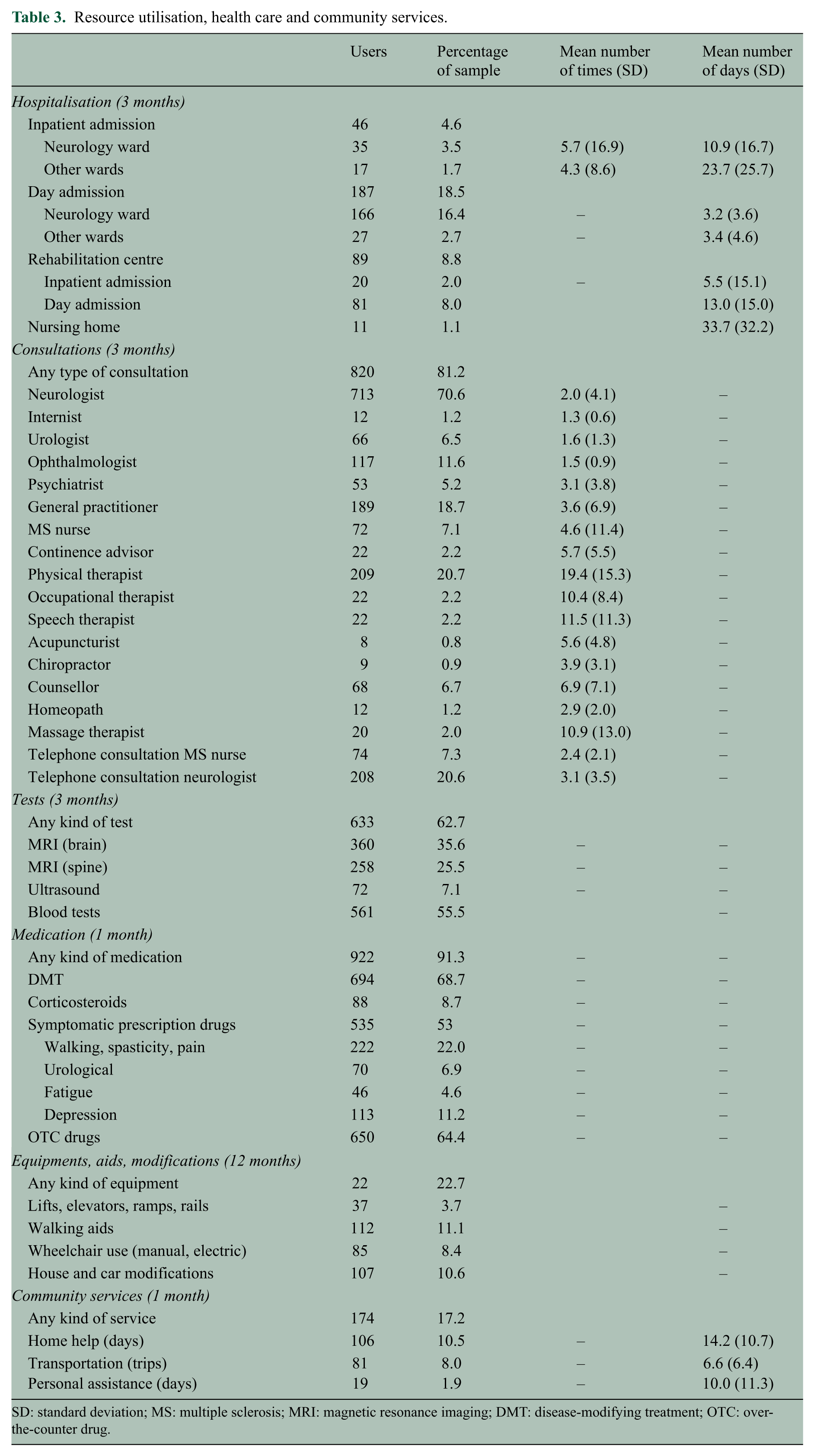
Resource utilisation is presented in Table 3. Inpatient admissions were rare, occurring in patients with a severe relapse or severe disease who spent the major part of the preceding 3 months in hospital: 46 patients (5%) were admitted as inpatients, most often to a neurology ward, 6 times on average and for a mean of 10.9 days (SD = 16.7 days). Day admissions were reported for 187 patients (19%) and were most likely linked to treatment administration, on average once a month. Inpatient or day admissions to rehabilitation centres occurred for 89 patients (9%).
Resource utilisation, health care and community services.
SD: standard deviation; MS: multiple sclerosis; MRI: magnetic resonance imaging; DMT: disease-modifying treatment; OTC: over-the-counter drug.
A majority of patients (820 patients, 81%) had a consultation during the past 3 months, most often with neurologists (71%), physiotherapists (21%) and general practitioners (19%). Investigations and tests were done for 63% of patients, with 360 patients (36%) undergoing magnetic resonance imaging (MRI) of the brain and 258 patients (26%) of the spine. Medications for MS and MS-related symptoms were used by 91% of the patients during the past month. Drugs other than DMTs (including corticosteroids) were used by 53% of the patients, predominantly treatments for walking, spasticity and pain (22%) and depression (11%). Non-prescription drugs were used by 64% of the patients.
Investments in equipment and devices to aid patients’ mobility were made during the past 12 months for or by 23% of the patients, most often for walking/mobility aids and modification to the house or the car.
Community and social services were used by 17% of the patients, most frequently home help. Help from family was used by 44% of the patients, on average 16.8 (SD = 11.8) days per month and 6.3 (SD = 7.3) hours per day. Both community services and informal care were related to disease severity (Figure 5).
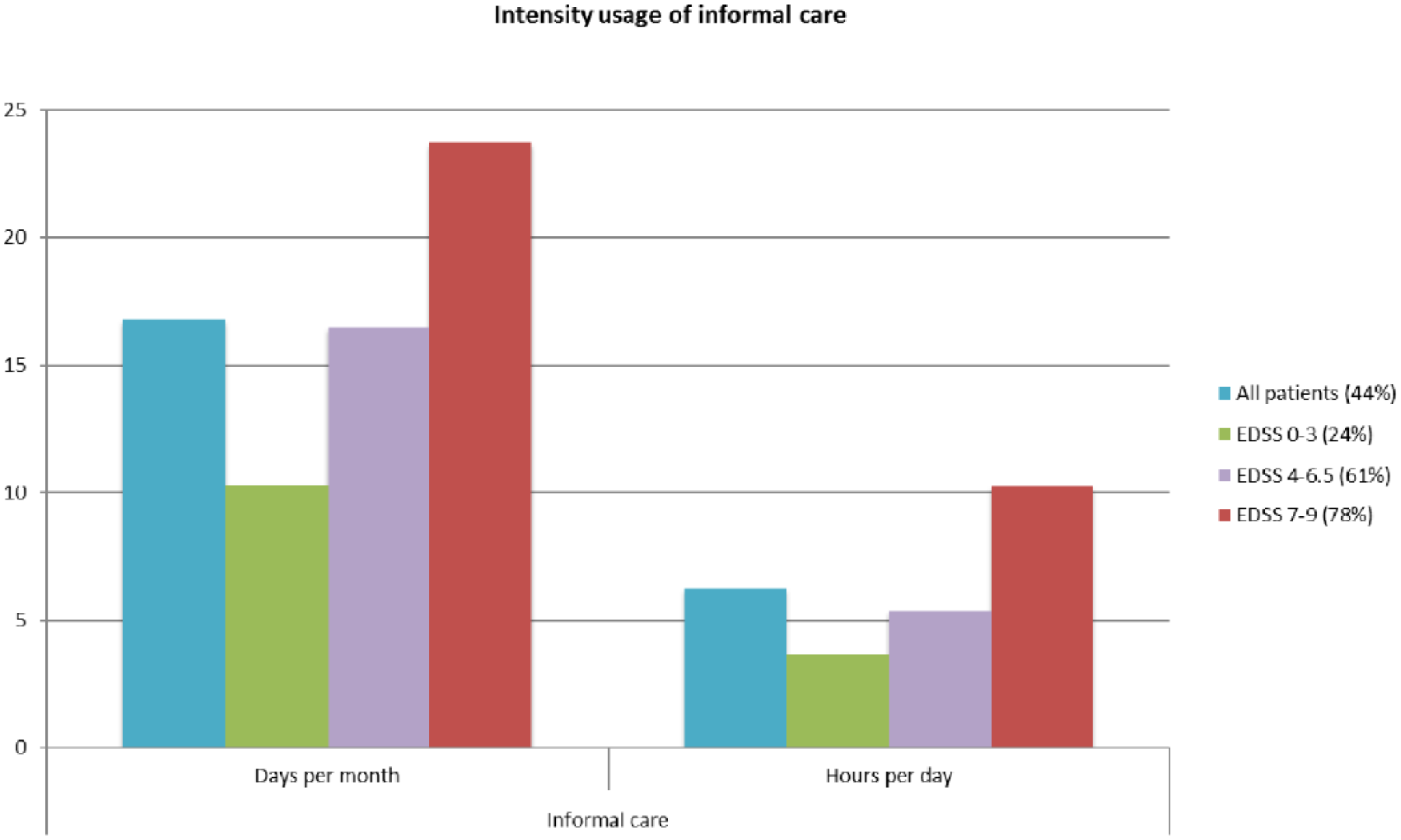
Use of informal care (days per month and hours per day, per user).
Costs
Total mean annual costs per patient for patients with mild, moderate and severe disease and by EDSS score are presented in Figure 6 and Table 4.
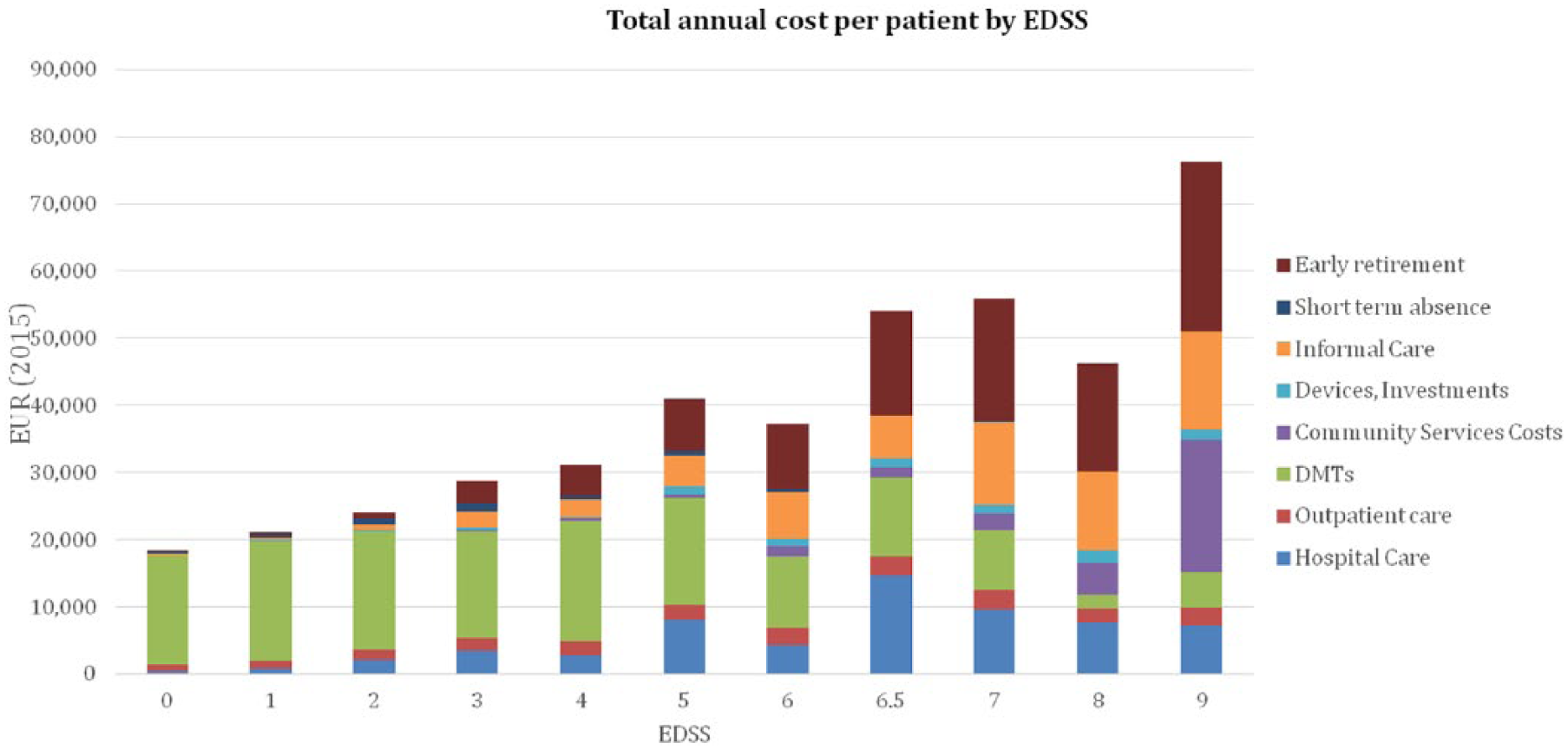
Total mean annual cost per patient by disease severity and by level of EDSS (N = 1010).
Total mean annual cost per patient by disease severity (mild, moderate and severe), N = 1010 (EUR 2015).
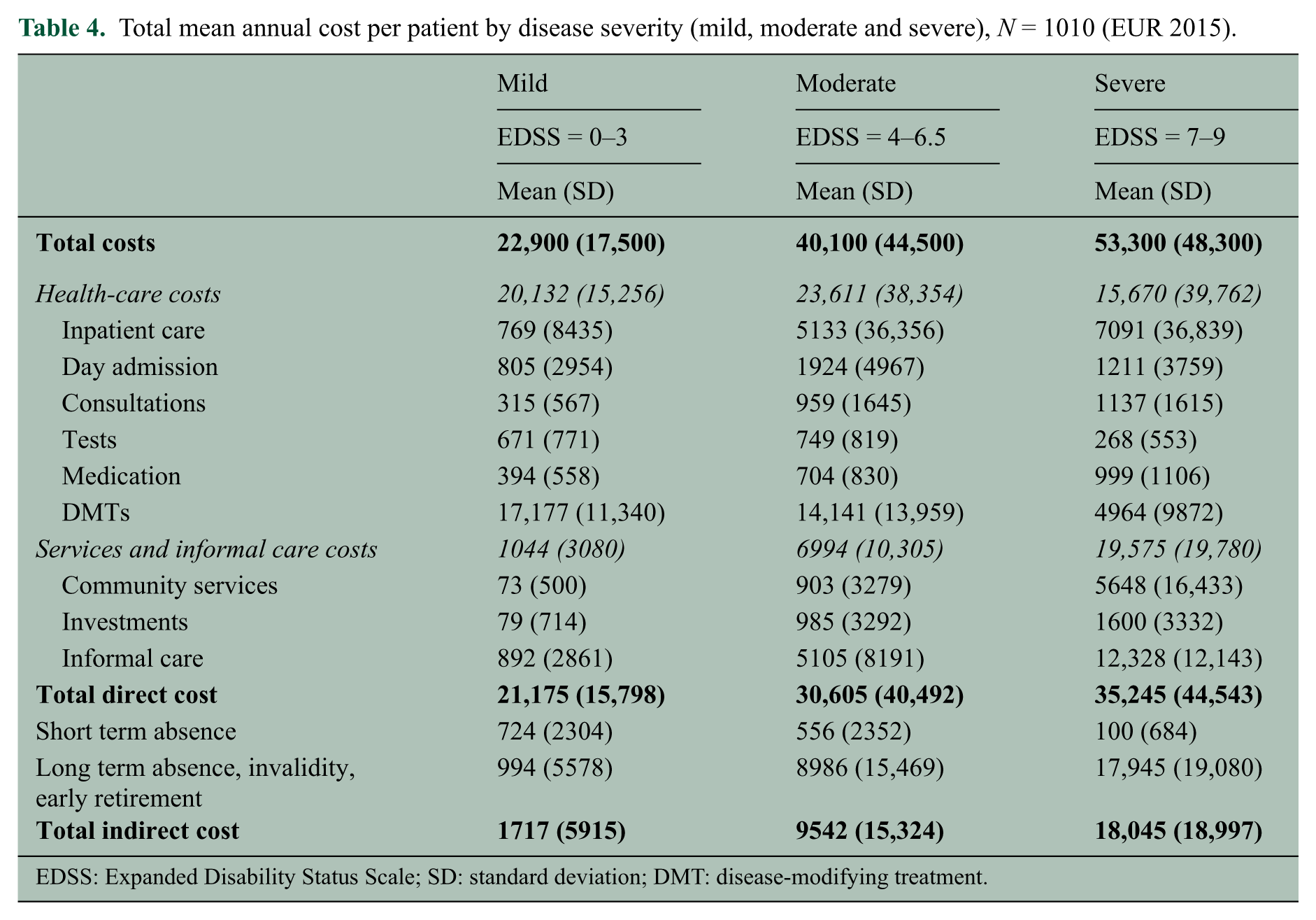
EDSS: Expanded Disability Status Scale; SD: standard deviation; DMT: disease-modifying treatment.
The average cost of a relapse for patients with an EDSS between 0 and 6 was estimated at €2620. All types of costs increased during a relapse, with hospital care representing 43% of the additional cost, informal care 28% and sick absence 11% (Figure 7).
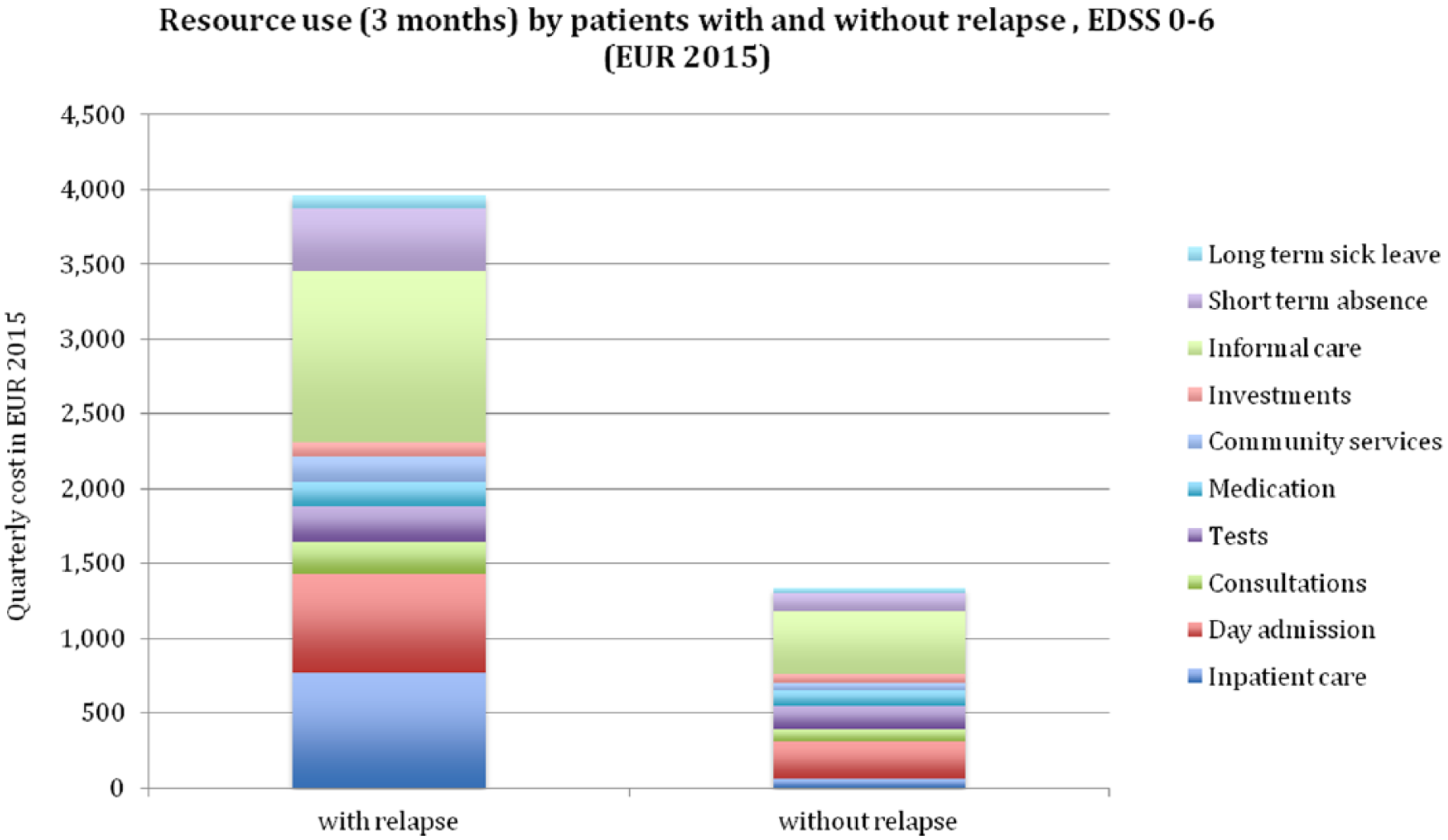
Relapse costs (3 months).
Discussion
This study provides an update to the current understanding of the burden of MS on patients, the health care system and society in general in Italy based on a cross-sectional survey conducted in 2015.
The Italian sample was young, as a result of mainly enrolling patients using a web mailing list, and although it included patients at all levels of disability, there was an overrepresentation of patients with early disease. Consequently, we did not extrapolate the mean cost in this sample to a national cost estimate, as it would likely result in an underestimation. The enrolment method may also partially explain the better educational attainment in our sample compared to the general population. Age and education may, in turn, explain that the absolute employment rate was not substantially lower than in the general population.
Overall, our results are in agreement with the literature, showing that the costs of MS increase with rising EDSS level, while utilities (QoL) decrease. 26
Disease symptoms and utility were very similar to those found in the other countries of the survey, attesting to the fact that the severity of the disease affects patients in the same way regardless of jurisdiction or heath care systems. In particular, in patients with advanced disability, all domains of HRQoL were compromised. The negative effect of MS is thus evident in different aspects of daily life and functioning, with different implications also for health policy. For instance, there is a need for more persistent monitoring to ensure that patients can benefit from appropriate social care.
Resource utilisation reflects the organisation of the Italian health care system, but certain tendencies are similar to the other countries. For example, compared to the study in 2005, inpatient care has declined very much, while the use of DMTs and of MRIs has increased. 5 However, the decrease in inpatient care may also partly be explained by fewer patients reporting a relapse than in 2005 as relapses often lead to hospitalisation. Similarly, the high percentage of DMT users in this study may partly be explained by the overrepresentation of patients with early or mild disease. The proportional use of specific DMTs was comparable to what is recorded in the Italian Barometer of MS in 2016 (www.aism.it). The considerable use of newer DMTs (almost 40% of users) may explain the increase in day admissions seen in this study, as a result of drug administration for some of the newer treatments. It also contributes to the overall increase in DMT costs, highlighted also in other studies,8,27,28 and representing about 75% of total costs for patients with mild disability.
Some of the other differences with the 2005 study also appear to be driven mostly by the fact that patients in the earlier sample had more severe disability: in this study, fewer patients had physiotherapy sessions, fewer had invalidity pensions and fewer used informal care. However, the proportion of patients requiring informal care increased from 24% at EDSS of 0–3 to 60% at EDSS of 4–6.5 and 78% at EDSS of 7–9. For this latter group, informal care represented over 20% of the total cost. Our findings appear to reflect the strong family ties in the Italian society and a specific attitude towards the use of family help.
An important finding of this study is the overwhelming presence of fatigue in almost all patients and the importance of cognitive difficulties, regardless of disease severity, seen also in other studies.29,30 Similarly, problems with anxiety and depression are present at the same level (in around 50% of the patients) throughout the disease. While our data do not allow investigating causal effects, it is of note that in all 16 countries in the study, a substantial number of patients are not able to work due to MS already very early in the disease and with basically no physical disability. Thus, the results of our study corroborate previous findings in German MS patients that ‘invisible’ symptoms such as fatigue, cognitive difficulties and mood disorders may have an enormous impact on work ability. 31
In conclusion, these data not only contribute to the existing literature on cost of MS but also characterise various aspects of the burden of MS on patients and society and capture patterns of resource utilisation that could inform future policy recommendations. In addition, these data provide input into cost-effectiveness analyses for reimbursement decisions.
Footnotes
Acknowledgements
The authors are grateful to Daiana Bezzini and Paola Zaratin (FISM) for supporting data collection, to Jennifer Eriksson and Mia Gannedahl (MAPI Group) for organisational and statistical support, to Barbara Rosengren for language editing and to Cara Harley for formatting.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: M.B. and M.P. have no conflicts of interest to declare; G.K. has received consulting fees from Almirall, Bayer, Biogen, Merck Serono, Novartis, Oxford PharmaGenesis, Sanofi Genzyme and Teva; and J.B., D.C. and J.D. were at the time of the study employed by the Mapi Group, a research company acting as consultants to pharmaceutical companies.
Funding
The author(s) declared receipt of the following financial support for the research, authorship and/or publication of this article: European Health Economics and MAPI have received funding for the full research and production of the manuscripts from Biogen.