
Abstract
Background:
The role of diet in multiple sclerosis (MS) is largely uncharacterized, particularly as it pertains to pediatric-onset disease.
Objective:
To determine the association between dietary factors and MS in children.
Methods:
Pediatric MS patients and controls were recruited from 16 US centers (MS or clinically isolated syndrome onset before age 18, <4 years from symptom onset and at least 2 silent lesions on magnetic resonance imaging). The validated Block Kids Food Screener questionnaire was administered 2011–2016. Chi-squared test compared categorical variables, Kruskal–Wallis test compared continuous variables, and multivariable logistic regression analysis was performed.
Results:
In total, 312 cases and 456 controls were included (mean ages 15.1 and 14.4 years). In unadjusted analyses, there was no difference in intake of fats, proteins, carbohydrates, sugars, fruits, or vegetables. Dietary iron was lower in cases (p = 0.04), and cases were more likely to consume below recommended guidelines of iron (77.2% of cases vs 62.9% of controls, p < 0.001). In multivariable analysis, iron consumption below recommended guidelines was associated with MS (odds ratio = 1.80, p < 0.01).
Conclusion:
Pediatric MS cases may be less likely to consume sufficient iron compared to controls, and this warrants broader study to characterize a temporal relationship. No other significant difference in intake of most dietary factors was found.
Keywords
Introduction
Multiple sclerosis (MS) typically onsets early in adulthood (age 20–40 years), but may extend into extremes of age. Cases of pediatric-onset MS (before age 18) are thought to account for approximately 3–5% of current adult MS patients. They constitute an important minority of cases as the study of factors early in life which could affect their disease may provide important insight into the disease more generally..1,2 Much remains to be elucidated in our understanding of MS pathophysiology, 1 and the role of dietary factors in influencing MS risk and progression remains largely uncharacterized, yet is a topic of frequent concern and anxiety for patients and their relatives. Dietary modifications such as increased use of dietary supplementation or adherence to classical “healthy” diets such as a Mediterranean or a low-fat, high-fiber diet are often adopted by those affected on anecdotal indications. 3 There are currently no dietary guidelines for patients with MS and their at-risk relatives. Disease association studies in this regard have so far focused on the roles of vitamin D and obesity, both of which are partly determined by diet, and for which a relatively consistent evidence base is now in place.4,5 Epidemiological findings such as that of latitudinal gradient of MS prevalence render the notion that MS is more prevalent in countries with a diet typically rich in its intake of calories, fat, dairy, and sugar. 6 The study of nutritional factors as they pertain to MS, and particularly pediatric MS, is however logistically difficult, and as such, studies to date have often been conducted in adult MS patients some time after disease onset, incorporating long retrospective periods (prone to recall bias) and with multiple possible confounding factors and a resulting limited evidence base of inconsistent findings.7–9 The possibility of dietary components acting as possible modifiable factors in pediatric MS susceptibility or progression means that establishing differences in dietary behavior between cases and controls, if any exist, potentially important for guiding future work on risk and/or disease management. This study utilized data from a multi-center case-control study to investigate associations between dietary intake and pediatric MS.
Materials and methods
Pediatric MS cases and controls
Children with MS were recruited from 16 MS centers at general pediatric hospitals in the United States (including University of California, San Francisco; State University of New York at Buffalo; University of Alabama at Birmingham; Boston Children’s Hospital; Massachusetts General Hospital; Mayo Clinic, Rochester; Stony Brook University Medical Center; Texas Children’s Hospital Baylor and Baylor College of Medicine; Loma Linda; Children’s Hospital of Philadelphia; Ann & Robert H. Lurie Children’s Hospital of Chicago; Children’s Hospital Colorado; University of Texas Southwestern; Children National; Primary Children’s Hospital, Salt Lake; Washington University in St. Louis) to take part in an ongoing case-control study of genetic and environmental risk factors for pediatric MS. Children from these centers were eligible for inclusion if they were between ages 3 and 21, had MS (in accordance with the McDonald MS criteria) or clinically isolated syndrome onset prior to age 18, were less than 4 years from symptom onset, and had at least 2 silent lesions on magnetic resonance imaging. 10 All cases were ascertained by a panel of at least two pediatric MS experts.
Control subjects were recruited from children under the age of 22 who were patients or siblings of patients at the same medical centers. Children were included if they had no personal history of autoimmune disease, no history of treatment with immunosuppressive therapy, no history of severe health conditions (individuals with asthma and eczema were included in the study), and no parental history of MS. Usually, one control subject was included per family and could be of any birth order within that family. Of note, there were two families with two eligible controls; in this case, the oldest child was selected for inclusion.
Questionnaires
Cases and controls or their parents, as appropriate, were asked to complete a standardized questionnaire before clinic visit incorporating the subject’s development, environmental exposures, medical history, demographic information (including age, sex, self-reported ethnicity (Hispanic/non-Hispanic), and race (American Indian/Alaska Native, Asian, Black/African American, Native Hawaiian/Pacific Islander, or White). In the vast majority of cases, the questionnaire was completed by the parents, as was true for both cases and controls. Ethical approval was obtained from the institutional review board at each institution. All participants and one of their parents signed assent and consent forms before enrollment.
Dietary intake of fiber, fat, protein, carbohydrate, fruit, vegetables, dairy, and iron was assessed through the Block Kids Food Screener (BKFS) self-report questionnaire, administered between November 2011 and January 2016 to cases and controls to be completed at the time of enrollment in the study. The included dietary variables were selected at the start of the study prior to commencement of analysis and selected as they were included in a data dictionary listing nutrients for which the questionnaire was designed (not including, for example, reliable capture of vitamin D intake), and for which the authors felt there were putative mechanisms or previous suggestion of an influence on MS or other neurological diseases. The BKFS was developed in 2007 by NutritionQuest and is a simple method of dietary assessment that has been validated against three, 24-hour dietary recalls in children aged 10–17 and takes approximately 10–12 minutes to complete. 11 The de-attenuated correlations (mitigating a weakening effect of measurement error on the correlation coefficient) for which the questionnaire was specifically validated (and from which other, particularly micronutrient information, was inferred) were fruit (de-attenuated correlation 0.60), vegetable (0.53), potatoes (0.88), legumes (0.82), whole grains (0.64), dairy (0.87), meat/fish/poultry (0.68), kcalories (0.66), protein (0.70), saturated fat (0.77), added sugar (0.48), glycaemic load (0.59), and glycaemic index (0.57). 11
The questionnaire consists of 41 questions that evaluate the frequency and portions of foods and beverages consumed during the preceding week. For specific questions, such as type of cereal and type of milk, participants were asked to select the response corresponding to the item they consumed the most. Subjects were instructed to select the frequency (none last week, 1 day, 2 days, 3–4 days, 5–6 days, or everyday) and then the food-specific portion size (e.g. 1 slice, 2 slices, or 3+ slices) that most closely matched their intake. The USDA’s (US Department of Agriculture) My Pyramid Equivalents Database (MPED; version 2.0 for USDA Survey Foods, 2003–2004) was used in identifying defined cup equivalents for portion sizes, and the food codes from BKFS food list were linked to the USDA’s Food and Nutrient Database for Dietary Studies (FNDDS) and the USDA’s MPED (Continuing Survey of Food Intakes by Individuals 2012). 11 The food list used in the BKFS was determined by analysis of data collected from the National Health and Nutrition Examination Survey, which incorporated almost 10,000 dietary recalls of 24-hour dietary recall information, 2002–2006. 11 The nutrient and food group analysis database for the BKFS was based upon consumption and population-weighted age–sex group of mean nutrient and food group dietary intake. 11
The BKFS was completed by subjects or their caregivers in accordance with instructions received from research staff. Subjects were excluded if they left >15 responses empty on the questionnaire or consumed an average daily calorie intake of <500 or >5000 kcal/day based on their responses (n = 22 excluded based on <500 kcal/day caloric estimate).
Statistical analysis
Analyses were performed using SAS Version 9.4 (SAS Institute, Cary, NC, USA). Chi-squared test was used to compare categorical variables and Kruskal–Wallis test was used to compare continuous variables to test an association between dietary intake variables and disease status (case status vs control status). Dietary intake recommended guidelines for different age groups were obtained from the Dietary Guidelines for Americans 2010 and the Institute of Medicine (US) Food and Nutrition Board.12,13 Multivariate logistic regression was done adjusting the results for age, sex, ethnicity, race, body mass index (BMI), and socioeconomic status using a multivariate logistic regression model.
Height and/or weight were missing for a number of participants (17 cases and 86 controls), and for these individuals, it was not possible to calculate BMI. Using CDC (Centers for Disease Control and Prevention) stature-for-age and weight-for-age growth charts, we approximated the age- and gender-specific z-scores of height and weight for cases and controls. We then applied the Markov chain Monte Carlo method of multiple imputation to obtain 10 imputed sets of z-scores for height and weight from case-control status, race, ethnicity, socioeconomic status, and the dietary effects (protein, carbohydrate, fat intake, etc.). Imputed sets of BMI were calculated for participants with missing height and/or weight data by back-transforming the z-scores for heights and weights. Sensitivity analyses were also performed by removing subjects for whom BMI was not available.
Results
Case and control characteristics
A total of 312 cases (mean disease duration 10.8 months) and 456 controls were included in the analysis population (percent females 62.5% and 52.9%, respectively; mean ages 15.1 and 14.4 years, respectively) (Figure 1). Baseline demographic characteristics of cases and controls are shown in Table 1.
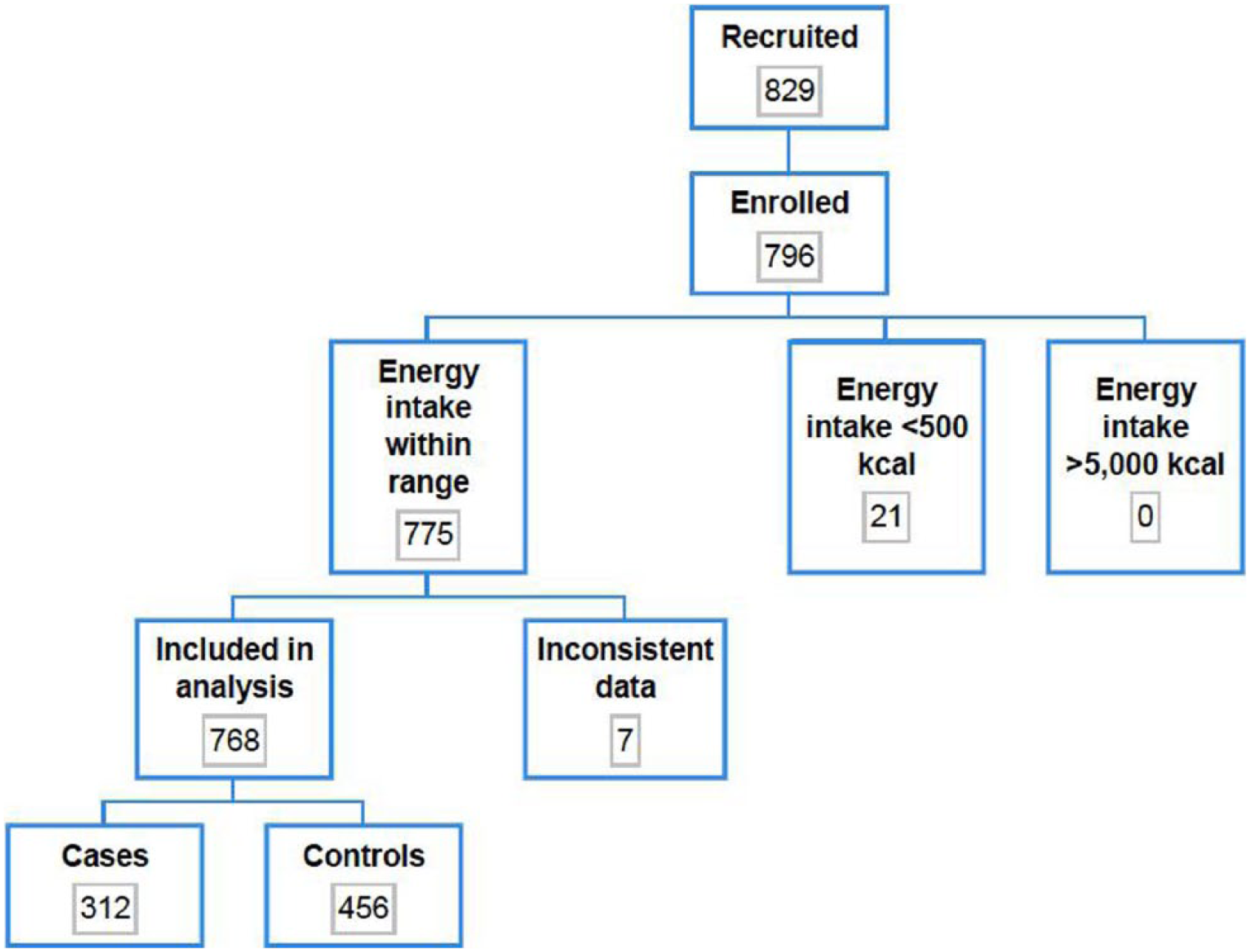
Flowchart of number of participants (cases and controls) evaluated for study inclusion.
Baseline characteristics of cases and controls.
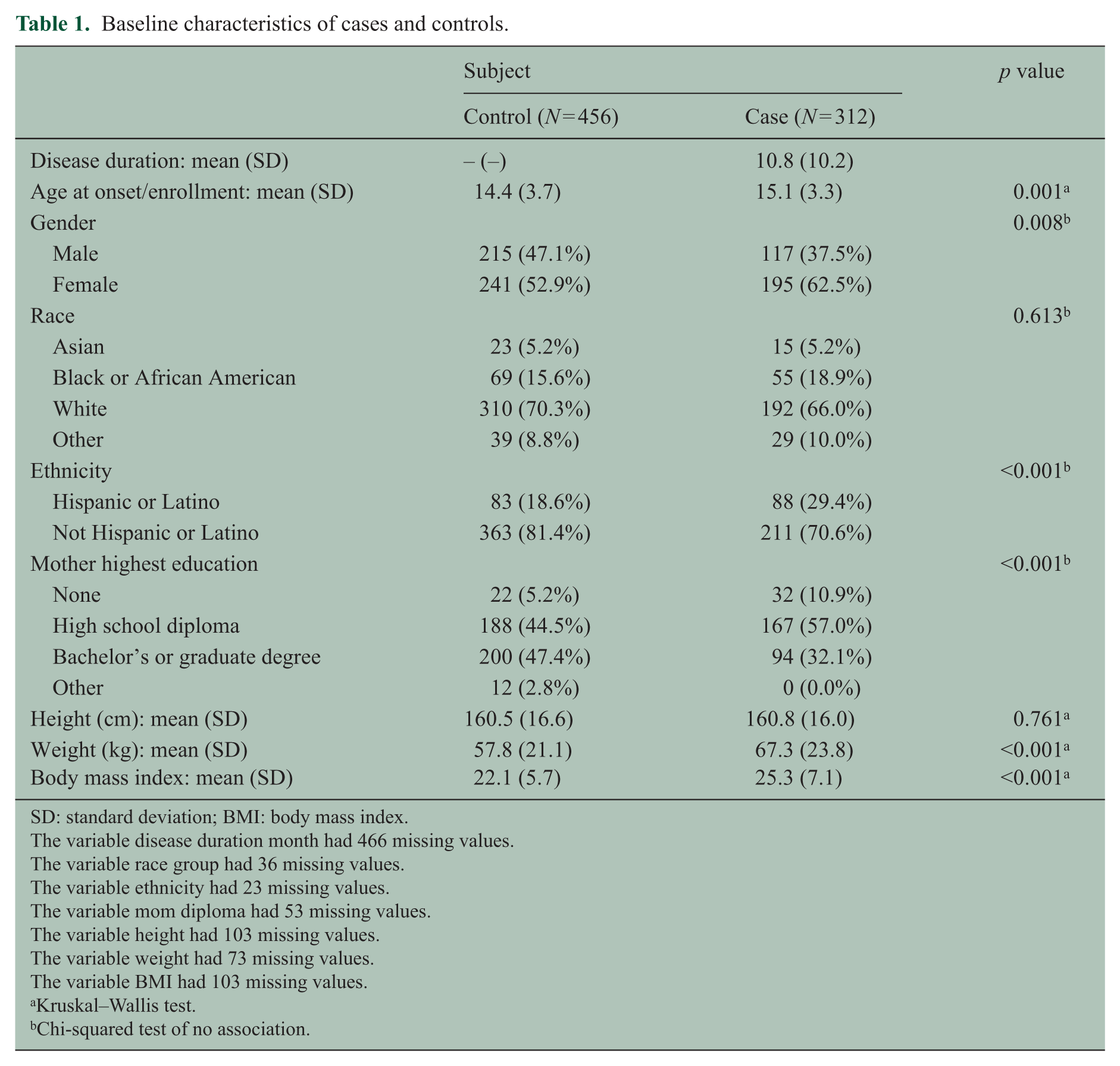
SD: standard deviation; BMI: body mass index.
The variable disease duration month had 466 missing values.
The variable race group had 36 missing values.
The variable ethnicity had 23 missing values.
The variable mom diploma had 53 missing values.
The variable height had 103 missing values.
The variable weight had 73 missing values.
The variable BMI had 103 missing values.
Kruskal–Wallis test.
Chi-squared test of no association.
Mean dietary intake in cases and controls
Baseline dietary intake for various nutrients is shown for each group in Table 2. Average dietary intake of fiber, iron, and dairy was significantly lower in cases compared to controls (p = 0.04, p = 0.04, and p = 0.01, respectively) (Table 2). In analysis of males and females separately, only average dietary fiber consumption in males differed between cases and controls (12.5 vs 11.3 g in controls vs cases, p = 0.04).
Average dietary intake of cases and controls.
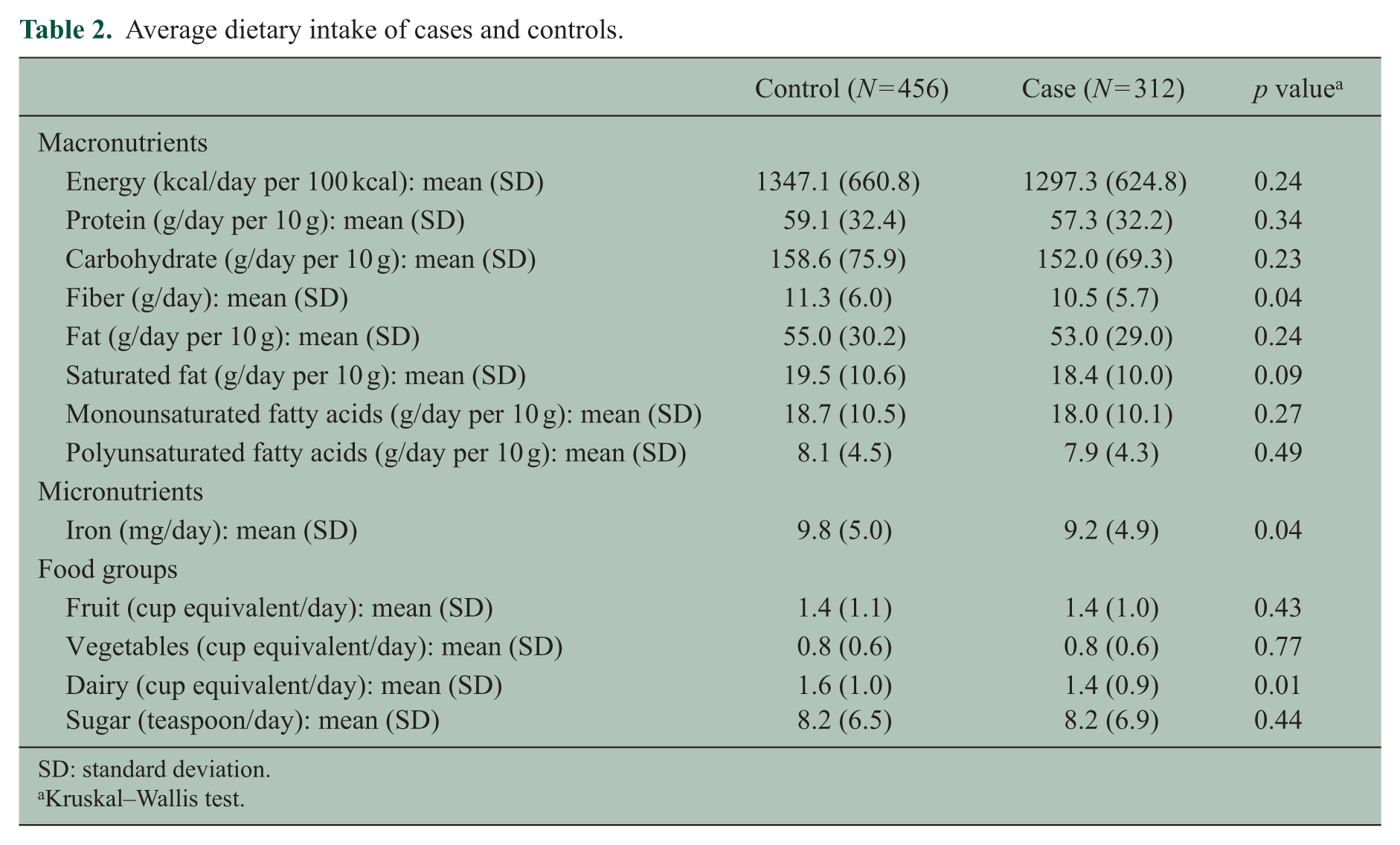
SD: standard deviation.
Kruskal–Wallis test.
There was no significant difference between the mean calorie intake for cases (1297 kcal/day) and controls (1347 kcal/day, p = 0.24), and mean percentage energy intake from protein, carbohydrate, and fat did not differ between cases and controls (17.5% vs 17.4%, p = 0.50; 47.6% vs 47.8%, p = 0.51; 36.3% vs 36.3%, p = 0.73, respectively). These remained insignificant in subgroup analysis of males and females separately. There was no difference between cases and controls in the likelihood of exceeding, being within, or consuming less than recommended dietary intake of protein, carbohydrate, fat, or fiber. Cases were, however, significantly more likely to consume less than recommended average dietary intake of iron (77.2% of cases vs 62.9% of controls, p < 0.001).
Multivariate association between dietary intake and pediatric MS
In analyses adjusted for age, sex, ethnicity, race, BMI, and socioeconomic status using a multivariate logistic regression model, there was no difference between cases and controls in average dietary intake of energy, fats, proteins, carbohydrates, sugars, fruits, vegetables, dairy, fiber, or iron (Table 3). However, multivariable analysis of categorical effects showed that “low” iron intake was associated with an increased MS risk (odds ratio = 1.80, 95% confidence interval (CI) 1.24–2.62, p < 0.01) (Table 4). Furthermore, multivariable models additionally adjusting for total energy intake did not markedly differ on any of the results. When analyses were repeated after removing subjects for whom BMI was imputed, the results were very consistent, and the magnitude and significance of the low iron effect remained (odds ratio = 1.70, 95% CI 1.15–2.52, p = 0.01). When analyses were repeated including only overweight or obese subjects for whom BMI data were available, the data were similarly consistent (Table 5).
Odds ratio estimates from multivariable analysis of pediatric multiple sclerosis by nutrient intake a .
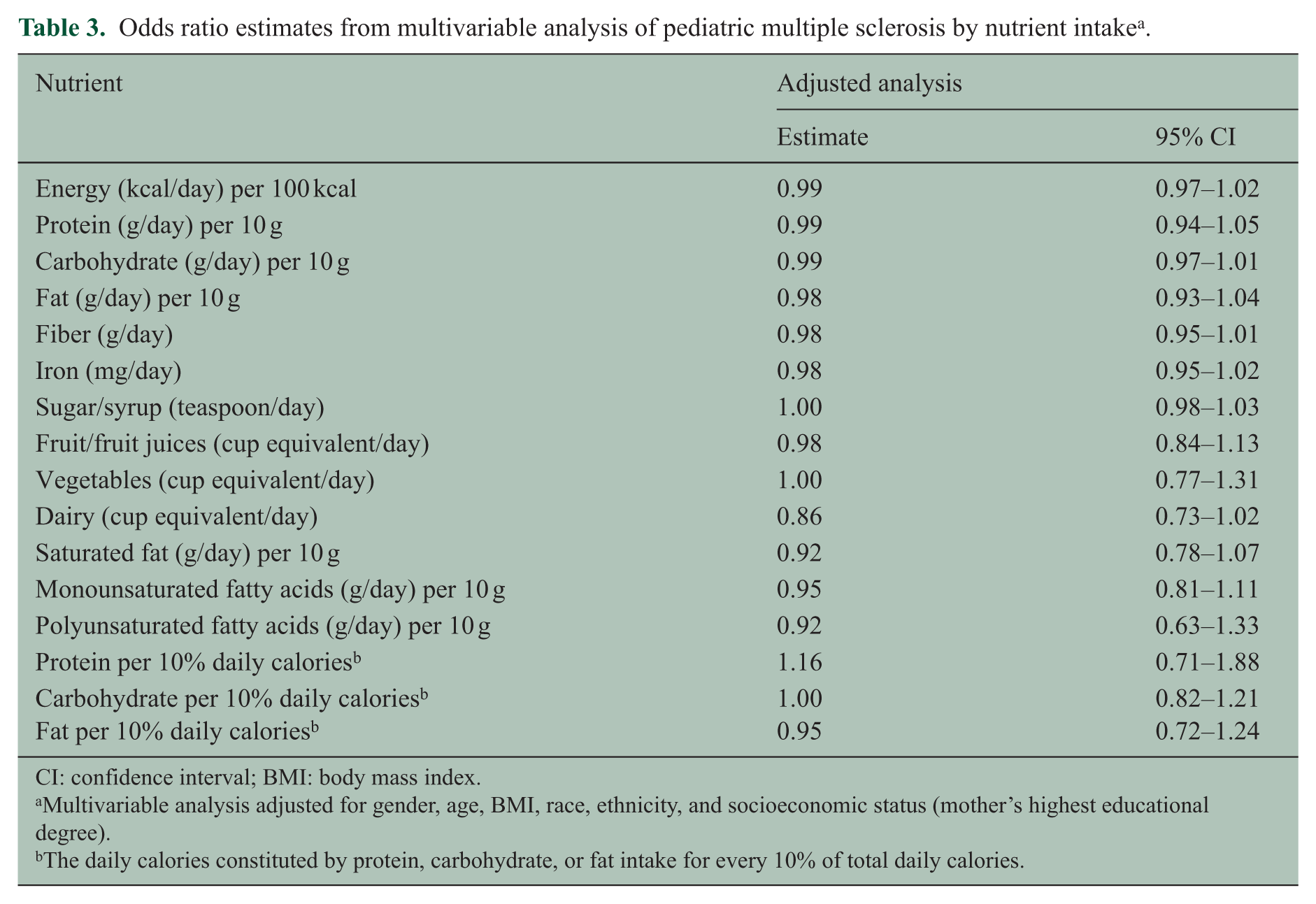
CI: confidence interval; BMI: body mass index.
Multivariable analysis adjusted for gender, age, BMI, race, ethnicity, and socioeconomic status (mother’s highest educational degree).
The daily calories constituted by protein, carbohydrate, or fat intake for every 10% of total daily calories.
Multivariable analysis of categorical nutrient intake a .
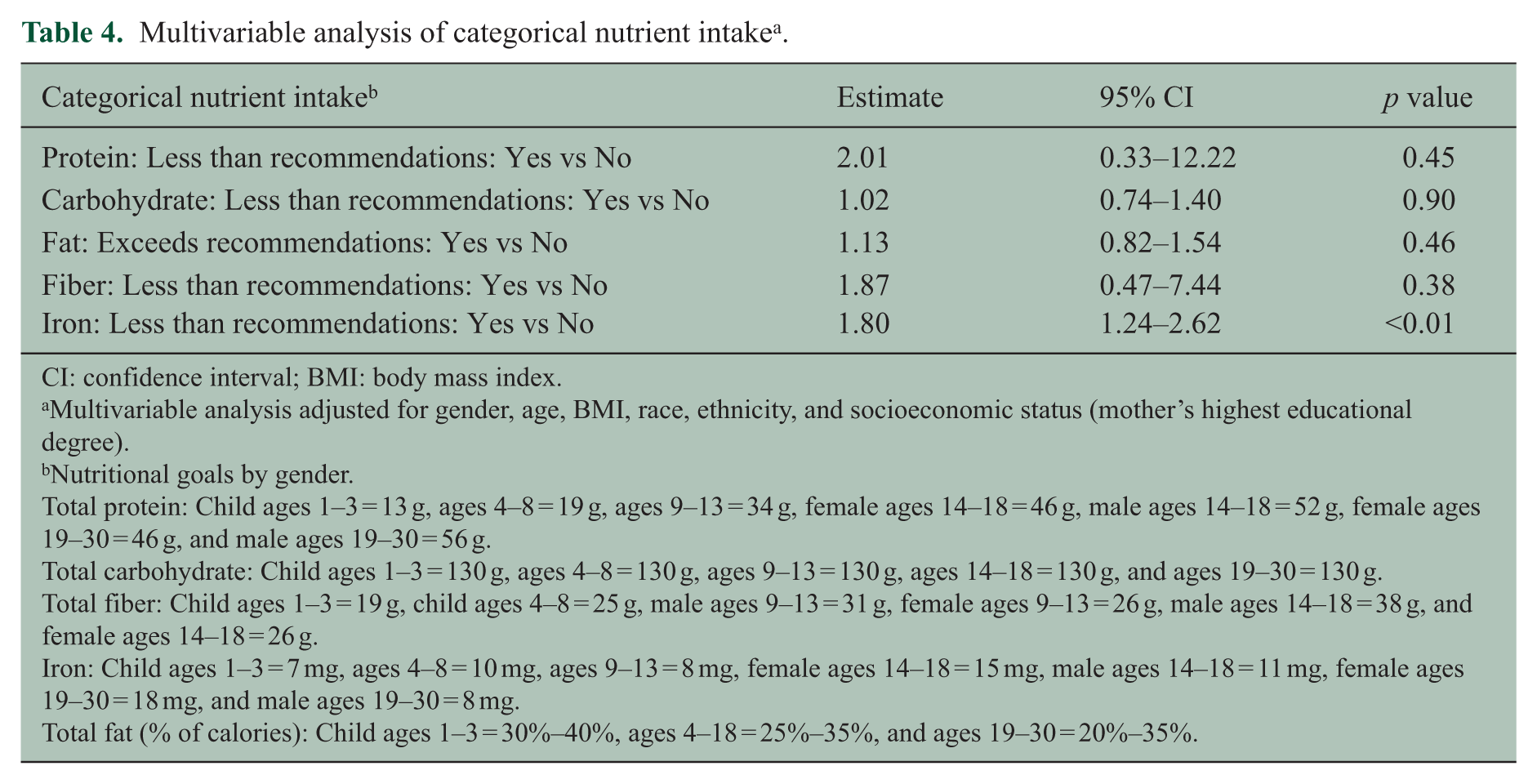
CI: confidence interval; BMI: body mass index.
Multivariable analysis adjusted for gender, age, BMI, race, ethnicity, and socioeconomic status (mother’s highest educational degree).
Nutritional goals by gender.
Total protein: Child ages 1–3 = 13 g, ages 4–8 = 19 g, ages 9–13 = 34 g, female ages 14–18 = 46 g, male ages 14–18 = 52 g, female ages 19–30 = 46 g, and male ages 19–30 = 56 g.
Total carbohydrate: Child ages 1–3 = 130 g, ages 4–8 = 130 g, ages 9–13 = 130 g, ages 14–18 = 130 g, and ages 19–30 = 130 g.
Total fiber: Child ages 1–3 = 19 g, child ages 4–8 = 25 g, male ages 9–13 = 31 g, female ages 9–13 = 26 g, male ages 14–18 = 38 g, and female ages 14–18 = 26 g.
Iron: Child ages 1–3 = 7 mg, ages 4–8 = 10 mg, ages 9–13 = 8 mg, female ages 14–18 = 15 mg, male ages 14–18 = 11 mg, female ages 19–30 = 18 mg, and male ages 19–30 = 8 mg.
Total fat (% of calories): Child ages 1–3 = 30%–40%, ages 4–18 = 25%–35%, and ages 19–30 = 20%–35%.
Odds ratio estimates by nutrient intake from multivariable analysis of overweight or obese pediatric multiple sclerosis cases (N = 122) and controls (N = 85) a .
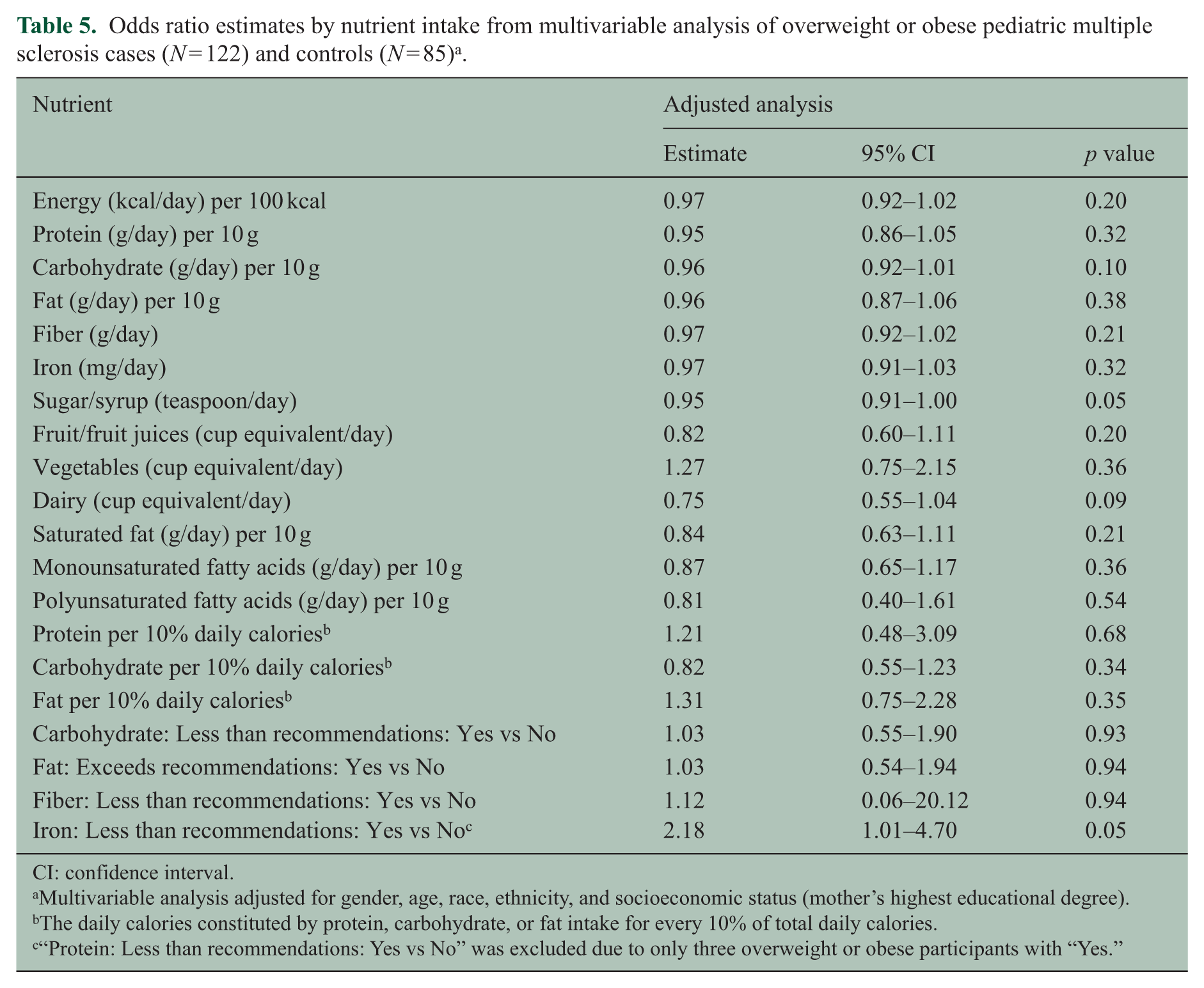
CI: confidence interval.
Multivariable analysis adjusted for gender, age, race, ethnicity, and socioeconomic status (mother’s highest educational degree).
The daily calories constituted by protein, carbohydrate, or fat intake for every 10% of total daily calories.
“Protein: Less than recommendations: Yes vs No” was excluded due to only three overweight or obese participants with “Yes.”
Discussion
This multi-center study suggests that there is no strong association between dietary intake of fiber, fat, carbohydrate, protein, fruits, vegetables, or dairy consumption, and pediatric MS. The data are suggestive of a presence of lower iron intake among cases of pediatric MS, and this observation warrants broader investigation in longitudinal studies.
To our knowledge, no other study has previously investigated the association between these dietary components and pediatric MS. Previous works exploring associations between adult MS and diet have been of conflicting results and of varied quality of methodology. Although it may be postulated that a Western diet high in, for example, saturated fats may influence MS, as has been suggested by some prior work, 14 the majority of studies including the only prospective study on this topic, which utilized two large cohorts of American women, have not found data supportive of this.15–17
However, an adult Australian case-control study of 267 cases examined any association between fat intake and risk of first clinical demyelinating event in a multi-center case-control study, also using a food frequency questionnaire. They found a significant reduction in risk of first clinical demyelination with higher omega-3 polyunsaturated fat dietary intake, with no observed association with total fat intake or other types of fat. Although we were unable to assess omega-3 specifically, further work may wish to investigate any role of omega-3 and other micronutrients in children with demyelinating disease. 18 Our results demonstrate a significantly higher weight and BMI among cases compared to controls, in support of existing evidence linking childhood obesity to an increased MS risk. 4
Intake of fruit and vegetables was similarly not found to be associated with MS in a Moscow hospital-based case-control study. 9 This was supported by the findings of a Canadian case-control study which reported no association with intake of fruit or vegetables, but did report a negative association between MS and intake of fiber (p = 0.05) and fruit juices, and a positive association between MS and intake of calories, animal fat, pork, and sweets/candy (females only). 8 No associations between intake of dietary carotenoids, vitamin C and vitamin E, and risk of MS were reported in a large American study. 19
Emerging research has linked deviations in the gut microbiota to modulation of the host immune system, and although we did not find evidence to support a strong association between pediatric MS and fiber, low dietary fiber intake has previously been postulated to promote a dysbiotic gut microbiome and a low-grade systemic inflammatory state which may contribute to MS.20,21
Our data suggesting lower iron intake in pediatric MS compared to controls are interesting in light of the long discussed area of whether iron has, if any, a harmful or helpful role in MS. 22 More recently, this debate garnered much attention following the emerged chronic cerebrospinal venous insufficiency (CCSVI) hypothesis of MS, suggesting the presence of harmful periventricular iron deposits in the brain. 23 Difficult to reason with this notion is the subsequent report that iron depositions are similar in groups with benign and secondary progressive MS. 24 Other work has also proposed that MS pathogenesis and/or clinical course may be influenced by abnormal iron depositions in the brain resulting in neurodegeneration.22,23 Furthermore, an association between shorter stature in children and iron deficiency has been suggested, but notably heights were similar across cases and controls in this study. 25
We consider that both deficiency and overloading of iron may impact normal functioning of both immune and neuronal cells and that balanced intake may be what is most important. Oligodendrocytes need high amounts of iron for the biochemical reactions involved in the maintenance of the large and complex myelin sheath.22,26,27 Microglia provide essential components such as iron to oligodendrocytes and in the case of mature oligodendrocytes achieve this through H-ferritin, an iron transfer system used solely by oligodendrocytes, in line with their heightened need. 22 This may speculatively render oligodendrocytes particularly vulnerable in states of iron deficiency. 26
Iron deficiency may also influence MS through its effect on immune system functioning and may result in thymus atrophy, impaired T-cell development, and reduced peripheral T cells. The iron transporter natural resistance-associated macrophage protein 1 (NRAMP1) has also been associated with numerous autoimmune diseases, implicating iron in their development. 28 Importantly, as this is a cross-sectional study, we are unable to determine a temporal relationship between low iron and pediatric MS, and our findings in this regard should therefore be considered hypothesis generating, rather than definitive. Whether a relationship between iron and MS exists, and in whichever direction of effect, will necessitate further investigation of whether altered iron levels are part of a mediating process in MS or part of its sequelae.
The strengths of this study include the relatively large number of pediatric cases (recruited across 16 US sites) with a diverse pediatric patient population, the evaluation of different dietary components using the same methodology, and careful case ascertainment. In addition, cases were enrolled early after onset (mean disease duration 11 months), and thus were unlikely to have changed their diet as there are no recommendations at this time about iron intake and MS. Limitations include that this is not a prospective study begun prior to MS onset (notably, we aimed to mitigate the impact of this by only including cases if they were within 4 years from symptom onset, but we cannot exclude the possibility that subjects changed their dietary habits between MS onset and the time of the study), the possibility of recall bias (we aimed to mitigate this by only asking for dietary data from the preceding week), the fact that the BKFS was not designed specifically for the assessment of all the selected nutrients, and a resulting potential tendency for underestimation of nutrient intake (we therefore cannot exclude undetected small effects). The validation study had notably not defined ethnicity of the participants to confirm the study is validated for specific food groups more greatly consumed in, for example, Hispanic populations. However, the BKFS is designed to ask specifically about dietary components which are more common among the Hispanic populations (e.g. burritos and Mexican fruit drinks). Furthermore, despite the fact that control children were also seen as patients in the same medical centers, we cannot exclude the possibility of selection bias. It is possible that the conditions for which the children were seen in clinic may have affected their diets, and these control children may therefore not be representative of children in the general population. However, most controls were enrolled from general pediatric clinics and as such a selection bias is less likely. In addition, the similarities of total mean calorie intake and mean percentage intake from protein, carbohydrate, and fat in both groups suggest overall a lack of bias in control enrollment.
Caloric consumption may also be underestimated in teenage age groups (specifically 18–19) due to increased alcohol and coffee intake which were not assessed in this study. We are also unable to account for potential confounding factors including other known MS risk factors such as vitamin D levels or Epstein-Barr virus infection status. Furthermore, application of correction for multiple testing has not been formally applied, and we leave it to the reader to interpret the results in the context of the conducted analyses of a range of dietary factors.
In conclusion, in this exploratory study, we observed no strong associations between most investigated dietary factors and pediatric MS, but highlight that further work elucidating any relationship between iron and MS would be of interest. Future work should aim to conduct a prospective study of pediatric MS risk, investigate the role of specific vitamins and minerals, and investigate the influence of dietary factors on disease outcomes in already established disease (e.g. relapse rate) using a longitudinal study design. We nonetheless hope that these results will act as reassurance to parents of pediatric MS patients and contribute support toward current clinical practice which, at present based on the available evidence base, does not recommend any particular diet modifications (with the exception of vitamin D repletion) for children with MS.
Footnotes
Acknowledgements
The authors thank parents and children who have participated in this study and the study coordinators who have tirelessly enrolled subjects. J.P. prepared the plan of analysis, prepared the first draft of the manuscript, and presented data at meetings. E.W. designed the study and obtained funding to support the work. She also enrolled cases and controls and participated in data analysis and edited the manuscript. B.S. and J.C.M. helped on preparing the plan of analysis. J.S.G., T.S., A.T.W., T.E.L., A.B., B.M.G., B.W.G., G.A., J.M.T., J.H., J.M.N., Y.H., J.R., M.C., L.K., M.G., L.B., M.R., T.C., S.M., and I.K. enrolled cases and controls and edited the manuscript. S.L.C. provided support to prepare plan of analysis and edited the manuscript. J.R., S.R., M.W., and T.C.C. provided support to coordinate the study, prepared plan of analysis, analyzed data, and edited the manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Pakpoor reports no disclosures. Dr Graves was supported by the Foundation for Consortium of Multiple Sclerosis Centers and the NIH Bridging Interdisciplinary Research Careers in Women’s Health programs during this work. She has been a one-time consultant for EMD Serono. Dr Waubant is funded by the National MS Society, the NIH, and the Race to Erase MS. She volunteers on an advisory board for a clinical trial of Novartis. Dr Krupp is supported by the National MS Society, NIH, Robert and Lisa Lourie Foundation, and Department of Defense. She has received honoraria, consulting payments, grant support, or royalties from Biogen, Medimmune, Novartis, Teva Neuroscience, Sanofi-Aventis, and EMD Serono. Dr Weinstock-Guttman received honoraria for serving in advisory boards and educational programs from Teva Pharmaceuticals, Biogen Idec, Novartis, Acorda, EMD Serono, and Genzyme and Sanofi. She also received support for research activities from the National Institutes of Health, National Multiple Sclerosis Society, National Science Foundation, Department of Defense, EMD Serono, Biogen Idec, Teva Neuroscience, Novartis, Acorda, Genzyme, and the Jog for the Jake Foundation. Dr Tanuja Chitnis has served as a consultant for Biogen Idec, Teva Neuroscience, Novartis, Sanofi-Aventis, and has received grant support from NIH, National MS Society, Guthy-Jackson Charitable Foundation, CMSC, Merck Serono and Novartis. Dr Rose has research funding from Teva Neuroscience and Biogen. He is a member of the Medical Advisory Board for the DECIDE trial which is funded by Biogen and AbbiV. Dr Casper has been supported by the National MS Society and the NIH (R01NS071463). Drs Belman, Ness, Gorman, Lotze, Rodriguez, Aaen, and James report no disclosures. Janace Hart and Timothy Simmons report no disclosures. Dr Carmichael reports no disclosures.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by the National Institutes of Health NS071463 (PI Waubant) and by the National MS Society HC 0165 (PI Casper).