
Abstract
Background:
The fronto-striatal network has been implicated in both fatigue, a common multiple sclerosis (MS) symptom, and goal attainment, which has been shown to reduce fatigue in healthy individuals.
Objectives:
To investigate whether stimulation of the fronto-striatal network through goal attainment (potential monetary gain) leads to fatigue reduction in MS and healthy control (HC) participants.
Methods:
In all, 14 healthy and 19 MS participants performed a gambling task during functional magnetic resonance imaging (fMRI). Participants were presented with an opportunity to receive monetary reward during the outcome condition of the task but not during the no outcome condition. Self-reported fatigue measures were obtained after each condition and outside of the scanner. Structural alterations were also examined.
Results:
A significant decrease in fatigue was observed after the outcome condition compared to the no outcome condition in both groups. Significantly greater activation was observed in the ventral striatum in association with the outcome condition compared to the no outcome condition in both groups. Ventromedial prefrontal cortex showed significantly greater activation during the no outcome condition compared to the outcome condition with greater difference between conditions in the HC group.
Conclusion:
This is the first functional neuroimaging study showing that stimulation of the fronto-striatal network through goal attainment leads to decreased on-task fatigue in MS and healthy participants.
Introduction
Up to 90% of individuals with multiple sclerosis (MS) report significant fatigue, 1 which negatively impacts their quality of life and rehabilitation outcomes.2,3 However, the neural mechanisms affected in fatigue are still very poorly understood. Recent evidence implicates the fronto-striatal network in fatigue experienced by several clinical populations, including individuals with MS.4,5 One current hypothesis suggests that engagement of the fronto-striatal brain network might alleviate fatigue. 6
The fronto-striatal network is topographically organized7,8 and can be segregated into four fronto-striatal loops: the visual loop, the motor loop, the executive loop, and the motivational loop. 9 The ventral striatum (VS; nucleus accumbens) and the ventromedial prefrontal cortex (VMPFC) are part of the motivational loop and have been shown to be involved in goal attainment. 10 Specifically, animal studies show that unexpected outcome presentation (e.g. an outcome that follows a stimulus or an action) is associated with increased firing rate of striatal neurons. 10 Human neuroimaging studies show similar results, demonstrating differential activation of the fronto-striatal network to rewards and punishments (positive and negative outcomes).11,12
Furthermore, it has been shown that healthy individuals, who are fatigued after performing a demanding cognitive task, experience a decrease in fatigue when presented with a goal to win a monetary reward. 13 Such evidence of the motivating influence of reward on fatigue could lead to novel treatment approaches; however, such evidence is lacking in persons with MS.
In this study, we investigated whether fatigue can be reduced through the use of monetary rewards in persons with MS and whether the effects of goal attainment on both fatigue and fronto-striatal activation are comparable to healthy controls (HCs). A goal can be defined as a valenced cognitive representation of a future event or experience which drives one to act toward attaining it. 14 Thus, in this study, we address the hypothesis that having a goal, such as winning money during gambling, will alleviate fatigue in HC and MS participants through engagement of the fronto-striatal brain network. We also examined whether structural alterations such as VS volume loss or altered integrity of the internal capsule (i.e. the white matter pathway that connects the prefrontal cortex (PFC) with the VS) would interfere with fronto-striatal network activation.
Methods
Participants
In all, 19 participants with MS 15 (17 relapsing-remitting MS, 1 primary-progressive MS, and 1 secondary-progressive MS) and 14 HC participants consented to participate in this study. Demographic information is provided in Table 1. All participants were female. Participants were excluded if they reported a significant history of medical or psychiatric disorders, drug abuse, or learning disability. Participants with MS were at least 4 weeks post most recent exacerbation and use of steroids, benzodiazepines, or neuroleptics. The mean disease duration of those with MS was 15.47 (range, 4–27) years. The Institutional Review Board of Kessler Foundation approved the research protocol. All subjects were reimbursed for their time.
Demographic information.
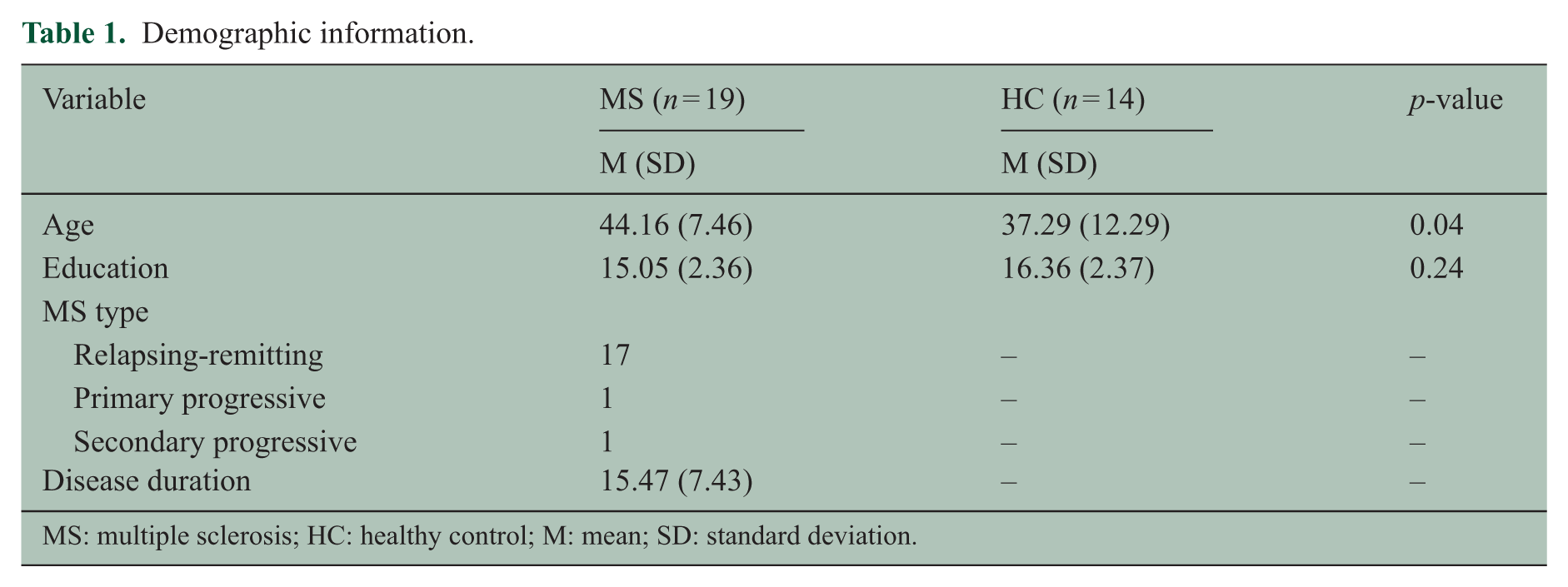
MS: multiple sclerosis; HC: healthy control; M: mean; SD: standard deviation.
Materials and procedure
Participants received a brain magnetic resonance imaging (MRI) scan conducted on a Siemens Skyra 3.0 T scanner (see Supplementary materials). “E-Prime” software was used for stimulus presentation and behavioral data acquisition.
Behavioral paradigm
Prior to beginning the neuroimaging procedures, participants were told that they would undergo MRI scanning while engaging in a card-guessing task. 12 The card-guessing task consisted of two conditions: outcome and no outcome. Participants were told that during the outcome condition they would be able to win a monetary bonus. Unbeknownst to participants, the probability of winning or losing was set to 50% in order for rewarding outcomes to stay unexpected. The bonus amount was fixed, regardless of performance (US$5). The no outcome condition served as the control condition.
During each trial of the outcome condition (Figure 1), participants were presented with an image of the back of a card for 4 seconds and had to guess whether the value on the front of the card was higher or lower than 5 (values ranged from 1 to 9, excluding 5). This was followed by a fixation point of varied duration (1–5 seconds). After the fixation point, participants were presented with feedback that reflected whether their guess was correct or incorrect: a green check mark indicated a correct guess and a win of US$1.00; a red X mark indicated an incorrect guess and a loss of US$0.50.
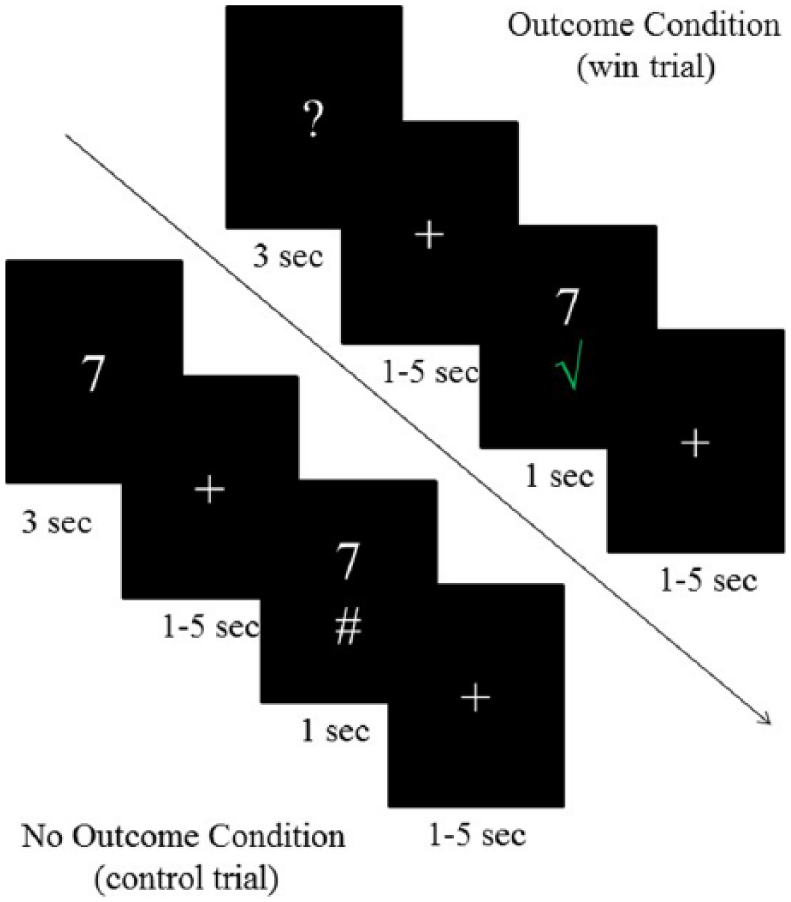
Depiction of the trial structure for the outcome and the no outcome conditions.
During each trial of the no outcome condition (Figure 1), participants viewed a card on every trial (4 seconds) that also showed its face (and therefore its number). They were instructed to indicate whether the value of the number was higher or lower than 5. This was followed by a fixation point of varied duration (1–5 seconds). After responding to the stimulus, participants were presented with a pound sign (#) to indicate that their response was recorded.
Task duration was approximately 22 minutes. There were two blocks per condition, each consisting of 60 trials, each lasting 7 seconds on average. The order of conditions and trials was randomized. Subjects were cued about the block they were in by seeing the question mark during the outcome block or the number during the no outcome block. After each block of each condition, participants were presented with a visual analogue scale (VAS-F) 16 to rate their state fatigue (i.e. current level of fatigue) on a scale from 1 (not at all) to 10 (extremely). All responses were recorded via an MRI-compatible button box.
At the end of the scanning session, participants filled out several questionnaires to assess trait fatigue (i.e. fatigue that is stable over time), depression, and motivational tendencies. Trait fatigue was assessed with the fatigue severity scale (FSS) and the modified fatigue impact scale (MFIS). These widely used questionnaires ask participants to rate fatigue-related statements based on what they experienced during the past week (FSS) and during the past 4 weeks (MFIS). Fatigue often co-occurs with depression, which has been shown to influence activity of the fronto-striatal network, 17 so participants also completed the Chicago Multiscale Depression Inventory (CMDI), a common depression assessment measure for MS.18,19 Motivational tendencies were assessed with the behavioral inhibition system/behavioral activation system (BIS/BAS) 20 questionnaire that assesses avoidance motivation and reward sensitivity, respectively. Participants also filled out a post-task questionnaire that inquired as to which condition was more engaging and how they felt in response to both correct and incorrect guessing during the outcome condition. These questions served as a manipulation check in order to make sure that the outcome condition stimulated goal attainment. This had an added advantage of allowing us to avoid reverse inference 21 from functional MRI data.
At the end of the study, participants were debriefed about the purpose of the experiment and were told that they (and all participants) received a fixed monetary bonus in the amount of US$5.
Data analysis
Behavioral data
Mean scores and standard deviations for each questionnaire were calculated for each participant and analyzed with independent-sample t-tests (MS vs HCs). To examine changes in state fatigue during task performance, a VAS-F difference score was computed for the outcome and no outcome conditions based on the participants’ fatigue ratings provided after each condition. State fatigue data from two MS participants were not obtained due to a computer error. A 2 × 2 mixed design analysis of variance (ANOVA) was conducted to examine differences between VAS-F scores (within-subject variable: outcome vs no outcome) and groups (between-subject variable: HC vs MS). Age was initially included as a covariate in our model; however, age did not significantly covary with VAS-F scores. Thus, age as a covariate was not included in the model. 22
fMRI data
Preprocessing of the functional data for each scanning run was performed using the Analysis of Functional NeuroImaging (AFNI) suite (https://afni.nimh.nih.gov/afni/) and entailed motion correction using six parameters, spatial smoothing (6 mm, full width at half-maximum (FWHM)), voxel-wise linear detrending, and despiking. The resulting data were warped into Talairach stereotaxic space. Motion parameters were included as regressors of no interest. A random-effects general linear model analysis with condition as a within-subject factor (outcome vs no outcome) and group as a between-subject factor (HC vs MS) was performed on regressors corresponding to the 1-second time period of outcome presentation (outcome condition and no outcome condition) and convolved with a canonical hemodynamic response function.
Small volume correction (SVC) 23 was performed on the VS and VMPFC since the main hypothesis is focused on these regions. Following Zink et al., 24 6-mm-radius spheres were drawn around the right and left VS (12, 8, −8). Based on a meta-analysis, 25 a 10-mm-radius sphere was drawn around the VMPFC (−16, 40, −18). The F threshold was set to 4.18 and parameter estimates were calculated for each condition (outcome vs no outcome) based on the voxels that survived pSVC < 0.05 in each region.
Structural MRI data
Gray and white matter volumes were calculated with SienaX. 26 Diffusion tensor imaging (DTI) measures were obtained using tract-based spatial statistics.27,28 Differences in VS volume were examined with FIRST (FMRIB’s Integrated Registration and Segmentation Tool). 29 To examine voxel-wise differences in VMPFC gray matter volume, we conducted voxel-based morphometry. 30 See Supplementary materials for detail.
Results
Behavioral results
VAS-F scores
ANOVA revealed a significant main effect of condition (F(29, 1) = 4.26, η = 0.13, p = .05; Figure 2). That is, in accordance with our hypothesis that goal attainment will have a general alleviating effect on the level of fatigue, both groups showed a significant reduction in VAS-F after the outcome condition relative to the no outcome condition. The interaction was not significant.
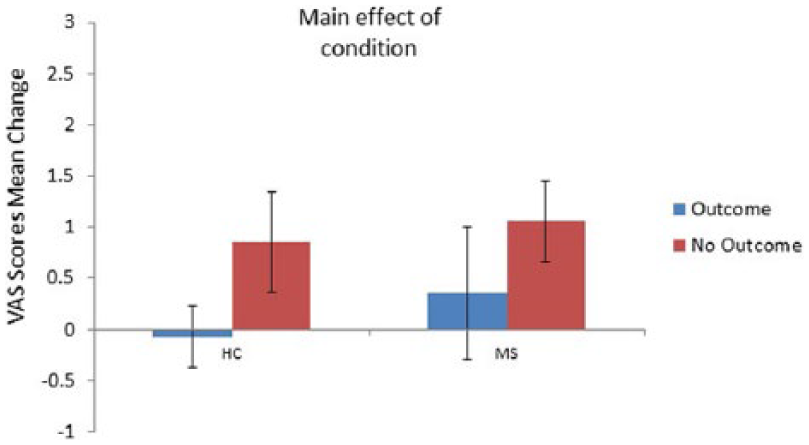
Mean change in VAS fatigue ratings from block 1 to block 2 of the outcome and no outcome conditions. Positive change indicates fatigue increase from block 1 to block 2; negative change indicates fatigue decrease from block 1 to block 2. Error bars represent standard error of the mean.
MRI results
VS
A significant main effect of condition was observed in the VS activation, bilaterally (left: F(29,1) = 7.62; right: F(29,1) = 7.99; psvc < 0.05; Figure 3; Table 2). That is, as was hypothesized, both groups showed increased VS activation during the outcome condition compared to the no outcome condition. The interaction was not significant.
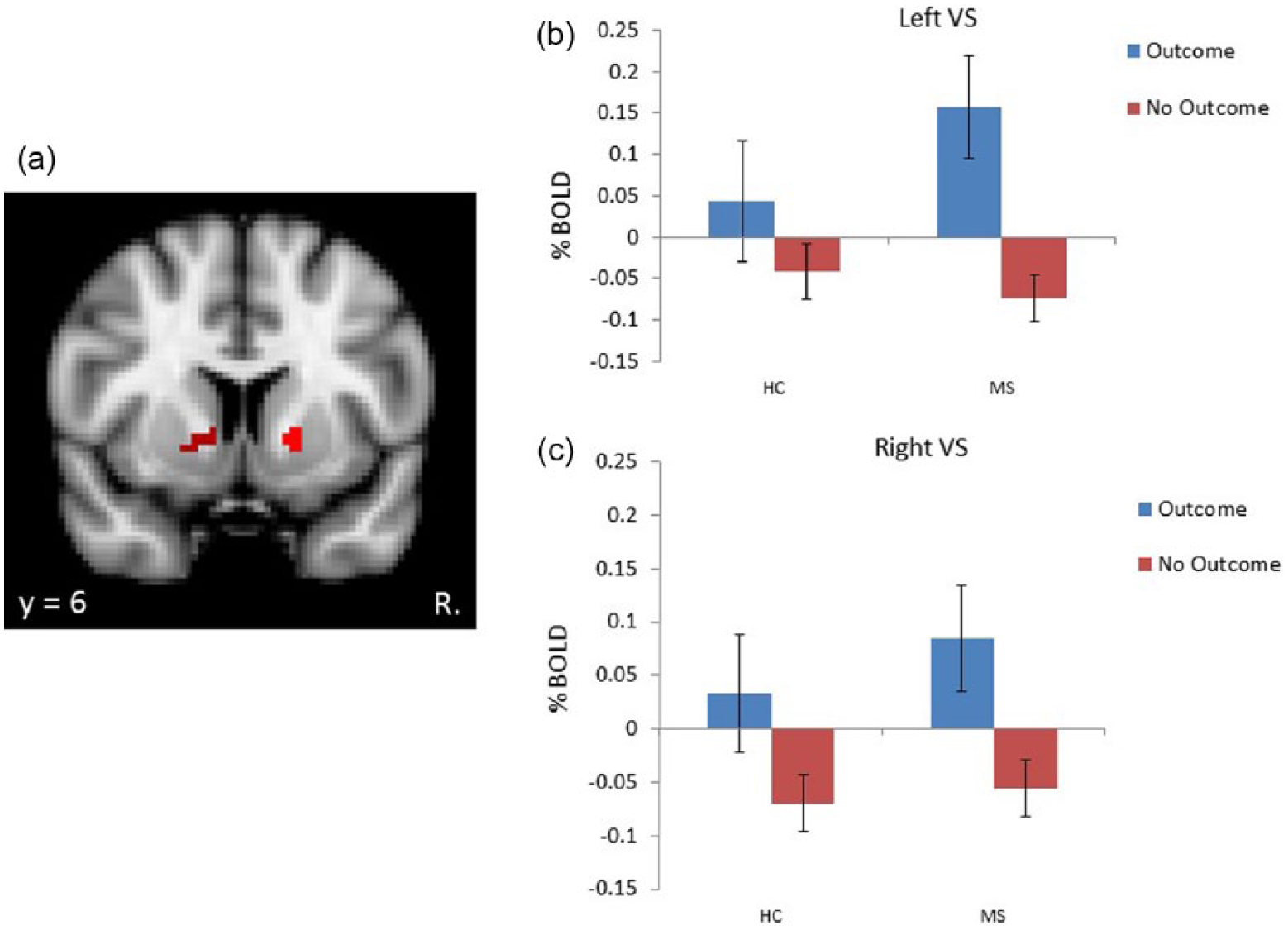
A. Depiction of activity in the striatum. B. BOLD activity from the left striatum (–16.5, 7.5, –1; Peak F=6.79) associated with the outcome and no outcome conditions. C. BOLD activity from the right stritum (13.5, 7.5, 1; Peak F=10.5) associated with the outcome and no outcome conditions. Error bars represent standard error of the mean.
Peak coordinates for each cluster within regions of interest.
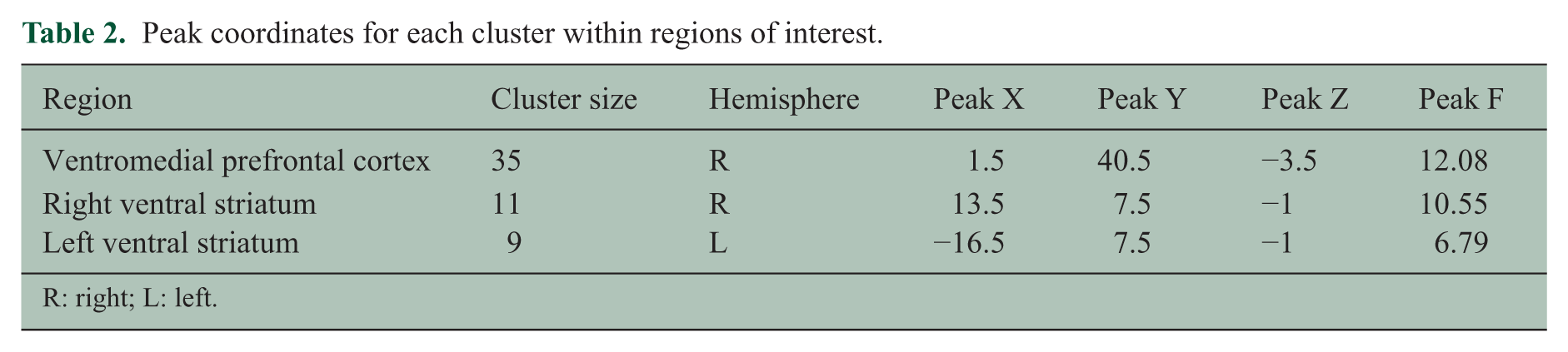
R: right; L: left.
VMPFC
The interaction of group × condition was significant in the VMPFC (F(29,1) = 3.4; psvc < 0.05; Figure 4; Table 2). The interaction was driven by greater activation in the HC compared to the MS group during the no outcome condition (t(30) = 1.85, p < 0.07). A main effect of condition was also observed (F(29, 1) = 27.24, p < 0.001).
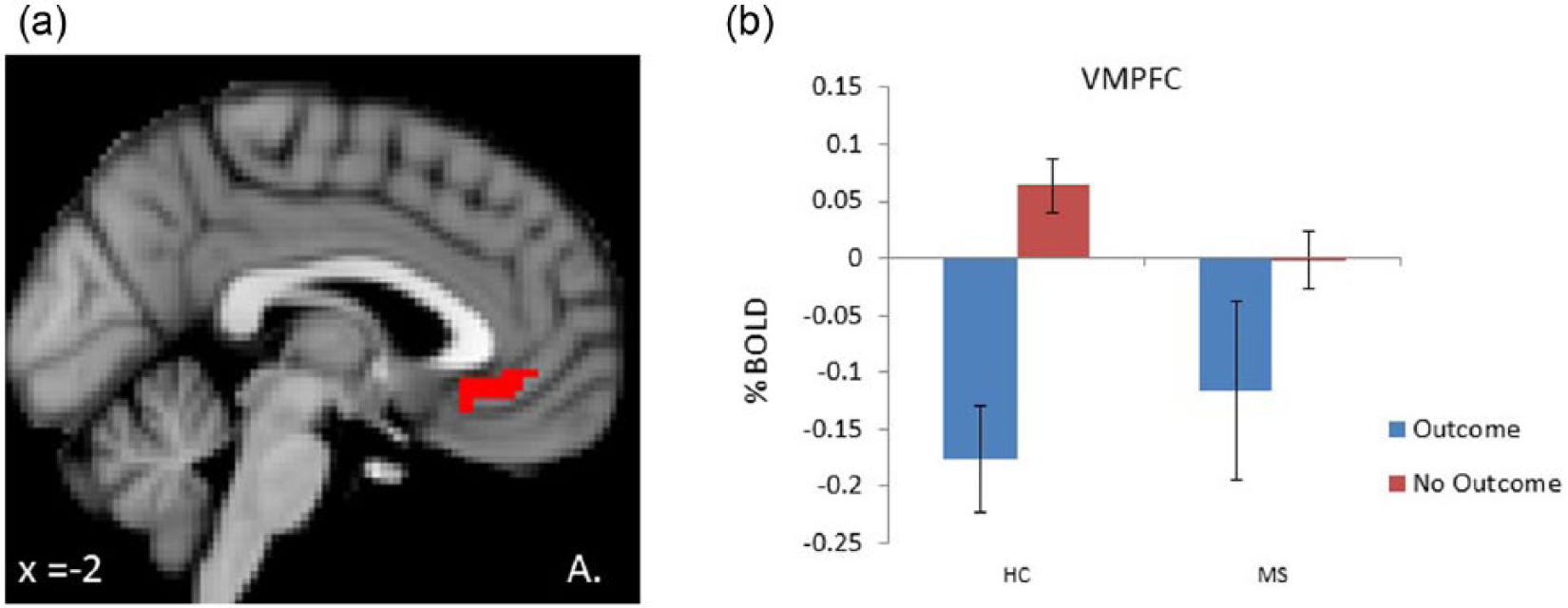
A. Depiction of activity in the VMPFC. B. BOLD activity from the VMPFC (1.5, 40.5, –3.4; Peak F = 12.08) associated with the outcome and no outcome conditions. Error bars represent standard error of the mean.
Structural MRI
The results for the structural MRI measures are displayed in Table 3. No difference in VS and VMPFC volume was observed between groups (see Supplementary materials for detail).
Structural MRI measures of multiple sclerosis patients and healthy controls.
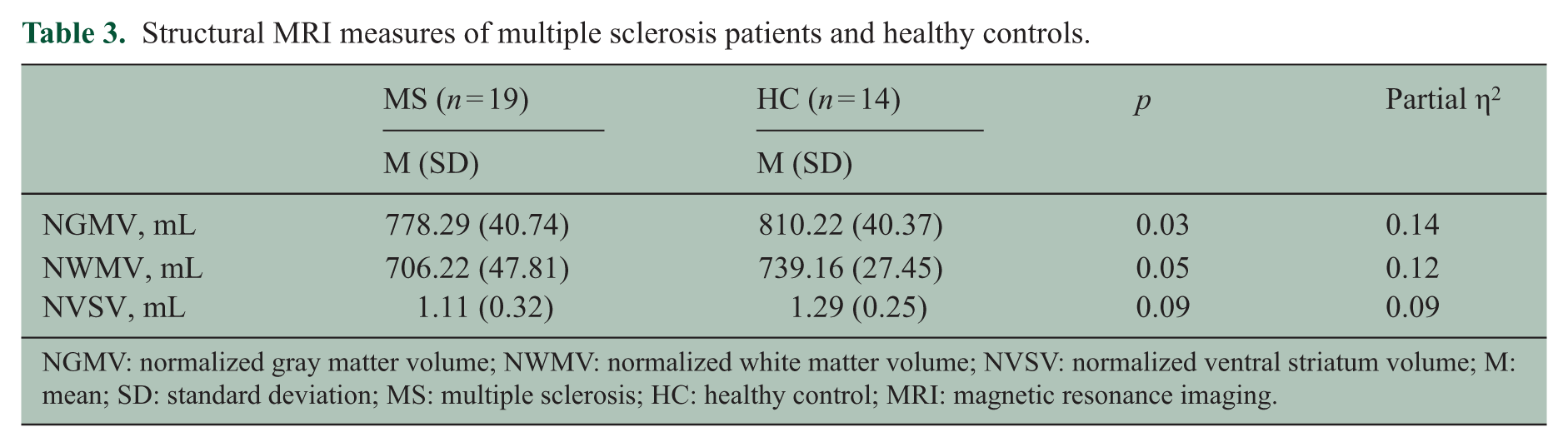
NGMV: normalized gray matter volume; NWMV: normalized white matter volume; NVSV: normalized ventral striatum volume; M: mean; SD: standard deviation; MS: multiple sclerosis; HC: healthy control; MRI: magnetic resonance imaging.
Questionnaires
Data from the post-task questionnaire showed that all participants were more engaged during the outcome condition and that the task stimulated goal attainment. No group differences in participants’ responses were observed (see Supplementary materials for detail).
Data from questionnaires on trait fatigue and motivational tendencies are presented in Table 4. As expected, the MS group showed significantly higher levels of trait fatigue (FSS (t(31) = 2.44, d = 0.87, p = 0.02) and MFIS (t(27) = 3.43, d = 1.37, p = 0.001)) compared to the HC group. The MS group scored significantly lower on the BAS Drive Subscale (t(31) = 2.14, d = 0.81, p = .04) of the BIS/BAS relative to the HC group. No significant group differences were observed on the CMDI.
Questionnaire results.
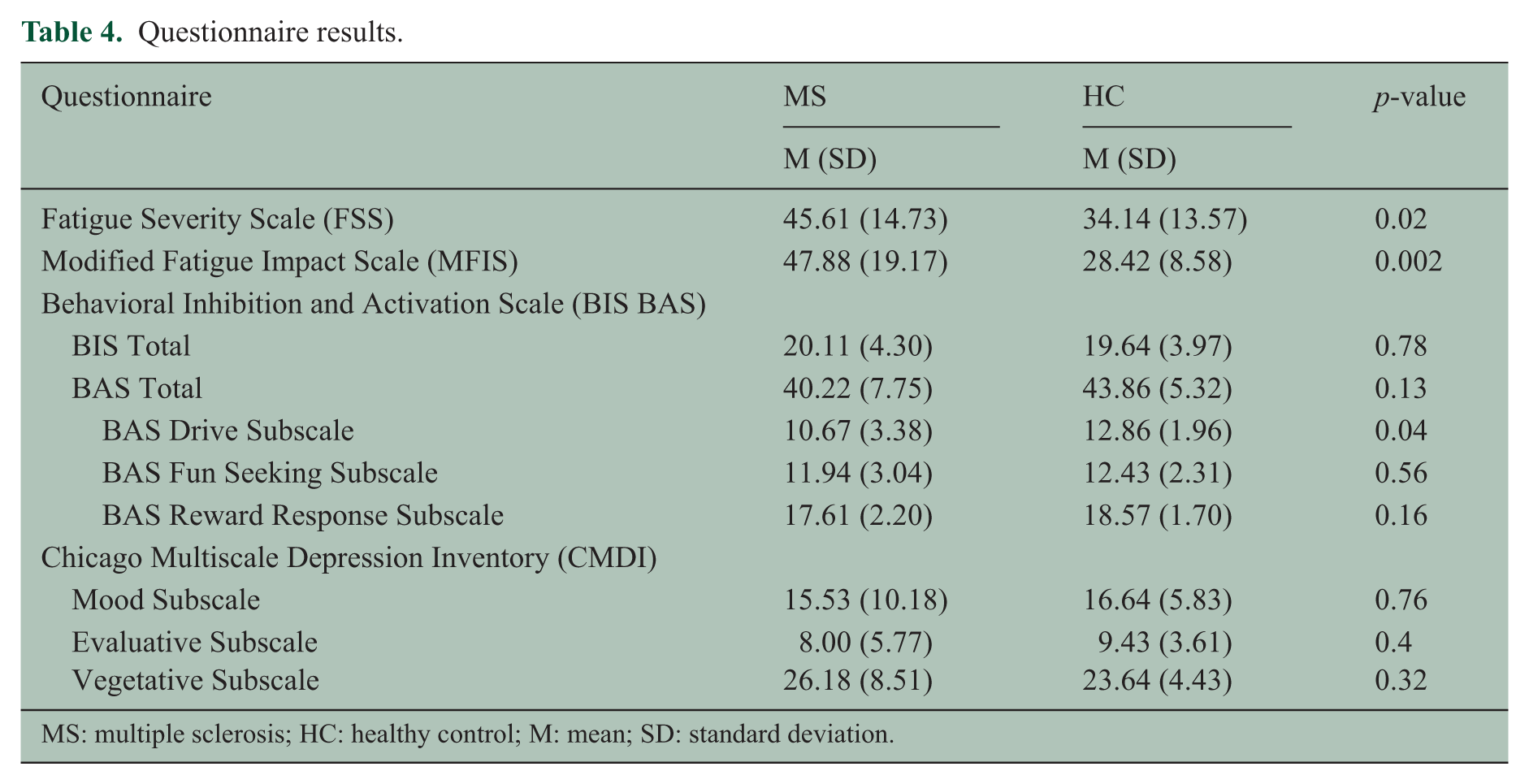
MS: multiple sclerosis; HC: healthy control; M: mean; SD: standard deviation.
As has been previously reported, 31 a reduction in motivational tendencies was correlated with an increase in trait fatigue measures. FSS was negatively correlated with the BAS scale (r = −0.39, p < 0.05) and drive sub-scale (r = −0.41, p < 0.05). MFIS showed a negative correlation with the BAS scale (r = −0.46, p < 0.05), drive (r = −0.46, p < 0.05) and reward responsiveness (r = −0.48, p < 0.05) sub-scales.
Discussion
This study examined a novel approach to fatigue reduction: the manipulation of the fronto-striatal network through outcome presentation. While undergoing an MRI scan, MS and HC participants were presented with a task in which the goal was to win money. Results showed that state fatigue decreased significantly after the outcome condition compared to the no outcome (control) condition and resulted in significant fronto-striatal brain activation in both groups. To the best of our knowledge, this is the first study to show that a behavioral reward can reduce self-reported fatigue and do so by influencing the fronto-striatal network in persons with MS in a manner that is comparable to HCs.
Behavioral findings
A significant decrease in state fatigue was observed in both MS and HC groups after the outcome condition compared to the no outcome condition, indicating that goal attainment reduces state fatigue. Furthermore, we observed a negative association between trait fatigue and motivational tendencies. These results are in line with previous findings 31 and suggest that the MS group, who experienced significantly greater trait fatigue than the HC group, might be more sensitive to negative outcomes and are less likely to experience positive affect when presented with rewarding outcomes. These results further suggest that individuals with MS might need a more salient reward in order to decrease fatigue to the same degree as it occurs in HCs.
fMRI findings
Numerous studies have shown a significant link between fatigue and impairment of fronto-striatal functioning.4,6 The fronto-striatal network plays a major role in goal attainment, such as in processing monetary rewards. In this study, we specifically examined VS and VMPFC functioning, key regions of the fronto-striatal network, during a gambling task with outcome and no outcome conditions, where outcomes were either monetary gains and losses or not rewarding (neutral feedback). Both groups showed increased VS activation during the outcome condition and decreased activation during the no outcome condition. This result is consistent with previous findings of greater activation of the VS to outcome presentation 12 and, in combination with the behavioral finding of reduced fatigue, supports our hypothesis that greater VS activation during outcome presentation would lead to reduced state fatigue.
Compared to the VS, VMPFC revealed a different pattern of activation. We observed decreased activation of the VMPFC during the outcome compared to the no outcome condition, with the difference between conditions being larger in the HC group. While this result is unexpected, we speculate that the observed pattern of activation might be explained by the no outcome condition being perceived as more pleasant than the outcome condition. Previous studies show that the VMPFC is involved in processing pleasantness and that uncertainty is deemed to be unpleasant.32,33 We thus speculate that the outcome condition in this study is more unpleasant because of the uncertainty it brings (probability of receiving a positive outcome is always 50%) compared to the no outcome condition that does not carry uncertainty.
Limitations and future directions
Since our study is the first to demonstrate the effect of goal attainment on fatigue in MS, future investigations are warranted to replicate the current findings and to do so in other populations that report fatigue, such as individuals with traumatic brain injury (TBI). Development of non-pharmacological intervention strategies will also benefit from investigations that assess the time scale of fatigue reduction through goal attainment (e.g. how long is fatigue reduced following a reward). To further examine whether fatigue can be decreased through goal attainment, another important step involves evaluating the impact of reward magnitude on fatigue. As mentioned above, a decrease in fatigue might depend on the saliency of the reward (e.g. US$1 vs US$5). Non-monetary consequences, such as performance feedback during learning, can also be rewarding. 34 For individuals with MS with cognitive deficits, performance feedback might be more valuable than a monetary outcome and thus might be a more salient motivator toward greater fatigue reduction and more robust fronto-striatal activation. Furthermore, given that reward valuation has been shown to be subjective and context-dependent,33,35,36 future studies should examine the modulatory effect of individual differences on the relationship between goal attainment and fatigue.
While in this study we specifically focused on the key regions of the motivational loop, 9 it is important to note that the gambling task that we utilized has been shown to activate other areas of the striatum. 12 Future studies should focus not only on the VS but also on the dorsal striatum that is part of the executive loop. Furthermore, the fronto-striatal network itself is not limited to the VS and the VMPFC. Thus, future investigations should also examine the interaction between the regions of this network during goal attainment as more and more research shows that there are differences between connectivity patterns of individuals with and without fatigue.37,38
Additionally, we did not observe group differences in fronto-striatal activation. Given between-group differences in trait fatigue (low vs high fatigue in HC vs MS, respectively), one might expect to see greater activation during the outcome condition in the HC than in the MS group. However, this study did not demonstrate such an effect, probably due to variability in blood-oxygen-level dependent (BOLD) signal associated with the outcome condition in both groups and a small sample size. Future studies should aim at replicating current findings with larger sample sizes.
Conclusion
The results of this study suggest that fatigue might be effectively reduced via a non-pharmacological method in fatigued individuals with MS, that is, through goal attainment. Goal attainment has been shown to depend on the fronto-striatal network, which is heavily enervated by dopamine. 39 Indeed, clinical trials show that medications such as methylphenidate (dopamine agonists) reduce fatigue in individuals with TBI, 40 Parkinson’s disease, 41 chronic fatigue syndrome, 42 and cancer, 43 while the Dopamine Imbalance Hypothesis suggests that fatigue arises due to the dopamine imbalance within the fronto-striatal network. 6 Thus, both pharmacological and non-pharmacological interventions seem to influence the fronto-striatal network. Increasing the amount of dopamine via medication or through behavioral strategies might lead to fatigue reduction by stimulating the motivation to achieve a goal (i.e. to be goal driven). This study extends findings from healthy individuals 13 and pharmacological investigations40–43 in clinical populations to individuals with MS and lays the foundation for the development of non-pharmacological fatigue treatment strategies focused on simple, non-invasive behavioral manipulations.
Footnotes
Acknowledgements
The authors would like to thank Samantha DePasque, Karolina Lempert, and Olga Boukrina for providing helpful feedback on the manuscript and analyses.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work has been funded, in part, by the National Multiple Sclerosis Society to E.D. (RG-1501-02630).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.