
Abstract
Objective:
Study aims were to determine the frequency of highly active disease in pediatric multiple sclerosis (MS), the response to natalizumab (NTZ) and fingolimod (FTY) treatment, and the impact of current treatment modalities on the clinical course.
Methods:
Retrospective single-center study in the German Center for MS in Childhood and Adolescence.
Results:
Of 144 patients with first MS manifestation between 2011 and 2015, 41.6% fulfilled the criteria for highly active MS. In total, 55 patients treated with NTZ and 23 with FTY demonstrated a significant reduction in relapse rate (NTZ: 95.2%, FTY: 75%), new T2 lesions (NTZ: 97%, FTY: 81%), and contrast-enhancing lesions (NTZ: 97%, FTY: 93%). However, seven patients switched from NTZ to FTY experienced an increase in disease activity. Comparing pediatric MS patients treated in 2005 with those treated in 2015 showed a 46% reduction in relapse rate and a 44% reduction in mean Expanded Disability Status Scale (EDSS).
Conclusion:
The rate of highly active disease among pediatric MS patients is high; more than 40% in our cohort. Response to NTZ and FTY treatment is similar if not better than observed in adults. Current treatment modalities including earlier treatment initiation and the introduction of NTZ and FTY have significantly improved the clinical course of pediatric MS.
Introduction
Several clinical features distinguish the course of disease in pediatric-onset multiple sclerosis (MS) from adult-onset MS. Relapse recovery is faster and more complete in pediatric MS, disability progression is slower, and the time before transition to secondary progression is longer.1,2 In contrast to this, patients with pediatric MS have a higher relapse rate and show more disease activity on magnetic resonance imaging (MRI).3,4 These well-recognized hallmarks of pediatric MS indicate a more active inflammatory process coupled with a better capacity for regeneration when compared to adult MS. Nonetheless, due to the young age at manifestation, patients with pediatric-onset MS reach a comparable level of handicap 10 years earlier than patients with adult-onset MS. 2 This highlights a pressing need for effective therapy strategies in this age group. In spite of this, the only drugs approved for pediatric use in Germany and many European countries are the beta interferons (INFβ) and glatiramer acetate (GA).5,6 Given the high level of central nervous system inflammation in pediatric MS, many patients are not treated sufficiently with these first-line disease-modifying therapies (DMTs). We performed this study to augment current knowledge on the use of natalizumab (NTZ) and fingolimod (FTY) in the treatment of highly active pediatric MS.
Methods
Single-center retrospective clinical study in the German Center for Multiple Sclerosis in Childhood and Adolescence at the University Medical Center Göttingen, Germany (Ethical approval number 21/12/03). Göttingen serves as a tertiary referral center for pediatric MS and has a database of 503 MS patients. All patients satisfy consensus definitions for pediatric MS as defined by the McDonald criteria and the criteria of the International Pediatric MS Group.7,8 Three separate cohorts were generated from the database to assess different aspects of highly active pediatric MS.
Cohort 1: proportion of pediatric MS patients with highly active disease and early predictors
The first cohort was established to determine the frequency of highly active disease in pediatric MS. Current German guidelines define highly active pediatric MS as ⩾1 attack within the previous year and the presence of ⩾9 T2 lesions or ⩾1 Gd-enhancing lesion while under therapy with INFβ, GA, or dimethylfumarate.9,10 Alternatively, criteria for highly active MS are fulfilled at diagnosis by the occurrence of two or more attacks coupled with progression of Expanded Disability Status Scale (EDSS) within the last 12 months and the presence of ⩾1 Gd-enhancing lesion or a significant increase in T2 lesions within the last 6–12 months. These criteria were introduced in 2011, thus only patients with a first clinical event between 2011 and 2015 and with a minimum of 12-month follow-up were included in cohort 1. Age at manifestation, sex, and MRI activity at first presentation were analyzed as parameters possibly predictive of an active disease course. The initial cranial and spinal MRIs of each patient were analyzed for total T2 lesion count and number of contrast-enhancing lesions. An MRI performed within 3 months of first diagnosis was defined as an initial MRI. Both T2 axial images and Flair sagittal images, if available, were evaluated for lesion count. Magnetic resonance (MR) data were acquired on a clinical 1.5 or 3 T MR scanner applying the following parameters: axial T2-weighted turbo spin echo (T2w) sequences (echo time (TE), 80–132 ms; repetition time (TR), 2111–6290 ms; slice thickness, 3–5 mm; gap ⩽1 mm), axial T1-weighted sequences (T1w; TE, 2.1–25 ms; TR, 150–873 ms; slice thickness, 2–6 mm; gap ⩽1 mm) before and 5 minutes after standard single-dose gadolinium (Gd) injection. Lesions were analyzed manually and independent of the analysis of the clinical history by B.H. and H.H. and in case of conflicting results re-evaluated by P.H. and J.G.
Cohort 2: treatment effect of NTZ and FTY in pediatric MS patients
All patients treated with NTZ and FTY were selected from the database of 503 patients. Patients with less than 6 months follow-up were excluded. Age at disease manifestation, age at commencement of therapy, number of relapses before and after therapy with NTZ or FTY, and EDSS were recorded for each cohort. Relapse rate for the 12-month period before and after therapy initiation with NTZ or FTY as well as the annualized relapse rate (ARR) for the total clinical disease duration prior to initiation of NTZ or FTY and the total follow-up duration after treatment were calculated. MRI data were analyzed for total number of T2 and Gd-enhancing lesions at the time of therapy initiation as well as the number of new T2 lesions and Gd-enhancing lesions 12 months prior to therapy and 6, 12, and 18 months after commencement.
Cohort 3: effect of current treatment modalities on relapse rate and EDSS in pediatric MS
Patients treated in 2005 were chosen to serve as a historical control group and were compared with a cohort treated in 2015. All patients receiving a DMT within one of the designated study years and with at least 12 months follow-up on treatment were included in the analysis. Age at manifestation, sex, time interval to initiation of a DMT, type of DMT in use during the respective year, EDSS, and number of relapses within the designated study year (relapse rate) were documented. To control for potential bias arising from significant differences in underling disease activity within the two cohorts, total T2 lesion load and number of Gd lesions on the initial MRI at manifestation were analyzed for each patient and compared between the cohorts.
Statistical analysis
Comparisons between independent groups were done with Fisher’s exact test for gender, t-test for age of onset, Wilcoxon rank-sum test for EDSS, and Poisson regression for count data like relapses and lesions. Similarly, a nonparametric alternative to the paired t-test and generalized estimation equations (GEE) Poisson regressions were used for paired measurements. p-values smaller than 5% were considered statistically significant. Analyses were done with R Stat 3.3.1 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Proportion of pediatric MS patients with highly active disease and early predictors (cohort 1)
Results are shown in Table 1 and Figure 1.
Proportion of pediatric MS patients with highly active disease.
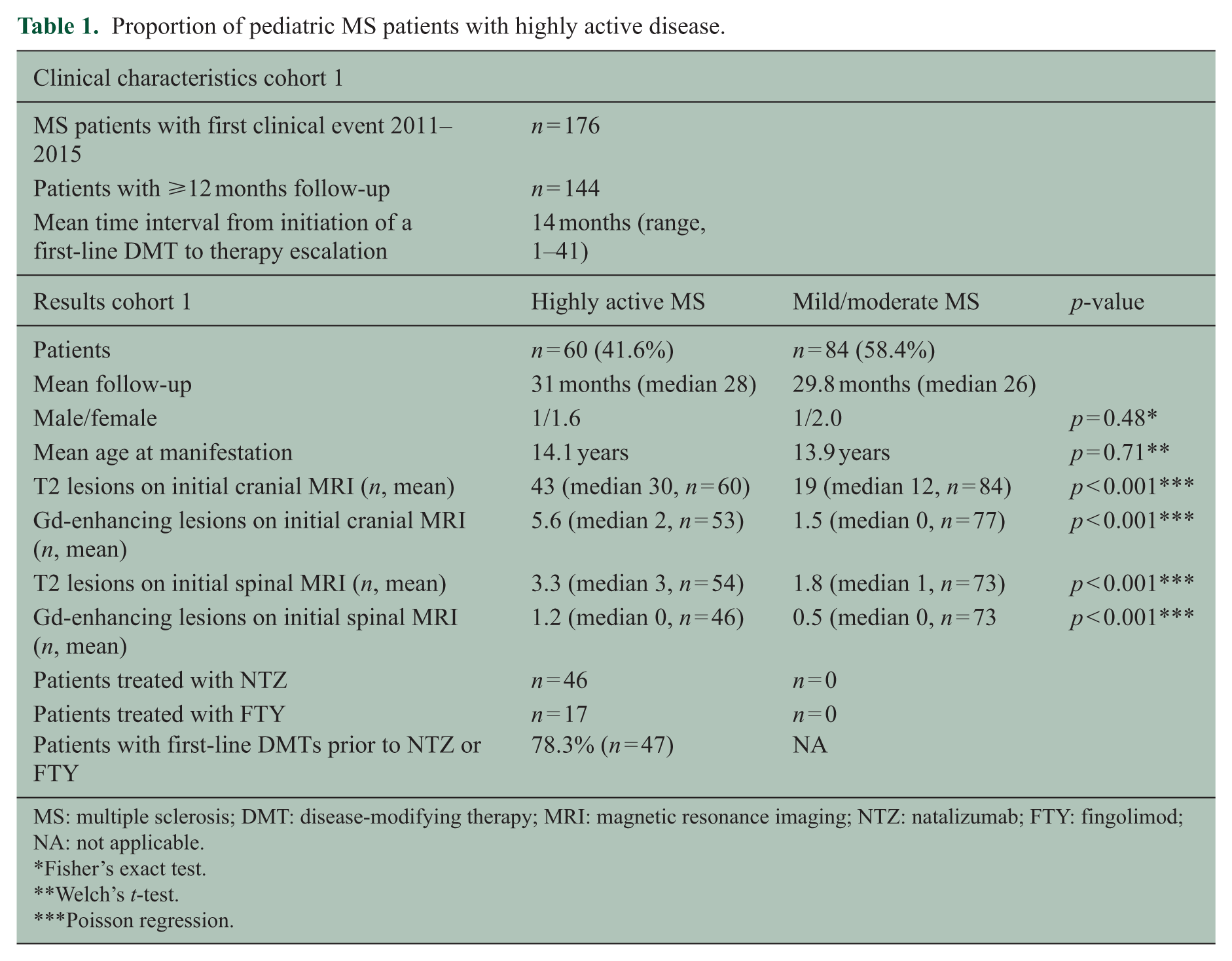
MS: multiple sclerosis; DMT: disease-modifying therapy; MRI: magnetic resonance imaging; NTZ: natalizumab; FTY: fingolimod; NA: not applicable.
Fisher’s exact test.
Welch’s t-test.
Poisson regression.
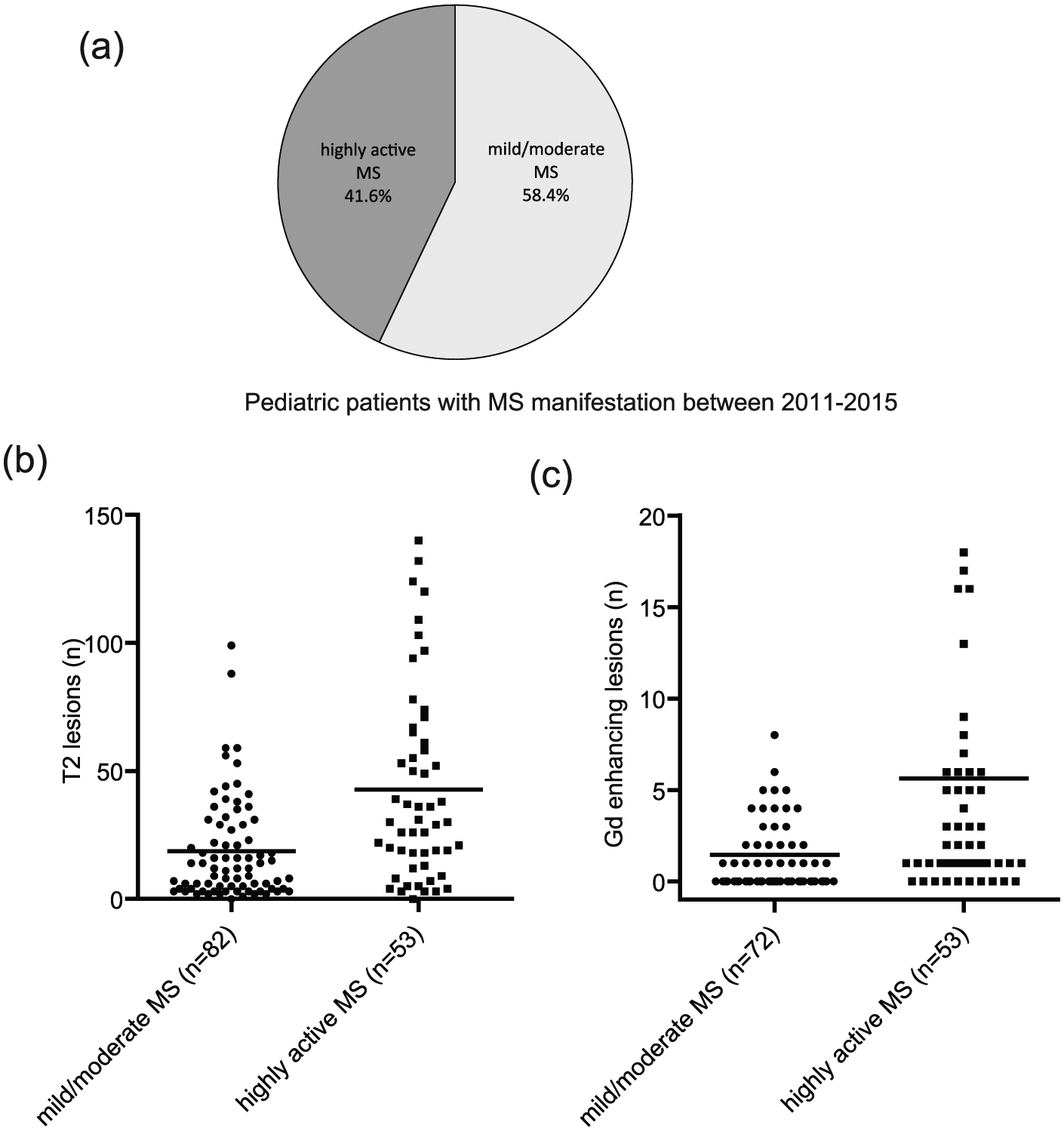
Highly active MS in patients with a first clinical manifestation 2011–2015 and early predictive factors. (a) Of 144 patients who fulfilled inclusion criteria, 41.6% fulfilled criteria for highly active MS. (b) Number of T2 lesions on initial MRI was significantly higher in highly active patients. (c) The same result was observed for number of Gd-enhancing lesions. Each dot represents one patient, horizontal line = mean.
Treatment effect of NTZ and FTY in pediatric MS patients (cohort 2)
Patient characteristics and comparative results for 6 and 12 months pre- and post-initiation of NTZ for 55 patients are shown in Table 2 and Figure 2(a)–(c). ARR dropped from 2.14 (n = 55, mean disease duration before NTZ therapy 24.7 months) to 0.13 (n = 55) after a mean follow-up time on therapy of 21.8 months (94% reduction). No further new T2 lesions or contrast enhancement were observed at 12 (n = 43) and 18 months (n = 31) follow-up. Comparison of mean EDSS at initiation of NTZ with mean EDSS at the end of follow-up also showed a reduction of 25% (1.6, n = 53, vs 1.2, n = 54, p = 0.011 (paired rank test)). Therapy with NTZ was generally very well tolerated with no or only minor side effects. One patient, who was not included in the efficacy study (follow-up <6 months), developed an infusion reaction during the third infusion and therapy was terminated. Anti-JC virus antibodies were analyzed in 62 patients, 18 (29%) were positive at initiation of NTZ. In total, 8 of 36 patients initially negative for anti-JC virus antibodies converted to positive over a total follow-up of 694 months (conversion rate: 13% per year).
Clinical characteristics and results following treatment with NTZ and FTY.
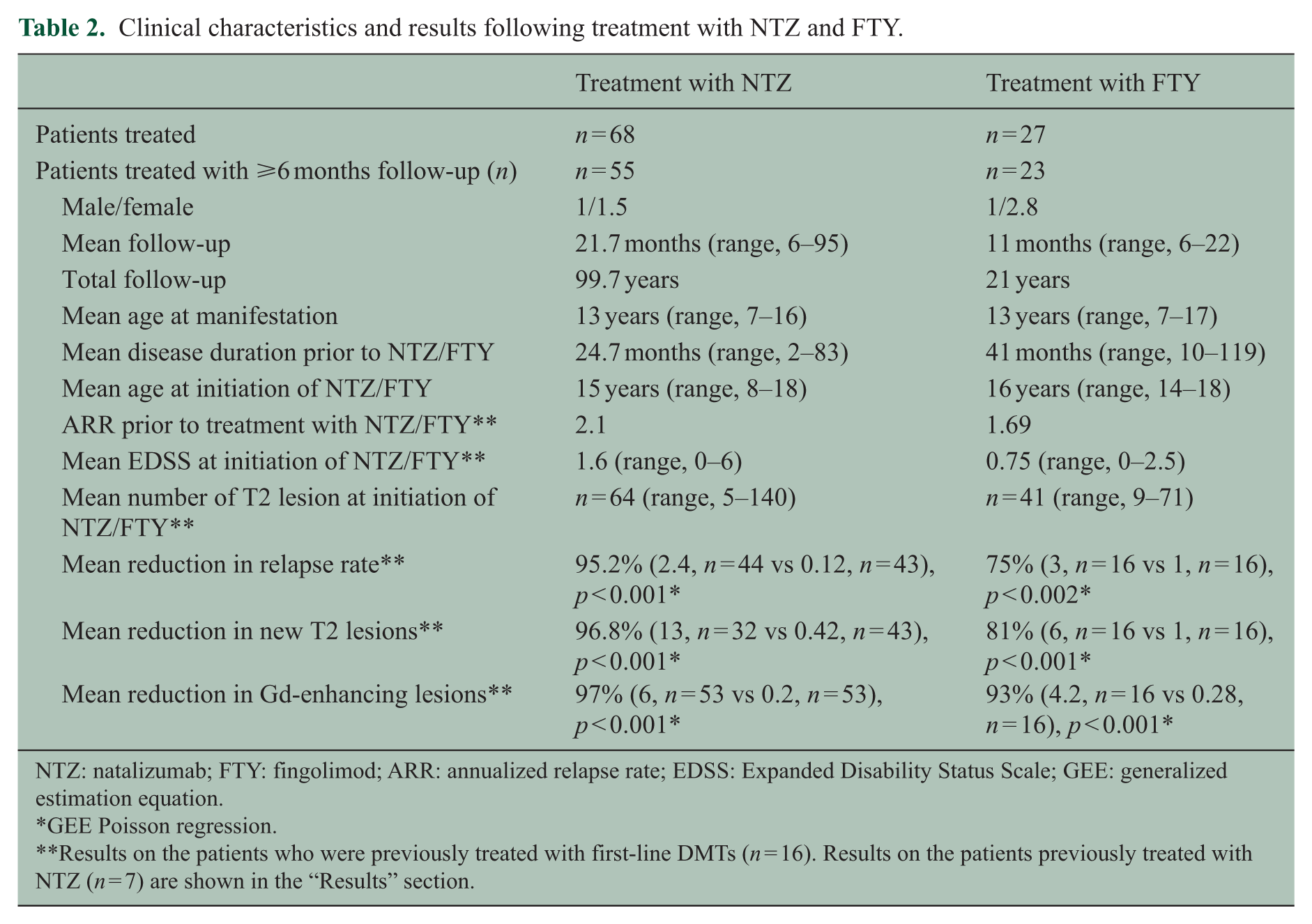
NTZ: natalizumab; FTY: fingolimod; ARR: annualized relapse rate; EDSS: Expanded Disability Status Scale; GEE: generalized estimation equation.
GEE Poisson regression.
Results on the patients who were previously treated with first-line DMTs (n = 16). Results on the patients previously treated with NTZ (n = 7) are shown in the “Results” section.
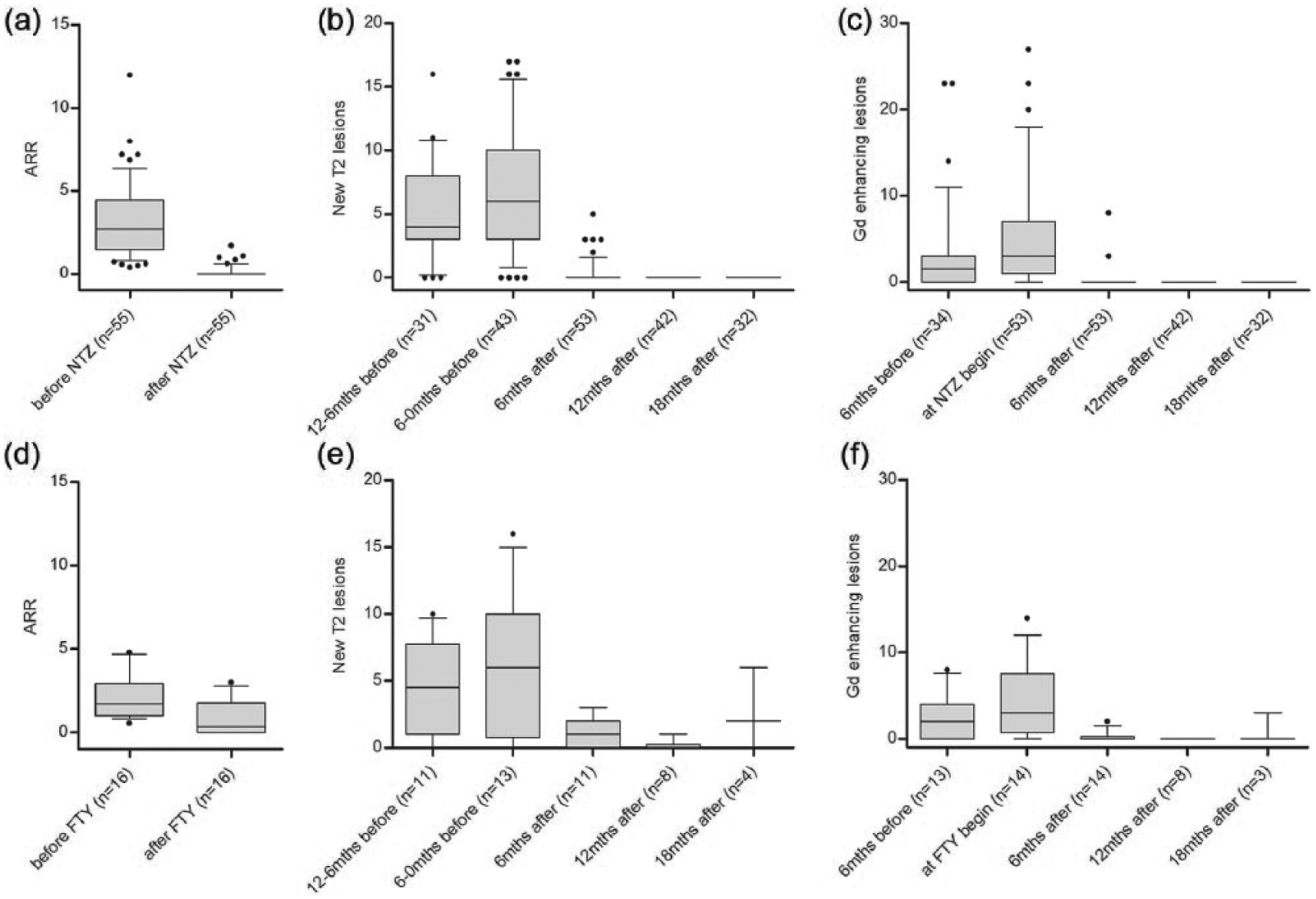
Effect of therapy with NTZ and FTY in pediatric MS patients. Results of patients switched from NTZ to FTY are reported in the “Results” section. ARR was calculated using time from clinical manifestation to start of NTZ/FTY treatment and total follow-up time on therapy (a, d). Number of new T2 lesions (b, e) and Gd-enhancing lesions (c, f) in 6-month intervals before and after the start of NTZ/FTY. Whiskers: 10–90 percentiles.
Patient characteristics of 23 patients treated with FTY and comparative results for 6 and 12 months pre- and post-initiation of FTY in 16 patients only pretreated with a first-line DMT are shown in Table 2 and Figure 2(d)–(f). Reason for change of medication in the patients pretreated with first-line DMTs was progression of disease as described above. The seven remaining FTY patients received prior treatment with NTZ. Switch to FTY followed a NTZ treatment period exceeding 2 years while concurrently positive for JCV antibodies. In these patients, the washout period for NTZ was 2 months. Several features distinguish these seven patients from the group pretreated with a first-line DMT including a younger mean manifestation age (11.8 years vs 14.2 years) and a higher mean T2 lesion count on MRI at FTY initiation (52 (median, 46; range, 24–99) vs 40 (median, 39; range, 9–71)). This group was therefore analyzed separately. All seven patients demonstrated an increase in disease activity following switch to FTY (patients with further relapses n = 4, with new T2 lesions n = 6, with Gd lesions n = 5, mean follow-up 9.5 months (range, 6–19)). Six of the seven patients were switched to alemtuzumab due to ongoing disease activity within the 18 months following the switch from NTZ to FTY. No serious side effects were seen with FTY treatment. Cardiac monitoring at the first dose of FTY was unremarkable in all patients. The following side effects were noted: transient lymphopenia (n = 3), transient cough (n = 1), urinary tract infection (n = 1), burning sensation in the legs (n = 2); transient in one patient, leading to discontinuation of FTY in the second patient.
Effect of current treatment regime on relapse rate and EDSS in pediatric MS (cohort 3)
Comparative data including clinical characteristics, mean relapse rate, and mean EDSS for a cohort of 38 patients from 2005 and 101 patients from 2015 are presented in Table 3 and Figure 3. Further analysis of the 2015 cohort revealed a lower ARR (0.22) for the patients receiving NTZ or FTY for highly active MS than for the patients on first-line therapy (0.62) with mild or moderate disease activity.
Effect of current treatment regime on relapse rate and EDSS in pediatric MS (Cohort 3).
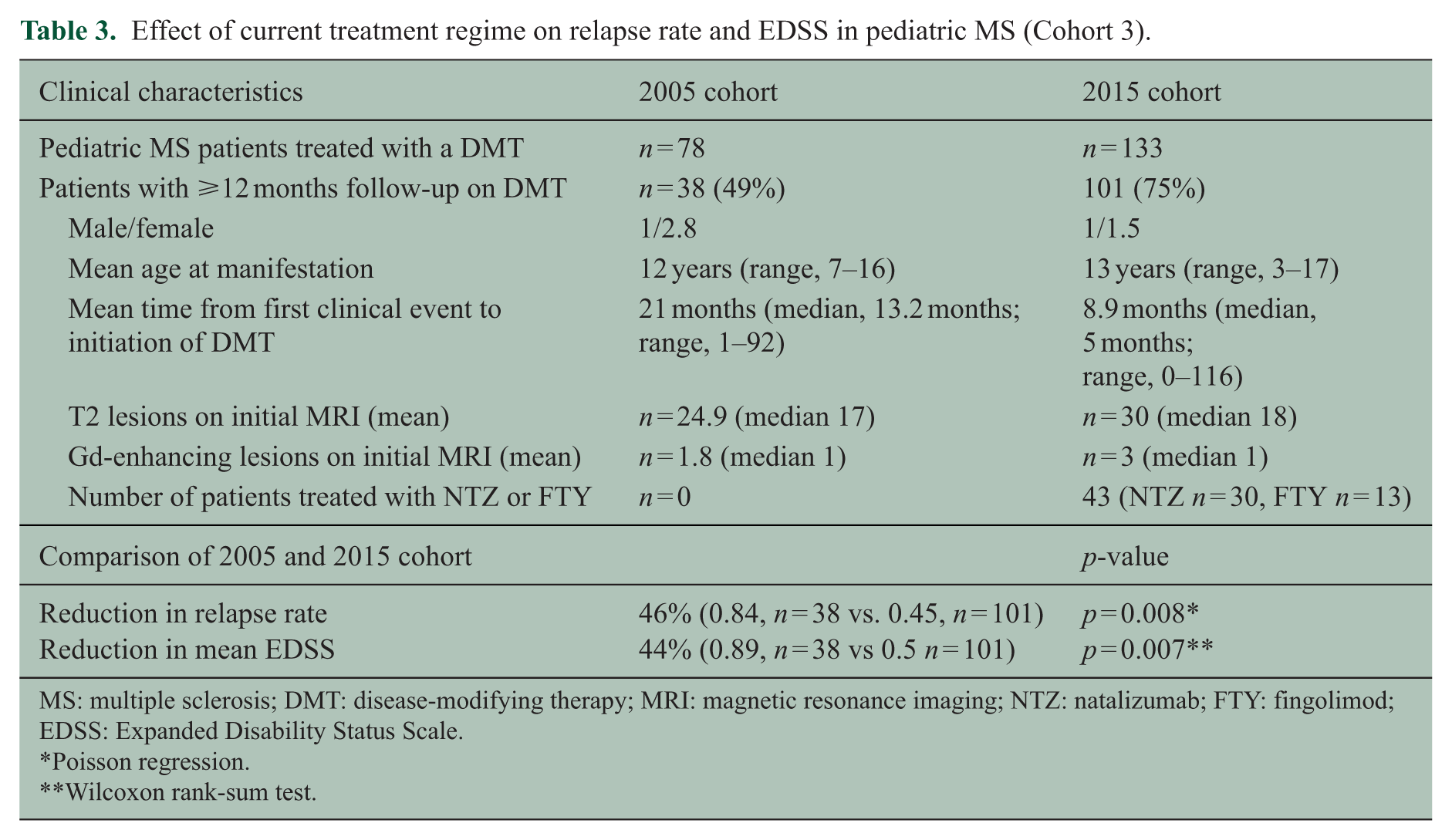
MS: multiple sclerosis; DMT: disease-modifying therapy; MRI: magnetic resonance imaging; NTZ: natalizumab; FTY: fingolimod; EDSS: Expanded Disability Status Scale.
Poisson regression.
Wilcoxon rank-sum test.
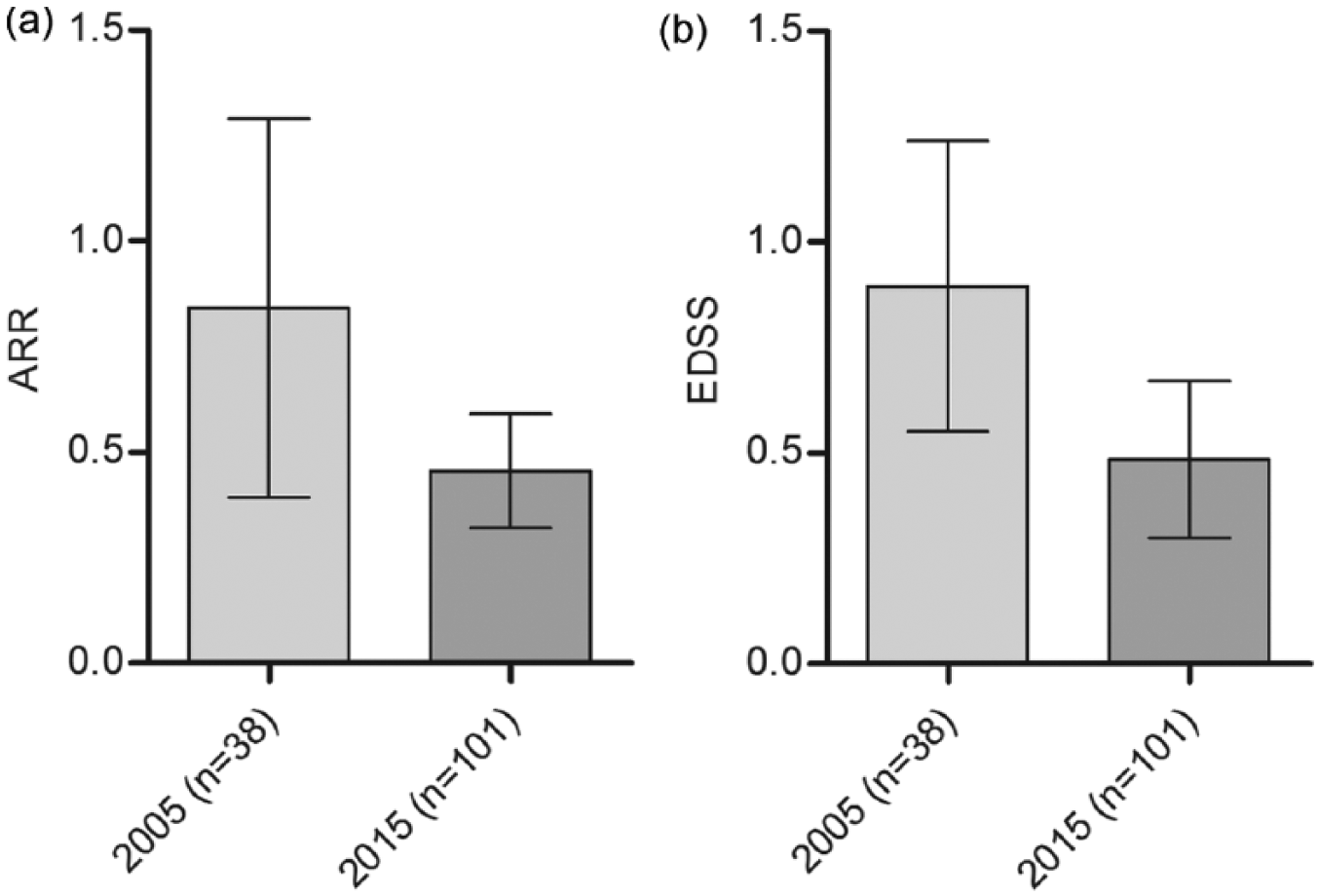
Effect of current treatment modalities on the clinical course of pediatric MS. (a) Relapse rate and (b) EDSS in the cohorts from 2005, all treated with first-line therapy and 2015 with 43% of patients on therapy with either NTZ or FTY. Mean with 95% CI.
Discussion
Several DMTs have been shown to be effective in adult patients with highly active MS. So far, however, very little is known about the treatment of this group of patients in pediatric MS. In order to bridge this gap in knowledge, we performed a retrospective study in the German Center for MS in Childhood and Adolescence. First, we attempted to establish the frequency of highly active MS within our cohort and identify possible factors indicative of a highly active course at the time of first presentation. We restricted the analysis to patients included in the database since 2011 as the criteria for highly active MS, as delineated in the guidelines of the German Neurology Association, were first implemented in this year. From a total of 144 patients who fulfilled inclusion criteria, 41% fulfilled the criteria for highly active MS. Male to female ratio was low (1:1.77) compared to other pediatric MS cohorts. This can be explained by the overrepresentation of younger MS patients in our cohort (mean age at manifestation 14 years), patients aged 16 years or older are commonly seen by adult neurologists in Germany. Comparing the mild to moderate patients with the highly active pediatric MS group showed no correlation between disease activity and sex or age at clinical manifestation. To be expected, considering that lesion load is part of the criteria for highly active MS, patients who fulfilled the criteria for highly active MS had significantly higher numbers of T2 and Gd-enhancing lesions already at the time of diagnosis compared to patients who were classified as having mild or moderate MS. Our results indicate that possibly as much as 40% of pediatric MS patients are not sufficiently treated with first-line DMTs and that a majority of these patients are already recognizable on first MRI. It must, however, be mentioned that Göttingen serves as a national tertiary referral center for pediatric MS and highly active patients might therefore be overrepresented in our cohort.
The second part of the study was aimed to study the effectiveness and tolerability of the two drugs most frequently used for the treatment of highly active MS: NTZ and FTY. In all, 68 patients in our database were treated with NTZ, 55 of these had sufficient follow-up. NTZ lead to a reduction in relapse rate from 2.4 to 0.12 (95%) very similar to that reported by Ghezzi and co-workers in 101 patients (2.3 pre NTZ vs 0.1 post), Kornek and co-workers in 20 patients (3.7 pre NTZ vs 0.4 post), Yeh and co-workers in 24 pediatric MS patients, and Alroughani and co-workers in 32 patients from Kuwait (1.66 pre NTZ vs 0.6 post).11–14 Concordant with previous studies, we also found an even stronger effect on MRI activity. In our cohort, no further disease activity was detected on MRI after 6 months of treatment in any of the 55 patients. Collectively, all studies, including ours, found a very strong effect on clinical and radiological disease activity in patients with highly active pediatric MS indicating that NTZ is an attractive drug for patients in this age group.
In total, 27 patients in our database have received FTY; 23 had sufficient follow-up for inclusion. In all, 16 of these patients were switched due to ongoing disease activity despite treatment with either INFβ or GA and 7 patients pretreated with NTZ were switched to FTY due to positive anti-JCV antibodies. In patients previously treated with INFβ or GA, relapse rate was reduced by 75%, number of new T2 lesions by 81%, and number of Gd-enhancing lesions by 93% following treatment with FTY. So far, only one study by Fragoso et al. 15 has analyzed the use of FTY in 17 pediatric MS patients in Brazil. Mean age at commencement of FTY and sex distribution were the same as in our cohort. In contrast to our study, four of the Brazilian patients were treatment naive and none of them had received prior NTZ treatment. As in our cohort, all patients were considered to have highly active MS. The effect of FTY treatment was even more favorable in the Brazilian cohort compared to ours. Only one of their patients experienced a relapse and follow-up MRI revealed only one new lesion in another patient. One obvious reason for this discrepancy is the shorter follow-up in the Brazilian study. Five of their patients had a follow-up interval shorter than 6 months and would have therefore been excluded from our study. A possible further explanation for our less favorable results may be that our cohort consisted of patients with more active disease. As MRI findings were not quantified in the Brazilian study, a comparison with our cohort is not possible. However, both studies indicate that therapy with FTY in patients previously treated with INFβ or GA results in a significant reduction of disease activity in pediatric MS patients.
Conversely, all patients switched from NTZ to FTY displayed an increase in relapse rate and MRI activity. The explanation for this discrepancy most likely lies in the different level of disease activity between the two groups. Only MS patients with very high disease activity receive treatment with NTZ when positive for anti-JCV antibodies. This higher level of disease activity is reflected in the higher lesion load in the NTZ group compared to the INFβ/GA group at the time of therapy switch. Our results therefore indicate a superior therapeutic effect of NTZ compared to FTY. This was also seen in studies from the United States, France, and Italy directly comparing the effect of FTY and NTZ in adult MS patients, all demonstrated a significantly higher relapse rate and MRI activity in the FTY-treated patients.16–18 Moreover, an increase in relapse rate after switch from NTZ to FTY has also been described in adult MS patients. 19
The most important risk associated with NTZ is progressive multifocal leukoencephalopathy due to infection with the JC virus. We have shown previously that more than 50% of pediatric MS patients are positive for anti-JC virus antibodies. Interestingly, the conversion rate of patients who were treated with NTZ described in this publication was much higher than the one we found in our previous study on a cohort of 256 pediatric MS patients (13% vs 4.37%). 20 An increased conversion rate under NTZ treatment has been previously described in adults with MS. 21 Other side effects of NTZ include hepatotoxicity, allergic reactions, and increased risks of infection. The treatment with NTZ and FTY was generally very well tolerated similar to what has been reported in other studies on pediatric MS patients.11–15 In our cohort, termination of NTZ was necessary in one case due to an infusion reaction. Other side effects were not observed. Most frequent side effects of FTY are bradycardia at treatment initiation, macular edema, diarrhea, back pain, headache, cough, and vomiting. Side effects in our cohort were mild. One patient discontinued FTY due to burning sensation in the legs.
Finally, we attempted to analyze the impact of the current treatment concept on the clinical course of pediatric MS patients by comparing a cohort of patients treated in 2005 with a 2015 cohort. Analysis of relapse rate and EDSS in 38 patients treated in 2005 compared to 101 treated in 2015 showed a reduction in relapse rate by 46% and mean EDSS by 44%. Most likely, the improvement of relapse rate and EDSS can be attributed to the introduction of NTZ and FTY as 43.6% of patients in 2015 were receiving an escalated therapy for highly active MS. Additionally, the shorter delay between diagnosis and start of therapy in 2015 compared to 2005 might also have contributed to the beneficial effect. The analysis also revealed that patients classified with mild or moderate disease activity in the 2015 cohort had a higher relapse rate than the highly active patients treated with NTZ or FTY, indicating that even more patients could benefit from a switch of therapy.
Obviously, the comparison with a historic control group has limitations especially when compared to a placebo controlled study. Between 2005 and 2015, the number of patients treated in Göttingen has grown significantly. To exclude that disease activity of presenting patients has also not changed over time, we analyzed the number of T2 lesions and Gd lesions at the time of diagnosis in both cohorts. The analysis showed that disease activity prior to DMT was relatively similar in both groups as were other patient characteristics. Other factors such as doctor and patient preferences affecting the choice of medication could not be controlled for and can therefore be considered limitations of this study.
The results of this study have influenced the treatment algorithm currently used in Göttingen. Patients are monitored more closely after manifestation to allow early identification of highly active disease. All patients with highly active disease are offered treatment with NTZ if the anti-JCV antibodies are negative and treatment with FTY if they are positive. Patients with extremely active disease are treated with NTZ regardless of the anti-JCV antibody status.
Collectively, our data indicate that almost half of pediatric MS patients have highly active disease. NTZ and FTY were well tolerated and at least equally effective as previously reported in adults. Our results further indicate that highly effective DMTs can have a major impact on the clinical course of pediatric MS. Presumably patients aged 18 years or below profit most from the use of NTZ and FTY as they are early in the course of their disease and have high disease activity.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: P.H. has received honoraria from Biogen idec, Novartis, Bayer Healthcare, and Merck Serono; B.H., D.E. and W.S. report no disclosures. H.H. has honoraria from Bayer Healthcare. K.R. has received honoraria from Merck Serono. He serves as a member of the Novartis advisory board. W.B. has received research support from Teva Pharmaceutical Industries Ltd, Biogen Idec, and Novartis. He is a member of scientific advisory boards of Teva Pharmaceutical Industries Ltd, Biogen Idec, Novartis, and Genzyme/Sanofi. He has received honoraria from Bayer Vital, Biogen Idec, Merck Serono, Teva Pharmaceutical Industries Ltd, Genzyme/Sanofi, and Novartis. J.G. serves as a member of the Novartis and TEVA scientific advisory board. She received honoraria from Biogen Idec, Bayer Healthcare, Novartis, and Merck Serono. She received research support from Novartis and Biogen Idec.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.