
Abstract
Background:
Few data are available on very long-term follow-up of pediatric multiple sclerosis (MS) patients treated with disease modifying treatments (DMTs).
Objectives:
To present a long-term follow-up of a cohort of Pediatric-MS patients starting injectable first-line agents.
Methods:
Data regarding treatments, annualized relapse rate (ARR), Expanded Disability Status Scale (EDSS) score, and serious adverse event were collected. Baseline characteristics were tested in multivariate analysis to identify predictors of disease evolution.
Results:
In total, 97 patients were followed for 12.5 ± 3.3 years. They started therapy at 13.9 ± 2.1 years, 88 with interferons and 9 with copaxone. During the whole follow-up, 82 patients changed therapy, switching to immunosuppressors/second-line treatment in 58% of cases. Compared to pre-treatment phase, the ARR was significantly reduced during the first treatment (from 3.2 ± 2.6 to 0.7 ± 1.5, p < 0.001), and it remained low during the whole follow-up (0.3 ± 0.2, p < 0.001). At last observation, 40% had disability worsening, but EDSS score remained <4 in 89%. One patient died at age of 23 years due to MS. One case of natalizumab-related progressive multifocal encephalopathy (PML) was recorded. Starting therapy before 12 years of age resulted in a better course of disease in multivariate analysis.
Conclusion:
Pediatric-MS patients benefited from interferons/copaxone, but the majority had to switch to more powerful drugs. Starting therapy before 12 years of age could lead to a more favorable outcome.
Introduction
The onset of multiple sclerosis (MS) during childhood or adolescence is currently reported in about 3%–10% of all MS subjects. 1 The large majority of pediatric MS (ped-MS) patients present a relapsing-remitting course, with a high relapse rate.2,3 In general, these patients reach levels of mild or severe disability after a longer time, but at a lower age compared to subjects with adult onset. 4 Most of the medications for MS have not been tested in pediatric patients with randomized controlled trials (RCTs), and data on disease modifying treatments (DMTs) in this population are mainly available from open label observational studies.5–14 So, one of the major issues of the treatment of ped-MS is the assessment of effectiveness and safety of DMTs in large cohort, followed for a long time. Interferon-beta (IFNB) and glatiramer acetate (GA) are the first options for the treatment of ped-MS, as largely used for many years. 15 At present, few data are available on very long-term follow-up of ped-MS subjects treated with DMTs.
In 2009, we published the results of a cohort of 130 ped-MS subjects treated with IFNB or GA, with a mean follow-up of about 5 years. 6 We present now the long-term results of this cohort, updated to 2016.
Methods
The study was designed as a retrospective evaluation of data prospectively acquired in specialized MS centers.
We invited all the centers that participated to a previous study evaluating treatment with IFNB or GA in ped-MS 6 to join this extension study. The original database was updated and modified including new fields related to type of treatments received, occurrence and number of relapses, Expanded Disability Status Scale (EDSS) score and presence of serious adverse events at the end of each treatment and at last follow-up. Data were extracted from clinical records of each MS center and included in the database, after anonymized. Data on magnetic resonance imaging (MRI) were not included as scans were obtained with a large variety of protocols, machines, readings and times of execution. Collection of data ended in May 2016.
According to the Italian standard of care, all centers follow MS patients on a regular basis, generally every 3 months. At each visit, the neurologist decides whether or not to confirm the ongoing medications in relation to both safety and effectiveness.
The study was authorized by the ethical committee of the coordinating center. Given the retrospective observational study design, according to the Italian law only a communication to local authorities is required.
Main study outcome
The main objective was to report data on treatments (e.g. number and type of immunomodulators received), on clinical evolution (i.e. relapse rate and disability measured by EDSS score), and on serious adverse events related to MS treatments. Any other adverse events were not reported because patients received many different medications and because of the risk of underestimation as they were not regularly collected with a standardized form.
Secondary objective was to compare annualized relapse rate (ARR) and EDSS score before and after starting DMTs. We also perform an exploratory analysis to identify predictors of MS clinical evolution. The following baseline characteristics were chosen as possible predictors: gender, age of MS onset, age of therapy initiation, MS duration before therapy initiation, ARR before therapy initiation (including the first attack), EDSS score at DMTs initiation, type of onset (monofocal or polyfocal), and type of first therapy (Avonex/GA or Rebif/Betaferon). The latter variable was added in the model because, in our previous study, ped-MS patients who started with Rebif/Betaferon had a worse outcome, probably because they had a more severe disease at onset. 6
Measures of MS clinical evolution were ARR during the whole treatment period and disability progression compared to baseline (defined by an increase in EDSS score ⩾ 1.5 points if baseline EDSS = 0, ⩾1 point if EDSS = 1–5, and ⩾ 0.5 points if baseline EDSS = 5.5) confirmed after 3 months.
Patients with no relapses and no disability progression after therapy initiation were considered to have no evidence of clinical disease activity (NEDA-2).
Statistical analysis
Descriptive statistics (mean, standard deviation, etc.) were used for continuous variables, while categorial variables were described as percentage of subjects falling in each group. We compared ARR and EDSS score before and after therapy initiation using Friedman and Wilcoxon tests. Baseline predictors were tested in a multivariate linear regression model for ARR, in a multivariate logistic regression model for disability worsening (method of variables selection: forward). Among baseline predictors, age of therapy initiation and MS onset were considered as binomial variables (< and ⩾12 years). The cut-off of 12 years was selected as an approximation of puberty onset 16 and because it is the age that separates children from adolescent according to MS diagnostic criteria. 17 All multivariate analyses were corrected for follow-up duration and MS center.
For the comparison between subgroups of patients, we used Mann–Whitney test (non-normal continuous variables) and chi-square test (categorical variables).
All p-values reported are two-tailed, and a p ⩽ 0.05 was considered statistically significant. Values of p ⩾ 0.05 and p ⩽ 0.1 were reported and considered as a possible trend. In univariate and multivariate analyses B coefficient and odds ratio are reported with confidence interval (CI) of 95%. All analyses were performed using IBM SPSS Statistic Release 21.0 for Mac.
Results
Baseline clinical and demographic characteristics
In total, 15 out of 18 centers accepted to participate to this extension study. Follow-up data could not be obtained for 33 patients: 12 were no more available because they were followed in the three non-participating centers, 9 could not be identified due to previous anonymization, 12 had moved to other cities/MS centers. Thereafter, 97 ped-MS patients could be included in the study (Table 1). The mean follow-up period of the whole cohort was 12.5 ± 3.3 years (range of 7–24 years). Mean age at last follow-up was 26.5 ± 3.9 years (range of 18–37).
Baseline demographic and clinical characteristics of the cohort.

pts: patients; MS: multiple sclerosis; y: years; SD: standard deviation; mo: months; ARR: annualized relapse rate; EDSS: Expanded Disability Status Scale.
Treatments
The large majority of ped-MS patients were initially treated with IFNB (57 Avonex, 31 Rebif/Betaferon), while 9 started with GA therapy (Figure 1). The first treatment was initiated between 1997 and 2007 (median, 2002). During the follow-up, 15 patients remained on their first treatment (Avonex: 9, Rebif: 4, GA: 2), while the majority (82) underwent at least one switch (a median of two switches per patient, range of 1–6).
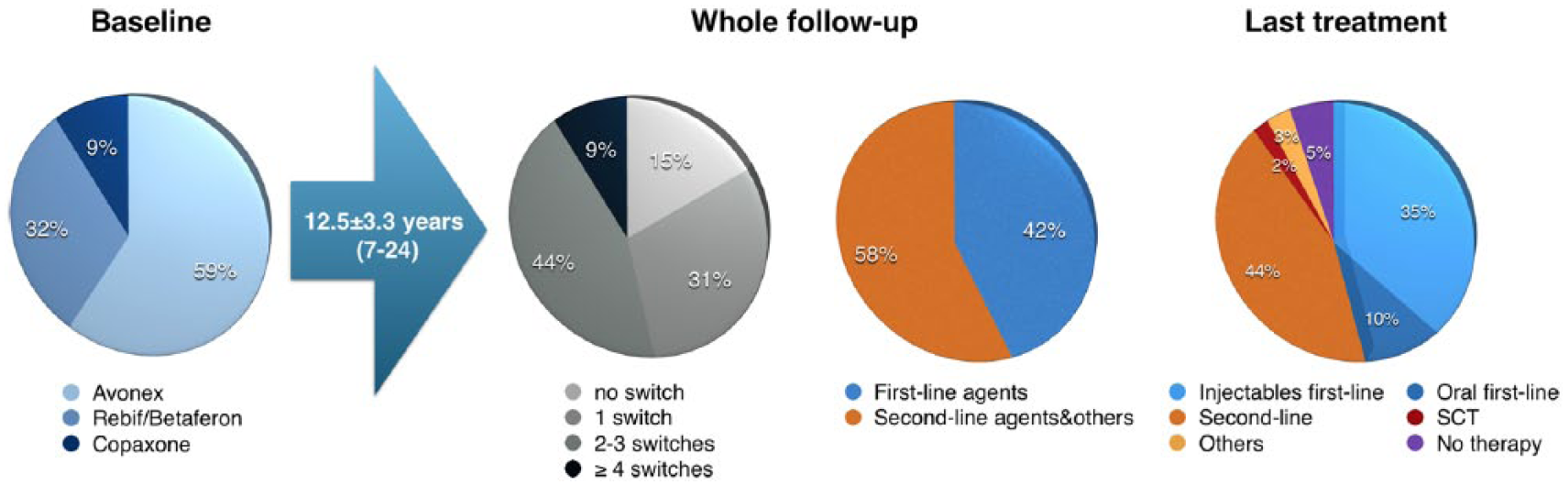
Treatment history of the whole cohort. First-line agents include injectable drugs (glatiramer acetate, interferons beta) and oral drugs (teriflunomide and dimethyl fumarate). Second-line agents: fingolimod, natalizumab, and alemtuzumab. Others: immunosuppressors (azathioprine, mitoxantrone, and cyclophosphamide), stem cell transplantation (SCT), and intravenous immunoglobulin.
The first switch occurred after a mean of 5.5 ± 3.8 years, and the second after 4.1 ± 3.3 years. The first switch was mainly to high-frequency IFN (Rebif or Betaferon), followed by natalizumab (NAT) or fingolimod (FTY). Subsequent switches were mainly to second-line therapy (FTY, NAT) (Supplementary Figure S1). Two patients underwent stem cell transplantation (SCT) due to persistent high disease activity.
Considering the whole follow-up period, 41 patients (40%) received only agents approved as first-line therapy (i.e. IFNB, GA, teriflunomide, and dimethyl fumarate), while the rest were switched to one or more agents approved as second-line (NAT, FTY, alemtuzumab) or to other treatments (azathioprine, cyclophosphamide, mitoxantrone, periodic intravenous immunoglobulins, SCT) at a variable time. At last observation, our patients, now young adults, were taking different drugs, but about one-third were still on first-line injectable agents (Figure 1).
In total, 21 ped-MS patients discontinued the therapy for 6 months or more during the follow-up period. The motivations were pregnancy (3), patient decision (8), progressive MS worsening despite of immunomodulant treatments (1), and unknown causes (9). At last follow-up, five patients were not taking any specific drugs for MS (Figure 1).
Clinical outcomes
Compare to pre-treatment phase the ARR (mean ± standard deviation (SD)) was significantly reduced during the first treatment (from 3.2 ± 2.6 to 0.7 ± 1.5, p < 0.001) and it remained low during the whole follow-up (0.3 ± 0.2, p < 0.001) (Figure 2).
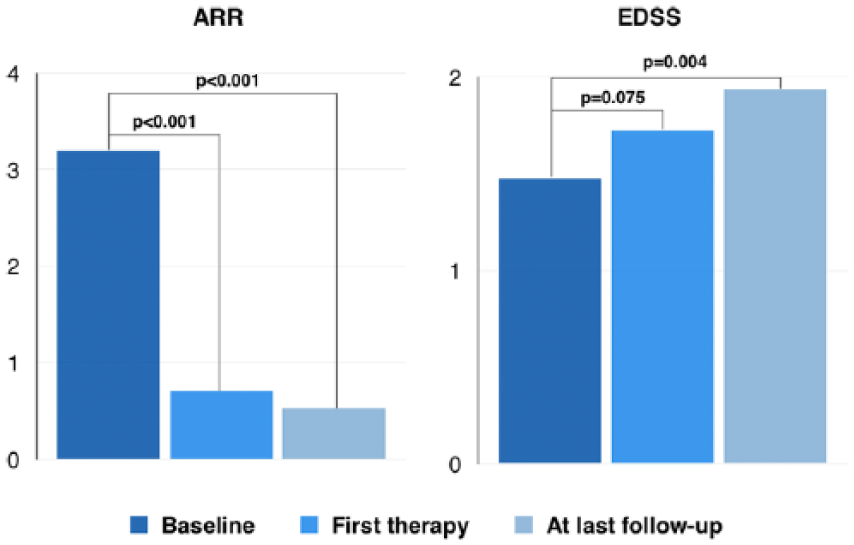
Clinical outcome of the whole cohort: mean ARR and EDSS score at baseline, after the end of first therapy and at last follow-up.
Globally, 39 out of 97 patients (40%) had an EDSS score worsening (by 1.7 ± 0.9 points) measured at the last follow-up with respect to baseline. Accordingly, EDSS score (mean ± SD (median, range)) showed a slight increase at the end of the first therapy (1.4 ± 0.9 (1.0, 0–5) to 1.6 ± 1.2 (1.5, 0–6), p = 0.075), more pronounced at the last observation (1.8 ± 1.5 (1.5, 0–10), p = 0.004) (Figure 2). At the end of the follow-up, the EDSS score was <2 in 59% of patients, 2 to 3.5 in 30%, 4 to 5.5 in 7%, and ⩾6 in 4% of cases (Figure 3), including one patient who died at the age of 23 years because of a malignant form of MS. In total, 10 patients (10%) had NEDA-2 during the whole follow-up period.
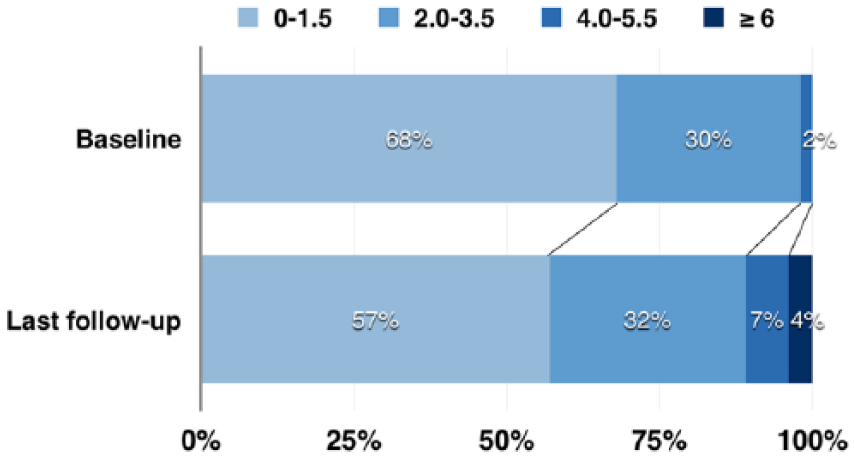
EDSS score subgroups at baseline and at last follow-up.
We observed a trend of disability progression in the 21 ped-MS patients who remained without therapy for more than 6 months with respect to those treated continuously (57% vs 35%, p = 0.07). Taking into account only the eight patients who discontinued therapy for their own decision, 50% of them had disability progression (see Supplementary Table S1).
Safety
A case of NAT-related progressive multifocal encephalopathy (PML) was recorded in a girl at the age of 23 years. At the time of PML diagnosis, NAT had been suspended 2 months before due to a “triple positivity” status (previous immunosuppression with mitoxantrone, > 2 years of treatment, presence of anti-JCV antibodies). The effects of PML were a transient deterioration of cognitive function and persistent drug-resistant focal epilepsy, partially controlled by a triple anti-epileptic therapy. After PML, she continued to be treated with DMTs (first GA, then FTY for recurrent disease activity). At last observation, her EDSS was 1.0.
One male patient died due to a highly active and progressive MS course. Briefly, disease onset was at 15 years of age, and Betaferon was started at 16 (baseline EDSS, 4.5). Due to persistent disease activity and disability progression, he was switched to other treatment (NAT, immunosuppressors) with no benefit. EDSS reached 9 at 21 years, and he died for respiratory complications at 23 years.
No other serious clinical or laboratory adverse events correlated to MS treatment were reported.
Baseline predictors of a worse MS course
Table 2 shows univariate and multivariate analyses for each clinical outcome (ARR, disability progression). In univariate analyses, a worse outcome was predicted by starting therapy after 12 years of age and choosing Rebif/Betaferon as first drugs. In the multivariate analysis, only age of therapy initiation was significantly correlated to both outcomes: in particular, starting therapy after 12 years of age was associated with an increase of 0.15 relapses per year (about 1 additional relapse every 6–7 years) and with a sevenfold higher risk of disability progression at last follow-up.
Univariate and multivariate analyses testing baseline characteristics as predictors of ARR and disability worsening. In table, B coefficient for linear regression model (ARR) and odds ratio for logistic regression model (disability worsening), both with CI 95% and p-value, are shown.
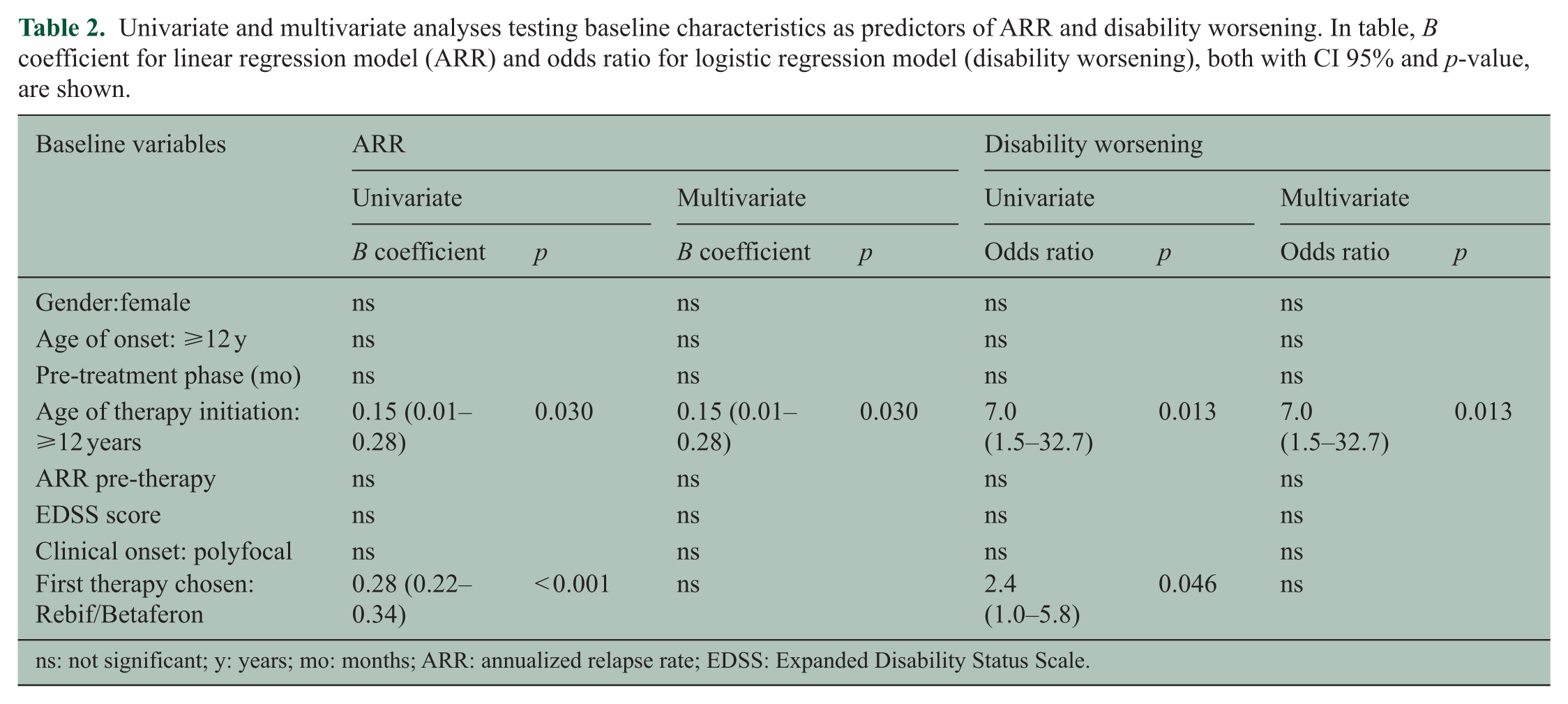
ns: not significant; y: years; mo: months; ARR: annualized relapse rate; EDSS: Expanded Disability Status Scale.
In Table 3, the comparisons of baseline characteristics and clinical outcomes between subgroups of ped-MS patients split by age of disease onset and by age of DMTs initiation are reported. Patients with an earlier MS onset had a female:male ratio of 1:1, a lower pre-treatment ARR, a longer pre-treatment phase, and they started DMTs at a lower age. According to the multivariate analysis, a worse outcome was observed at the end of the first treatment in ped-MS patients starting treatment after 12 years (higher ARR and higher EDSS score), that was confirmed at last follow-up, with a higher risk of disability progression (47% vs 11%, p = 0.005).
Comparison of baseline characteristics and clinical outcomes of ped-MS patients splitted by age of MS onset and by age of therapy initiation.
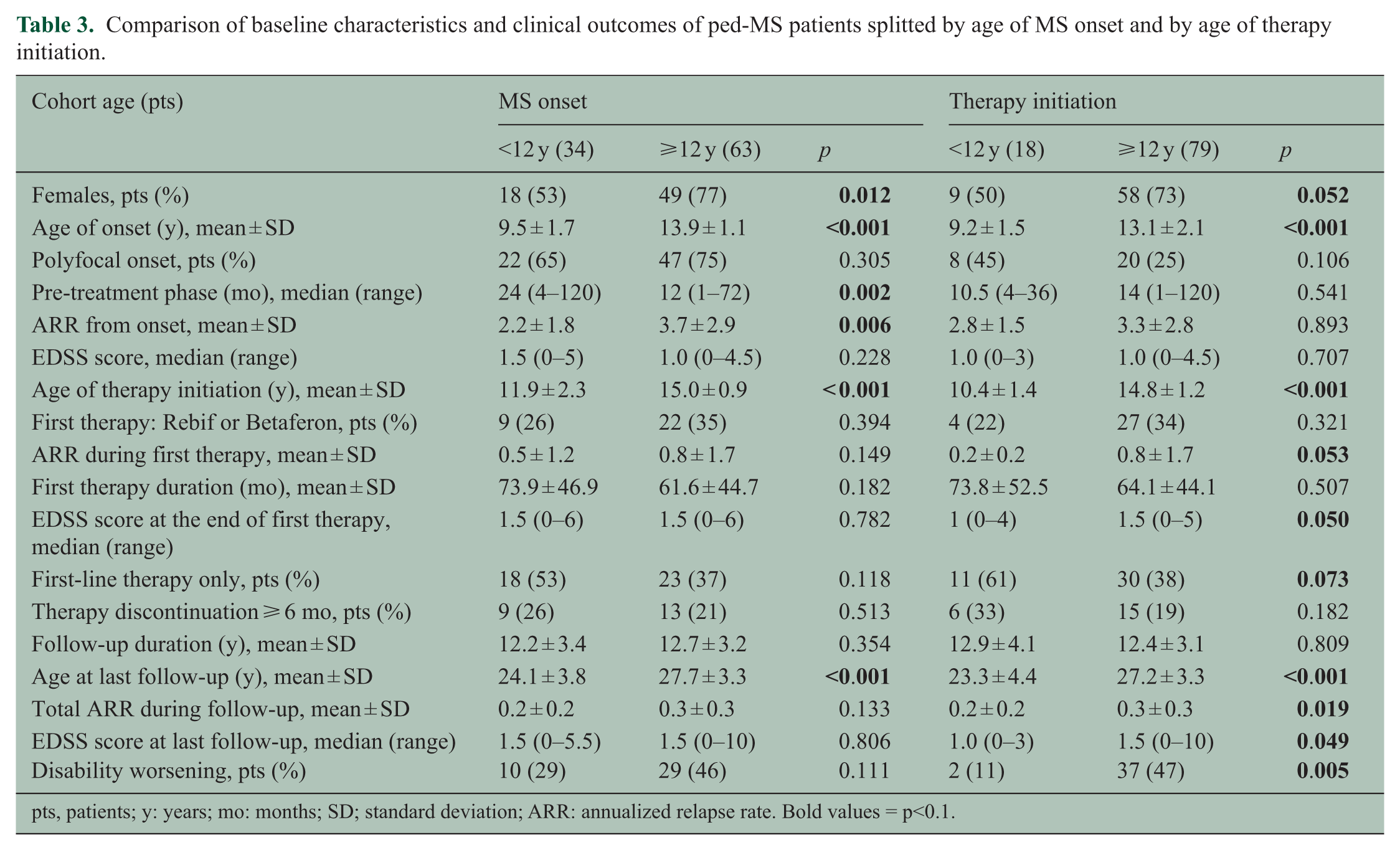
pts, patients; y: years; mo: months; SD; standard deviation; ARR: annualized relapse rate. Bold values = p<0.1.
Discussion
The main aim of our study was to report long-term data of a cohort of ped-MS patients initially treated with injectable agents (IFNB and GA) and followed for a mean of 12 years.
Being aware of retrospective study limitations, we assumed that the quality of data was reliable as provided by centers with a large experience in MS management, most of them participating to RCTs and using a standardized database (iMED). As detailed data on mild adverse events occurring during treatment with IFNB, GA, and NAT had been published in other studies,5,6,11–13,18,19 we paid attention here only to occurrence of severe ones.
Baseline characteristics of our cohort were similar to those of other ped-MS populations previously published.4–14,20,21 A gender ratio of 1:1 in children with MS onset before 12 years of age was confirmed.22–25
The most frequent first-line therapy given was Avonex, probably due to the advantage of a low frequency of administration. The majority of subjects changed their first treatment after about 5.5 years, switching to different drugs. Due to the very long follow-up, reasons of each switching could not be classified, but we could assume that the main motivation was lack of efficacy. In fact, the first switch was toward high-frequency IFNB (Rebif/Betaferon) or to NAT/FTY, clearly indicating the need of more powerful treatments. Considering the whole follow-up, about 60% of patients escalated to second-line agents (NAT, FTY, alemtuzumab) or to other treatments (immunosuppressors, immunoglobulin and stem cell transplantation). The percentage of switchers in our cohort is higher than previously reported in another study, 26 probably because of our longer observation.
The mean ARR significantly decreased under the first treatment with respect to pre-treatment phase (from 3.2 ± 2.6 to 0.7 ± 1.5). However, the majority moved to other DMTs. Subsequently, the number of patients for each therapy and the time of exposure to medications were highly variable, making it difficult to analyze the response to each treatment. Globally, the ARR remained low during the whole follow-up (about one relapse every 3 years). These data are in line with previous reports, where pre-treatment ARR ranged from 1.9 to 3.2 and then it declined to 0.04–0.9 after treatment initiation.7–14,20,21
Disability showed a slightly but significant deterioration with time (median 1.0 at baseline, median 1.5 at last observation), and one patient died due to a highly active form of MS unresponsive to treatments. However, the majority (89%) remained on a low-moderate disability (EDSS score ⩽ 3.5). In previous studies, mean EDSS score after 10 years ranged from 1.2 to 4,22,27–29 and the percentage of patients with EDSS ⩾ 4 after 10 years ranged from 15% to 40%.4,21,29,30 Globally, disability levels of our cohort are among the lowest reported in the literature and are very similar to those of a recently published study 22 where, as in our own, the large majority of patients were treated few years after disease onset. In older studies, where less ped-MS patients received some treatments, disability progression was faster, and reached higher EDSS score.4,28,29 So, it could be argued that the more favorable evolution of MS is due to the effect of treatment, only partially explained by slower evolution of the disease in pediatric patients. This would be in line with a recent study showing that adult MS patients with a recent diagnosis reached EDSS 6 at an older age with respect to those with an older diagnosis, when none or fewer treatment were available. 31 Indeed, other factors could influence the differences of timing and severity of disability progression among the studies (e.g. baseline characteristics, country, and type of recruitment).
During the follow-up, about one patient every five discontinued therapy for at least 6 months. These patients showed a trend to have an EDSS score worsening at last follow-up. To draw any conclusion about this finding is very difficult lacking data about reasons of discontinuation.
During the follow-up, one subject developed NAT-related PML at the age of 23. No other serious adverse events correlated to MS treatment were reported.
In univariate analyses, two variables were correlated to a worse MS outcome: choosing Rebif/Betaferon as first treatment and starting DMTs after 12 years of age. Probably, the first is related to the fact that these drugs were given to ped-MS patients with a worst disease evolution since onset, as already observed in our previous study. 6 In agreement with this hypothesis, the multivariate model found that only starting DMTs after 12 years of age remained significantly associated with both MS outcomes. It could be argued that this finding is mainly due to a better course of the disease in younger pediatric patients. Although previous studies found that ped-MS patients had higher chances to compensate brain damage 32 and that capacity of remyelination decrease with age even in adolescent, 33 other studies did not find any significant differences in the clinical evolution of ped-MS patients stratifying for age of onset.20–22 Only two works found a better outcome in children with MS onset < 10/11 years, but in multivariate analysis age of onset did not correlate to disability scores.4,34 So, our hypothesis is that younger ped-MS patients could respond better to DMTs. This could be due to a more pronounced inflammatory pattern in children with MS, as suggested by MRI data. 35 Moreover, immune system cells involved in cerebral damage could be different in pre-pubertal age. 35 Actually, in younger children a better ability of the central nervous system to recover from damages could be added to a possible higher response to DMTs, leading to a better prognosis. In any case, these findings should be taken cautiously due to important limitations (e.g. small sample size, selection bias, lack of a priori hypothesis, lack of MRI data, and multiple test bias) and should be confirmed in a different and larger cohort to be considered for practical therapeutic implication.
Concluding, ped-MS patients benefited from injectable first-line agents, but after a mean of 5–6 years, the large majority had to switch to more powerful DMTs. The EDSS score and ARR remained globally low over the long follow-up, but in 40%, disability was increased at last observation and one patient died due to MS. These findings underline the need of a careful treatment selection in ped-MS population, considering efficacy as the pivotal aim. Finally, starting DMTs before 12 years of age could lead to a more favorable outcome.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Baroncini received travel grants from Genzyme, Novartis, and Merck for participation at national and international congresses; he received personal compensation from Almirall for scientific publication and honoraria from Sanofy for participating to advisory board. Dr Zaffaroni received personal compensations for speaker or consulting fees or travel expenses from Almirall, Biogen Idec, Genzyme, Merck Serono, Novartis, Roche, and Teva Dr Moiola received honoraria for speaking at scientific meetings or for participating to advisory board from Novartis, Teva, Sanofi-Genzyme, Merck, Biogen. Dr Lorefice received speaker fee from Teva and serves on scientific advisory boards for Biogen. Dr Fenu received honoraria for consultancy from Novartis and for speaking from Merck Serono and Teva. Dr Iaffaldano served on scientific advisory boards for Biogen Idec and Novartis, and received funding for travel and/or speaker honoraria from Genzyme, Biogen Idec, Merck-serono, Teva, and Novartis. Dr Simone has no disclosures. Dr Fanelli has no disclosures. Dr D’Amico received speaking honoraria from Biogen, Bayer Schering, Merck Serono, Novartis, Genzyme, Teva. Professor Patti received research grant from MIUR and FISM and personal fees for speaking and advisory board activities by Almirall, Bayer, Biogen, Celgene, Merck, Novartis, Roche, Sanofi-Genzyme, and Teva. Dr Capobianco received fees for scientific meeting and advisory board from Biogen, Teva, Almirall, Bayer, Merck Serono, Novartis, and Sanofi-Genzyme. Dr Bertolotto received honoraria for serving in the scientific advisory boards of Biogen, Merck, Mylan, Sanofi-Genzyme, and received speaker honoraria from Biogen, Genzyme, Novartis, Teva; his institution received grant support from Almirall, Bayer, Biogen, Genzyme, Merck, Novartis, Teva, from the Italian Multiple Sclerosis Society, Fondazione Associazione Ricerca Biomedica ONLUS and San Luigi ONLUS. Professor Gallo has been consultant and has received funding for travel and speaker honoraria from Merck Serono, Biogen Idec, Sanofi-Aventis, Genzyme, Teva, Roche, Admiral, Novartis Farma and Bayer Schering; has received research support from Bayer, Biogen Idec/Elan, MerckSerono, Genzyme, Novartis, Roche and Teva; and has received research grant from the University of Padova, Veneto Region of Italy, the Italian Association for Multiple Sclerosis, the Italian Ministry of Public Health. Dr Margoni has no disclosures. Dr Miante has no disclosures. Dr Milani has no disclosures. Professor Amato received research grants and honoraria as speaker and member of advisory boards from Merck, Biogen, Byer, Sanofi Genzime, Roche, Teva and Almirall. Dr Righini received research support from Novartis and Genzyme. Dr Bellantonio reports the following disclosures: Novartis, Biogen, and Genzyme. Dr Scandellari has no disclosures. Dr Costantino reports the following disclosures: Novartis, Biogen, Teva, and Genzyme. Professor Scarpini has no disclosures. Dr Bergamaschi received honoraria for scientific lectures and travel payment from Biogen, Novartis, Teva, Genzyme, Bayer Schering, Merck Serono, and Almirall. Dr Mallucci received support to travel to scientific meetings from Bayer Schering, Biogen Idec, Genzyme, Merck Serono, Novartis, Sanofi-Aventis, Teva; received speaker honoraria from Biogen Idec and served on the scientific advisory board for Genzyme and Merck Serono. Professor Comi received compensation for consulting services and/or speaking activities from Novartis, Teva, Sanofi, Genzyme, Merck, Biogen, Roche, Almirall, Celgene, Forward Pharma, and Excemed. Dr Ghezzi received fees for consultant or speaking activity from Merck Serono, Novartis, Genzyme, Biogen Idec, Teva, Almirall.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.