
Abstract
Objective:
Since recent studies suggested a role of the striatum and prefrontal cortex for multiple sclerosis (MS)-related fatigue, we investigated resting-state functional connectivity alterations of striatal subdivisions and the dorsolateral prefrontal cortex (dlPFC).
Methods:
Resting-state functional magnetic resonance imaging was acquired in 77 relapsing–remitting MS patients (38 fatigued (F-MS), 39 non-fatigued (NF-MS)) and 41 matched healthy controls (HC). Fatigue severity was assessed using the fatigue severity scale. Seed-based connectivity analyses were performed using subregions of the striatum and the dlPFC as regions of interest applying non-parametric permutation testing.
Results:
Compared to HC and NF-MS patients, F-MS patients showed reduced caudate nucleus and ventral striatum functional connectivity with the sensorimotor cortex (SMC) and frontal, parietal, and temporal cortex regions. Fatigue severity correlated negatively with functional connectivity of the caudate nucleus and ventral striatum with the SMC and positively with functional connectivity of the dlPFC with the rostral inferior parietal gyrus and SMC.
Conclusion:
MS-related fatigue is associated with reduced functional connectivity between the striatum and sensorimotor as well as attention and reward networks, in which the ventral striatum might be a key integration hub. Together with increased connectivity between the dlPFC and sensory cortical areas, these connectivity alterations shed light on the mechanisms of MS-related fatigue.
Introduction
Lesional, 1 atrophy, 2 positron emission tomography, 3 and task-elicited functional magnetic resonance imaging (fMRI) studies4,5 have consistently implicated the basal ganglia and in particular the striatum in the pathophysiology of multiple sclerosis (MS)-related fatigue. 6 Given these findings, impaired motor and non-motor – i.e., associative and limbic – connectivity of the striatum has been suggested as one of the main substrates of fatigue. 1 In recent years, resting-state (RS) fMRI has become a reliable way to measure functional connectivity between brain regions. RS fMRI demonstrated abnormal functional connectivity of the striatal nuclei with cortical brain regions in MS-related fatigue.7,8 However, anatomy and connectivity of the striatum are complex and characterized by abundant and diverse cortical projections, thus requiring more fine-grained analyses to fully investigate its role in MS fatigue pathophysiology. In addition, the dorsolateral prefrontal cortex (dlPFC)—a central hub for premotor and cognitive functions9,10—has recently been linked to fatigue, while its exact contribution to fatigue is so far only poorly understood.4,11
Here, we investigated correlates of fatigue using seed-based functional connectivity analyses of (1) the caudate nucleus and the putamen, (2) six functional subregions of the striatum, and (3) the dlPFC in a well-characterized cohort of relapsing–remitting MS. Importantly, we employed non-parametric permutation testing to address recent concerns of inflated false-positive rates obtained with parametric statistics. 12
Materials and methods
Subjects
We retrospectively studied 39 fatigued MS patients (F-MS), 38 non-fatigued MS patients (NF-MS)—collected from ongoing prospective studies in our institute—with relapsing–remitting MS fulfilling the 2010 revised McDonald criteria 13 and 41 healthy controls (HC) matched for age and gender. Fatigue was assessed using the fatigue severity scale (FSS). 14 Patients were classified as fatigued if they had at least a score of FSS = 4. 15 The FSS was chosen over other potential fatigue rating scales (e.g. Modified Fatigue Impact Scale) since it assesses impact of fatigue on daily living rather than primary symptoms, which reduces potential confounding of results by primary motor or cognitive symptoms. The inclusion criteria were (1) no change in immunomodulatory therapy in the last 3 months, (2) no acute relapse, (3) no corticosteroid therapy in the last 30 days, and (4) Expanded Disability Status Scale (EDSS) 0–6. Subjects with a Beck Depression Inventory II (BDI-II) score ⩾20 indicating moderate or severe depression were excluded. All patients underwent a full neurological examination and EDSS assessment. To assess motor function, all subjects performed the 9-Hole Peg Test for right and left arm and hand function and the Timed 25-Foot Walk for leg function and ambulation. Cognitive performance was assessed with the Symbol Digit Modalities Test (SDMT), testing processing speed and attention.
All studies were approved by the local ethics committee at Charité – Universitätsmedizin Berlin and conducted in accordance with the Declaration of Helsinki in its currently applicable version and applicable German laws.
MRI acquisition
MRI data were acquired on a 3T Siemens Tim Trio scanner at the Berlin Center of Advanced Neuroimaging at Charité – Universitätsmedizin Berlin. RS fMRI data were acquired using a single-shot echo-planar imaging sequence (TR = 2250 ms, TE = 30 ms, voxel size = 3.4 × 3.4 × 3.4 mm, 260 volumes, acquisition matrix = 64 × 64, field of view (FOV) = 218 mm, acquisition time = 9 minutes 45 seconds; eyes closed). High-resolution structural MRI data were collected using a 3D T1-weighted magnetization-prepared rapid acquisition gradient echo (MPRAGE) sequence (TR = 1900 ms, TE = 2.55 ms, voxel size = 1 × 1 × 1 mm, matrix = 256 × 256, FOV = 256 mm, and 176 contiguous sagittal slices) and a fluid-attenuated inversion recovery (FLAIR) sequence (TR = 6000 ms, TE = 388 ms, voxel size = 1 × 1 × 1 mm, matrix = 256 × 256, FOV = 256 mm, and 176 contiguous sagittal slices).
RS fMRI analysis
Pre-processing
Single-subject preprocessing was performed using DPARSFA (http://www.rfmri.org/DPARSF), based on SPM12 (www.fil.ion.ucl.ac.uk/spm/), including the following steps: (1) discarding the first 10 volumes; (2) slice-time correction; (3) realignment; (4) spatial normalization to the Montreal Neurological Institute (MNI) standard space; (5) smoothing with a Gaussian filter of 4 mm full width at half maximum (FWHM); (6) nuisance regression of cerebrospinal flow, white matter (WM), and global signal; (7) temporal band-pass filtering (0.01–0.1 Hz); and (8) data masking. To take into account head motion as a possible confounder, we performed multiple regression of 24 motion parameters and between-group comparisons of mean framewise displacement (FD) and applied (9) scrubbing—discarding all volumes with an FD > 0.5 mm and the preceding and the two subsequent volumes. Three subjects had an absolute motion greater than 2.5 mm and were excluded from all analyses. Mean FD was not significantly different between groups (F-MS: 0.21, NF-MS: 0.18, HC: 0.19; p = 0.5223).
Seed-based connectivity analysis
To assess functional connectivity changes of the striatum and dlPFC, the following bilateral seeds were used: caudate nucleus and putamen, using masks derived from the probabilistic Harvard-Oxford subcortical structural atlas in FSL. 7 In previous research, three caudate and three putamen subregions of the striatum were identified based on a meta-analysis of peak activations. 16 We chose to investigate these striatal subregions as spherical regions of interest (ROIs) with a radius of 4 mm: inferior ventral striatum (MNI peak coordinates x, y, and z: ±9, 9, −8) and superior (±10, 15, 0) ventral striatum, dorsal caudate (±13, 15, 9), dorsal caudal putamen (±28, 1, 3), dorsal rostral putamen (±25, 8, 6), and ventral rostral putamen (±20, 12, −3). The dlPFC seed was determined based on a meta-analysis of cognitive tasks which found a center of peak activation at ±40, 31, and 34. 17 This was used to define a spherical ROI for the dlPFC with a radius of 10 mm, as described in previous research. 18 All ROIs were visually inspected to avoid overlap and to assure localization within anatomical boundaries (Figure 1). Correlation analyses between the average time series from each seed region and the signal time series in each voxel within the acquired whole-brain image set were then performed. The Z-score functional connectivity maps for each subject were generated by displaying all voxels whose signal time series was significantly correlated with the seed region (p < 0.05).
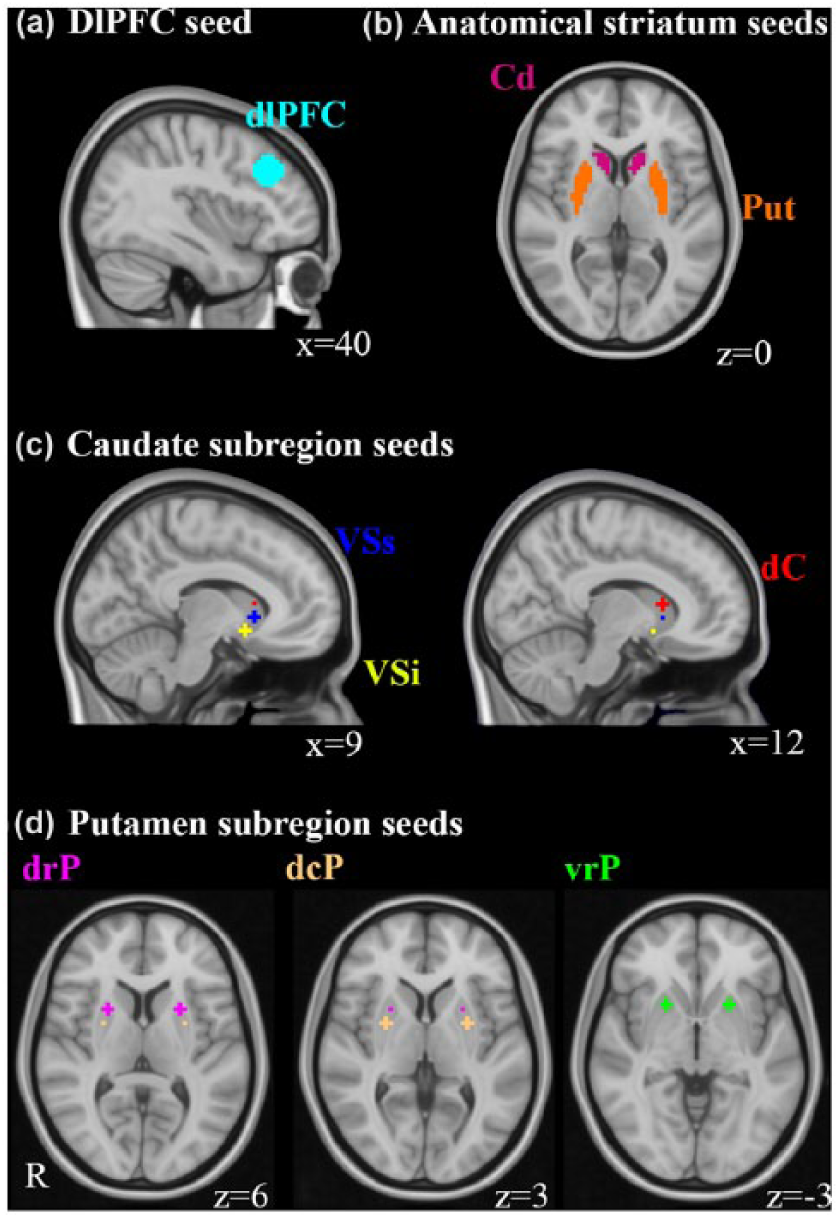
Regions of interest (ROIs) for the subregions of the striatum and the dorsolateral prefrontal cortex (dlPFC). (a) DlPFC ROI with a 10-mm radius containing a total of 171 voxels. (b) Anatomical ROIs of the caudate nucleus and putamen. (c and d) Subregion of the striatum with three caudate (VSi: ventral striatum inferior; VSs: ventral striatum superior; dC: dorsal caudate) and three putamen ROIs (dcP: dorsal caudal putamen; vrP: ventral rostral putamen; drP: dorsal rostal putamten), each containing a total of seven voxels.
Structural MRI analysis
Lesion volume
Lesion volume was calculated from FLAIR and T1-weighted images by applying the Lesion Segmentation Tool (LST, version 1.2.3.; www.statistical-modelling.de/lst.html) with subsequent manual lesion correction.
Volumetric assessment
Volumes of gray matter, WM, and global brain were obtained using FSL SIENAX (https://fsl.fmrib.ox.ac.uk/fsl/fslwiki/SIENA). Caudate nucleus and putamen volumes were obtained using FSL FIRST (https://fsl.fmrib.ox.ac.uk/fsl/fslwiki/FIRST). All measurements were normalized with the V-scaling factor to reduce head-size-related variability between subjects.
Statistical analysis
Functional connectivity group-level analyses were carried out for each seed region using non-parametric testing as implemented in FSL randomise (5000 permutations). Significant clusters were determined using threshold-free cluster enhancement. A family-wise error-corrected cluster significance threshold of p < 0.05 was applied. Two sample t-test analyses were performed to assess functional connectivity differences between MS and HC and between F-MS, NF-MS, and HC.
In addition, correlation analyses were performed between functional connectivity and fatigue scores with sex, age, EDSS, and normalized gray matter volume (NGMV) as covariates of no interest in all MS patients and in all HC. Correlation analyses were also performed in patients between functional connectivity and BDI scores. To correct for lateralization effects, handedness was modeled as covariate of no interest in all analyses. Local maxima of significant clusters were determined and their locations expressed in terms of x, y, and z coordinates into the MNI space. Significant clusters were localized using the probabilistic Harvard-Oxford structural atlas in FSLeyes (https://fsl.fmrib.ox.ac.uk/fsl/fslwiki/FSLeyes).
Analyses of demographic, clinical, and brain volume measurements between F-MS, NF-MS, and HC were carried out using R software, version 3.3.1 (http://www.R-project.org). All values are reported as mean ± standard deviation or median and range as appropriate. Post hoc analysis was carried out using independent two-sample t-tests or Nemenyi’s test as appropriate. Bonferroni correction was applied for all post hoc analyses. Normality was assessed using Lilliefors test. Homogeneity of variance across groups was assessed using Levene’s test. The statistical threshold for significance was set at p < 0.05. Correlation between fatigue severity and demographic, clinical, and structural MRI variables were assessed using Spearman’s Rank correlation coefficient.
Results
Table 1 summarizes demographic, clinical, and radiological characteristics of the final data set: 39 F-MS patients, 38 NF-MS patients, and 41 HC. Compared to HC, MS patients showed significantly smaller bilateral putamen volume (left: p = 0.01, right: p = 0.03). MS subjects presented significantly less WM volume than HC. Other volume measurements did not differ between groups. EDSS and BDI scores correlated positively with FSS scores in MS patients (EDSS, r = 0.32, p = 0.006; BDI, r = 0.7, p < 0.001). Other clinical characteristics and volume measurements did not correlate with fatigue severity in MS patients.
Demographic, clinical, and radiological characteristics in the fatigue-MS (F-MS) group, non-fatigue MS (NF-MS) group, and healthy control (HC) group.
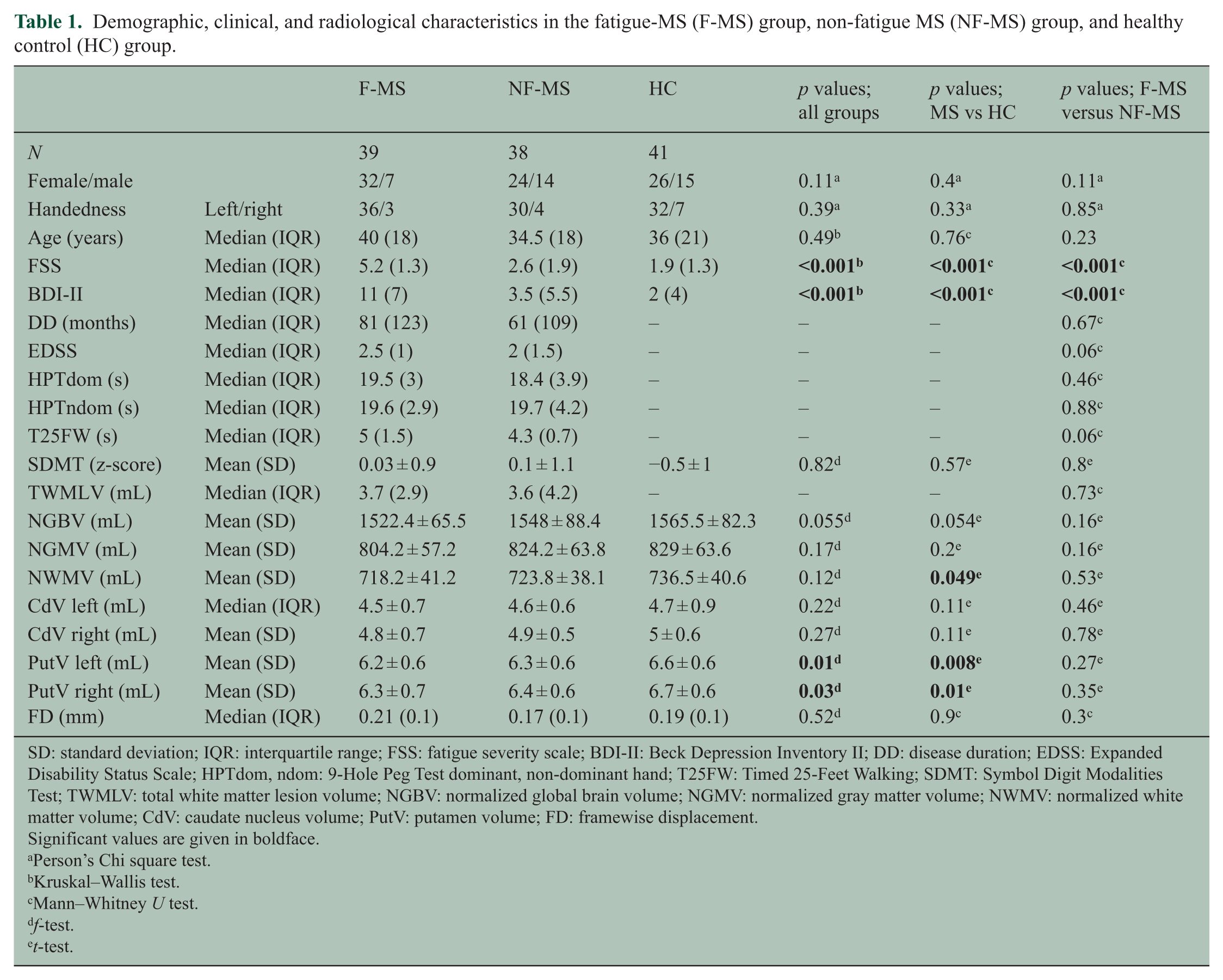
SD: standard deviation; IQR: interquartile range; FSS: fatigue severity scale; BDI-II: Beck Depression Inventory II; DD: disease duration; EDSS: Expanded Disability Status Scale; HPTdom, ndom: 9-Hole Peg Test dominant, non-dominant hand; T25FW: Timed 25-Feet Walking; SDMT: Symbol Digit Modalities Test; TWMLV: total white matter lesion volume; NGBV: normalized global brain volume; NGMV: normalized gray matter volume; NWMV: normalized white matter volume; CdV: caudate nucleus volume; PutV: putamen volume; FD: framewise displacement.
Significant values are given in boldface.
Person’s Chi square test.
Kruskal–Wallis test.
Mann–Whitney U test.
f-test.
t-test.
Caudate nucleus, superior ventral striatum, and dlPFC seed regions showed statistically significant functional connectivity group differences (Table 2). Compared to NF-MS patients and HC, F-MS patients showed reduced bilateral caudate nucleus and left superior ventral striatum functional connectivity with the sensorimotor cortex (SMC; supplementary motor area and precentral and postcentral gyrus; Figure 2). In addition, F-MS patients showed reduced right caudate nucleus functional connectivity with the middle frontal gyrus (MFG), parietal lobule and precuneus, reduced functional connectivity of the left whole caudate nucleus with the parietal lobule, and left superior ventral striatum functional connectivity with the parietal lobule and MFG compared to NF-MS patients (Figure 2). Compared to HC, F-MS presented reduced functional connectivity for the left ventral striatum superior with the inferior temporal gyrus. We observed no significant differences between NF-MS and HC for the caudate nucleus and superior ventral striatum. Contrasting F-MS and all MS subjects with HC, the left dlPFC exhibited reduced functional connectivity with the precuneus, interior parietal lobule, and posterior cingulate cortex (Figure 2). Other striatum subregions showed no significant group differences in functional connectivity between F-MS, NF-MS, and HC.
Group comparison, correlation with fatigue severity and BDI scores. Threshold-free cluster enhancement, 5000 permutations, cluster level, p ≤ 0.05, family-wise error corrected.
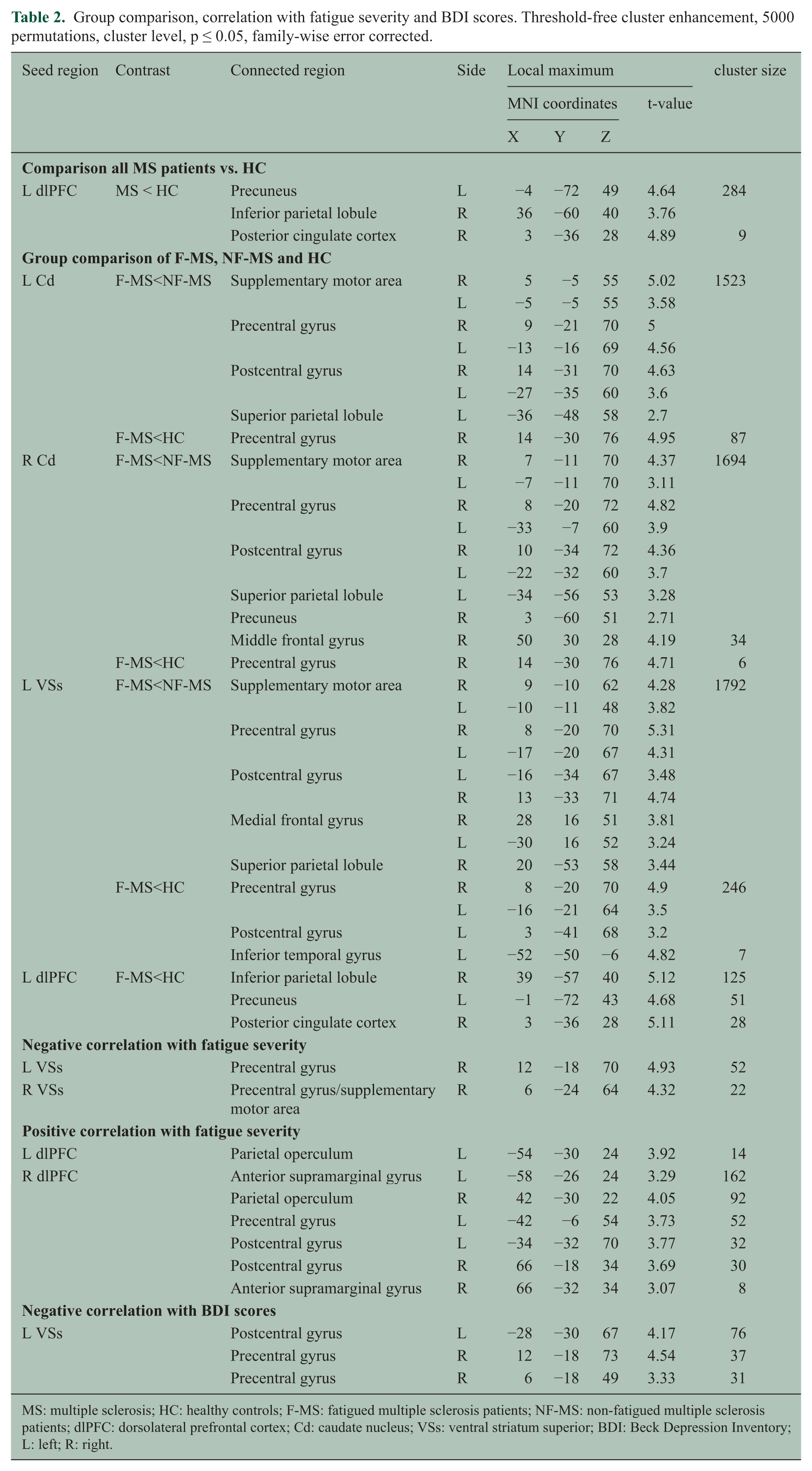
MS: multiple sclerosis; HC: healthy controls; F-MS: fatigued multiple sclerosis patients; NF-MS: non-fatigued multiple sclerosis patients; dlPFC: dorsolateral prefrontal cortex; Cd: caudate nucleus; VSs: ventral striatum superior; BDI: Beck Depression Inventory; L: left; R: right.
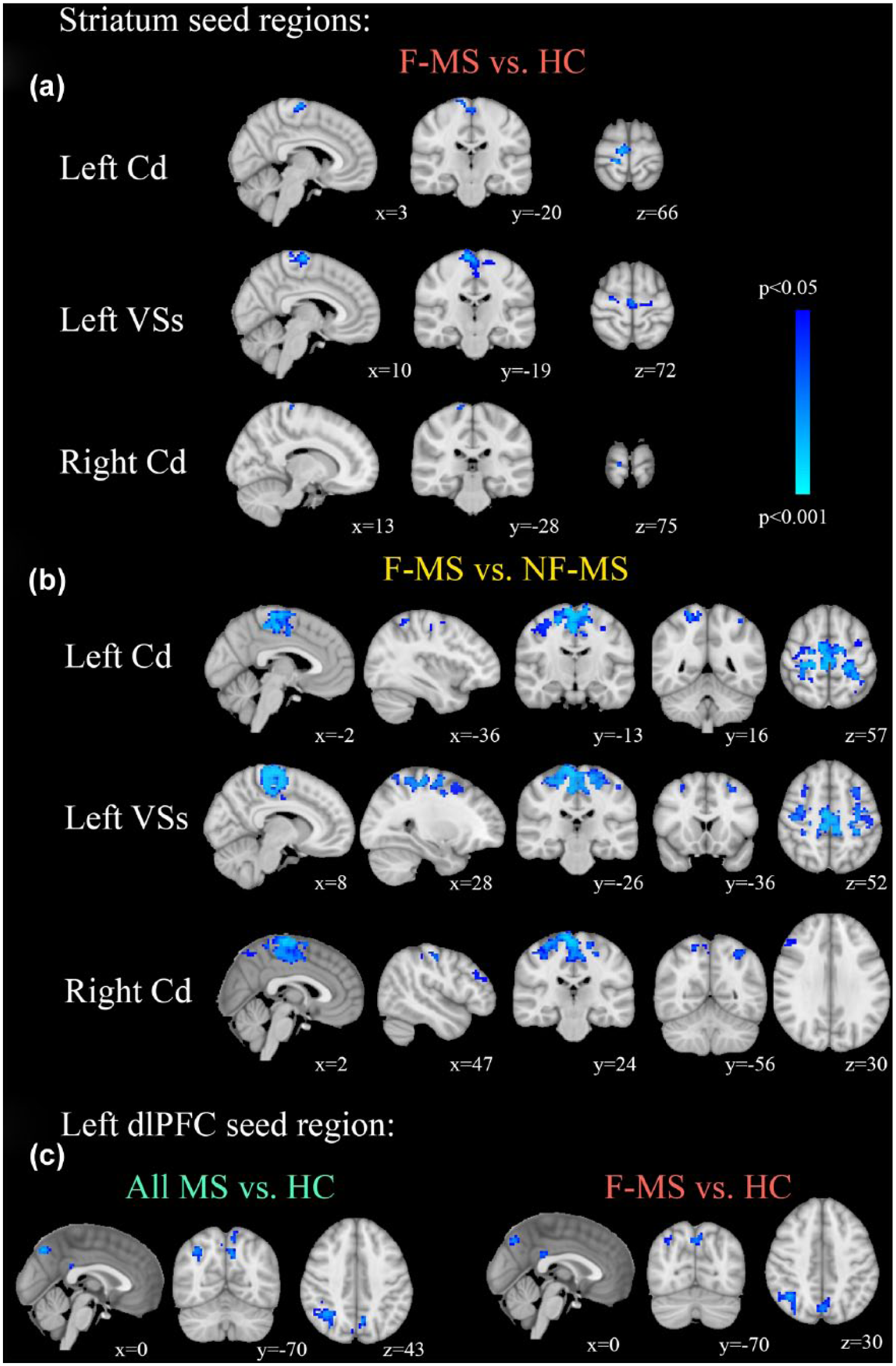
Group comparison of functional connectivity (FC) between all MS patients and healthy controls (HC) as well as fatigue-MS patients (F-MS), non-fatigue MS patients (NF-MS), and HC. Compared to (b) NF-MS and (a) HC, F-MS presented reduced functional connectivity (FC) for the whole caudate nucleus (Cd) and ventral striatum superior (VSs) with the sensorimotor cortex (SMC: supplementary motor area, precentral gyrus, and postcentral gyrus). Compared to (b) NF-MS, F-MS presented reduced FC for the whole caudate Cd and VSs with the superior frontal cortex, medial frontal cortex, superior parietal lobule, inferior parietal lobule, and inferior temporal lobule. (c) All MS patients and F-MS presented reduced FC for the left dlPFC with the precuneus, parietal lobule, and posterior cingulate cortex compared to HC (threshold-free cluster enhancement, 5000 permutations, cluster level p < 0.05, and FWE corrected).
In all MS patients, correlation analyses showed higher FSS scores associated with lower functional connectivity of the left caudate nucleus and bilateral superior ventral striatum with the supplementary motor area and precentral gyrus (Figure 3). Moreover, higher FSS scores were associated with higher functional connectivity of the right dlPFC with the supramarginal gyrus, parietal operculum, and postcentral and precentral gyrus and of the left dlPFC with the supramarginal gyrus (Figure 3). In HC, no significant correlation was found between functional connectivity and fatigue severity. Higher BDI scores were associated with lower functional connectivity of the left superior ventral striatum with the pre- and postcentral cortex. BDI scores did not correlate with functional connectivity for other striatum subregions, the whole caudate and putamen and the dlPFC.
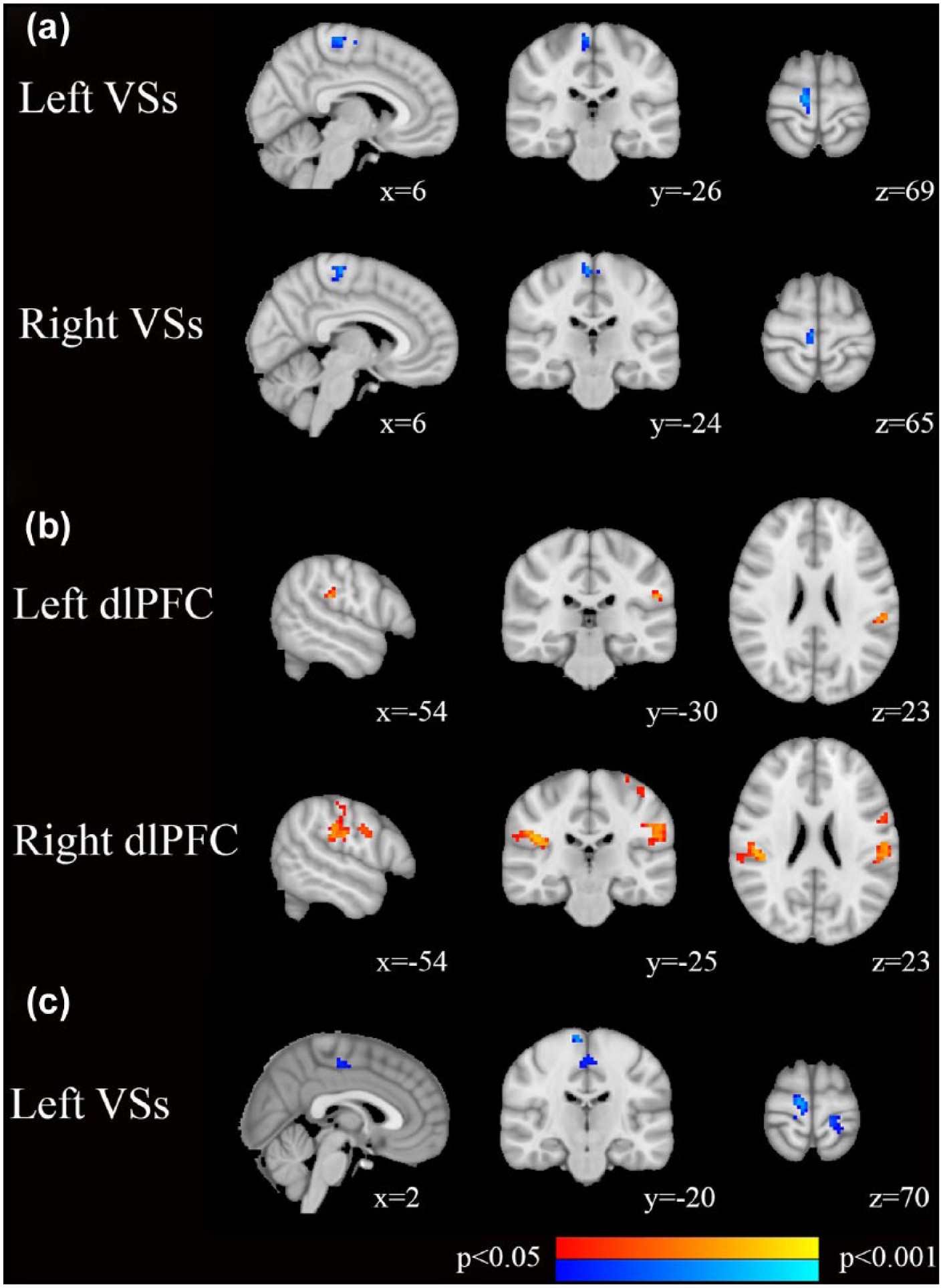
Correlation of functional connectivity (FC) with FSS (a and b) and (c) BDI scores. (a) Fatigue severity correlated with decreased FC of the bilateral ventral striatum superior (VSs) with the supplementary motor area and precentral gyrus in MS patients. (b) Fatigue severity correlated with increased FC for the right dorsolateral prefrontal cortex (dlPFC) with the bilateral supramarginal gyrus, right parietal operculum, bilateral postcentral gyrus, and left precentral gyrus and for the left dlPFC with the left parietal operculum in MS patients. (c) BDI scores correlated with decreased FC of the left VSs with the supplementary motor area and precentral gyrus in MS patients (threshold-free cluster enhancement, 5000 permutations, cluster level p < 0.05, and FWE corrected).
Discussion
This study aimed to elucidate the pathophysiological correlates of MS-related fatigue by investigating striatal subregions and dlPFC functional connectivity in a large, well-characterized study population applying robust statistical methods. We identified reduced functional connectivity of the whole caudate nucleus with sensorimotor and frontal, parietal, and temporal cortex regions in patients with MS-related fatigue compared to MS patients without fatigue and HC. A more fine-grained subregional analysis of the striatum revealed that specifically superior ventral striatum functional connectivity was reduced in F-MS, while other striatum subregions did not show connectivity alterations. In addition, dlPFC exhibited reduced connectivity with the parietal cortex, precuneus, and posterior cingulate cortex and hyperconnectivity with the rostral inferior parietal lobe in F-MS.
Recent research1–5 consistently implicated the striatum in the pathophysiology of MS-related fatigue. However, these studies did not distinguish between striatal subdivisions, neglecting their complex architecture and wide range of functions. 19 Moreover, a recent functional connectivity study demonstrated the existence of multiple connectional hubs of the striatum with different functional interactions. 20 Here, we addressed this issue using a systematic subregion analysis of the striatum, revealing that specifically superior ventral striatum functional connectivity alterations were associated with MS-related fatigue. This suggests that the superior ventral striatum is the striatal connectional hub central to the pathophysiology of MS-related fatigue. The connections of the superior ventral striatum overlap to several brain regions associated with reward regulation, attention, and motor functions.19,21 This convergence of different cortical area connections to one connectional hub could explain the overlap of effort-reward imbalance,1,22 sensorimotor, 8 and attention network23–25 affection in MS-related fatigue.
Effort–reward imbalance, that is, perceiving high-performance costs and low benefits, has been proposed as a central feature of fatigue and was linked to the dysfunction of corticostriatal circuitry.1,7,22 In this study, reduced cortical–ventral striatum functional connectivity might represent a correlate of effort–reward imbalance. In line with this hypothesis, a recent study found that reward presentation improved MS-related fatigue and led to higher blood-oxygen-level-dependent (BOLD) activation in the ventral striatum. 26 Interestingly, injection of endotoxin in HC to experimentally induce an inflammatory challenge leads to sickness behavior including fatigue and reduced BOLD signal in the ventral striatum to reward presentation. 27
Group comparisons and correlation analyses furthermore revealed reduced caudate nucleus–sensorimotor functional connectivity in MS patients with fatigue, indicating a functional decoupling between these regions. In contrast, we observed an association between higher fatigue severity and increased functional connectivity of the caudate nucleus with the precentral gyrus in a previous study. However, in our previous study, more lateral regions of the SMC were involved and the current analysis involved a significantly higher sample size. 7 In summary, altered functional connectivity between the basal ganglia and the SMC complements previous studies that observed atrophy, 2 reduced glucose metabolism, 3 and reduced task-related BOLD activation 4 in both the SMC and the caudate nucleus in patients with MS-related fatigue.
In addition to caudate–sensorimotor network functional connectivity abnormalities, we found decreased functional connectivity of the caudate nucleus and ventral striatum with the intraparietal sulcus, frontal eye field, and dlPFC related to fatigue in MS patients. These are key nodes of the frontoparietal attention network and are implicated in initiating and sustaining attention. 10 We hypothesize that the frontoparietal attention network lacks corticostriatal integration in MS patients with fatigue. Indeed, recent research in HC found that functional connectivity of the frontoparietal attention network was altered after a fatiguing fMRI task. 28 Moreover, we previously observed that MS patients with fatigue had an impaired ability to sustain a saccadic eye-movement task over time—a proposed function of the frontoparietal attention network. 29
MS patients showed a positive correlation between fatigue severity and functional connectivity of the dlPFC with the rostral inferior parietal lobe (parietal operculum and supramarginal gyrus). The dlPFC processes motor and sensory information, maintains sensory stimuli, 9 represents perceived effort, 4 encodes reward amount, and is activated when anticipated rewards signal future outcomes. 19 The rostral inferior parietal lobe integrates higher level sensory information, plays an important role in maintenance and shifting of attention, and is strongly connected with the dlPFC via the ventral portion of the superior longitudinal fasciculus. 10 Thus, we hypothesize that increased frontoparietal functional connectivity is a maladaptive process that contributes to the pathophysiology of MS-related fatigue, possibly mediating effort–reward imbalance. Indeed, overactivation 4 of the dlPFC and dlPFC hyperconnectivity 11 with temporal and occipital brain regions has recently been described in task-elicited fMRI trials in MS-related fatigue. Interestingly, transcranial direct current stimulation of the dlPFC improved fatigue of MS-patients. 30
Furthermore, the whole MS patient group and the sub-group of F-MS exhibited reduced functional connectivity of the dlPFC with key hubs of the posterior default mode network (pDMN), that is, the inferior parietal lobule, precuneus, and posterior cingulate cortex, compared to HC. The pDMN is preferentially activated during internally focused tasks and pDMN alterations have previously been associated with MS-related fatigue. 7 Reduced dlPFC-pDMN functional connectivity was also found in depression and was interpreted as an impaired link between external (dlPFC) and internal attention functions (pDMN). 31 Moreover, we observed reduced caudate–pDMN (i.e. precuneus) functional connectivity in F-MS compared to NF-MS in our study. Similar functional connectivity alterations have previously been reported both in MS-related fatigue 7 and non-MS subjects with depression. 32 Together these findings suggest that reduced connectivity of the pDMN with the dlPFC and the caudate might represent an overlap of depression and fatigue symptoms.
All patients with BDI-II scores ⩾20 indicating moderate to severe depressive symptoms were excluded from our analysis to avoid bias. Nevertheless, BDI scores were negatively correlated with functional connectivity between the ventral striatum superior and the SMC. As in previous studies, FSS and BDI scores in our study were highly correlated. Comparing BDI and FSS items, a high resemblance in many questions of both questionnaires is apparent. This regards for example exhaustion, tiredness, and lack of drive, which could explain the high correlation between both questionnaires. 33 As a consequence, most patients with fatigue will also yield increased BDI scores. The similarity between these scores therefore likely contributes to the resemblance between FSS and BDI correlation results in our analysis and—given the exclusion of patients with BDI score ⩾20—rather reflects fatigue than depression. However, given the intricate relationship between both symptoms, an association of both depression and fatigue with the observed functional connectivity changes cannot be fully ruled out.
Normalized striatum volumes obtained in our study using automated segmentation with FSL FIRST are within the range of volumes observed in previous studies using the same method.34,35 It should be noted, however, that these estimates are larger than volumes derived using manual segmentation. 36 Indeed, automated approaches generally tend to yield greater absolute volumes. However, volumes obtained using automated and manual segmentation pipelines are highly correlated. Moreover, there is a good reliability and comparability for studies applying the same segmentation technique, 37 an observation that is corroborated by similar volumetric results obtained in different study populations.34,35
A limitation of our study is the cross-sectional design. Longitudinal studies are necessary to further clarify the relationship between functional connectivity changes and fatigue and its temporal dynamics. Strengths of our study include the large sample size and the use of strict non-parametric permutation testing with threshold-free cluster enhancement. The latter addresses recent concerns of inflated rates of false-positive results in functional imaging studies that used parametric testing and cluster inference. 12
To conclude, MS-related fatigue was associated with impaired functional connectivity of the striatum with sensorimotor, attention, and reward networks. As subregion analyses suggested, the superior ventral striatum may be a key integrational hub impaired in MS-related fatigue. In addition, increased connectivity between dlPFC and sensory cortical regions may also contribute to the pathophysiology of MS-related fatigue. To further understand the role of the striatum and its subcortical context, studies should investigate dopaminergic input regions of the striatum, for example, substantia nigra and ventral tegmentum, and combine thalamic and striatal functional connectivity subregion analyses. Since our study design involved a prior selection of ROIs, future studies could employ connectivity matrices derived from whole-brain parcellations to study global connectivity changes.
Footnotes
Acknowledgements
J.B.-S. and C.F. have contributed equally.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.