
Abstract
We identified five female patients retrospectively with relapsing short-segment partial myelitis whose clinical and paraclinical features were suggestive of cord involvement of multiple sclerosis (MS)-type albeit not rigidly fulfilling the 2017 McDonald criteria. Notably, these patients had not developed any typical MS-like brain lesions despite repeated neuroimaging assessments over years. Comprehensive work-up for differential diagnoses of MS and other causes of transverse myelitis particularly neuromyelitis optica spectrum disorders had been consistently negative on longitudinal follow-up. Thus, we postulate a possible entity of pure spinal MS which may represent a novel forme fruste within the MS disease spectrum.
Keywords
Introduction
The position paper on the 2017 McDonald criteria timely highlights the need for careful deliberation and further research into certain types of atypical demyelinating conditions with atypical presentations. 1 We hereby highlight a cohort of Asian patients with relapsing pure short-segment partial myelitis (SSPM), that is, pure spinal multiple sclerosis (MS), who may represent a novel forme fruste within the MS disease spectrum.
Objective
To identify patients with pure spinal MS and describe the phenotype while justifying the establishment of such postulated diagnosis.
Method
A single neurologist (S.V.) retrospectively reviewed medical records of 493 consecutive patients in the Demyelinating Diseases Database at Kuala Lumpur General Hospital, Malaysia. Figure 1 shows the algorithm of inclusion and exclusion of patients. We postulated that pure spinal MS patients were patients with (1) relapsing/recurrent SSPM, (2) cerebrospinal fluid (CSF) oligoclonal bands (OCBs) positivity upon testing, (3) magnetic resonance imaging (MRI) of brain not fulfilling the 2017 McDonald criteria, (4) good response to interferon and other MS disease-modifying therapies (DMTs), and (5) who had all other alternative diagnoses ruled out. All patients with myelitis due to non-MS idiopathic inflammatory demyelinating diseases (IIDDs) and non-IIDDs (refer Figure 1) were excluded.
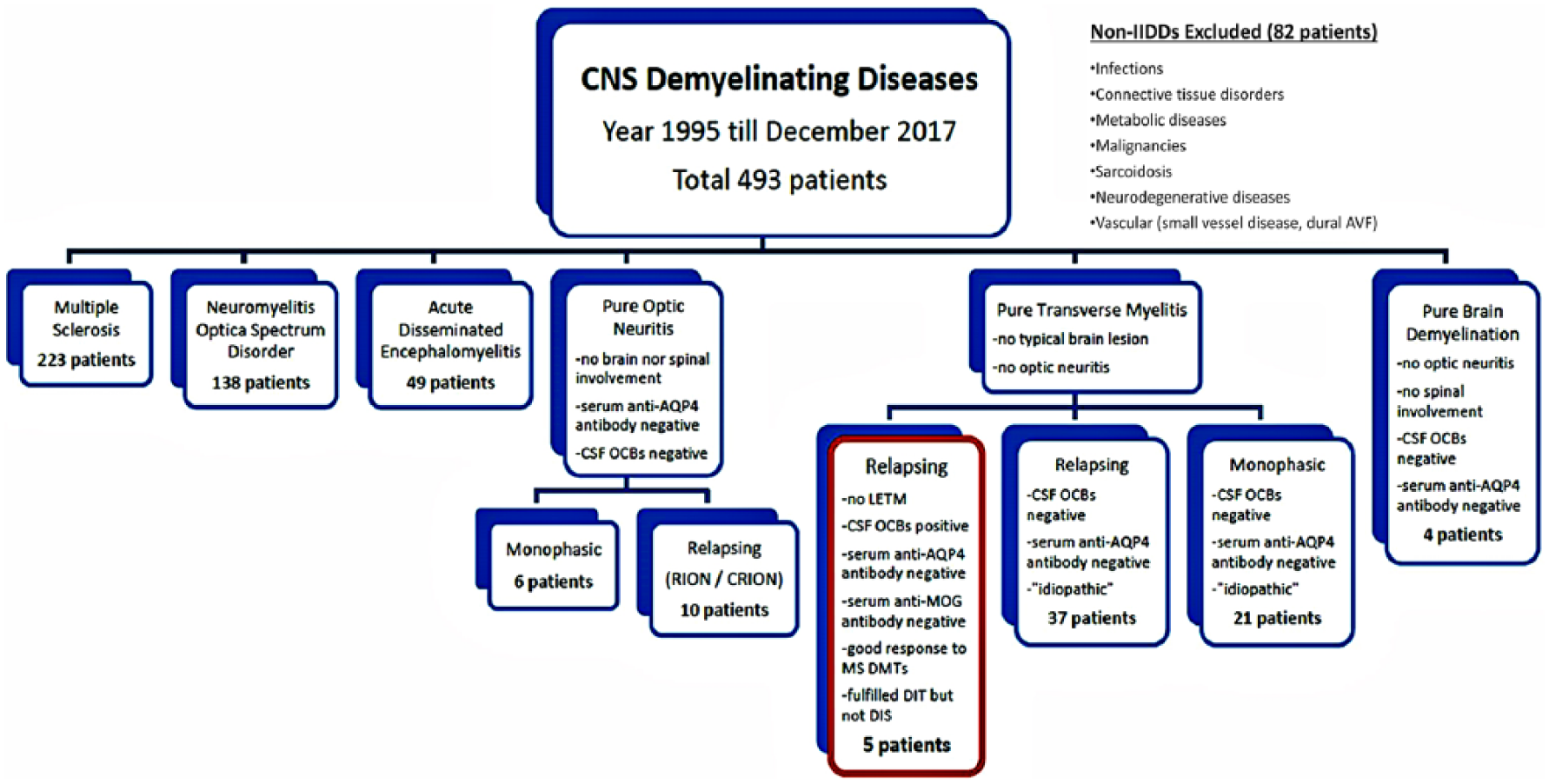
Inclusion and exclusion processes which ended with the selection of five patients with pure spinal multiple sclerosis.
Good response to MS DMTs was defined as (1) recovery of functional status, that is, Expanded Disability Status Scale (EDSS) to baseline/near baseline or stable disease with no worsening of baseline EDSS > 1.0 point over the course of DMTs, (2) significant reduction in annualized relapse rate (ARR), and (3) no new MRI T2 or Gadolinium-enhancing lesions while on DMTs.
Results
Five female patients with pure spinal MS were identified. Their mean age at the disease onset: 30 years, mean disease duration: 13 years, and mean follow-up duration: 11 years.
Clinical features
Four patients demonstrated relapsing–remitting course, while one patient demonstrated progressive relapsing course (see Supplemental Figures 1–5; see Table 1).
Background and clinical features of pure spinal MS patients.
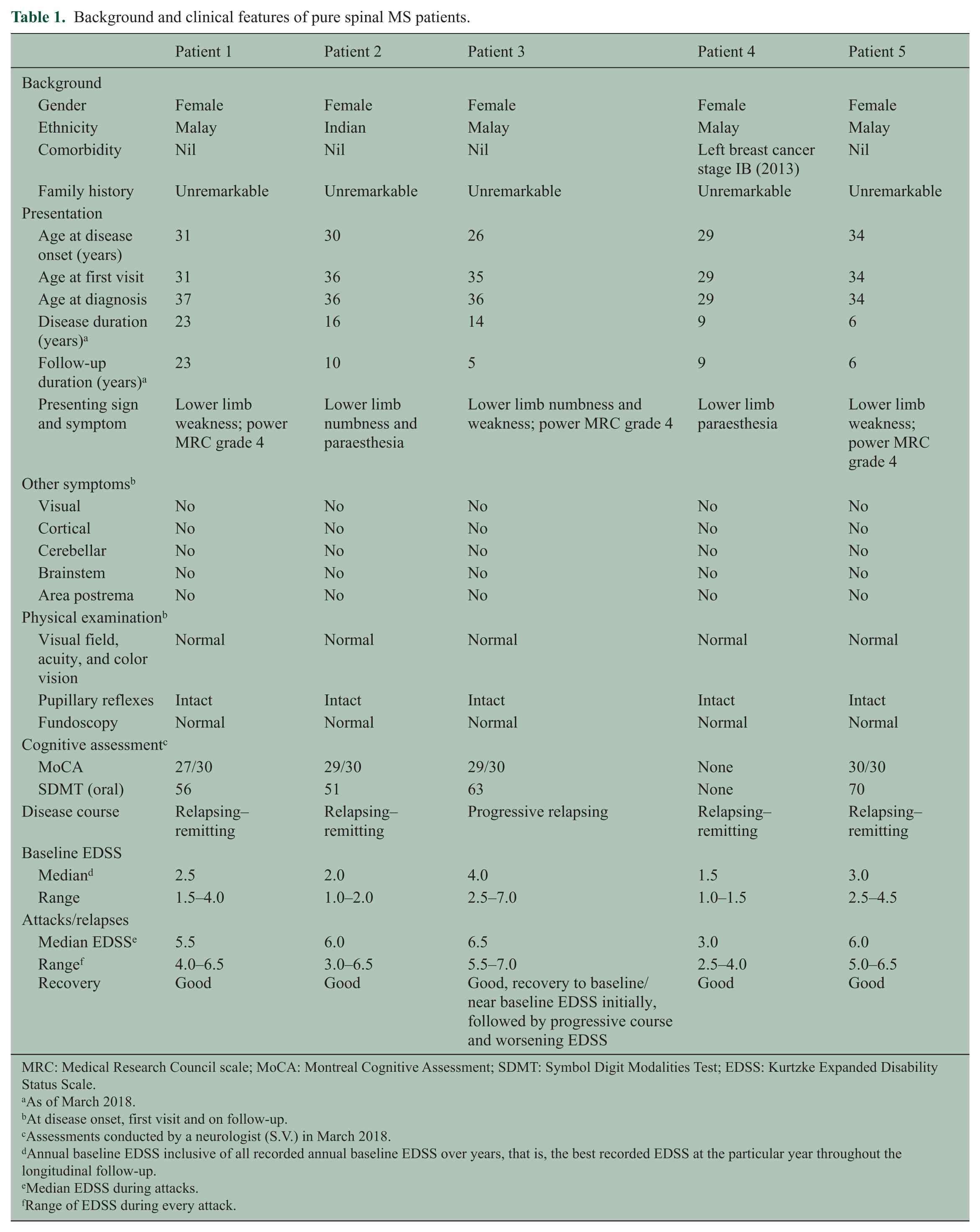
MRC: Medical Research Council scale; MoCA: Montreal Cognitive Assessment; SDMT: Symbol Digit Modalities Test; EDSS: Kurtzke Expanded Disability Status Scale.
As of March 2018.
At disease onset, first visit and on follow-up.
Assessments conducted by a neurologist (S.V.) in March 2018.
Annual baseline EDSS inclusive of all recorded annual baseline EDSS over years, that is, the best recorded EDSS at the particular year throughout the longitudinal follow-up.
Median EDSS during attacks.
Range of EDSS during every attack.
All five patients presented with recurrent partial myelopathy but demonstrated no features to suggest cortical, cerebellar, brainstem, area postrema, or visual tract lesions, both at their disease onset and on follow-up. Their attacks consisted of SSPM with median EDSS: 5.5 (range: 2.5–7.0) during attacks. The nadir EDSS was 7.0 in Patient 3 as she was unable to walk ≥20 m and opted for wheelchair ambulation during the worst attacks. Their attacks were mostly steroid responsive with good recovery as evidenced by the return of limb motor power and EDSS to baseline/near baseline.
Cognitive assessments through Montreal Cognitive Assessment and Symbol Digit Modalities Test revealed no obvious impairment.
Laboratory and neurophysiological findings
Analysis of paired CSF and serum OCBs in four patients demonstrated OCBs in CSF but not in serum. Patient 5 refused lumbar puncture. CSF findings atypical of MS 1 were absent. None were anti-AQP4 antibody positive despite repeated assessments. Four patients were tested negative for anti–myelin oligodendrocyte glycoproteins (MOG) antibody. Nor-mal visual evoked potentials with abnormal somatosensory evoked potentials were recorded (see Table 2).
Laboratory, neurophysiological, and neuroimaging characteristics of pure spinal MS patients.
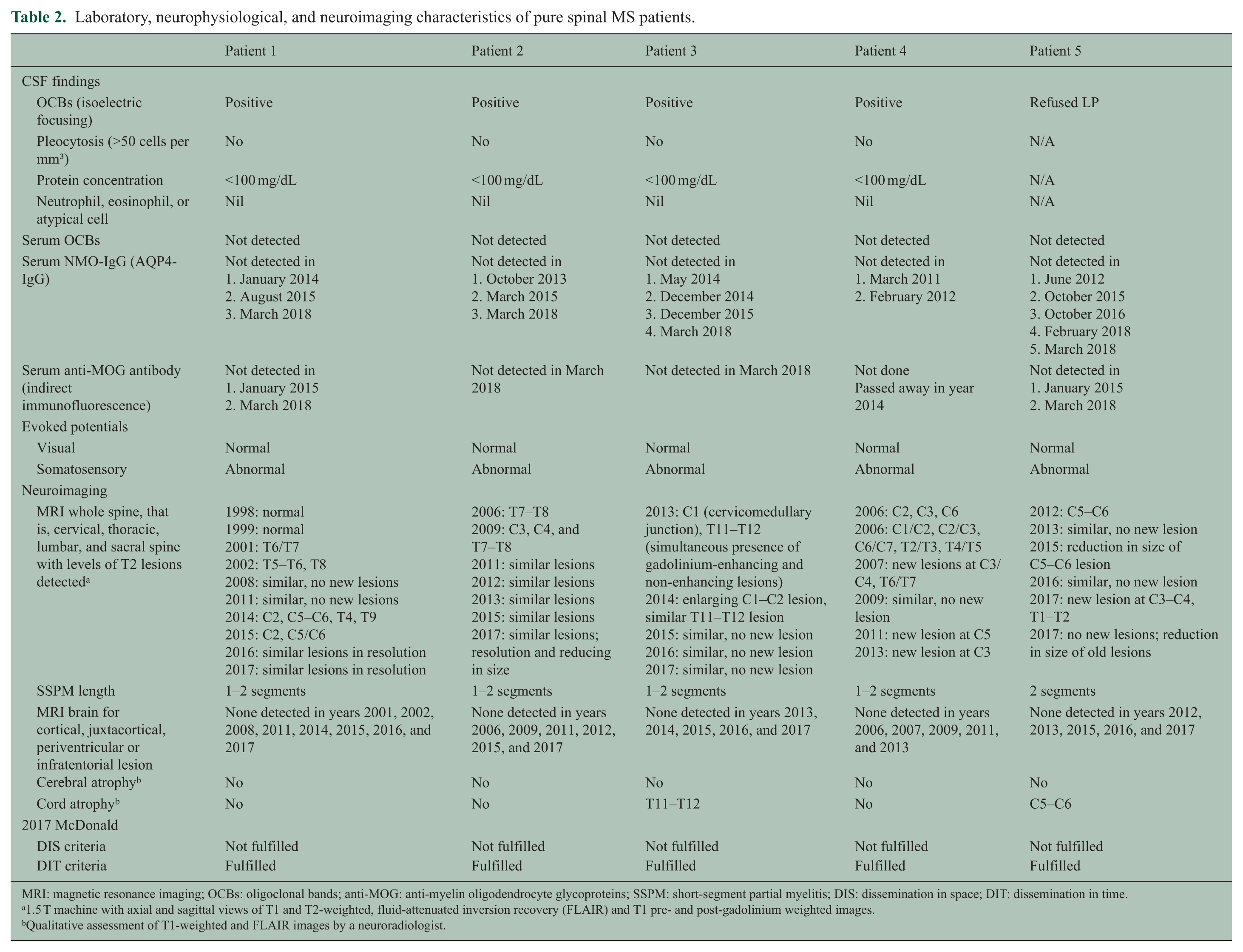
MRI: magnetic resonance imaging; OCBs: oligoclonal bands; anti-MOG: anti-myelin oligodendrocyte glycoproteins; SSPM: short-segment partial myelitis; DIS: dissemination in space; DIT: dissemination in time.
1.5 T machine with axial and sagittal views of T1 and T2-weighted, fluid-attenuated inversion recovery (FLAIR) and T1 pre- and post-gadolinium weighted images.
Qualitative assessment of T1-weighted and FLAIR images by a neuroradiologist.
Comprehensive work-up for alternative diagnoses of myelitis, namely, infections, thyroid and other metabolic diseases, vascular diseases, subacute combined degeneration of spinal cord, autoimmune and connective tissue diseases, sarcoidosis, Behcet’s syndrome, and paraneoplastic screening was consistently negative.
Neuroimaging of the brain and whole spine
Sequential MRI of brain and whole spine (cervical, thoracic, and lumbosacral) did not show MS-/neuromyelitis optica spectrum disorder (NMOSD)-like dissemination in space (DIS; see Table 2). In the absence of typical MS-like brain lesions, 1 all five patients developed peripheral cord lesions with lengths of ≤2 vertebral segments at different cervical and thoracic cord levels (see Figure 2).

Brain and spinal cord MRI images (sagittal and axial views) of pure spinal multiple sclerosis patients.
They demonstrated dissemination in time (DIT) through the (1) presence of both Gadolinium-enhancing and non-enhancing lesions simultaneously in a single scan and (2) presence of new T2 or Gadolinium-enhancing lesions on follow-up scans.
Longitudinally extensive spinal cord lesion suggestive of longitudinally extensive transverse myelitis (LETM) was not seen. There was no obvious brain volume loss (cerebral atrophy) upon qualitative assessment by neuroradiologist.
Treatment and progress
These patients demonstrated good response to interferons when initiated, as well as when changed to other DMTs, namely, fingolimod due to relapses on interferon in Patient 2 and teriflunomide due to injection-related side effects in Patient 1 (see Table 3). None deteriorated while being compliant to DMTs as evidenced by their stable EDSS. Cumulatively for these five patients, ARR without DMTs = 0.80, ARR on DMTs = 0.16, relative ARR on DMTs = 0.20, and rate of reduction in ARR while on DMTs = 80% (p < 0.001; see Table 4). There were only three true relapses (two in Patient 2 as mentioned and one in Patient 3 due to non-compliance to interferon) throughout the 18.5 cumulative years on DMTs among them. Radiologically, with the initiation of DMTs, resolution and reduction in the size of existing spinal cord lesions were observed without new lesions.
Treatments and progress of pure spinal MS patients.
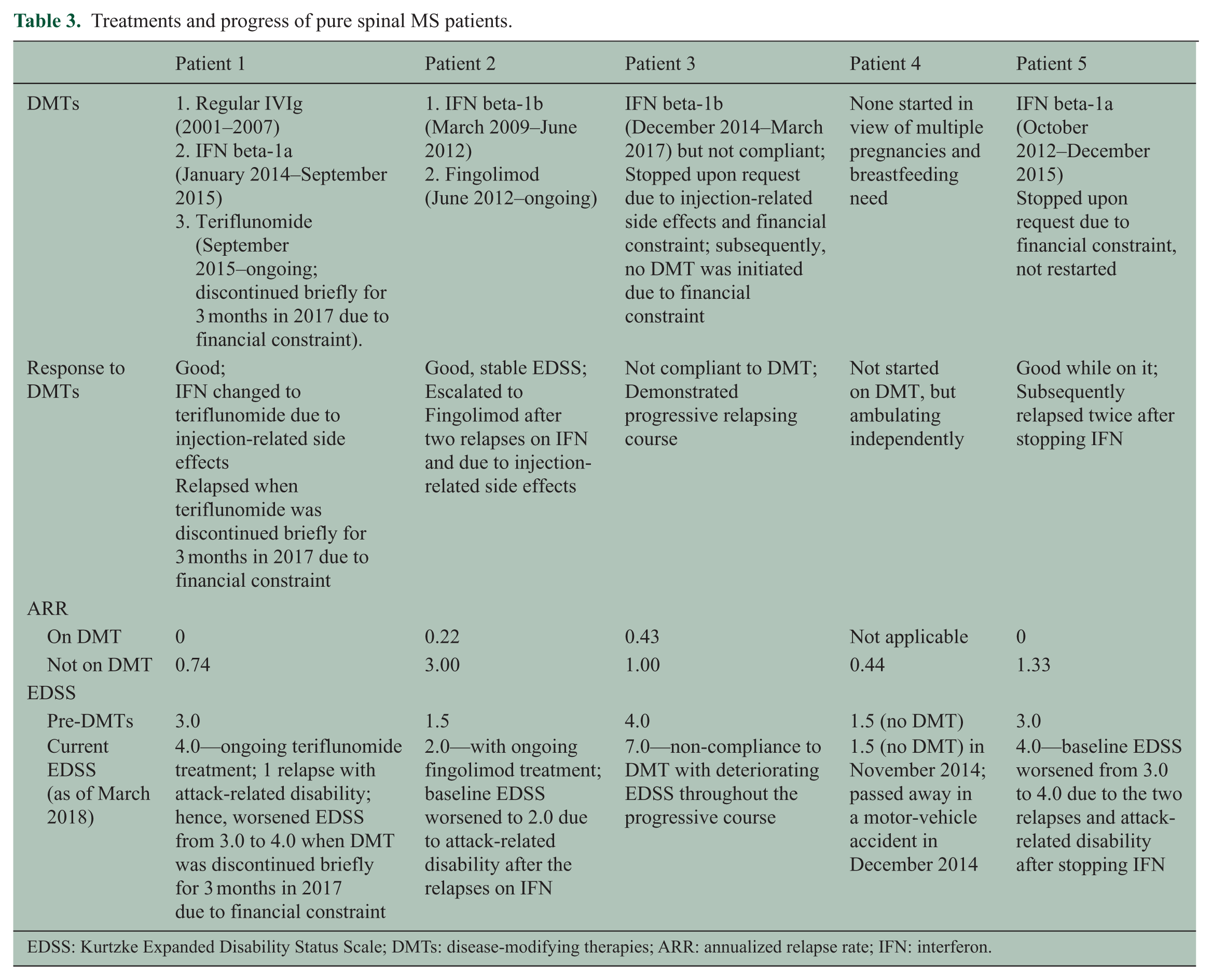
EDSS: Kurtzke Expanded Disability Status Scale; DMTs: disease-modifying therapies; ARR: annualized relapse rate; IFN: interferon.
Cumulative number of years, number of attacks, ARR, and relative ARR while on DMTs and not on DMTs for the five patients cumulatively.
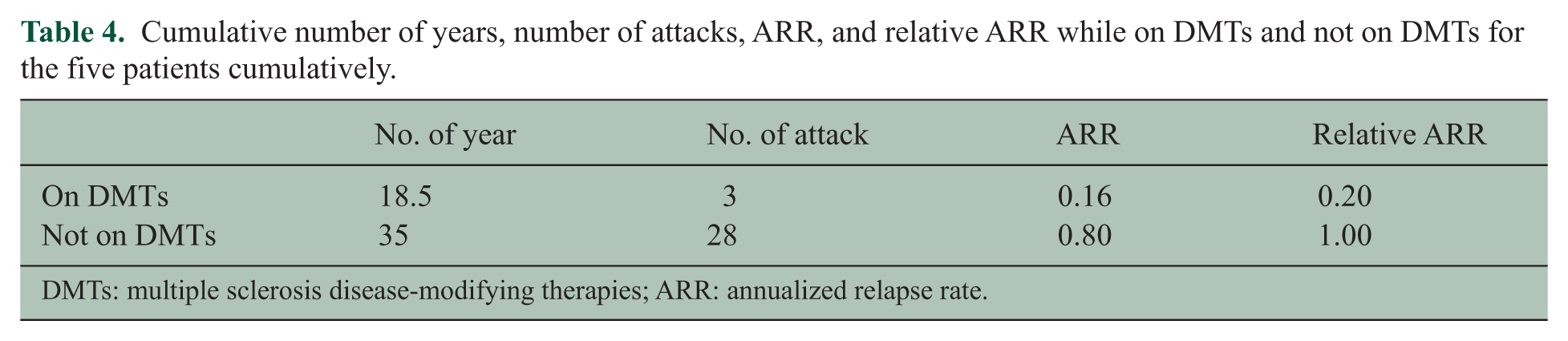
DMTs: multiple sclerosis disease-modifying therapies; ARR: annualized relapse rate.
Patient 3 was not compliant to and subsequently terminated interferon therapy due to injection-related side effects and financial constraints. She demonstrated progressive course with gradually worsening baseline EDSS over years. Patient 5 who opted to terminate DMT due to financial constraint subsequently relapsed and developed new MRI T2 cord lesion, followed by attack-related disability. Meanwhile, due to recurrent pregnancies and breastfeeding need, no DMT was started for Patient 4 who demonstrated accumulation of asymptomatic new T2 cord lesions over years.
Discussion
Literature review using PubMed with MeSH terms “multiple sclerosis,” “recurrent myelitis,” and “short myelitis” revealed no existing report on pure spinal MS. These five patients did not fulfill the 2017 McDonald criteria 1 nor the 2015 International NMOSD criteria. 2 Thus, we postulate that they may represent a novel, never reported entity of pure spinal MS yet to be established, defined, and categorized.
These patients demonstrated features suggesting an MS-type myelitis while making NMOSD2,3 and other IIDDs unlikely, namely, (1) peripheral instead of central cord lesions; (2) absence of LETM, optic neuritis, area postrema syndrome, and encephalopathy; (3) positive CSF OCBs; (4) repeatedly negative anti-AQP4 antibody; (5) negative anti-MOG antibody; (6) attacks with moderate severity but good recovery, (7) good response to MS DMTs with relapse frequency controlled and no clinical or radiological deterioration while on DMTs, and (8) the presence of progressive course in some. There are reports suggesting that interferons and fingolimod are inefficacious and may even exacerbate NMOSD.4–7 Hence, these patients’ response to DMTs may further support an MS-type pathology over NMOSD. None had cerebral atrophy or cognitive dysfunction. Anti-MOG-related pathology was ruled out as well. 8
The SSPM in Patient 4 was unlikely paraneoplastic as the onset was 7 years prior to the breast cancer occurrence with no LETM nor severe progressive disability.9,10
Conclusion
The 2017 McDonald criteria rightly allude to the presence of atypical groups of demyelination which require further research. We concur by sharing knowledge on a cohort of Asian patients with relapsing SSPM who phenotypically resemble MS-type partial myelitis with relapsing and progressive disease courses albeit not fulfilling the McDonald criteria as they demonstrated DIT over years but DIS only within the spinal cord in the absence of typical MS-like brain or optic nerve lesions. We hereby postulate a possible diagnosis of pure spinal MS, which may represent a novel forme fruste within the MS disease spectrum, thus heralding the need for continuing research and exploration.
Supplemental Material
MSJ775912_supplementary_figure_1 – Supplemental material for Pure spinal multiple sclerosis: A possible novel entity within the multiple sclerosis disease spectrum
Supplemental material, MSJ775912_supplementary_figure_1 for Pure spinal multiple sclerosis: A possible novel entity within the multiple sclerosis disease spectrum by Jie Ping Schee and Shanthi Viswanathan in Multiple Sclerosis Journal
Supplemental Material
MSJ775912_supplementary_figure_2 – Supplemental material for Pure spinal multiple sclerosis: A possible novel entity within the multiple sclerosis disease spectrum
Supplemental material, MSJ775912_supplementary_figure_2 for Pure spinal multiple sclerosis: A possible novel entity within the multiple sclerosis disease spectrum by Jie Ping Schee and Shanthi Viswanathan in Multiple Sclerosis Journal
Supplemental Material
MSJ775912_supplementary_figure_3 – Supplemental material for Pure spinal multiple sclerosis: A possible novel entity within the multiple sclerosis disease spectrum
Supplemental material, MSJ775912_supplementary_figure_3 for Pure spinal multiple sclerosis: A possible novel entity within the multiple sclerosis disease spectrum by Jie Ping Schee and Shanthi Viswanathan in Multiple Sclerosis Journal
Supplemental Material
MSJ775912_supplementary_figure_4 – Supplemental material for Pure spinal multiple sclerosis: A possible novel entity within the multiple sclerosis disease spectrum
Supplemental material, MSJ775912_supplementary_figure_4 for Pure spinal multiple sclerosis: A possible novel entity within the multiple sclerosis disease spectrum by Jie Ping Schee and Shanthi Viswanathan in Multiple Sclerosis Journal
Supplemental Material
MSJ775912_supplementary_figure_5 – Supplemental material for Pure spinal multiple sclerosis: A possible novel entity within the multiple sclerosis disease spectrum
Supplemental material, MSJ775912_supplementary_figure_5 for Pure spinal multiple sclerosis: A possible novel entity within the multiple sclerosis disease spectrum by Jie Ping Schee and Shanthi Viswanathan in Multiple Sclerosis Journal
Footnotes
Acknowledgements
The authors would like to thank the Director General of Health Malaysia for the permission to publish this paper. The authors acknowledge the contribution of Dr Norzaini Rose bt Mohd Zain in the qualitative assessment of MRI brain volume, in particular on the presence of cerebral atrophy. Dr Norzaini Rose is a neuroradiologist currently serving in the Department of Radiology, Kuala Lumpur General Hospital, Malaysia. Jie Ping Schee contributed to study design, acquisition of data, analysis and interpretation of data, and manuscript drafting. Shanthi Viswanathan contributed to study concept and design, analysis and interpretation of data, study supervision, manuscript drafting and critical revision of manuscript for intellectual content.
Ethics approval
Ethics approval for the study was obtained from the Medical Research and Ethics Committee Malaysia (ref no. 10503), valid for 1 year from September 2017 till September 2018.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consents were obtained from patients for the publication of their clinical information and MRI images. For Patient 4 who passed away, informed consent was obtained from her next of kin (sister).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.