
Abstract
The care of multiple sclerosis (MS) in France is based on two complementary interlinked networks: MS expert centers in university hospitals and regional networks of neurologists. The routine use of European database for multiple sclerosis (EDMUS) in all those centers has paved the way for the constitution of a national registry, designated as Observatoire Français de la Sclérose En Plaques (OFSEP). It promotes a prospective, standardized, high-quality, and multimodal collection of data. On June 2018, there were 68.097 files, with 71.1% females, representing 761,185 person-years. This huge database is open to the scientific community and might contribute exploring unresolved issues and unmet needs in MS.
The care of multiple sclerosis (MS) by neurologists in France is based on two complementary and closely interlinked networks: MS expert centers and regional networks of neurologists dedicated to MS. All have been using EDMUS, a specific software with standardized language, fully integrated in daily practice, for many years. 1 In 2011, they decided to formally collaborate by creating Observatoire Français de la Sclérose en Plaques (OFSEP), a nationwide systematic longitudinal follow-up study of MS persons, funded for a 10-year tenure by the “Investments for the Future” program. Objectives were to expand the existing cohort, combining clinical and magnertic resonance imaging (MRI) data with biological samples, providing a unique source of information on MS epidemiology in France, with a particular focus on pharmaco-epidemiology of recently introduced disease-modifying treatments (DMTs).
Patients and methods
All French neurologists using European database for multiple sclerosis (EDMUS) agreed to participate and to open the collection of data to their regional network. 1 Lorraine is the only administrative region with an exhaustive and certified registry for MS patients (ReLSEP). Patients are included if they are diagnosed with MS according to the latest criteria, or present radiologically and clinically isolated syndromes (RISs and CISs) suggestive of MS and MS-related conditions, that is, neuromyelitis optica spectrum disorders (NMOSDs) and anti-MOG disease.
Clinical data are collected during routine follow-up visits, usually at least once a year, retrospectively at the first visit and prospectively thereafter. A minimal mandatory data set has been defined (Supplementary data, Figure 1); it includes demographic and socioeconomic characteristics, a description of the disease (neurological episodes, disability, and description of brain or spinal cord magnetic resonance imaging (MRI) scans) and disease-modifying treatments (DMTs; dates of start and stop, reason for stopping). Serious adverse events related to a treatment or not, are systematically collected since January 2017. Biological samples are collected in a subset of patients and only once because of financial constraints: RIS, CIS, relapsing-remitting multiple sclerosis (RRMS), primary-progressive multiple sclerosis (PPMS), NMOSD, acute disseminated encephalomyelitis (ADEM), progressive multifocal leukoencephalopathy (PML) (Supplementary data, Table 1). They are stored in certified local biobanks (ISO9001 standards, NF S96-900) with quality assessments. Brain and spinal cord MRIs prescribed as part of patient care are carried out, whenever possible, according to standardized acquisition OFSEP protocols (Supplementary data, Table 2). 2 Pseudonymized MRIs are stored in a centralized imaging resource center (http://shanoir.org).
Data confidentiality and safety are ensured according to the recommendations of the French Commission Nationale Informatique et Libertés (CNIL). OFSEP has received approval for storing clinical, biological, and imaging data for research purpose. Patients give informed consent for their data to be stored in the database and used for research, in France and abroad (www.ofsep.org/en/cohort/ofsep-consent). The cohort has been registered to clinicaltrials.gov under the number NCT02889965.
OFSEP is supported by a grant from the French Government and the EDMUS Foundation. It also received continuous support from the Aide à la Recherche sur la Sclérose en Plaques (ARSEP) Foundation.
Results
On 15 June 2018, 68,097 patients’ records from 36 centers have been collected. After exclusion of duplicates and inconsistencies, NMOSD or ADEM, missing date of disease onset and uncertain diagnosis, 56,134 records were analyzed. There were 39,913 females (71.1%). Mean age at onset was 32.5 (±10.7) years; 62.4% started between 20 and 39 years, 5.5% before the age of 18 and 6.3% after 50. Median disease duration was 12.2 years; 25% have been followed for more than 20 years. OFSEP represents 761,185 person-years with data from MS onset to last follow-up, including 393,805 person-years collected prospectively. Onset was RRMS in 88.7%, with a mean age at onset of 32.0 (±10.5) years; 11.3% were progressive from onset (PPMS), at 44.1 (± 10.8) years. Distribution of the clinical course of MS according to disease duration and to patients’ age illustrates the relation of the progressive phase with time and age (Supplementary data, Figure 2). Mean number of Expanded Disability Status Scale (EDSS) evaluations per patient was 8 (±10), mean time between two evaluations was 0.93 (±1.64) year. There were overall 392,281 EDSS evaluations. Completeness of a pre-defined selection of data is presented in Figure 1. When comparing ReLSEP to the rest of the OFSEP cohort (Table 1), initial course of MS differed slightly but remained within the range usually described in natural history studies. ReLSEP had a better diagnostic certainty, perhaps due to the specific effort done locally in Lorraine to enter paraclinical data that contribute to establish the diagnosis. Age and MS duration at last follow-up were longer in Lorraine and could also account for the higher proportion of secondary-progressive multiple sclerosis (SPMS) patients (29% vs 17.6%). A higher proportion of ReLSEP patients were not treated with DMTs at the last follow-up (43.9% vs 34%).
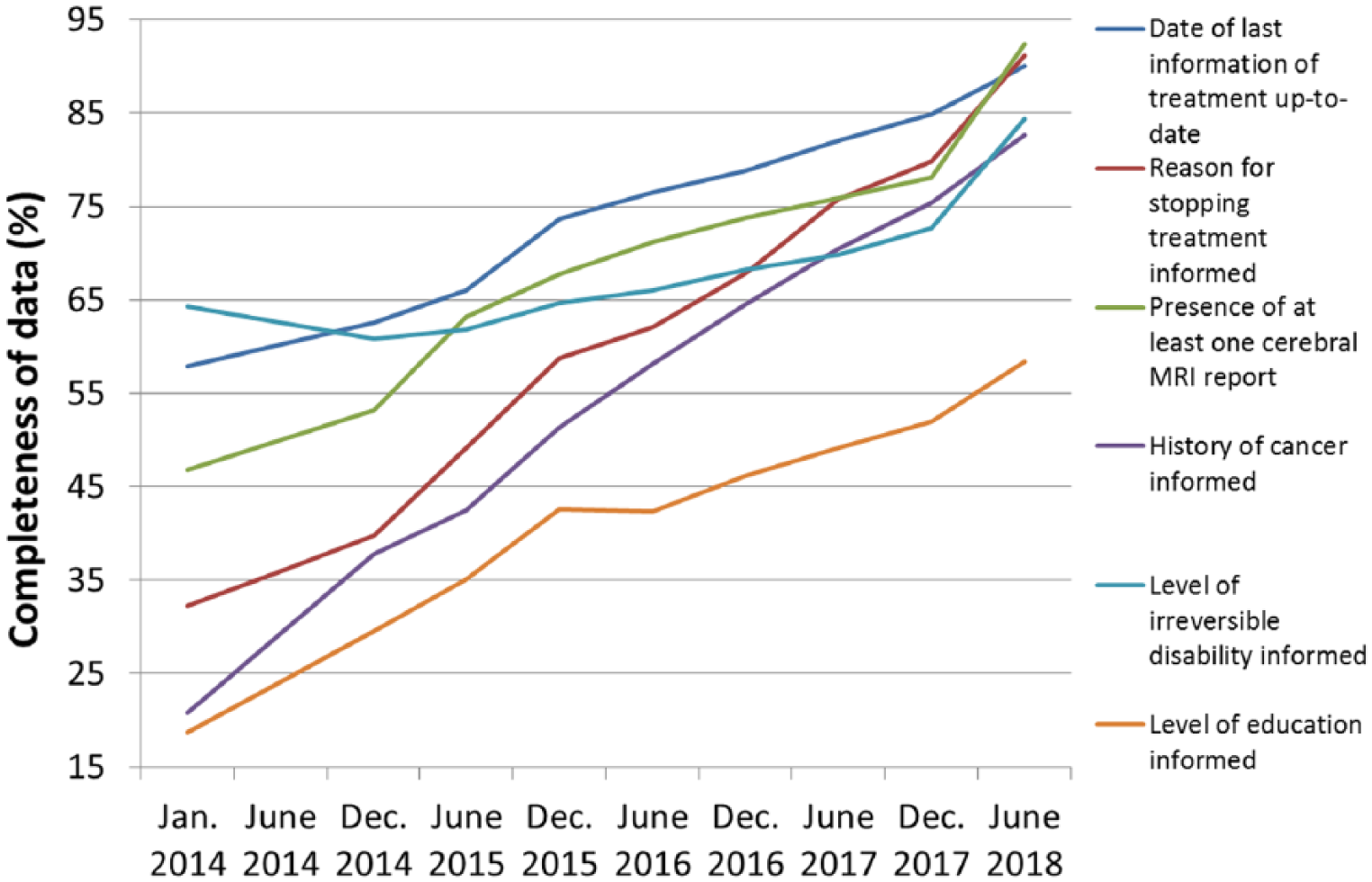
Evolution of the OFSEP data completeness since 2014.
Demographic and clinical characteristics of the Lorraine registry (ReLSEP) compared to all other OFSEP patients.
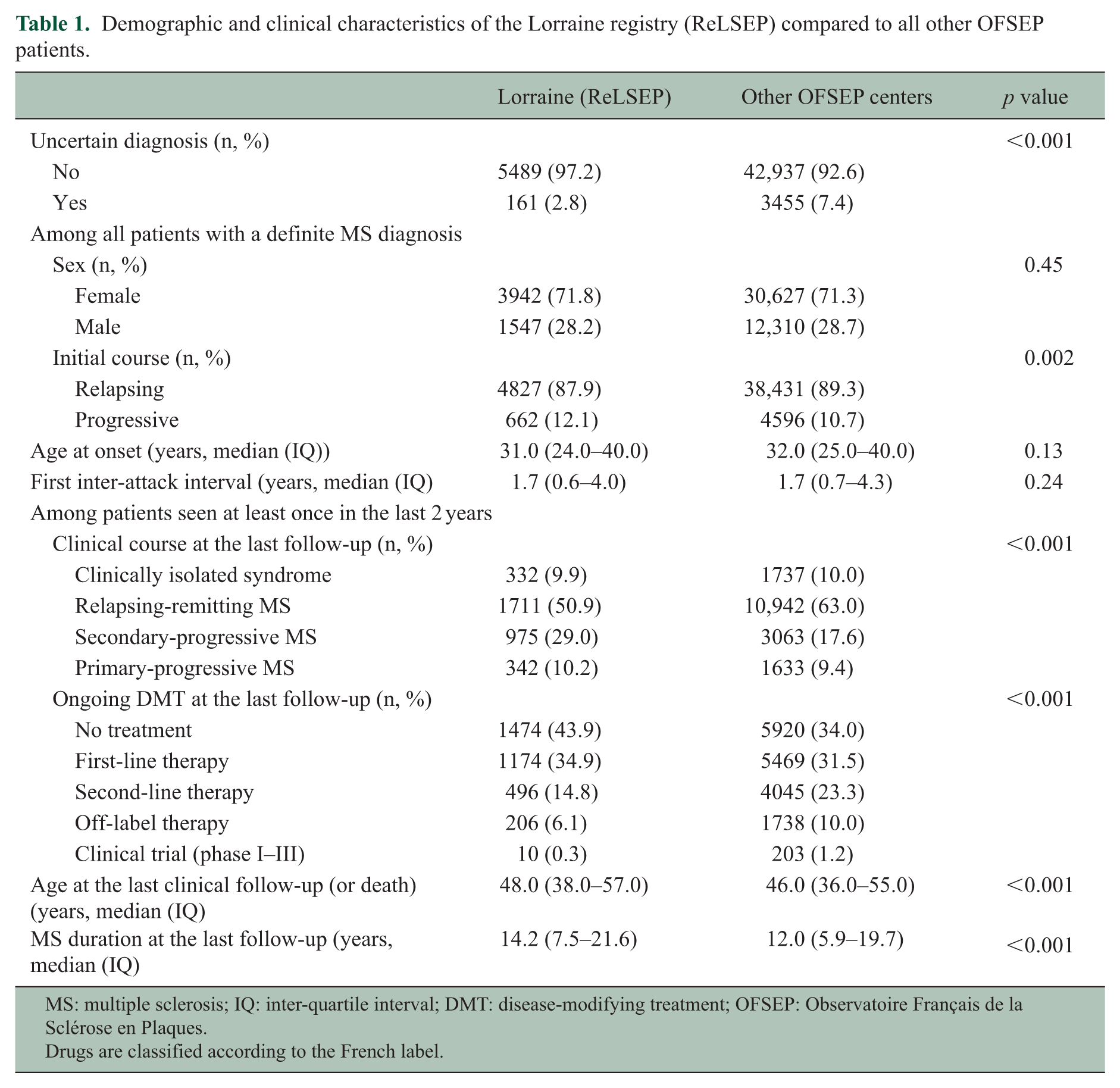
MS: multiple sclerosis; IQ: inter-quartile interval; DMT: disease-modifying treatment; OFSEP: Observatoire Français de la Sclérose en Plaques.
Drugs are classified according to the French label.
Raw MRI acquisitions are available in OFSEP standards for 1276 patients, 300 with at least two different time points. Biological kits (including cerebrospinal fluid (CSF) in 50%) have been collected in more than 1000 patients.
Discussion
In 2011, France launched a “big epidemiological and research tool” for MS by granting the OFSEP cohort. This national registry combines not only clinical data but also standardized MRI and biological samples. Currently, OFSEP includes over 68,000 records, more than 50% of the French cases identified in the national insurance database. Baseline characteristics of the entire cohort are similar to large natural history studies. The comparison with the ReLSEP registry shows however that OFSEP might over-represent treated patients and miss some who are not treated, at the beginning of the disease or more frequently at later stages, that might not be followed by neurologists anymore. The higher proportions of patients treated with second-line and off-label therapies in OFSEP might also be explained by some recruitment bias toward more active patients seen in referral centers.
OFSEP has implemented a strategy to improve the quality of its data and samples. The EDMUS software has an integrated data verification tool to identify missing or incoherent data. Twice a year, a quality report is sent to all centers, with queries on incoherent data entries. Information documents, data quality indicators, training sessions and audits are displayed. Since 2016, the annual funding allocated to the centers to facilitate data collection takes into account quality indicators, beside the number of cases.
Real-world data can contribute improving the post-marketing surveillance of DMTs. Implementing studies within a unique registry could inform individual risk management programs on safety, efficacy, good use, and risk/benefit balance of DMTs but also provide a unique data set to estimate the cumulative risks of treatments, help define the best therapeutic strategies in the future and compare DMTs in real-life settings. In this setting, besides specific drug reports provided regularly to industrials or French health authorities, OFSEP already contributed to evaluate the comparative effectiveness of first and second-line DMTs,3,4 the risk or rebound after natalizumab withdrawal 5 and the impact of risk stratification on PML incidence in France. 6 These objectives have been shared since 2013 with four other MS registries (MSBase, Denmark, Italy, Sweden) within the BigMSData network. Efforts have been made to improve standardization and quality that are necessary to collaborate.7–9 A first common project evaluated the optimal time to start treatment in RRMS. 10 A core protocol using exclusively real-world data generated by the registries for post-marketing studies has been designed in collaboration with industrials involved in MS and is currently under evaluation by the European Medicines Agency.
Supplemental Material
MSJ815602_Annex_1 – Supplemental material for Observatoire Français de la Sclérose en Plaques (OFSEP): A unique multimodal nationwide MS registry in France
Supplemental material, MSJ815602_Annex_1 for Observatoire Français de la Sclérose en Plaques (OFSEP): A unique multimodal nationwide MS registry in France by Sandra Vukusic, Romain Casey, Fabien Rollot, Bruno Brochet, Jean Pelletier, David-Axel Laplaud, Jérôme De Sèze, François Cotton, Thibault Moreau, Bruno Stankoff, Bertrand Fontaine, Francis Guillemin, Marc Debouverie and Michel Clanet in Multiple Sclerosis Journal
Supplemental Material
MSJ815602_Supplementary_Data – Supplemental material for Observatoire Français de la Sclérose en Plaques (OFSEP): A unique multimodal nationwide MS registry in France
Supplemental material, MSJ815602_Supplementary_Data for Observatoire Français de la Sclérose en Plaques (OFSEP): A unique multimodal nationwide MS registry in France by Sandra Vukusic, Romain Casey, Fabien Rollot, Bruno Brochet, Jean Pelletier, David-Axel Laplaud, Jérôme De Sèze, François Cotton, Thibault Moreau, Bruno Stankoff, Bertrand Fontaine, Francis Guillemin, Marc Debouverie and Michel Clanet in Multiple Sclerosis Journal
Footnotes
Acknowledgements
In memory of Prof Christian Confavreux, who devoted his career to the development of EDMUS, OFSEP, and more generally to national, European, and worldwide collaborations to improve our knowledge of MS and patient’s care. The authors are indebted to the patients for their participation to the OFSEP project and Mrs Véronique Millot for assistance in preparing the manuscript. They are deeply grateful to the International Advisory Board for their continuous support and appreciated advice: Prof Steven Reingold (New York, USA), Prof David Miller (London, UK), Prof Neil Scolding (Bristol, UK), and Prof Hartmut Wekerle (Munich, Germany). S.V., R.C., and F.R. contributed to the study concept and design, analysis and interpretation, writing of the manuscript. F.G. contributed to the acquisition of data, analysis and interpretation, and critical revision of the manuscript for important intellectual content. B.B., J.P., D.-A.L., J.D.S., F.C., T.M., B.S., B.F., M.D., and M.C. contributed to the study concept and design, acquisition of data, analysis and interpretation, and critical revision of the manuscript for important intellectual content. OFSEP investigators are listed in Annex 1.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: S.V. has received consulting and lecturing fees, travel grants, and unconditional research support from Biogen, Geneuro, Genzyme, MedDay, Merck Serono, Novartis, Roche, Sanofi Aventis, and Teva Pharma. B.B. has received consulting and lecturing fees, travel grants, and unconditional research support from Actelion, Biogen, Genzyme, MedDay, Novartis, Merck Serono, Roche, Sanofi Aventis, and Teva Pharma. J.P. has received consulting and lecturing fees, travel grants, and unconditional research support from Biogen, Genzyme, Novartis, MedDay, Merck Serono, Roche, Sanofi Aventis, and Teva Pharma. D.-A.L. has received consulting and lecturing fees, travel grants, and unconditional research support from Biogen, Genzyme, Novartis, Merck Serono, Roche, Sanofi Aventis, and Teva Pharma. J.D.S. has received consulting and lecturing fees, travel grants, and unconditional research support from Biogen, Genzyme, Novartis, Merck Serono, Roche, Sanofi Aventis, and Teva Pharma. F.C. has received consulting and lecturing fees, travel grants, and unconditional research support from Biogen, Novartis, Bracco imaging, Bayer Schering, and Guerbet. T.M. has received consulting and lecturing fees, travel grants, and unconditional research support from Biogen, Genzyme, Novartis, Merck Serono, Roche, Sanofi Aventis, and Teva Pharma. B.S. has received consulting and lecturing fees, travel grants, and unconditional research support from Biogen Idec, Merck Serono, Novartis, Genzyme, Teva Pharma, and Roche. B.F. has received a research grant from Biogen and is supported by funding from the “Investment for the Future” program ANR-10-IAIHU-06 and ANR-10-INBS-01-D1. M.D. has received consulting and lecturing fees, travel grants, and unconditional research support from Biogen, Genzyme, Novartis, Merck Serono, Roche, Sanofi Aventis, and Teva Pharma. The remaining authors have no financial disclosure to declare.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Observatoire Français de la Sclérose en Plaques (OFSEP) is supported by a grant provided by the French State and handled by the “Agence Nationale de la Recherche,” within the framework of the “Investments for the Future” program, under the reference ANR-10-COHO-002, by the Eugène Devic EDMUS Foundation against multiple sclerosis and by the ARSEP Foundation.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.