
Abstract
Magnetic resonance imaging (MRI) has revolutionized the diagnosis and management of people living with multiple sclerosis (MS). However, conventional MRI sequences and measures currently used in clinical practice have limitations in the appropriate diagnosis, prediction of future disability, and monitoring of disease activity in MS. A specific challenge is the accurate and timely diagnosis of progressive subtypes of MS. This article will summarize emerging MRI measures that may be of utility as clinical tools in diagnosis and prediction in MS. Although a wide range of MRI techniques have different strengths and weaknesses, those that will be discussed in this article include the “central vein sign,” leptomeningeal inflammation/enhancement, conventional and quantitative spinal cord imaging, susceptibility-weighted imaging, and high-field MRI techniques. There are a number of novel and emerging MRI techniques that hold promise in improving diagnosis, prediction, and disease monitoring in MS.
Introduction
The widespread availability of magnetic resonance imaging (MRI) has revolutionized the diagnosis and management of people living with multiple sclerosis (MS). Conventional MRI protocols of the brain, which typically include T1-weighted, T2-weighted, fluid-attenuated inversion recovery (FLAIR), and diffusion-weighted sequences, 1 have greatly facilitated the diagnosis and clinical management of people living with MS. The most recent revisions to the McDonald criteria in 2017 enable the diagnosis of MS in the vast majority of patients at the first clinical presentation. 2 Furthermore, MRI is frequently used not only for diagnosis but also as a predictive tool of disease course and to monitor disease activity and treatment response in relapsing-remitting MS.
Although there is clear utility of clinical-grade, conventional MRI in the diagnosis and management of MS in daily practice, it is not without limitations. The latest revisions to the McDonald criteria facilitate the early diagnosis of MS; however, the increase in sensitivity comes at the risk of a decrease in specificity, 3 which increases the likelihood of misdiagnosis when applied in inappropriate or ambiguous clinical settings. Recent studies have demonstrated that misdiagnosis of MS is not uncommon, even in experienced academic centers.4,5 Furthermore, another recent study demonstrated that even among experienced MS neurologists, the 2017 McDonald diagnostic criteria for MS are frequently utilized incorrectly. 6
Another challenge in clinical practice is the inability to rapidly and accurately diagnose progressive variants of MS, including primary-progressive MS (PPMS) and secondary-progressive MS (SPMS). A significant contribution to the delays and uncertainty observed when diagnosing progressive MS is that there is no clear imaging biomarker that is specific for progressive MS, or that signifies the transition from relapsing to progressive MS [e-1].
After an individual is diagnosed with MS, there are numerous additional unmet needs in clinical practice. One of the most evident is the need for improved methods to predict disease activity and disease course in individual patients. The ability to more accurately predict disease activity and disease course would facilitate delivering personalized, optimal therapy to individual patients, which would improve clinical outcomes in the longer term. Although conventional, clinical-grade MRIs have moderate predictive value for future disability at the time of MS diagnosis, 7 their utility is limited in this regard [e-2]. As such, the need for improved methods to predict MS disease course is evident, and novel and emerging imaging measures may have significant utility by addressing some of the limitations of conventional, clinical-grade MRI techniques.
This article will summarize emerging MRI measures that may be of utility as clinical tools in diagnosis and prediction in MS. Although a wide range of MRI techniques hold promise and have different strengths and weaknesses, those that will be discussed in this article include the “central vein sign” (CVS), leptomeningeal (LM) inflammation/enhancement, conventional and quantitative spinal cord imaging, susceptibility-weighted imaging, and high-field MRI techniques.
The CVS
Susceptibility-based MRI sequences, including T2*-weighted sequences, enable the visualization of central veins within white matter lesions (WMLs) that are not easily seen on T2-based sequences (Figure 1).8–10 The observed hypointensity is related to deoxyhemoglobin within WMLs which is often related to the presence of a central vein. When visualized within a WML, these “central veins” are suggestive of perivenular inflammation and demyelination, which is a pathological hallmark of lesions [e-3] related to MS. Although the sequences and methods to optimally evaluate the central vein are still under debate, a number of studies and recently published consensus criteria by the North American Imaging in MS Cooperative (NAIMS) have been useful to guide on-going studies on this subject. 11
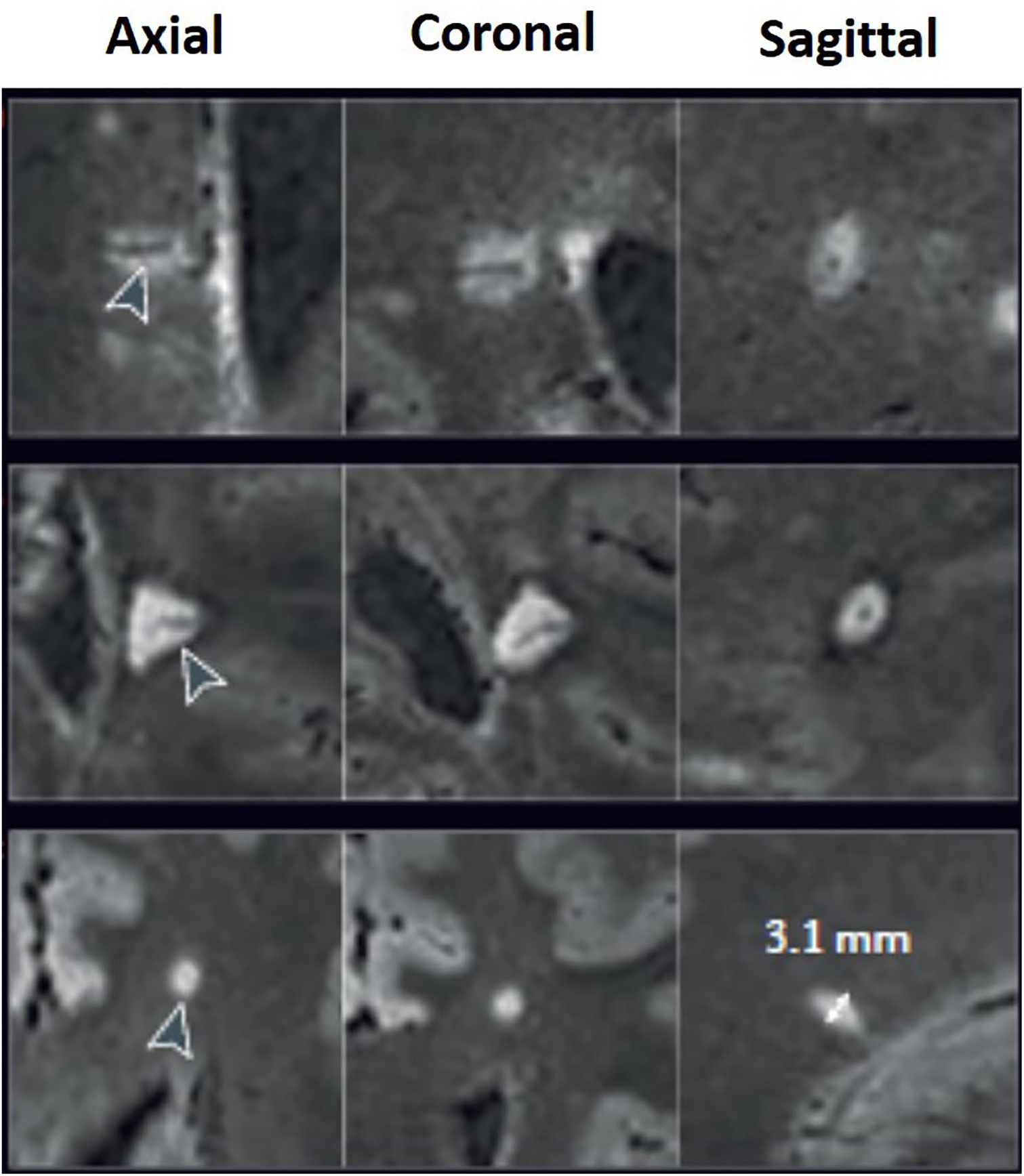
FLAIR* (combined T2*-weighted MRI and fluid-attenuated inversion recovery) sequences demonstrating white matter lesions with visible central veins (axial, coronal, and sagittal views). This figure was reproduced with permission from Sati P, Oh J, Constable RT, et al. The central vein sign and its clinical evaluation for the diagnosis of multiple sclerosis: a consensus statement from the North American Imaging in Multiple Sclerosis Cooperative. Nat Rev Neurol 2016; 12(12): 714–722. doi: 10.1038/nrneurol.2016.166. Epub November 11 2016.
A number of groups have demonstrated the potential clinical utility of identifying central veins in WML, as the presence of a large proportion of WML demonstrating central veins (the CVS) has utility in distinguishing MS from other white matter disorders12,13 [e-4]. Although different criteria have been proposed, at the current time, the 40% threshold (defined as >40% of WML demonstrating the CVS) appears to be the most robust criterion to distinguish MS from other white matter disorders. Simplified criteria, including the six-lesion rule 8 (defined as six or more lesions demonstrating the CVS as an indication that individuals have a high likelihood of having MS), have also been proposed to adequately distinguish MS from other white matter disorders, and proposed criteria continue to evolve. Automated techniques are also being developed to detect the CVS, which may alleviate the practical concerns regarding time and resources that are required when all WMLs in the brain in a particular patient need to be evaluated for the CVS. 14
Preliminary studies also suggest that there may be predictive value in identifying the CVS. A recent study that evaluated the CVS in a cohort of radiologically isolated syndrome (RIS) subjects found that the majority (90%) of RIS subjects meet the 40% threshold that has been proposed to distinguish MS from other white matter disorders. 15 Furthermore, there were significant relationships between the proportion of CVS-positive WML and spinal cord lesions, which is a known risk factor for conversion of RIS to MS [e-5]. Taken together, these findings suggest that the proportion of CVS-positive WML may not only be useful in diagnosing MS but also may have prognostic value in early MS. Prospective follow-up of this cohort will be necessary to validate these findings, and further study is on-going in early MS populations.
LM inflammation in MS
Pathologically, LM inflammation is frequently observed in both early and late stages of multiple sclerosis, but difficult to visualize in vivo utilizing conventional post-contrast T1-weighted MRI sequences. Recently, post-contrast FLAIR sequences have demonstrated significantly increased sensitivity to LM enhancement (LME) in a number of neurological disease states, including stroke and various other neuroimmunological disorders 16 [e-6].
There has been variability in the reported prevalence of LME, with prevalence rates ranging from 1% to 90%.17–20 Differences in MS patient demographics and technical factors likely account for the wide variability observed, such as dose of gadolinium utilized and wash-in times, magnet strength, and sequence utilized. One early study found in a cohort of 229 MS patients that LME occurs frequently (seen in 74 of 299 cases) is seen more commonly in progressive versus relapsing MS and is associated with increasing clinical disability. 17 Pathologically, LME was found to be associated with perivascular lymphocytic and mononuclear infiltration with flanking subpial cortical demyelination, suggesting that this finding may be a useful in vivo marker of cortical pathology, which has thus far been difficult to visualize even on high-field MRI. More recent studies have demonstrated a high prevalence of LME (50%–90%) using high-field platforms (7T)19,20 and that LME is associated with accelerated gray matter atrophy and greater disability. 20 In addition, SPMS had a higher likelihood of having multiple LME foci in comparison to relapsing-remitting MS (86% vs 18%). A recent study 20 found an association of LME and focal cortical thinning, but mainly in relapsing-remitting MS. 21 Two recent studies on 7T MRI platforms showed conflicting relationships of LME presence and cortical lesions. One study demonstrated strong relationships between the presence of cortical lesions and LME, while the other study did not observe such a relationship.22,23 Although a number of studies demonstrate the clinical significance of LME, the conflicting results observed with prevalence and relationship to other well-established MRI findings illustrate that further study is needed to clarify the significance of this finding.
Although the optimal sequences, magnet strength, and timing of gadolinium administration to detect LME in MS is still under debate, accumulating evidence suggests that this finding may be relevant to clinical disability, specifically in progressive MS variants. As a result, with further validation, LME may become a useful diagnostic tool to distinguish progressive versus relapsing MS. Moreover, if LME detectable by post-contrast FLAIR MRI is relevant to cortical pathology and evolving clinical disability, it has the potential to be a useful marker of treatment response in clinical trial and practice settings. However, given its prevalence in other neurological disease states, LME is not likely be useful in distinguishing MS 24 from other white matter disorders.
Spinal cord imaging
The spinal cord is a structure that is highly relevant to clinical disability and commonly involved across the spectrum of MS disease subtypes, but particularly in progressive MS.25,26 In clinical practice, lesion-based measures in the spinal cord on MRI are frequently used in the diagnosis of MS, as the spinal cord occupies one of the regions of the central nervous system that can demonstrate “dissemination in space” in the 2017 McDonald criteria. 2 Moreover, in PPMS, lesions in the spinal cord play a key role in the diagnosis, with the presence of two or more lesions in the spinal cord comprising one of the three criteria needed for diagnosis. Improved MRI sequences, including T1-based sequences (magnetization-prepared rapid gradient-echo (MPRAGE) and phase sensitive inversion-recovery ( PSIR)) in the cervical spinal cord, improve lesion conspicuity, which can facilitate an earlier diagnosis of MS 27 [e-7].
However, lesion-based measures have limited value in disease prediction and monitoring, as the vast majority of MS patients have lesions in the spinal cord, and correlations between lesion-based measures in the spinal cord and clinical disability are limited [e-2,8]. Advanced, quantitative MRI measures have demonstrated robust correlations with clinical disability in MS, which is an advantage over lesion-based measures,28,29 making it possible that these measures may have clinical utility in disease prediction and monitoring.
Spinal cord atrophy, particularly atrophy of the gray matter, has been shown to occur early in the disease course of MS, and to correlate strongly with clinical disability (Figure 2).26,30 In addition, there is evidence of much more pronounced atrophy in progressive versus relapsing MS 29 [e-9]. Other advanced, quantitative MRI measures, including diffusion-tensor imaging and magnetization-transfer imaging, have demonstrated increased sensitivity and specificity to underlying tissue microstructure and have demonstrated high relevance to clinical disability (Figure 2).28,29,31 Given their strong relationships with clinical disability, these tools have potential utility as diagnostic, prediction, and disease-monitoring tools in clinical practice. However, before any of these measures can be of utility in these realms, important technical considerations, such as minimizing measurement variability and establishing reference values to set appropriate cut-off thresholds must be addressed. Furthermore, for disease prediction, longitudinal relationships between these spinal cord MRI measures and clinical disability need to be established, as this information will guide how these measures can be used in disease prediction in individual patients.31,32 Longitudinal change in quantitative spinal cord MRI measures were evaluated in a recent study that followed patients for approximately 5 years. This study demonstrated that individual trajectories of change are highly relevant to disability progression over 5 years, 33 highlighting the importance of incorporating subject-specific components when analyzing quantitative MRI measures.
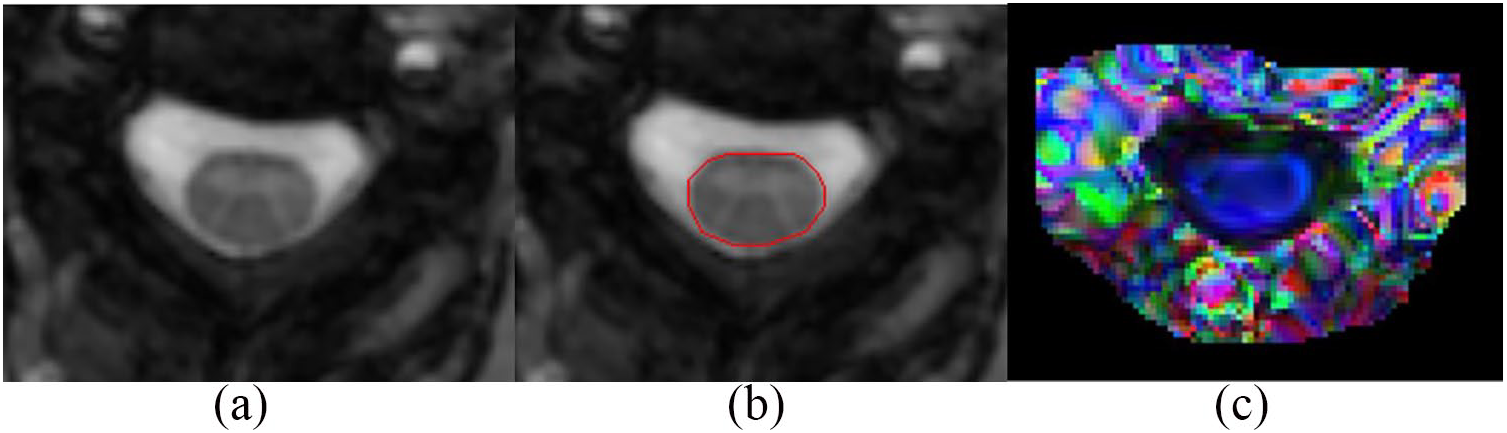
Quantitative spinal cord MRI: automated segmentation of spinal cord cross-sectional area (a, b); color-coded diffusion-tensor imaging map (c). Blue represents spinal cord tracts running in the rostrocaudal axis; green represents tracts running anteroposterior; and red represents tracts running mediolateral. This figure was reproduced with permission from Oh J, Sotirchos ES, Saidha S, et al. Relationships between quantitative spinal cord MRI and retinal layers in multiple sclerosis. Neurology 2015; 84(7): 720–728. doi: 10.1212/WNL.0000000000001257. Epub January 21 2015.
Taken together, these findings suggest that both conventional and emerging quantitative MRI measures in the spinal cord may be of utility in the diagnosis, prediction, and monitoring of patients with MS, but numerous practical issues require further work before they can be utilized in clinical practice.
Paramagnetic rims in MS
Pathologically, chronic lesions with active, “smoldering” inflammation and slow expansion are known to be an important substrate of neurological disease progression in MS [e-10]. These chronic, active lesions are seen across the spectrum of MS, but observed particularly in large proportions in progressive MS. Susceptibility-weighted imaging sequences on high-field MRI platforms (7T) are sensitive to iron content in tissue, and persistent “paramagnetic rims” around lesions has been histopathologically validated to represent chronic inflammatory infiltration related to macrophages and microglia, as well as on-going demyelination. Using a 7T platform, one pivotal study demonstrated that approximately 50% of acute MS lesions evolve to harbor persistent paramagnetic rims, and that these lesions fail to regress, and gradually lose T1-signal over time, suggesting that they represent areas of irreversible and on-going tissue damage. 34 Moreover, individuals with a high proportion of paramagnetic rims are much more likely to have clinical disability and progressive disease [e-11]. These findings suggest that the presence of a large proportion of paramagnetic rims in MS may be useful as a diagnostic tool for progressive MS, and that these may be of utility in disease prediction and monitoring across the spectrum of MS.
Detection of paramagnetic rims is now feasible on 3T platforms, and preliminary studies suggest that there may be predictive value in the detection of paramagnetic rims, even in the earliest stages of MS. A recent study demonstrated that in radiologically isolated syndrome (RIS), the majority of subjects have lesions that demonstrate the “paramagnetic rim sign” (PRS). Furthermore, there were strong correlations observed between PRS + lesions and spinal cord lesions, which is a known risk factor for conversion of RIS to MS, suggesting that there may be predictive value of detecting PRS + lesions across the spectrum of MS. 35
Although the optimal sequences, post-acquisition processing, and analysis methods need further study and validation, these observations suggest that detecting PRS + lesions may be useful in the diagnosis of progressive MS, may have predictive value in early MS, and may be useful to monitor disease progression across the spectrum of MS.
Ultra-high field MRI techniques
Ultra-high-field MRI platforms, including 7T MRI platforms, allow for increased spatial resolution in comparison to lower-field platforms, enabling improved visualization of anatomic detail of brain and spinal cord tissue in various neurological disorders [e-12]. In MS, high-field MRI has been utilized in a variety of applications, with the most common being in the identification and characterization of cortical lesions, which have been much more difficult to visualize on lower-field platforms.
Cortical lesions are well-known to be present across the spectrum of MS and strongly correlated with clinical disability progression.36,37 In the 2017 revisions of the McDonald criteria, 2 cortical lesions now occupy a region that constitutes “dissemination in space,” making the identification of cortical lesions of potential utility from a diagnostic standpoint. Cortical lesions are observed commonly, even in early MS, and there are different cortical lesion morphologies that can be discernable on high-field platforms, 38 which may correspond to Type I–III lesions that have been described histopathologically [e-13]. Using quantitative T2* relaxation rates, one study demonstrated gradients of tissue perturbance in early versus late stages of MS, further supporting the role of subpial demyelination in mediating clinical disability in MS. 39
High-field MRI platforms also allow for improved visualization of acute and chronic MS lesions. Utilizing these techniques, it is evident that lesions can demonstrate differential patterns of gadolinium contrast enhancement at lesion formation (centripetal or centrifugal), and this pattern is relevant to the “fate” of such lesions. Specifically, the pattern of contrast enhancement seen with lesions demonstrating centripetal enhancement (outside-in pattern of enhancement) seems related to acute blood–brain barrier opening and the inflammatory edge of acutely evolving lesions. With contrast enhancement resolution,34,40 a proportion of these initially centripetally enhancing lesions develop persistent paramagnetic rims around lesions, which are suggestive of failure of repair mechanisms, and on-going neurodegeneration, which has obvious clinical implications. As such, evaluating contrast enhancement patterns of acute lesion formation may be useful in the prediction of MS disease course and disease monitoring. Further study will be useful in this regard.
Given the role of cortical lesions in early and late MS pathology and its relationship to clinical disability, it is likely that high-field platforms may become useful in the diagnosis, prediction, and monitoring of people living with MS. Furthermore, the pattern of contrast enhancement visualized on 7T platforms in acute lesions may also have predictive value. However, availability and technical considerations preclude widespread use of high-field platforms and related techniques at the current time.
Conclusion
There are a number of challenges in MS clinical practice, including the limitations of conventional MRI techniques in the diagnosis, subtyping, predicting disease course, and monitoring of people living with MS. A number of emerging imaging techniques are promising to address some of these limitations, and this article summarizes select techniques of relevance.
However, before any of these emerging MRI techniques can be implemented in clinical practice, a number of technical issues, including time, resources, measurement variability, and appropriate reference values which will guide cut-off thresholds, need to be determined. With further study and validation, it is likely that many of these techniques will be incorporated into clinical care in the upcoming years, which will enable improved management and treatment optimization of people living with MS.
Supplemental Material
MSJ871817_supplemental_references – Supplemental material for New imaging approaches for precision diagnosis and disease staging of MS?
Supplemental material, MSJ871817_supplemental_references for New imaging approaches for precision diagnosis and disease staging of MS? by Jiwon Oh and Nancy L Sicotte in Multiple Sclerosis Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr J.O. has no relevant financial disclosures and Dr N.L.S. has no relevant financial disclosures.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr J.O. has received funding from the MS Society of Canada and the National MS Society for studies described in this manuscript. Dr N.L.S. has received funding from the National MS Society and PCORI.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.