
Abstract
Background:
Persons with multiple sclerosis (PwMS) are disproportionately burdened by depression compared to the general population. While several factors associated with depression and depression severity in PwMS have been identified, a prediction model for depression risk has not been developed. In addition, it is unknown if depression-related genetic variants, including Apolipoprotein E (APOE), would be informative for predicting depression in PwMS.
Objective:
To develop a depression prediction model for PwMS who did not have a history of depression prior MS onset.
Methods:
The study population included 917 non-Hispanic white PwMS. An optimized multivariable Cox proportional hazards model for time to depression was generated using non-genetic variables, to which APOE and a depression-related genetic risk score were included.
Results:
Having a mother who had a history of depression, having obstructive pulmonary disease, obesity and other physical disorders at MS onset, and affect-related symptoms at MS onset predicted depression risk (hazards ratios (HRs): 1.6–2.3). Genetic variables improved the prediction model’s performance. APOE ε4/ε4 and ε2/x conferred increased (HR = 2.5, p = 0.026) and decreased (HR = 0.65, p = 0.046) depression risk, respectively.
Conclusion:
We present a prediction model aligned with The Precision Medicine Initiative, which integrates genetic and non-genetic predictors to inform depression risk stratification after MS onset.
Introduction
Depression is one of the most prevalent psychiatric disorders in the United States, and it is more common in individuals afflicted with chronic diseases and has been linked to increased risk of mortality when coupled with other chronic disorders. 1 Depression is also exceptionally prevalent among persons with multiple sclerosis (PwMS), with a 50% lifetime risk which is higher than the general population and the majority of other chronic diseases.2,3 In PwMS, untreated and undiagnosed depression may be common, resulting in poorer quality of life, diminished treatment compliance, and poorer prognosis.4–6 In addition, increased depression symptom severity has been also associated with greater physical impairments.7,8 Therefore, improved methods and tools for identifying PwMS at risk for depression after onset would play a valuable role in early risk stratification and the optimization of MS care and depression monitoring.
To date, various risk factors for depression in PwMS have been identified, including several medical and psychiatric conditions, increased central nervous system inflammation, and possibly pathomorphological changes in the brain. 9 However, constructing prediction models for clinical utility, such as to improve screening for depression-related phenotypes in PwMS, have not been examined. In addition, several genetic variants confer risk for depression-related phenotypes, including Apolipoprotein E (APOE) ε4 and ε2 alleles conferring increased and decreased depression risk, respectively.10–13 Interestingly, in 101 PwMS, APOE ε2 demonstrated a similar protective effect against depression. 14 No other study has since assessed this relationship, nor evaluated the utility of genetic variables for depression risk assessment in PwMS.
In this study, we aim to develop a depression prediction model comprised of non-genetic factors measurable at MS diagnosis that specifically considers genetic factors, to predict depression risk in PwMS who did not have a history of depression prior MS onset. We also present a nomogram to guide depression risk stratification of PwMS, aligned with The Precision Medicine Initiative, to help identify those who may benefit from regular depression screening and monitoring considering no prior history of depression before MS onset. 15
Methods
Study population
The study population consisted of non-Hispanic white PwMS who participated in Accelerated Cure Project (ACP) for MS, provided informed consent, and reported their first symptom suggestive of MS at/after the age of 18 years. ACP is a cross-sectional, open-access database with detailed epidemiologic data from PwMS—the inclusion and exclusion criteria have been previously described. 16 In short, PwMS were recruited from the communities surrounding 10 MS specialty centers across the United States (Barrow Neurological Institute, Beth Israel Deaconess Medical Center, Johns Hopkins School of Medicine, Ohio State University Medical Center, Shepherd Center Inc., Stanford University, Tisch MS Research Center of New York, University of Colorado, University of Massachusetts Medical School, and University of Texas Southwestern Medical Center). An extensive questionnaire administered by a neurologists or trained ACP staff collected detailed medical histories and other epidemiologic information. There were 970 PwMS who reported no history of depression prior their onset of MS, of whom 919 (94.5%) PwMS had genotypic data after quality control (Supplementary Methods).17,18
Non-genetic predictors
The non-genetic baseline predictors of interest were self-reported, and included sex, birth year, age of MS onset, age of MS diagnosis, MS subtype at onset, symptoms experienced at onset (motor, cerebellar, spasticity, optic nerve, facial-motor, facial-sensory, general sensory, brainstem/bulbar, cognitive, sexual, bladder/bowel, affect, and fatigue, as previously described), 18 years of education, family history of depression among first degree (mother, father, sibling, child) and other relatives (mother’s and father’s side), family history of MS, family history of other autoimmune diseases, ever smoker, smoking status within the 5 years prior MS onset (since the risk conferred by tobacco smoke attenuates after 5–10 years from quitting), 19 and histories of the following conditions at MS onset: infectious mononucleosis, obesity, chronic obstructive pulmonary disease (COPD), hypercholesterolemia, hypertension, heart disease, type II diabetes, any cardiometabolic condition, cancer, other neurological disorders, physical disorders, other autoimmune diseases, and other non-depression psychological conditions (see Supplementary Methods).
Genetic predictors
Tagging variants for two prominent MS risk variants were available: HLA-A*02:01 (rs2975033T) and HLA-DRB1*15:01 (rs3135388A). The APOE genotypes were assigned based on genotypes for rs429358 and rs7412. An indicator variable was constructed to capture ε4/ε4, ε2/x (carriers), and other allelic combinations as the reference category. We also constructed a depression-related genetic risk score (GRS) for 875 PwMS with complete data for 30 single nucleotide polymorphisms (SNPs; Supplementary Methods).12,13
Statistical analyses
The distributions of all predictors were compared between PwMS who were never depressed prior MS onset but reported a subsequent history of depression to those who remained never depressed. Nonparametric Wilcoxon–Mann–Whitney tests were used for continuous predictors, and Pearson’s chi-square tests were used for all categorical predictors, except for those with counts ⩽5 where Fisher’s exact tests were used instead.
Creating an optimized baseline model
Considering the large number of non-genetic predictors with variable underlying correlations, it was important to implement a variable selection method prior to conducting multivariable Cox proportional hazard (time-to-depression) models. Using R v3.5, we compared the performance of five variable selection methods: (1) both-direction, (2) forward, and (3) backward stepwise regression, all using Akaike information criterion (AIC) rather than a p-value threshold; (4) Least Absolute Shrinkage and Selection Operator (LASSO) regression with 20-fold cross-validation; and (5) a stochastic genetic algorithm ranked by AIC (R package glmulti). 20 Each method was applied to the full data to construct candidate baseline models of selected non-genetic predictors. The discrimination capacity of the models was estimated using optimism-corrected C-indexes from a 150-replication bootstrap resampling validation method. The calibration of the models was measured by comparing predicted versus actual probability of depression at two time points (occurring within 10 and 20 years of MS onset) using the optimism-corrected mean absolute error generated from a 40-time resampled bootstrap method. We then added the genetic predictors that were marginally associated (p < 0.10) with time-to-depression to the candidate model of non-genetic predictors that maximized discrimination and minimized mean absolute error (calibration) to determine whether the genetic predictors improved discrimination and calibration, and therefore warranted investigation.
Survival analyses
Multivariable Cox proportional hazards models were conducted for the candidate model that had the best discrimination and calibration using the stcox function as implemented in STATA v13.1 (StataCorp, College Station, TX). Not all variables in the model were statistically significant; therefore, nested models were compared using likelihood ratio tests to determine the most parsimonious combination of genetic and non-genetic predictors for survival analyses. Variables were excluded if their exclusion resulted in a comparative likelihood ratio test p > 0.10. After the removal of non-informative variables, there was sporadic missing values (<1.2%) for a few of the retained non-genetic predictors in the final model. We considered the inclusion of indicator variables to capture the missing observations; however, results did not vary (data not shown); therefore, we report results for the less parameterized models based on 901 PwMS with non-missing data across the final subset of predictors.
Three outcomes were assessed: depression at any point after the onset of MS, depression within 10 years of MS onset, and depression within 20 years of MS onset. These time-to-event outcomes were defined as the time difference between age of first symptoms suggestive of MS and age of first occurrence of depression. Since the proportional hazards model assumes a continuous hazard function, we used the exact partial-likelihood method to handle tied failures. The proportionality assumption for the models and predictors were assessed using scaled Schoenfeld residuals (stphtest function). The goodness-of-fit of the final model was assessed using the Gronnesby and Borgan test and Arjas like plots of the Martingale residuals (stcoxgof function). Variation explained by the final model was based on a Royston’s modification Nagelkerke’s R2 statistic (str2ph function). 21 A nomogram was constructed to visualize how the weights of the predictors in the final model could be used to assess depression risk in PwMS in 10 and 20 years after MS onset (nomocox function). 22 A two-sided alpha level of 0.05 was used for all definitions of statistical significance.
Ethical approval
This study was approved by the Case Western Reserve University Institutional Review Board (Protocol Number: IRB-2016-1583).
Results
Study population
The study population included 917 PwMS who were never depressed prior MS onset, of whom 184 (20.1%) subjects subsequently reported a history of depression with 61.4% and 85.9% experiencing depression within 10 and 20 years after MS onset, respectively (Table 1). Those with a history of depression were older at study interview, had an earlier age of MS onset, had a longer disease duration of MS, had a lower education, and more likely to be ever smokers compared to those who were never depressed. The two groups did not differ by sex or MS subtype, nor by their family histories of MS or other autoimmune disorders. PwMS with a history of depression compared to never depressed PwMS reported a higher burden of depression among their mothers (26.6% vs 15.4%), siblings (28.3% vs 13.1%), and children/grandchildren (6.5% vs 1.9%), but not their fathers or extended relatives. They were also more likely to report a history of obesity (8.7% vs 4.7%) and COPD (10.9% vs 4.5%) at MS onset compared to never depressed PwMS. There were also slight differences in the prevalence of reporting facial-motor and sensory impairments at MS onset between those with subsequent depression and those who were never depressed. The distribution of APOE differed between the groups with 3.8% and 1% of PwMS with ε4/ε4 and 14.7% and 20.6% of PwMS with ε2/x genotypes between the depressed and never-depressed groups, respectively. Also, differing between the two groups was the distribution of HLA-A*02:01 (p = 0.022), with a suggestive difference for the depression GRS (p = 0.097), and no difference in HLA-DRB1*15:01 genotypes (p = 0.82).
Distribution of socio-demographic, lifestyle/behavioral, and health-related characteristics in PwMS who were depression naïve at MS onset. a
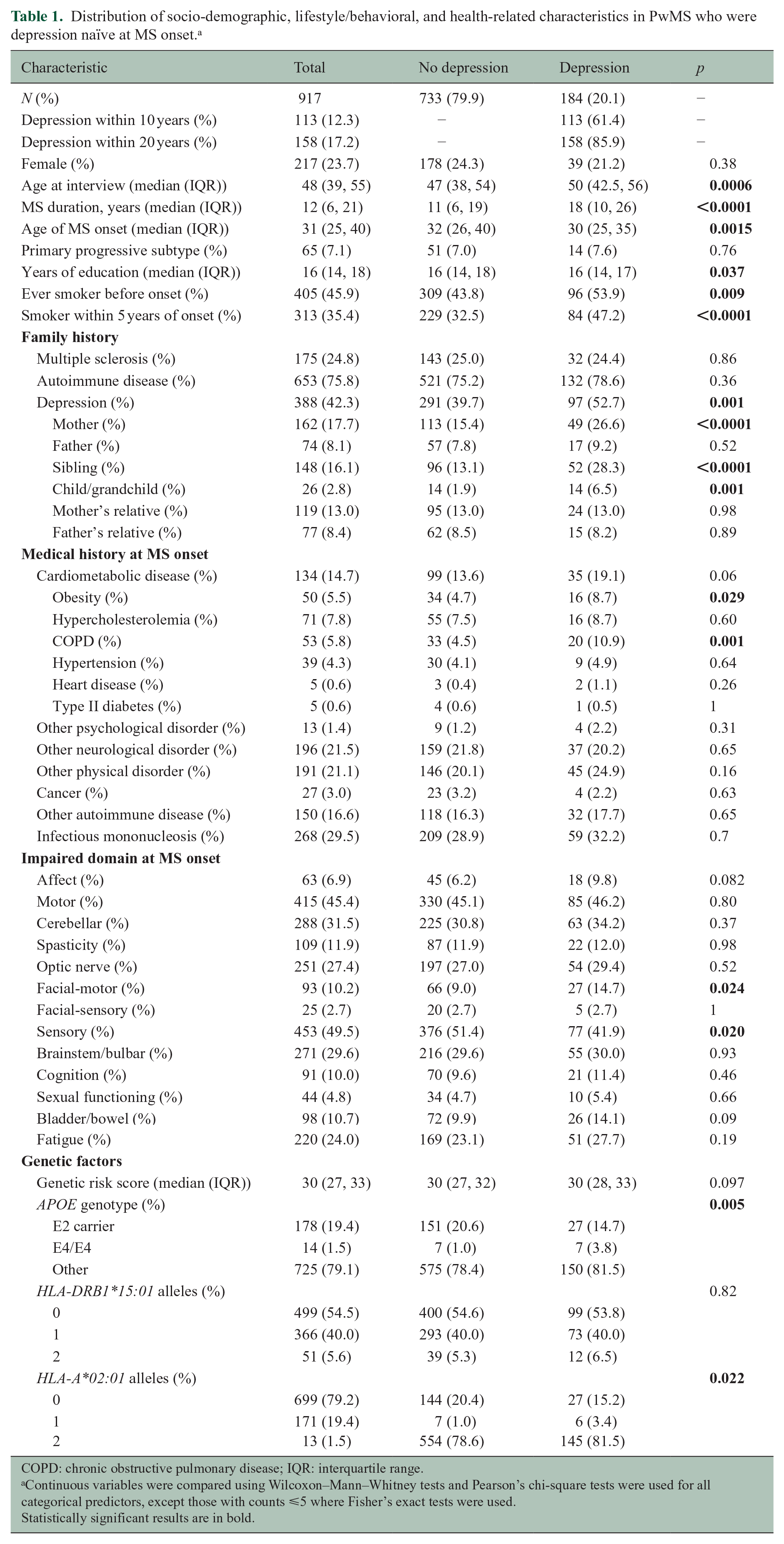
COPD: chronic obstructive pulmonary disease; IQR: interquartile range.
Continuous variables were compared using Wilcoxon–Mann–Whitney tests and Pearson’s chi-square tests were used for all categorical predictors, except those with counts ⩽5 where Fisher’s exact tests were used.
Statistically significant results are in bold.
Model selection
Of the five model selection methods, the both-direction stepwise, backward stepwise, and genetic algorithm yielded the same prediction model of non-genetic variables with the best performance; this was based on their respective cross-validated maximized discrimination and minimized calibration estimates (Supplementary Table 1). This best model consisted of nine predictors. Nonlinear and interaction terms were considered, and as a sensitivity analysis, the model selection methods generated candidate models for depression within 5, 10, 15, and 20 years separately, but there was no significant improvement over the original model (data not shown). To this non-genetic model of nine predictors, we added the depression-related GRS and APOE, since they were marginally associated with depression in univariate Cox proportional hazards models (p < 0.1; Supplementary Table 2). The inclusion of these genetic variables improved model performance (Supplementary Table 1) and were therefore retained in the base model. Not all predictors in the base model were significantly associated with depression; therefore, nested models were compared across PwMS with complete data (Supplementary Table 3). The final model consisted of having a mother with a history of depression; histories of other physical disorders, COPD, and obesity at MS onset; impairments in affect at MS onset; and APOE (Table 2).
Multivariable adjusted hazard ratios for depression risk at any time point, within 10 years, and within 20 years. a
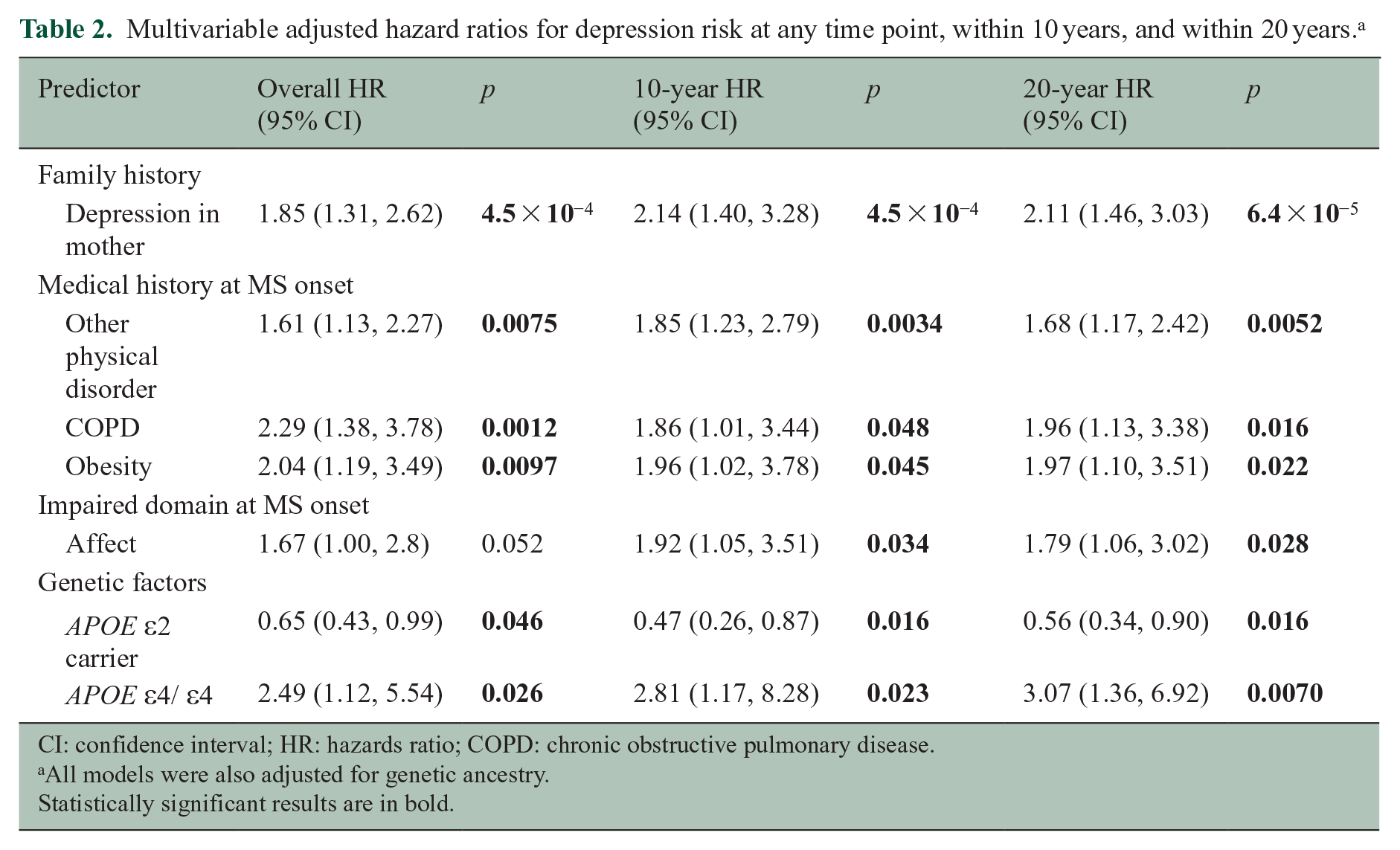
CI: confidence interval; HR: hazards ratio; COPD: chronic obstructive pulmonary disease.
All models were also adjusted for genetic ancestry.
Statistically significant results are in bold.
Survival analyses
The predictor with the strongest magnitude of effect was APOE ε4/ε4, consistently conferring increased risk of depression compared to the reference genotypes (ε3/ε3 and ε3/ε4) across time points (hazards ratio (HR): 2.49, 95% confidence interval (CI): 1.12, 5.54; p = 0.026; HR10year: 2.81, 95% CI: 1.17, 8.28; p = 0.023; HR20year: 3.07, 95% CI: 1.36, 6.92; p = 0.007) (Table 2). Interestingly, ε2 carrier status significantly decreased the risk of depression compared to the reference genotypes (HR: 0.65, 95% CI: 0.43, 0.99; p = 0.046; HR10year: 0.47, 95% CI: 0.26, 0.87; p = 0.016; HR20year: 0.56, 95% CI: 0.34, 0.90; p = 0.016). A Kaplan–Meier curve illustrates the survival function for these APOE genotype groups in Figure 1, with the step function for ε4/ε4 much lower and for ε2 carriers much higher than the reference group. All non-genetic predictors increased risk for depression by more than 60% across time points including having other physical disorders and impairments in affect at onset. A history of COPD and obesity and having a mother with a history of depression increased the risk for depression twofold (Table 2).
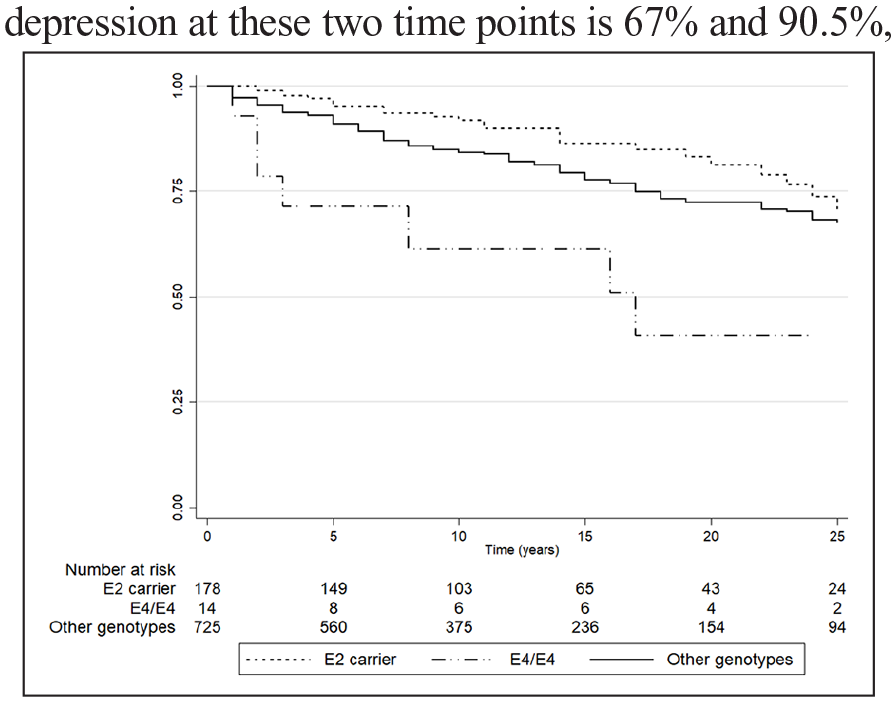
Kaplan–Meier curve for APOE genotypes.
The final model explained 16.3% of the variation in the data; it also had good fit and all predictors met proportional hazards assumptions (p > 0.05; Supplementary Table 4 and Supplementary Figure 1). This final model was therefore used to generate a nomogram (Figure 2). The probability of surviving depression-free for an average PwMS who was never depressed prior MS onset but had a APOE ε4/ε4 genotype (10 points), a history of obesity at MS onset (5 points), and a mother with a history of depression (4.5 points) is 33% and 9.5% at year 10 and 20, respectively; thus, the risk of depression at these two time points is 67% and 90.5%, respectively.
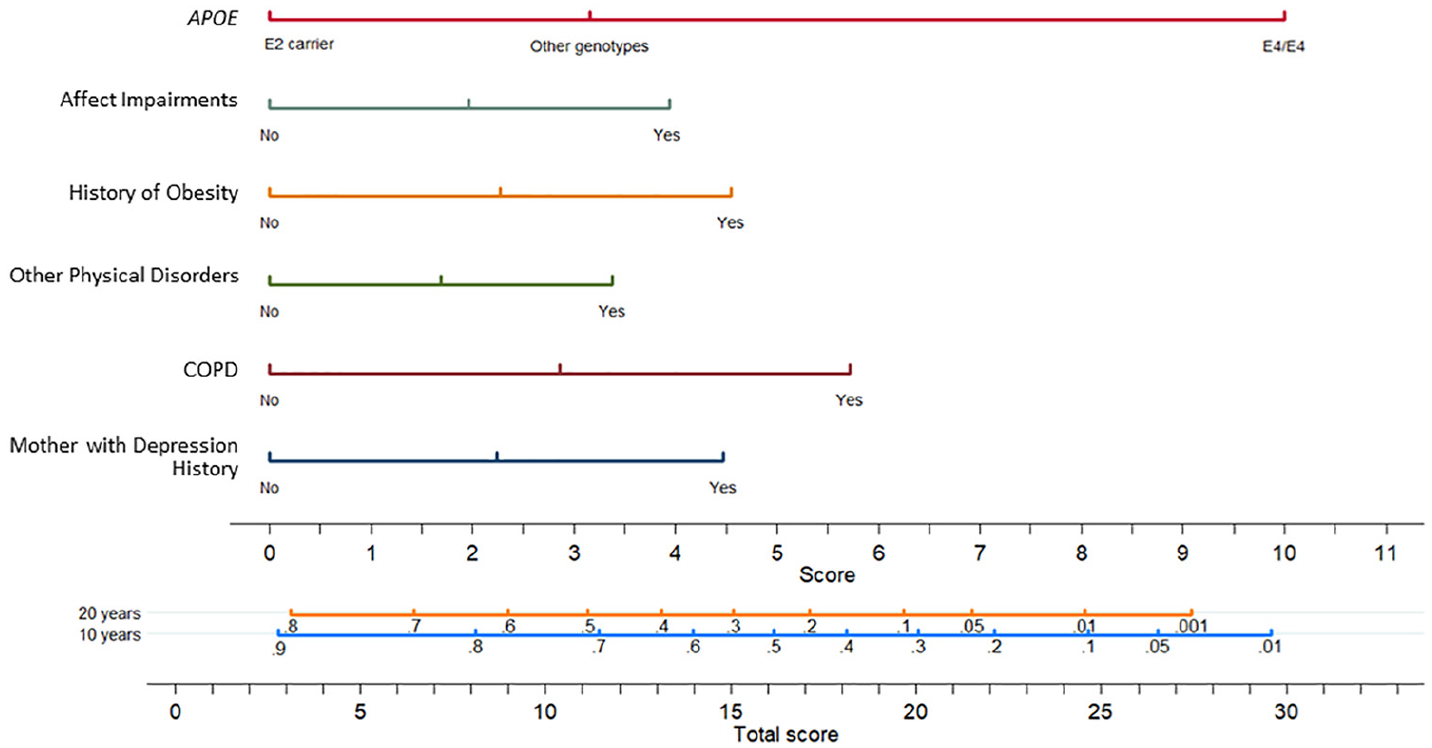
A nomogram for depression risk after MS onset for PwMS who were depression-naïve at MS onset, illustrating the probability of depression-free survival at year 10 and 20. The points assigned to the value for each predictor is determined by their value on the score line. Points are then added across predictors to generate the total score which is then compared to the probability of surviving depression-free for years 10 and 20. For example, for a PwMS with only APOE ε4/ε4, their score is 10 points; therefore, the probability of remaining depression-free at year 10 is ~75% and at year 20 is ~55%.
Discussion
Depression is the most common co-occurring psychiatric condition in PwMS, 9 and severely contributes to adverse outcomes, with depression or increased depression symptom severity resulting in poorer adherence to treatment, diminished quality of life, and accelerated accrual of physical impairments.5–8 In an era where genomic health research is ever-expanding, discerning a role for how genetic knowledge can be incorporated with non-genetic information to improve patient assessment and outcomes is the primary objective for The Precision Medicine Initiative. 15 To align with this initiative, we here present a framework by which genetic predictors can be integrated with easy to measure non-genetic predictors to advance risk stratification for PwMS who were never depressed prior MS onset. The inclusion of genetic factors resulted in a prediction model with improved performance. In fact, the strongest predictor of depression was the APOE ε4/ε4 genotype. We also replicated the protective effect of APOE ε2/X genotypes on depression risk in PwMS. Our results also highlighted the importance of considering comorbid health at MS onset, specifically COPD, obesity, and other physical disorders. Collectively, the prediction model allowed us to develop a nomograph for predicting depression risk, which has the potential to significantly mitigate adverse depression-related outcomes in PwMS by identifying those with higher depression risk much earlier in their disease course.
APOE alleles are complexly associated with several neurological, cardiometabolic, and other chronic conditions, most prominently with Alzheimer’s Disease, but they are not associated with MS risk or severity.23–26 It is the most abundant apolipoprotein in the brain, primarily expressed in astrocytes and expressed at lower levels in oligodendrocytes and other cell types, with extensive involvement in normal brain functioning that is modulated by genetic variation. 25 Interestingly, APOE ε4, the predominant Alzheimer’s Disease risk allele, is associated with decreased white myelin water fraction and gray matter volume in infants, which are also brain pathomorphological changes that occur early in the MS disease course—however, it is unclear if APOE is associated with these features in MS.27–29 Similar morphological changes have been observed in specific brain tissues in depression-related phenotypes, including among PwMS. 9 A meta-analysis of seven non-Hispanic white studies demonstrated that ε2 alleles conferred a protective effect, while ε4 alleles conferred an increased risk for depression-related phenotypes. 10 In a modest sample size of 101 PwMS, a similar significant effect was observed for ε2 carriers, and a non-significant association for ε4 carriers. 14 No prior study of PwMS has specifically tested the association between ε4/ε4 and depression; thus, here we report for the first time a very strong effect for this low frequency genotype (1.5% in this population). We are also the first study to test and replicate the protective association for ε2 alleles and depression risk in PwMS. Considering the nuanced relationships among cognitive decline, depression, and APOE, as well as their associations with morphological features, there is no clear pathophysiological mechanism that currently explains the pronounced APOE-depression associations we have observed in PwMS, and therefore this relationship warrants further attention.
Other predictors capturing other aspects of the heritable component of depression were also associated with depression risk in PwMS. Having a mother with a history of depression had a strong effect on depression risk in PwMS in our study, which is consistent with results from a study of the general population. 30 In MS, there have been four modestly size studies (N < 150) that reported conflicting associations for a family history of depression and depression risk. 31 As a result, we sought to characterize depression risk using more detailed measures of family history. Due to the likely underlying correlations among the individual measures of family history of depression in first degree and other relatives, we employed variable selection approaches to identify the most informative and independent predictors. Depression among first degree relatives, except one’s father, was more common among PwMS reporting depression after onset (Table 1). However, after employing variable selection, only having a mother with a history of depression was informative. This result suggests that adding resolution to the collection of family history of depression can provide significant insights. The other measure capturing the heritable component of depression was the depression-related GRS, which was marginally associated with depression risk in PwMS (p = 0.07). However, it was not retained in our final model which may be due to the heterogeneity in the depression-related phenotypes (i.e. broad depression, probable major depressive disorder (MDD), and MDD measured via self-reported or through diagnostic codes) used to identify the SNPs that comprised the GRS and depression self-reported by the current study participants.12,13 Nonetheless, the findings collectively demonstrate a prominent effect for aspects of the heritable component of depression on depression risk in PwMS.
Depression risk was also strongly predicted by comorbid health conditions present at the onset of MS. This is consistent with literature for the general population demonstrating that multimorbidity significantly confers increased depression risk, particularly among those with chronic conditions. 32 With respect to MS, very few studies have specifically investigated the impact of comorbid health conditions on depression and depression symptom severity. Results from longitudinal analyses of electronic medical records for 2083 PwMS, COPD, type II diabetes, and higher body mass index significantly contributed to increases in depression symptom severity.7,33 These findings are consistent with those presented with COPD and obesity at onset significantly predicting subsequent depression. We also observed a strong predictive effect for having any of the following physical disorders: osteoarthritis, osteoporosis, kidney disease, gallstones, anemia, chronic fatigue syndrome, or fibromyalgia. Thus, comorbidities at MS onset warrant closer attention, not only because they contribute to adverse outcomes, but because they can be readily obtained and can be then used to significantly inform depression risk.
We note that these predictors of depression risk in this population of PwMS are likely not MS-specific, but generally predictive of depression. This can be perceived as a strength, as we demonstrate how such factors can be highly informative for depression risk stratification in PwMS. It is also noteworthy that several characteristics were not informative for predicting depression risk despite their univariate association, including age of MS onset, education, and smoking status. However, these traits have been shown to influence depression symptom severity. 7 Also not associated with depression risk was sex, which has also been shown to influence depression symptom severity. 7 A possible reason for the lack of association for sex in the current study might be due to the operational definition of the outcome, which required subjects to have no history of depression prior the onset of MS. Interestingly, HLA risk variants, a family history for MS and other autoimmune diseases, other comorbidities (i.e. cancer), and symptomatology experienced at onset of MS were not predictive of depression risk, except for changes in their mood or depression that were out of the ordinary, which could be due to recall bias.
This study has several strengths, the first being the rare opportunity to integrate genetic and non-genetic predictors to build a novel and robust risk prediction model aligned with the goals of The Precision Medicine Initiative. The model was designed to incorporate predictors that would be measurable at MS onset and diagnosis, and therefore very early in the disease process. We demonstrate for the first time a pronounced increased risk for depression due to APOE ε4/ε4 in PwMS and were also able to replicate the prior observation that ε2/x was protective against depression. Thus, these APOE findings are novel and warrant further attention considering their strong predictive effects. We also demonstrated a prominent effect for a mother’s history of depression and comorbid health conditions, both which could be readily measured in PwMS. Our final strength is the inclusion of a nomogram that can be used to easily identify patients who would benefit from regular depression screening. We must also acknowledge that the primary limitation of this study was that the non-genetic variables were based on self-reported responses to a questionnaire administered by a neurologist or trained research staff, and therefore prone to recall and measurement error biases. However, a validation study of self-reported comorbidity in 400 MS patients demonstrated moderate or better levels of agreement with medical records for depression, chronic lung disease, hypertension, and other common physical and mental comorbidities. 34 Nonetheless, we would assume biases introduced by self-report would result in non-differential misclassification of the exposures and outcome, which would bias the associations toward the null for binary measures. Furthermore, considering the strong magnitude of associations, it is unlikely that unmeasured confounding could explain all the observed risk.
In conclusion, we present the first predictive model to inform risk stratification in PwMS that integrates genetic and non-genetic predictors. It is important to identify PwMS at risk for depression considering its pervasive negative impact on outcomes in PwMS. The results add novel resolution to the association for APOE on depression risk, as well as the utility of a more detailed family history of depression and comorbid health on depression risk prediction. Our final prediction model is based on APOE genotypes and readily measurable non-genetic characteristics, and therefore could be promptly used to improve risk stratification and case identification of depression in PwMS.
Supplemental Material
MSJ921073_Supplementary_Figure_1 – Supplemental material for Predicting self-reported depression after the onset of multiple sclerosis using genetic and non-genetic factors
Supplemental material, MSJ921073_Supplementary_Figure_1 for Predicting self-reported depression after the onset of multiple sclerosis using genetic and non-genetic factors by Frances M Wang, Mary F Davis and Farren BS Briggs in Multiple Sclerosis Journal
Supplemental Material
MSJ921073_Supplementary_Methods – Supplemental material for Predicting self-reported depression after the onset of multiple sclerosis using genetic and non-genetic factors
Supplemental material, MSJ921073_Supplementary_Methods for Predicting self-reported depression after the onset of multiple sclerosis using genetic and non-genetic factors by Frances M Wang, Mary F Davis and Farren BS Briggs in Multiple Sclerosis Journal
Supplemental Material
MSJ921073_Supplementary_Tables – Supplemental material for Predicting self-reported depression after the onset of multiple sclerosis using genetic and non-genetic factors
Supplemental material, MSJ921073_Supplementary_Tables for Predicting self-reported depression after the onset of multiple sclerosis using genetic and non-genetic factors by Frances M Wang, Mary F Davis and Farren BS Briggs in Multiple Sclerosis Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.