
Abstract
During PREVENT (a phase 3, randomized, double-blind, placebo-controlled, time-to-event study) and its open-label extension (interim analysis), 33 adults with aquaporin-4 immunoglobulin G-positive neuromyelitis optica spectrum disorder (AQP4-IgG + NMOSD) received eculizumab monotherapy for a median of 2.8 years (range, 14 weeks–5.2 years). At 192 weeks (~4 years), 96% of these patients were free from adjudicated relapses (Kaplan–Meier analysis; 95% confidence interval, 75.7–99.4). During PREVENT, 95% (20/21) of patients receiving eculizumab monotherapy had no disability worsening. Eculizumab monotherapy provides effective long-term relapse prevention, relieving the chronic immunosuppression burden in patients with AQP4-IgG + NMOSD. ClinicalTrials.gov; PREVENT: NCT01892345; open-label extension: NCT02003144.
Introduction
Aquaporin-4 immunoglobulin G-positive neuromyelitis optica spectrum disorder (AQP4-IgG + NMOSD) is an autoimmune central nervous system disorder characterized by relapses leading to accumulating disability. 1 Adverse events (AEs) of chronic immunosuppressive therapy (IST) may limit its tolerability and effectiveness in NMOSD.
Eculizumab, a humanized monoclonal antibody targeting terminal complement protein C5, was the first approved treatment for AQP4-IgG + NMOSD. 2 In PREVENT, a phase 3, randomized, double-blind, placebo-controlled, time-to-event study (NCT01892345), eculizumab significantly reduced relapse risk versus placebo (adjudicated relapses: 3.1% vs 42.6% of patients; hazard ratio: 0.058; 95% confidence interval (CI): 0.017–0.197; p < 0.0001).3,4 Eculizumab was well tolerated, with a safety profile consistent with that in other indications.3,5–8
Although permitted, 34 of 143 PREVENT participants received no concomitant IST. 3 All patients receiving eculizumab monotherapy remained relapse-free at week 96, versus 40% receiving placebo alone. 3 This report describes eculizumab monotherapy’s long-term efficacy in AQP4-IgG + NMOSD during PREVENT and its open-label extension (OLE; interim analysis; NCT02003144).
Methods
PREVENT’s methodology has been published previously. 3 Briefly: 143 adults were randomized (2:1) to eculizumab (intravenous maintenance dosage, 1200 mg/2 weeks) or placebo; stable-dose IST was permitted (excluding rituximab and mitoxantrone); patients were vaccinated against Neisseria meningitidis. 3 The primary endpoint was time to first adjudicated relapse; PREVENT ended after 23 adjudicated relapses. 3 In total, 119 patients (eculizumab/eculizumab, 78; placebo/eculizumab, 41) received maintenance-dosage eculizumab in the OLE, with concomitant IST at physician discretion.
We report data from a post hoc analysis (PREVENT and interim OLE: data cutoff, 31 July 2019) of a prespecified subgroup receiving eculizumab monotherapy or placebo alone (no concomitant IST) throughout PREVENT and/or the OLE.
PREVENT/OLE were approved by institutional review boards of participating institutions. All study participants provided written informed consent.
Results
Patients
Patient disposition during PREVENT and the OLE is shown in Supplemental Figure S1. In PREVENT, 34 patients received no concomitant IST (eculizumab, 21; placebo, 13); 15 and 12 patients, respectively, entered the OLE. Thirty-three patients receiving eculizumab monotherapy (PREVENT + OLE, 15; PREVENT only, 6; OLE only, 12; Figure 1(a)) were followed up for 87.3 patient-years (PY; median, 2.9 years/patient; range, 23.1–272.1 weeks) and had 85.3 PY of treatment. Eculizumab monotherapy duration was 14.1–271.3 weeks (median, 2.8 years/patient).
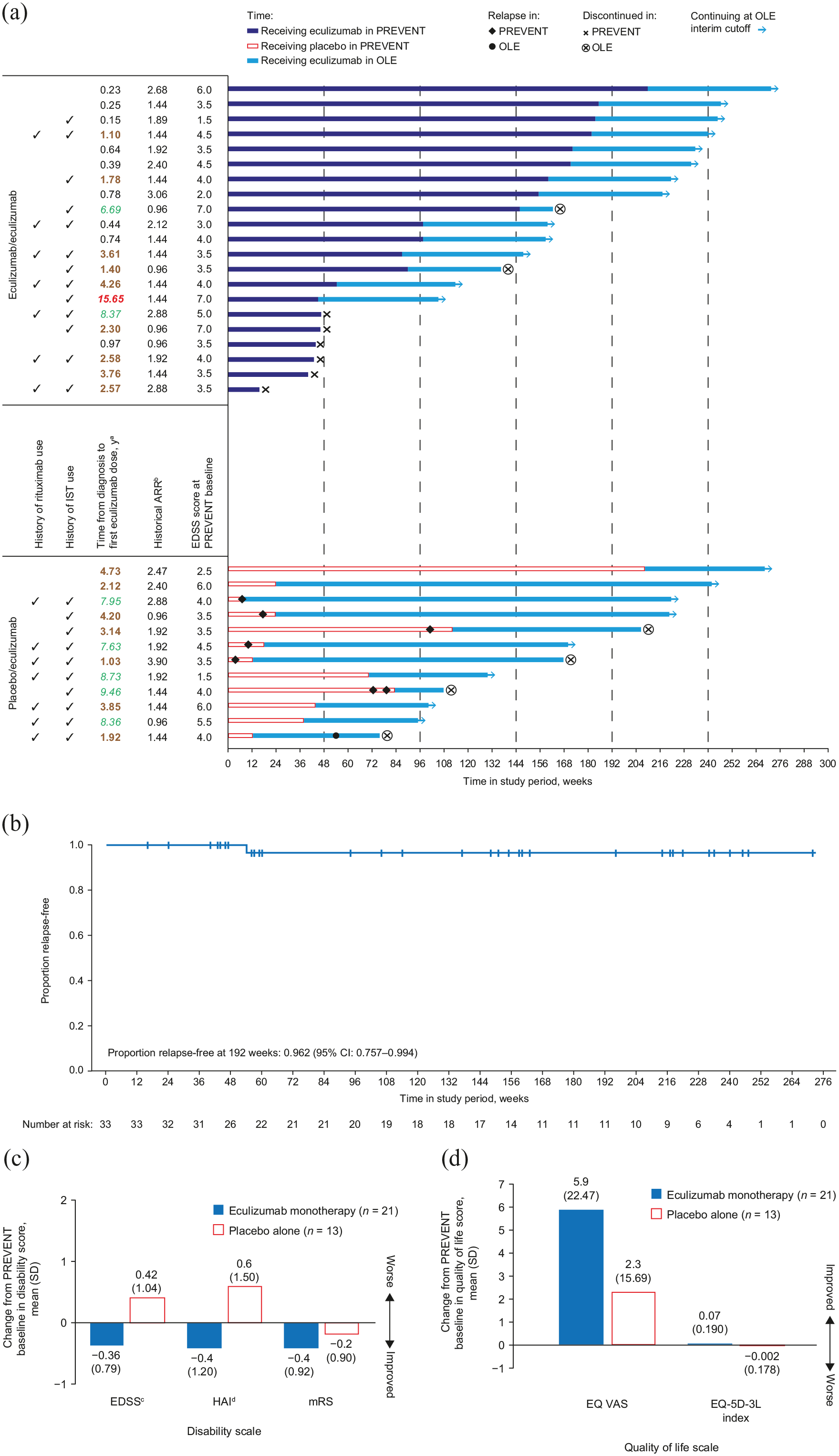
Eculizumab monotherapy efficacy outcomes in patients not using concomitant immunosuppressive therapies. (a) Clinical profiles of patients receiving eculizumab monotherapy during PREVENT and OLE (n = 33). (b) Time to first adjudicated relapse in patients receiving eculizumab monotherapy during PREVENT and OLE. (c) Changes during PREVENT in mean (SD) disability scores by treatment group. (d) Changes during PREVENT in mean (SD) quality of life scores by treatment group.
Baseline demographic characteristics and disease history for patients not using concomitant immunosuppressive therapies.
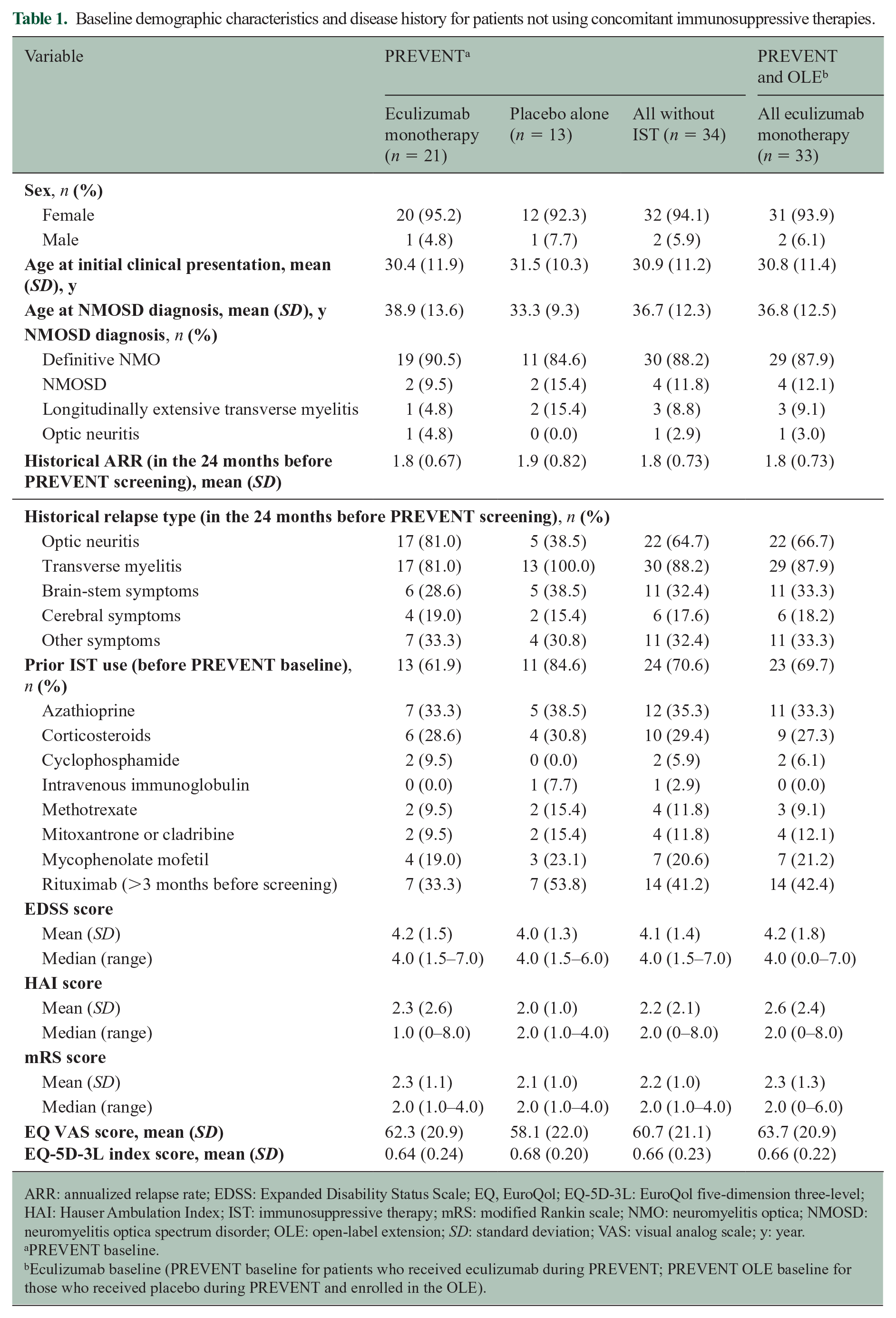
ARR: annualized relapse rate; EDSS: Expanded Disability Status Scale; EQ, EuroQol; EQ-5D-3L: EuroQol five-dimension three-level; HAI: Hauser Ambulation Index; IST: immunosuppressive therapy; mRS: modified Rankin scale; NMO: neuromyelitis optica; NMOSD: neuromyelitis optica spectrum disorder; OLE: open-label extension; SD: standard deviation; VAS: visual analog scale; y: year.
PREVENT baseline.
Eculizumab baseline (PREVENT baseline for patients who received eculizumab during PREVENT; PREVENT OLE baseline for those who received placebo during PREVENT and enrolled in the OLE).
Six patients withdrew from PREVENT, and six discontinued the OLE (Supplemental Table S1). At interim data cutoff, 63.6% (21/33) continued to receive monotherapy. Most (69.7%; 23/33) had previously used IST (ceasing 28.9 weeks (median; range, 3.0–707.1 weeks) before PREVENT), and 42.4% (14/33) had previously used rituximab (median, 33.8 weeks (range, 19.6–129.4 weeks) from last dose to PREVENT start). Baseline characteristics are summarized in Table 1.
Relapses during PREVENT and the OLE
One of 33 patients receiving eculizumab monotherapy experienced an adjudicated relapse (major myelitis (Supplemental Methods), optic spinal impairment scale motor subscale score increase from 1 to 3) after 380 days in the OLE (and 75 days of placebo alone in PREVENT). The adjudicated annualized relapse rate for this group was 0.012 (95% CI: 0.002–0.082) versus 0.625 (95% CI: 0.313–1.250) for the PREVENT placebo alone group (n = 13). At 192 weeks of eculizumab monotherapy, 96.2% of patients were free from adjudicated relapses (cumulative probability estimate from Kaplan–Meier analysis, 0.962; 95% CI: 0.757–0.994; Figure 1(b)). Clinical profiles of these 33 patients are summarized in Figure 1(a). No further adjudicated relapses were reported with eculizumab monotherapy through 1 June 2020.
During the OLE, 17/88 patients (19.3%) using concomitant IST at baseline stopped using IST (reasons were not recorded). No adjudicated relapses were reported for these patients during 44.3 weeks (median; range, 0.3–186.3 weeks) of subsequent eculizumab monotherapy.
Impact on measures of disability and quality of life during PREVENT
Of 34 patients receiving no concomitant IST throughout PREVENT, 1/21 (4.8%) and 5/13 (38.5%) receiving eculizumab and placebo, respectively, experienced Expanded Disability Status Scale (EDSS) score worsening by PREVENT end (increase ⩾2 from 0, ⩾1 from 1–5, or ⩾0.5 from ⩾5.5 at baseline). Similarly, 1/21 (4.8%) and 4/13 (30.8%) patients, respectively, experienced Hauser Ambulation Index (HAI) score worsening by PREVENT end (increase ⩾2 from 0, or ⩾1 from ⩾1 at baseline).
Between PREVENT baseline and end, mean EDSS and HAI scores improved with eculizumab monotherapy and deteriorated with placebo alone. There were greater improvements in mean modified Rankin scale and EuroQol visual analog scale (EQ VAS) and five-dimension three-level index (EQ-5D-3L) scores with eculizumab monotherapy versus placebo alone (Figure 1(c) and (d)). Improvements in EQ VAS and EQ-5D-3L with eculizumab monotherapy persisted through the OLE (mean (standard deviation (SD)) changes from baseline to interim analysis: 5.9 (17.82) and 0.04 (0.175), respectively).
Safety
AE and hospitalization rates during eculizumab monotherapy are shown in Supplemental Table S2. The rate of serious infections during PREVENT and the OLE was lower with eculizumab monotherapy (2.3 events/100 PY) than with placebo alone (7.8 events/100 PY). No meningococcal infections or deaths were reported with eculizumab monotherapy through 1 June 2020.
Discussion
In PREVENT, eculizumab (with/without concomitant IST) reduced relapse risk by 94%.3,4 PREVENT’s design allowed analysis of eculizumab monotherapy over a median of 2.8 years (maximum, 5.2 years) in 33 patients. Although patient numbers were limited, follow-up times ranged widely (23–272 weeks) and analyses were descriptive; these data provide evidence for eculizumab monotherapy’s long-term efficacy with a full duration that remains to be determined. At 192 weeks of eculizumab monotherapy, 96% of patients were relapse-free. During PREVENT, 95% of patients receiving eculizumab monotherapy had no disability worsening and greater quality of life improvements versus placebo alone; available data suggested that these quality of life improvements persisted during the OLE. Eculizumab monotherapy’s long-term safety profile was similar to overall safety observations during PREVENT; notably, the rate of serious infections was low. Further research and clinical reports of eculizumab monotherapy are necessary to confirm these findings.
Efficacy data for other novel therapies without concomitant ISTs in AQP4-IgG + NMOSD have been published, and further data are needed for comparison because of study differences in patients and relapse definitions. In summary, relapse risk reductions in patients with AQP4-IgG + NMOSD have been reported for satralizumab monotherapy versus placebo alone (83% and 55% relapse-free after 48 weeks, respectively; n = 64) 9 and inebilizumab monotherapy versus placebo alone (88% and 57% relapse-free after 28 weeks, respectively; n = 213). 10 In PREVENT, 100% and 61% of patients remained relapse-free after 48 weeks of eculizumab monotherapy and placebo alone, respectively (n = 34). 3
In conclusion, these findings provide evidence for effective long-term management of AQP4-IgG + NMOSD with eculizumab monotherapy, avoiding the use of off-label IST. This may be particularly valuable for patients at increased risk of AEs and those intolerant of IST.
Supplemental Material
sj-docx-1-msj-10.1177_13524585211038291 – Supplemental material for Eculizumab monotherapy for NMOSD: Data from PREVENT and its open-label extension
Supplemental material, sj-docx-1-msj-10.1177_13524585211038291 for Eculizumab monotherapy for NMOSD: Data from PREVENT and its open-label extension by Sean J Pittock, Kazuo Fujihara, Jacqueline Palace, Achim Berthele, Ho Jin Kim, Celia Oreja-Guevara, Ichiro Nakashima, Michael Levy, Shulian Shang, Marcus Yountz, Larisa Miller, Róisín Armstrong and Dean M Wingerchuk in Multiple Sclerosis Journal
Supplemental Material
sj-pdf-1-msj-10.1177_13524585211038291 – Supplemental material for Eculizumab monotherapy for NMOSD: Data from PREVENT and its open-label extension
Supplemental material, sj-pdf-1-msj-10.1177_13524585211038291 for Eculizumab monotherapy for NMOSD: Data from PREVENT and its open-label extension by Sean J Pittock, Kazuo Fujihara, Jacqueline Palace, Achim Berthele, Ho Jin Kim, Celia Oreja-Guevara, Ichiro Nakashima, Michael Levy, Shulian Shang, Marcus Yountz, Larisa Miller, Róisín Armstrong and Dean M Wingerchuk in Multiple Sclerosis Journal
Supplemental Material
sj-pdf-2-msj-10.1177_13524585211038291 – Supplemental material for Eculizumab monotherapy for NMOSD: Data from PREVENT and its open-label extension
Supplemental material, sj-pdf-2-msj-10.1177_13524585211038291 for Eculizumab monotherapy for NMOSD: Data from PREVENT and its open-label extension by Sean J Pittock, Kazuo Fujihara, Jacqueline Palace, Achim Berthele, Ho Jin Kim, Celia Oreja-Guevara, Ichiro Nakashima, Michael Levy, Shulian Shang, Marcus Yountz, Larisa Miller, Róisín Armstrong and Dean M Wingerchuk in Multiple Sclerosis Journal
Footnotes
Acknowledgements
The authors would like to thank all investigators and collaborators who contributed to PREVENT (those associated with this subgroup are listed in the Supplemental Materials), as well as the participating patients and their families. We thank Kenji Fujita, Guido Sabatella, Murat Terzi, Natalia Totolyan, Shanthi Viswanathan, and Kai-Chen Wang for their contributions to abstracts on earlier analyses of PREVENT monotherapy data. We also thank Amy Pace of Alexion Pharmaceuticals for statistical support and manuscript review, Cynthia Carrillo-Infante of Alexion Pharmaceuticals for reviewing safety data, and Pratap Singh and Xiang Gao of Alexion Pharmaceuticals for pharmacokinetic/pharmacodynamic analysis. We would like to acknowledge Ruth Gandolfo of Oxford PharmaGenesis, Oxford, UK, who provided medical writing assistance in the production of this manuscript (funded by Alexion Pharmaceuticals).
Author Contributions
S.J.P., S.S., L.M., and R.A. contributed to the concept and design of the study. All authors contributed to the acquisition, analysis, or interpretation of data, and to drafting/critical revision of the manuscript for important intellectual content and final approval of the manuscript. PREVENT study group members who provided and cared for study patients in this subgroup and collected data from them are listed as study collaborators in the Supplemental Materials.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: S.J.P. reports grants, personal fees, and nonfinancial support from Alexion Pharmaceuticals; grants from Autoimmune Encephalitis Alliance and Grifols; grants, personal fees, nonfinancial support, and other support from MedImmune; other support from Astellas; and personal fees from UCB. He has a patent, Patent# 8,889,102 (Application#12-678350, Neuromyelitis Optica Autoantibodies as a Marker for Neoplasia)—issued; a patent, Patent# 9,891,219B2 (Application#12-573942, Methods for Treating Neuromyelitis Optica (NMO) by Administration of Eculizumab to an individual that is Aquaporin-4 (AQP4)-IgG Autoantibody positive)—issued; a patent, GFAP-IgG—pending; a patent, Septin-5-IgG—pending; a patent, MAP1B-IgG—pending; and a patent, KLHL11—pending. K.F. reports personal fees and other support from Alexion Pharmaceuticals during the conduct of the study. Outside the submitted work, he has received personal fees and other support from Asahi Kasei Medical, Bayer, Biogen, Chugai Pharma, Eisai, Mitsubishi Tanabe Pharma, Novartis, Ono Pharmaceutical, Sumitomo Dainippon Pharma, Takeda, Teijin Pharma, and Viela Bio (formerly MedImmune); and grants from the Ministry of Education, Science and Technology of Japan and the Ministry of Health, Welfare and Labor of Japan. J.P. is partly funded by highly specialized services to run a national congenital myasthenia service and a neuromyelitis service. She has received support for scientific meetings and fees for advisory work from Abide Therapeutics, Alexion Pharmaceuticals, ARGENX, Bayer Schering, Biogen Idec, Chugai Pharma, EuroImmun, Genzyme, MedDay, MedImmune, Merck Serono, Novartis, Roche, Teva, UCB, and Viela Bio; grants from Abide Therapeutics, Alexion Pharmaceuticals, Bayer Schering, Biogen Idec, Chugai Pharma, Genzyme, MedImmune, Merck Serono, Novartis, and Teva; and grants for research studies from Eugène Devic European Network, Grant for Multiple Sclerosis Innovation, Guthy-Jackson Charitable Foundation, John Fell Fund, Medical Research Council, MS Society, Myaware, Oxford Health Services Research Committee, and UK National Institute for Health Research. A.B. reports compensation for clinical trials received by his institution from Alexion Pharmaceuticals, Biogen, Merck Serono, Novartis, Roche, Sanofi Genzyme, and Teva; and personal fees and nonfinancial support from Alexion Pharmaceuticals, Bayer, Biogen, Celgene, Merck Serono, Mylan, Novartis, Roche, and Sanofi Genzyme. H.J.K. has received a grant from the National Research Foundation of Korea; reports consultancy/speaker fees from Alexion Pharmaceuticals, Aprilbio, Celltrion, Eisai, HanAll BioPharma, Merck Serono, Novartis, Sanofi Genzyme, Teva-Handok, and Viela Bio; serves on a steering committee for Viela Bio (formerly MedImmune); and is a co-editor for the Multiple Sclerosis Journal and an associate editor for the Journal of Clinical Neurology. C.O.-G. has received speaker fees from Biogen Idec, Celgene, Genzyme, Novartis, Roche, Sanofi Merck, and Teva. I.N. reports personal fees from Biogen Japan, Mitsubishi Tanabe Pharma, Novartis, and Takeda; and grants from LSI Medience, the Ministry of Education, Science and Technology of Japan, and the Ministry of Health, Welfare and Labor of Japan. M.L. reports research support from Alexion Pharmaceuticals, Alnylam, ApoPharma, Sanofi Genzyme, Takeda (formerly Shire), Viela Bio (formerly MedImmune), and ViroPharma; and serves as a consultant for Alexion Pharmaceuticals, ApoPharma, Chugai Pharma, MedImmune, Quest Diagnostics, Sanofi Genzyme, and Takeda (formerly Shire). S.S., M.Y., and L.M. are employees of and hold stock in Alexion Pharmaceuticals. R.A. was an employee of and holds stock in Alexion Pharmaceuticals. D.M.W. reports grants from Alexion Pharmaceuticals during the conduct of the study; and personal fees from Biogen, Celgene, Genentech, MedImmune, Novartis, Reistone Biopharma, TG Therapeutics, and Third Rock Ventures.
Note
Alexion Pharmaceuticals, Inc became part of AstraZeneca on 21 July 2021 and is now Alexion, AstraZeneca Rare Disease.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Alexion Pharmaceuticals.
Data Availability Statement
Alexion will consider requests for disclosure of clinical study participant-level data provided that participant privacy is assured through methods like data de-identification, pseudonymization, or anonymization (as required by applicable law), and if such disclosure was included in the relevant study informed consent form or similar documentation. Qualified academic investigators may request participant-level clinical data and supporting documents (statistical analysis plan and protocol) pertaining to Alexion-sponsored studies. Further details regarding data availability and instructions for requesting information are available in the Alexion Clinical Trials Disclosure and Transparency Policy at http://alexion.com/our-research/research-and-development. Link to data request form: ![]()
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.