
Abstract
In a large acute myelitis cohort, we aimed to determine whether brighter spotty lesions (BSLs)—using the refined terminology—on spinal magnetic resonance imaging (MRI) help distinguish aquaporin-4 antibody-positive neuromyelitis optica spectrum disorder (AQP4-NMOSD) from myelin oligodendrocyte glycoprotein antibody disease (MOGAD). An experienced neuro-radiologist and two neurologists independently analyzed 133 spinal MRI scans (65 from MOGAD and 68 from AQP4-NMOSD) acquired within 1 month of attacks. BSLs were observed in 18 of 61 (30%) participants with AQP4-NMOSD, while none of 49 participants with MOGAD showed BSL (p < 0.001). BSL during the acute phase would be useful to differentiate AQP4-NMOSD from MOGAD.
Keywords
Introduction
Recently, myelin oligodendrocyte glycoprotein antibody disease (MOGAD) was differentiated from aquaporin-4 antibody-positive neuromyelitis optica spectrum disorder (AQP4-NMOSD) based on differences in underlying pathogenic mechanisms. 1 Despite these differences, AQP4-NMOSD and MOGAD demonstrates some similar clinical and radiological manifestations, such as longitudinally extensive transverse myelitis (LETM). 2 Due to the different therapeutic responses and clinical outcomes reported between AQP4-NMOSD and MOGAD, 1 early and accurate differential diagnosis of AQP4-NMOSD and MOGAD is important. Differential diagnosis basically depends on statues of AQP4 and myelin oligodendrocyte glycoprotein (MOG) antibodies, but considering that assays for antibodies are not always timely available in clinical practice, identification of the other discriminative radiological and/or clinical features is warranted.
On spinal magnetic resonance imaging (MRI), a brighter spotty lesion (BSL) is defined as a more hyperintense (brighter) spotty lesion on axial T2 imaging than the usual T2-hyperintense (bright) lesion. 3 BSL is a helpful radiological feature for discriminating AQP4-NMOSD from multiple sclerosis or other causes of myelopathy;3–9 however, BSL was not explicitly defined in some previous studies, and prior investigations did not focus on direct comparison of BSL in a large acute myelitis cohort of AQP4-NMOSD and MOGAD. Therefore, we used the term “brighter” spotty lesion—in contrast to “bright” spotty lesion—to clearly reflect updates to our research lexicon. 3 Using the refined terminology, this study aimed to determine whether BSL—observed on spinal MRI during the acute phase—is useful in differentiating AQP4-NMOSD from MOGAD.
Methods
Participants with MOGAD and AQP4-NMOSD, who (1) experienced at least one myelitis attack and (2) underwent spinal MRI during the acute phase (within 1 month after the myelitis attack), were enrolled. From 2005 to 2021, 49 consecutive participants from six Korean hospitals with positive results for MOG antibodies using a live cell-based assay, were included. 10 In addition, 61 age-/attack severity–matched participants from the National Cancer Center with positive results for AQP4 antibodies tested by a live cell-based assay were included (Supplemental Material Reference 1); 48 of those were also included in our previous study, 3 and their spinal MRI findings were re-analyzed blindly. In total, 133 spinal MRI scans, including 65 scans from MOGAD and 68 from AQP4-NMOSD, were retrospectively collected. All MRI scans were performed using a 1.5–3 T scanner from different centers; therefore, the MRI protocols could not be fully standardized.
The radiological findings were analyzed independently by one experienced neuro-radiologist and two neurologists blinded to the diagnosis. BSL was defined as an extraordinarily hyperintense spotty lesion on axial T2-weighted imaging; the signal should be at least as high as the surrounding cerebrospinal fluid (CSF). On T1-weighted imaging, the signal should not be as low as the surrounding CSF because of its distinction from syringomyelia. 3 LETM was defined as the length of the lesion over three vertebral segments. 2 The transversally extensive lesions were defined as axial lesions extending over half of the cross-sectional area. 3 The presence of BSL, lesion length, axial location, and the presence of gadolinium enhancement were investigated.
The radiological findings between participants with AQP4-NMOSD and those with MOGAD were compared using Fisher’s exact test or chi-square test. Cronbach’s α coefficient, used to estimate inter-rater variability, was 0.93 for BSL and greater than 0.9 for all cases.
The institutional review board of each participating hospital approved this study, and written informed consent was obtained from all participants.
Results
Table 1 shows the demographics and spinal MRI findings of participants with AQP4-NMOSD and MOGAD. For AQP4-NMOSD, the median age at MRI was 38.4 years and the disability severity was 3.5, as assessed by the expanded disability status scale score at the attack nadir. For MOGAD, the median age at MRI was 35 years and the disability severity was 3.5.
Demographics and spinal MRI findings of participants with AQP4-NMOSD and MOGAD.
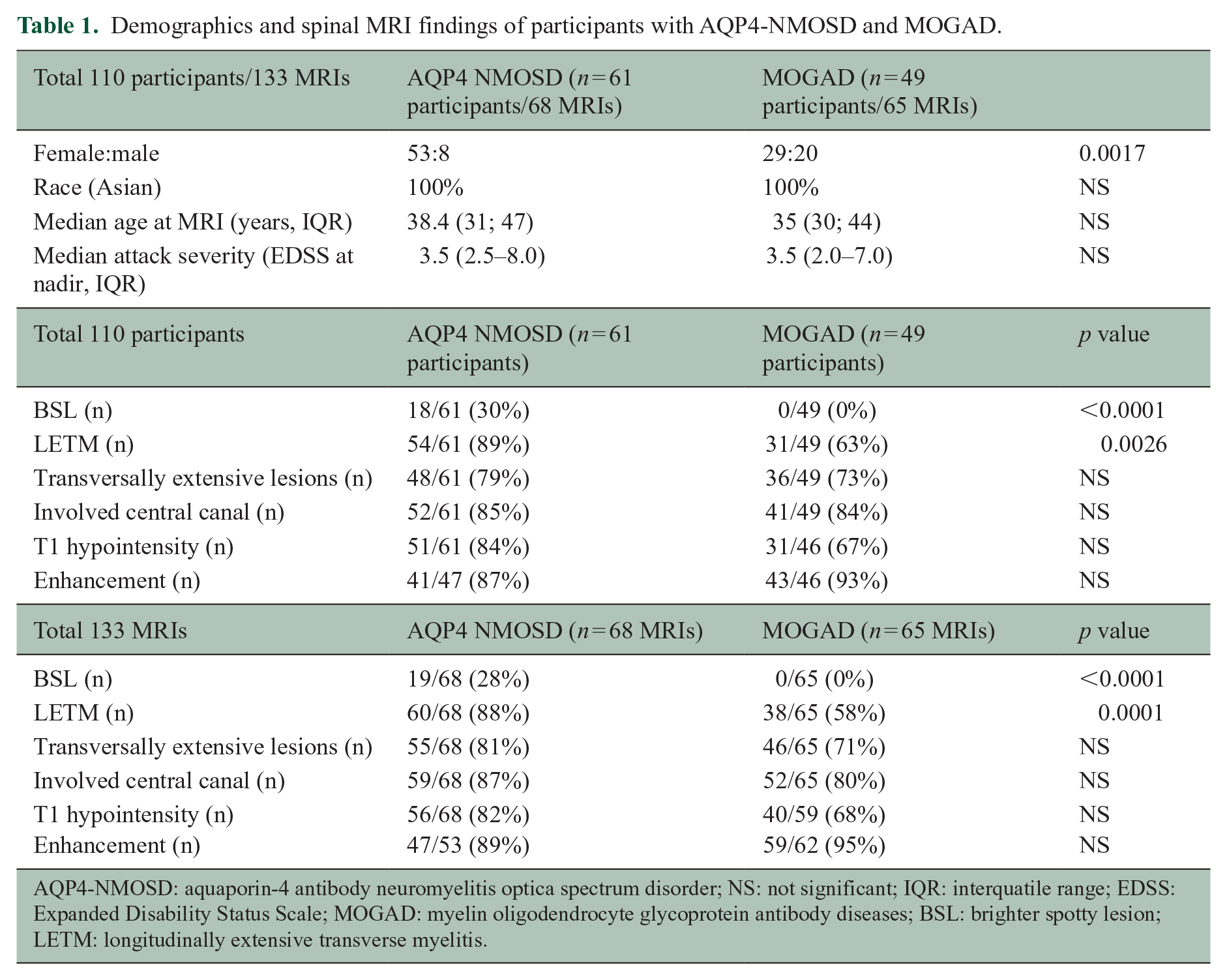
AQP4-NMOSD: aquaporin-4 antibody neuromyelitis optica spectrum disorder; NS: not significant; IQR: interquatile range; EDSS: Expanded Disability Status Scale; MOGAD: myelin oligodendrocyte glycoprotein antibody diseases; BSL: brighter spotty lesion; LETM: longitudinally extensive transverse myelitis.
Among a total of 110 participants (133 MRI scans), BSLs were found in 18 of 61 (30%) participants (19 of 68 (28%) MRI scans) with AQP4-NMOSD (Figure 1), while none of 49 participants (0 of 65 MRI scans) with MOGAD had BSLs (p < 0.0001). Other axial findings, T1 hypointense lesions and gadolinium enhancements were not significantly different between AQP4-NMOSD and MOGAD. LETM was commonly observed in both participants with AQP4-NMOSD (54/61, 89%) and MOGAD (31/49, 63%), but the difference was significant (p = 0.0026). In two of the seven participants with AQP4-NMOSD but without LETM, BSLs were observed.
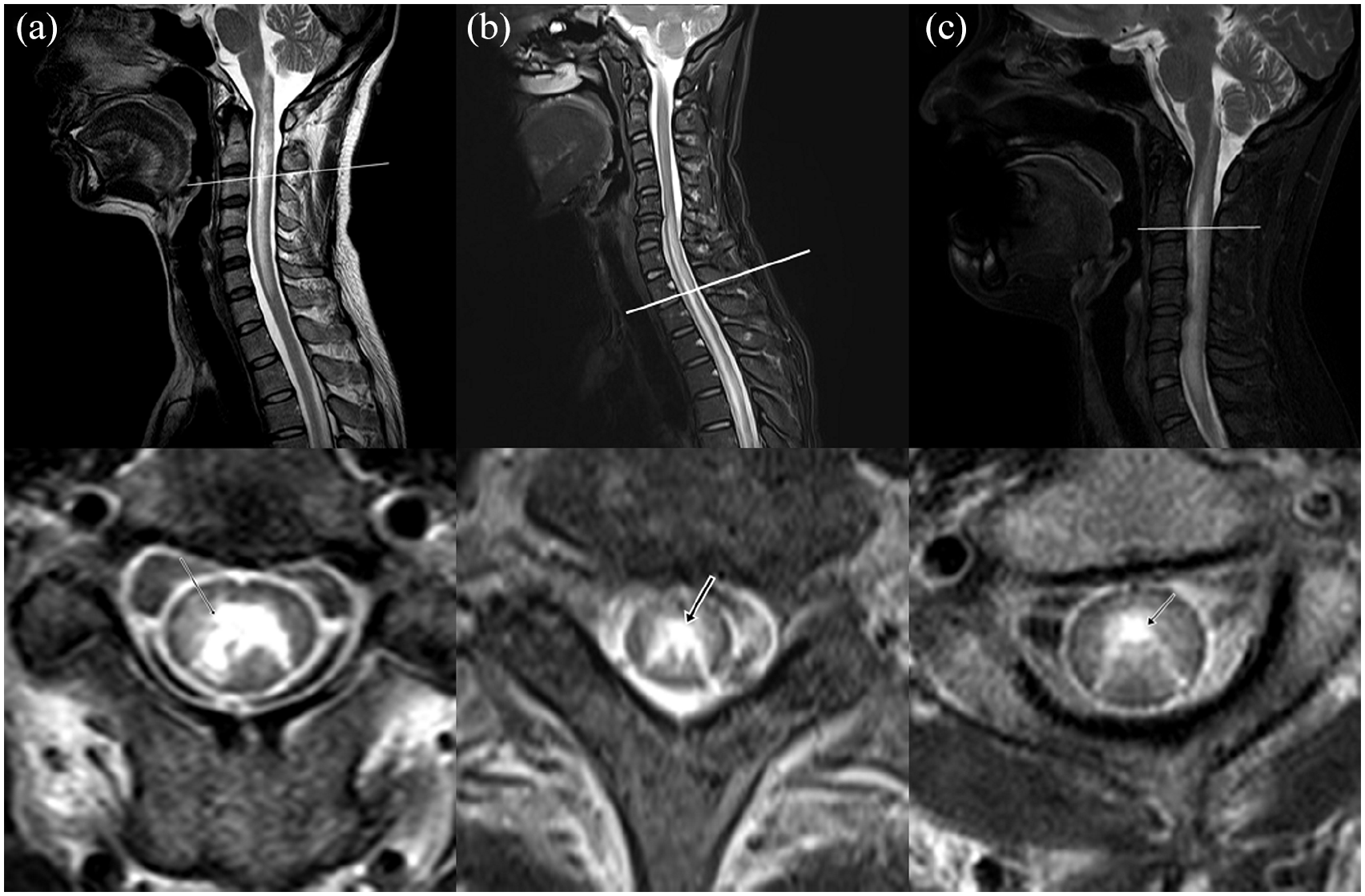
(a, b, c) Three representative cases of brighter spotty lesions in the AQP4 antibody-positive neuromyelitis optica spectrum disorder.
Discussion
In this study, we used a refined term and directly compared BSL in a large acute myelitis cohort of AQP4-NMOSD and MOGAD; BSL was not observed in MOGAD, while 30% of AQP4-NMOSD showed BSL, comparable to the previous studies using the same definition of this study (27%–40%).3,9 A few studies recently evaluated BSL in a very small number of participants with MOGAD. Two of those studies reported that BSLs were observed in 50% (2/4 or 5/10) of patients with MOGAD adhered to definitions of BSL as a “T2 hyperintense spotty lesion” or “bright spots.”6–8 Another study revealed no BSL (0/4) in MOGAD using the same definition of our prior study. 9 These findings highlight the importance of proper application of BSLs in practice. In contrast to exclusive observation of BSL in AQP4-NMOSD, other axial findings on spinal MRIs, including transversally extensive and central canal involvement, were not significantly different between the AQP4-NMOSD and MOGAD groups. LETM was commonly observed (63%) in MOGAD, consistent with previous results (62%–79%) (Supplemental Material Reference 2).2 Notably, in this study, 29% (2/7) of AQP4-NMOSD participants without LETM could be additionally diagnosed with AQP4-NMOSD using BSLs.
Several limitations were entailed in this study. The MRI protocols could not be completely unified because of their retrospective nature; however, the exams reflected real-world clinical practice. In addition, all participants were enrolled from the Asian population, and the clinical implications of BSL beyond its diagnostic value should be elucidated. Further prospective investigations, including pathological evaluations in diverse racial groups, are required.
In conclusion, when a precise definition of BSL was adopted, BSL was a useful discriminator of myelitis in AQP4-NMOSD and MOGAD. If this finding is reproduced by future investigation, BSL may emerge as a characteristic feature for revising the diagnostic criteria for AQP4-NMOSD.
Supplemental Material
sj-docx-1-msj-10.1177_13524585211060326 – Supplemental material for Brighter spotty lesions on spinal MRI help differentiate AQP4 antibody-positive NMOSD from MOGAD
Supplemental material, sj-docx-1-msj-10.1177_13524585211060326 for Brighter spotty lesions on spinal MRI help differentiate AQP4 antibody-positive NMOSD from MOGAD by Jae-Won Hyun, Hye Lim Lee, Jaehong Park, Jiah Kim, Ju-Hong Min, Byoung Joon Kim, Seung Woo Kim, Ha Young Shin, So-Young Huh, Woojun Kim, Ji Won Seo, Ki Hoon Kim, Su-Hyun Kim and Ho Jin Kim in Multiple Sclerosis Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: H.L.L., J.P., J.K., B.J.K., S.W.K., H.Y.S., S.Y.H., W.K., J.W.S., K.H.K. report no disclosures. J.W.H. has received a grant from the National Research Foundation of Korea. J.H.M. has lectured, consulted, and received honoraria from Bayer Schering Pharma, Merk Serono, Biogen Idec, Sanofi Genzyme, UCB, Samsung Bioepis, and Roche; received a grant from the National Research Foundation of Korea. SHK has lectured, consulted, and received honoraria from Bayer Schering Pharma, Biogen, Genzyme, Merck Serono, and UCB; and received a grant from the National Research Foundation of Korea. K.H.J. received a grant from the National Research Foundation of Korea and research support from Aprilbio and Eisai; received consultancy/speaker fees from Alexion, Aprilbio, Biogen, Celltrion, Daewoong, Eisai, GC Pharma, HanAll BioPharma, MDimune, Merck Serono, Novartis, Roche, Sanofi Genzyme, Teva-Handok, UCB, and Viela Bio; and is a co-editor for the Multiple Sclerosis Journal and an associated editor for the Journal of Clinical Neurology.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Research Foundation of Korea (grant nos. NRF-2020R1F1A1072174 & NRF-2018R1A5A2023127).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.