
Abstract
Background
Data are sparse regarding the safety of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) vaccines in patients with multiple sclerosis (MS).
Objective
To estimate (1) the pooled proportion of MS patients experiencing relapse among vaccine recipients; (2) the rate of transient neurological worsening, adverse events, and serious adverse events; (3) the previous outcomes of interest for different SARS-CoV-2 vaccine types.
Methods
Systematic review and meta-analysis of pharmacovigilance registries and observational studies.
Results
Nineteen observational studies comprising 14,755 MS patients who received 23,088 doses of COVID-19 vaccines were included. Mean age was 43.3 years (95% confidence interval (CI): 40–46.6); relapsing-remitting, secondary-progressive, primary-progressive MS and clinically isolated syndrome were diagnosed in 82.6% (95% CI: 73.9–89.8), 12.6% (95% CI: 6.3–20.8), 6.7% (95% CI: 4.2–9.9), and 2.9% (95% CI: 1–5.9) of cases, respectively. The pooled proportion of MS patients experiencing relapse at a mean time interval of 20 days (95% CI: 12–28.2) from vaccination was 1.9% (95% CI: 1.3%–2.6%; I2 = 78%), with the relapse risk being independent of the type of administered SARS-CoV-2-vaccine (p for subgroup differences = 0.7 for messenger RNA (mRNA), inactivated virus, and adenovector-based vaccines). After vaccination, transient neurological worsening was observed in 4.8% (95% CI: 2.3%–8.1%) of patients. Adverse events and serious adverse events were reported in 52.8% (95% CI: 46.7%–58.8%) and 0.1% (95% CI: 0%–0.2%) of vaccinations, respectively.
Conclusion
COVID-19 vaccination does not appear to increase the risk of relapse and serious adverse events in MS. Weighted against the risks of SARS-CoV-2-related complications and MS exacerbations, these safety data provide compelling pro-vaccination arguments for MS patients.
Keywords
Introduction
Neuroimmunological adverse events have been reported as rare, but serious complications following immunization against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). 1 Although the exact pathophysiological mechanisms implicated in neuroimmunological reactions to SARS-CoV-2 vaccines remain to-date poorly elucidated, a vaccine-induced over-activation of the innate immune system, including both humoral and cell-mediated immune responses is speculated. Particularly for patients with pre-existing autoimmune diseases, including multiple sclerosis (MS), the propagation of vaccine-induced autoimmunity poses serious concerns regarding the potential risk for vaccine-triggered disease exacerbations.
Regarding SARS-CoV-2 vaccine safety, it is noteworthy that patients with MS have not been included in the seminal randomized controlled clinical trials (RCTs) for regulatory approval of currently licensed vaccines. While post-marketing surveillance data are still collated, the so-far available safety evidence in the MS patient population derives mainly from observational studies and clinical registries, with limited sample of vaccinated MS patients. On the contrary, the landscape of SARS-CoV-2 vaccinology is rapidly evolving,2,3 with novel technologies and different types of vaccines being granted emergency use authorization worldwide, thereby necessitating continuous monitoring especially in populations at high risk for autoimmunity.4 Among the currently employed SARS-CoV-2 vaccine technologies, inactivated virus vaccines, viral vector vaccines, nucleic acid (messenger RNA (mRNA; and recently DNA)) vaccines, and protein subunit vaccines have been licensed in different countries across the globe. 4 Despite the galloping pace of SARS-CoV-2 vaccine advances, there is currently very limited evidence on the comparative safety of different SARS-CoV-2 vaccine types in MS.
Current practice guidelines recommend immunization with any type of available SARS-CoV-2 vaccine for MS patients, including those receiving immunosuppressive disease-modifying therapies (DMT). 5 Although accumulating evidence suggests that the benefits of SARS-CoV-2 vaccines outweigh any potential vaccine-related risks, there is still considerable vaccine hesitancy among MS patients. To the best of our knowledge, the safety of SARS-CoV-2 vaccines in the MS population has not been previously assessed using a meta-analytical approach. The aim of the present systematic review and meta-analysis was thus, threefold: (1) to estimate the pooled proportion of MS patients experiencing relapse among vaccine recipients; (2) to estimate the rate of transient neurological worsening, adverse events, and serious adverse events; and (3) to assess the previous outcomes of interest in patients exposed to different types of SARS-CoV-2 vaccines.
Methods
Standard protocol approvals, registrations, and patient consents
The pre-specified protocol of the present systematic review and meta-analysis has been registered in the International Prospective Register of Ongoing Systematic Reviews PROSPERO (Registration Number: CRD42021282052). The meta-analysis is reported according to the updated Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and data are presented according to the Meta-Analysis of Observational Studies Epidemiology (MOOSE) proposal. This study did not require an ethical board approval or written informed consent due to the study design (systematic review and meta-analysis).
Data sources, searches, and study selection
A systematic literature search was conducted independently by three reviewers (MIS, MVC, and AT) to identify eligible RCTs and observational studies on SARS-CoV-2 vaccination of patients with multiple sclerosis (MS). We searched MEDLINE and Scopus, using the following search terms: “Covid-19 vaccines,” “SARS-CoV-2 vaccines,” “mRNA vaccines,” “Multiple sclerosis,” “Clinically isolated syndrome,” and “Optic neuritis.” The full search string used is provided in the Supplement (eMethods). No language or other search restrictions were applied. Our search spanned from inception of each database to 17 November 2022. We also searched the reference lists of published studies manually, as well as conference abstracts, including the abstracts of the annual meeting of the European Committee for the Treatment and Rehabilitation In Multiple Sclerosis (ECTRIMS), to ensure the comprehensiveness of the bibliography.
Studies that provided clinical data in patients vaccinated against SARS-CoV-2 with any type of MS were eligible for inclusion. We excluded studies (1) including patients with uncertain MS, clinically isolated syndrome (CIS) or optic neuritis (ON) diagnoses; (2) reporting interventions or outcomes not aligned with our inclusion criteria; and (3) case series, case reports, narrative and systematic reviews, commentaries, non-peer reviewed studies, and pre-prints. In case of data overlap between studies, we retained the study with the largest data set. All studies were independently evaluated by four reviewers (MIS, MVC, AT, LP) and disagreements were settled by mutual consensus after discussion with the corresponding author (SG).
Quality control, risk of bias assessment, and data extraction
Eligible studies were subjected to quality control and risk of bias assessment employing the Cochrane risk of bias (RoB 2) tool 6 for RCTs, and the Risk Of Bias In Non-randomized Studies of Interventions (ROBINS-I) tool 7 for observational studies. Quality control and risk of bias assessment were conducted independently by two reviewers (MIS and LP), and disagreements were settled by consensus after discussion with the corresponding author (SG).
Data extraction was performed in structured forms, including author names, study design, country, type of vaccines administered, doses of vaccines reported, number of included MS patients, patients’ characteristics, and outcome events.
Outcomes
An aggregate data meta-analysis was performed with inclusion of the identified studies. The primary outcome of interest was the pooled proportion of patients experiencing relapse among included MS patients receiving COVID-19 vaccination.
Secondary outcomes of interest comprised (1) the proportion of patients with transient neurological worsening (i.e. transient deterioration of MS symptoms after vaccination or pseudo-relapse); (2) the proportion of patients with adverse events (including post-vaccination fever, injection-site tenderness/pain, myalgia, arthralgia, malaise, nausea, headache, and fativational, and their main characterisgue); and (3) the proportion of patients with serious adverse events (i.e. serious life-threatening or extended hospitalization events). Baseline characteristics of patients, including sex, age, type of MS, disease duration, history of DMT, and disability status (assessed by the Expanded Disability Status Scale (EDSS)) were also analyzed. All outcomes were further assessed after stratification by (1) vaccine type (mRNA, inactivated virus, adenovirus vector) and (2) vaccine dose (first, second, and third).
Statistical analysis
For the aggregate meta-analysis, we calculated for each dichotomous outcome of interest the corresponding pooled proportions with 95% confidence intervals (95% CI), after the implementation of the variance-stabilizing double arcsine transformation. For studies reporting continuous outcomes in median values and corresponding interquartile ranges, we estimated the sample mean and standard deviation using the quantile estimation method. Continuous outcomes were assessed by mean difference (MD). In the cases where no events were observed for assessed outcomes in included studies, a continuity correction was performed in accordance with the Cochrane Handbook. The random-effects model of meta-analysis (DerSimonian and Laird) was used to calculate the pooled estimates. Subgroup differences between different study designs were assessed by the Q test for subgroups. Heterogeneity was assessed with the I2 and Cochran Q statistics. For the qualitative interpretation of heterogeneity, I2 values > 50% and values > 75% were considered to represent substantial and considerable heterogeneity, respectively. The significance level for the Q statistic was set at 0.1. Publication bias across individual studies was assessed when more than four studies were included in the analysis of the outcomes of interest, using funnel plot inspection and the Egger’s linear regression test when more than 10 studies were included, and the equivalent z test for each pooled estimate with a two-tailed p value < 0.05 was considered statistically significant. All statistical analyses using the OpenMetaAnalyst 8 and R software version 3.5.0 (package: metafor). 9
Data availability statement
All data generated or analyzed during this study are included in this article and its supplementary information files.
Results
Literature search and included studies
The systematic database search yielded a total of 263 records from the MEDLINE and SCOPUS databases, after the exclusion of potential duplicates (Figure 1). After initial screening, we retrieved the full text of 76 records that were considered potentially eligible for inclusion and after reading the full-text articles, 57 were further excluded (Supplemental eTable 1). Finally, we identified 19 eligible studies for inclusion.10–28 All studies were observational, and their main characteristics are presented in Table 1, while per study definitions of MS relapse and transient neurological worsening are provided in Supplemental eTable 2. The PRISMA flow chart of the current meta-analysis is available in Figure 1.
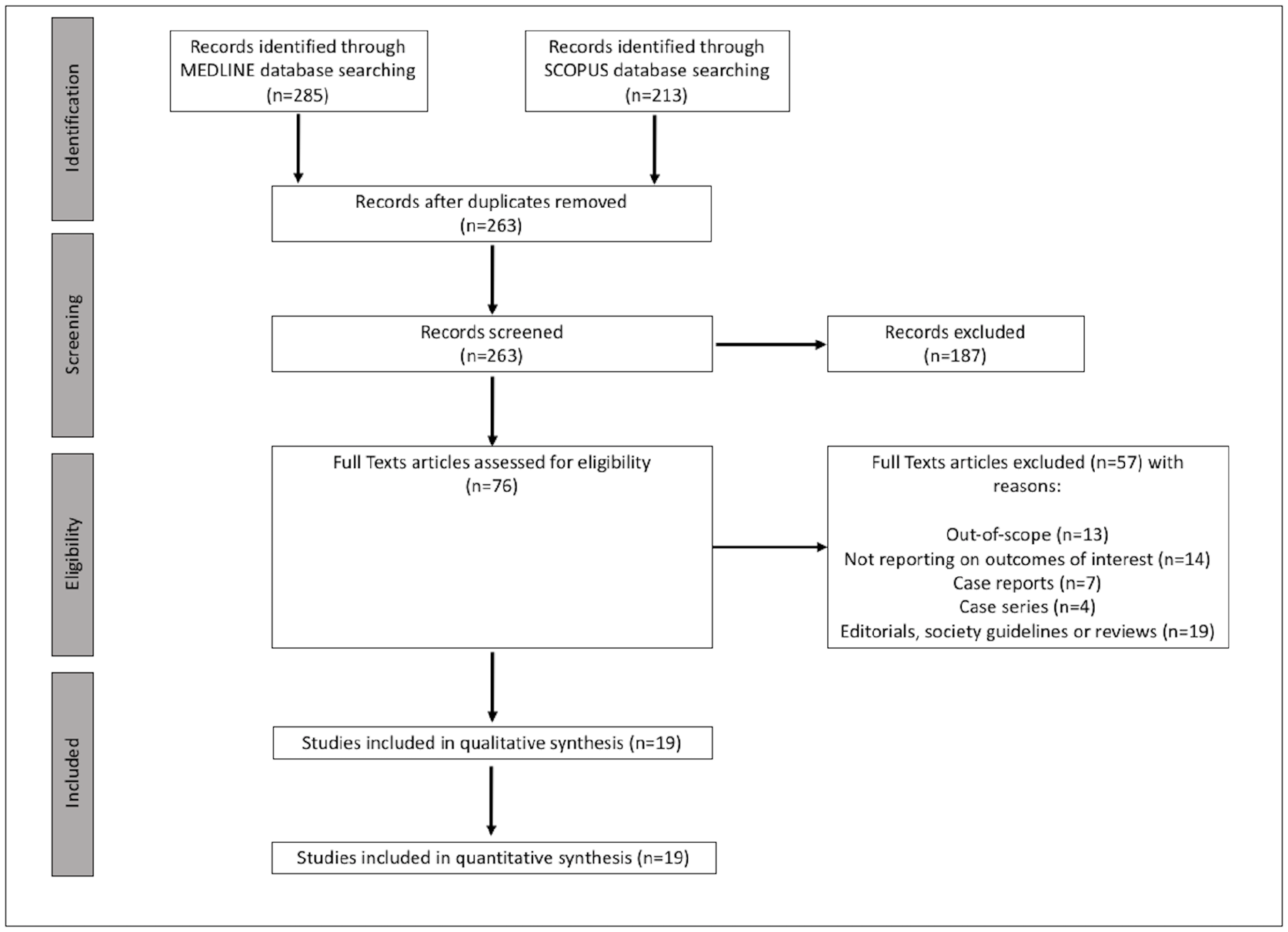
Flow chart presenting the selection of eligible studies.
Main characteristics of studies (n = 19) included in the systematic review.
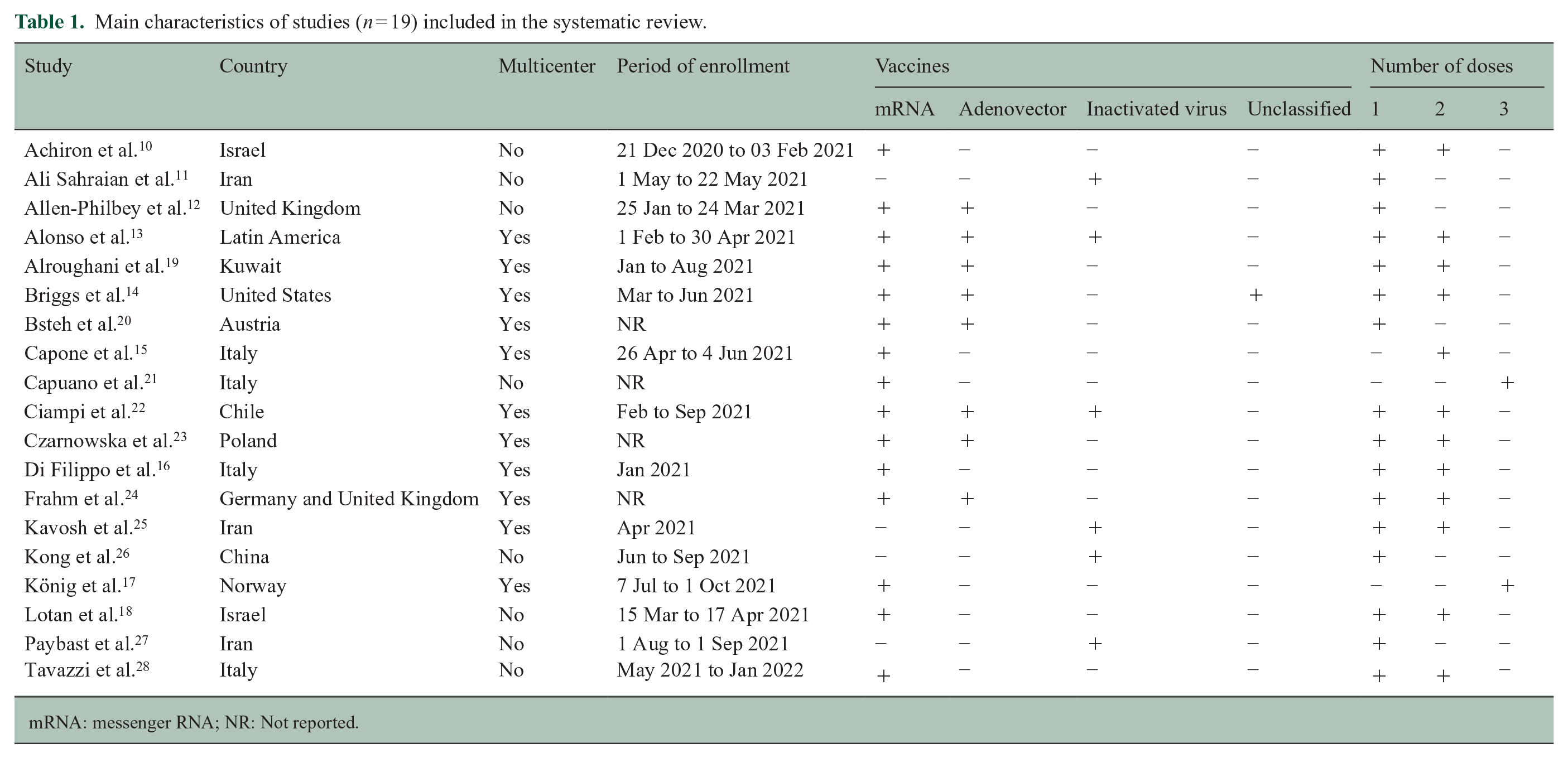
mRNA: messenger RNA; NR: Not reported.
Quality control of included studies
The risk of bias in the included observational studies was assessed by the ROBINS-I tool 7 and is presented in Supplemental eFigures 1 and 2. The majority of studies presented significant selection bias by including patients accepting to complete online questionnaires, while the outcomes were patient-reported and only rarely adjudicated; hence, significant information and reporting biases also existed.
Quantitative analyses
According to the extracted data, 14,755 patients with MS received a total of 23,088 doses of any kind of COVID-19 vaccine. A first vaccine-dose was administered to 14,755 patients, the second dose was administered to 8473 patients, and 177 patients were reported to have received a third dose of COVID-19 vaccination. The majority of the patients received an mRNA vaccine (n = 6956), followed by inactivated virus vaccine in 2590 patients, while adenovirus-vector vaccine was administered in 1424 patients. None of the included studies reported on DNA vaccines or subunit vaccines, as only India has so far approved the DNA-based ZyCoV-D vaccine, 3 while subunit vaccines have only very recently been granted emergency use authorization in several countries.
Baseline characteristics
More than 71% of the patients were women (95% CI: 68.3%–74.5%; 17 studies; I2 = 92%; p for Cochran Q < 0.001; Supplemental eFigure 3) and the mean age was 43.3 years old (95% CI: 40.0–46.6; 16 studies; I2 = 99%; p for Cochran Q < 0.001; Supplemental eFigure 4). The most prevalent type of MS was relapsing-remitting MS (RRMS; pooled proportion 82.6%; 95% CI: 73.9%–89.8%; 13 studies; I2 = 99%; p for Cochran Q < 0.001; Supplemental eFigure 5), followed by secondary-progressive MS (12.6%), primary-progressive MS (6.7%) and clinically isolated syndrome (2.9%). The mean disease duration was 10.3 years (95% CI: 9.4–11.2; 14 studies; I2 = 97%; p for Cochran Q < 0.001; Supplemental eFigure 6) and 84.7% of patients had been under DMT (95% CI: 74.7%–92.5%; 15 studies; I2 = 99%; p for Cochran Q < 0.001; Supplemental eFigure 7). The pooled mean disability score at inclusion was calculated at 2.5 points (95% CI: 2.2–2.7; 13 studies; I2 = 97%; p for Cochran Q < 0.001; Supplemental Supplemental eFigure 8), measured by the EDSS when reported in each study.
The mean follow-up duration after any dose of COVID-19 vaccination was 93.3 days (95% CI: 51.6–135.1; six studies; I2 = 99%; p for Cochran Q < 0.001; Supplemental eFigure 9), with the exception of the study by Briggs et al. 14 which reported adverse events within 24 hours after vaccination.
Primary outcome
The pooled proportion of patients experiencing a relapse post COVID-19 vaccination was 1.9% (95% CI: 1.3%–2.6%; 14 studies; I2 = 78%; p for Cochran Q < 0.001; Supplemental eFigure 10), after a mean of 20 days (95% CI: 12.0–28.2; 4 studies; I2 = 95%; p for Cochran Q < 0.001; Supplemental eFigure 11). When the analysis was stratified according to vaccine type, no subgroup differences were disclosed (p for subgroup differences = 0.738; Figure 2) between the different types of COVID-19 vaccines: (1) mRNA: 1.7% of the patients relapsed (95% CI: 1.1%–2.5%; eight studies; I2 = 4%; p for Cochran Q = 0.403); (2) inactivated virus: 1.4% of the patients relapsed (95% CI: 0.8%–2.3%; six studies; I2 = 40%; p for Cochran Q = 0.137); and (3) adeno-vector: 1.5% of the patients relapsed (95% CI: 0.5%–2.9%; four studies; I2 = 0%; p for Cochran Q = 0.738). However, when different doses of vaccines were assessed, significant subgroup differences emerged (p for subgroup differences = 0.023; Figure 3): (1) 1.1% of the patients relapsed after the first vaccine dose (95% CI: 0.8%–1.5%; seven studies; I2 = 28%; p for Cochran Q = 0.216); (2) 1.2% of the patients relapsed after the second vaccine dose (95% CI: 0.5%–2.1%; two studies; I2 = 77%; p for Cochran Q = 0.004); and (3) no patients were reported to have relapsed after the third vaccine dose (pooled proportion 0.5%; 95% CI: 0%–2.1%; two studies; I2 = 0%; p for Cochran Q = 0.632).
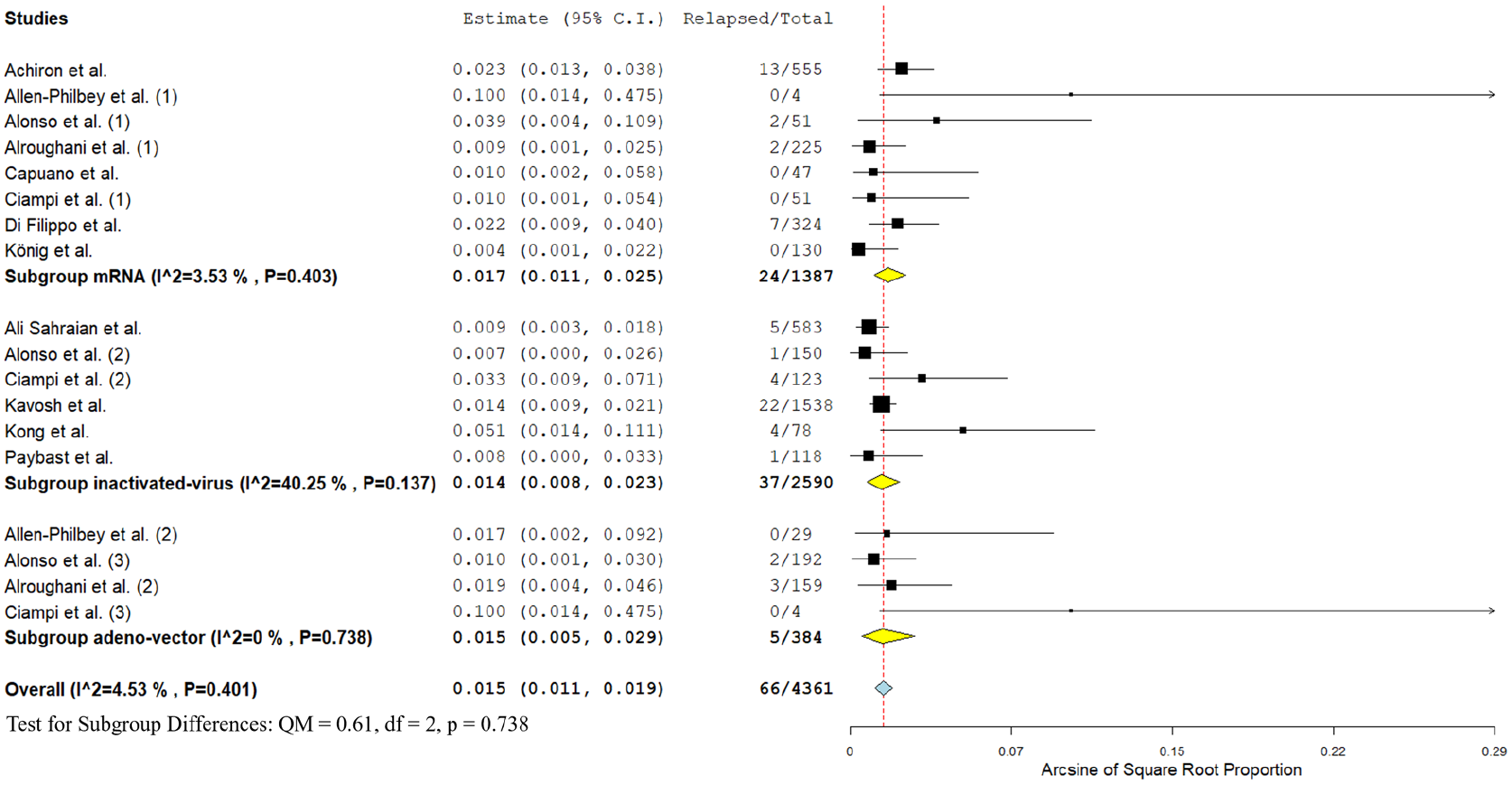
Forest plot presenting the pooled proportion of patients experiencing relapses among the total MS patients having received COVID-19 vaccination, stratified by vaccine type.
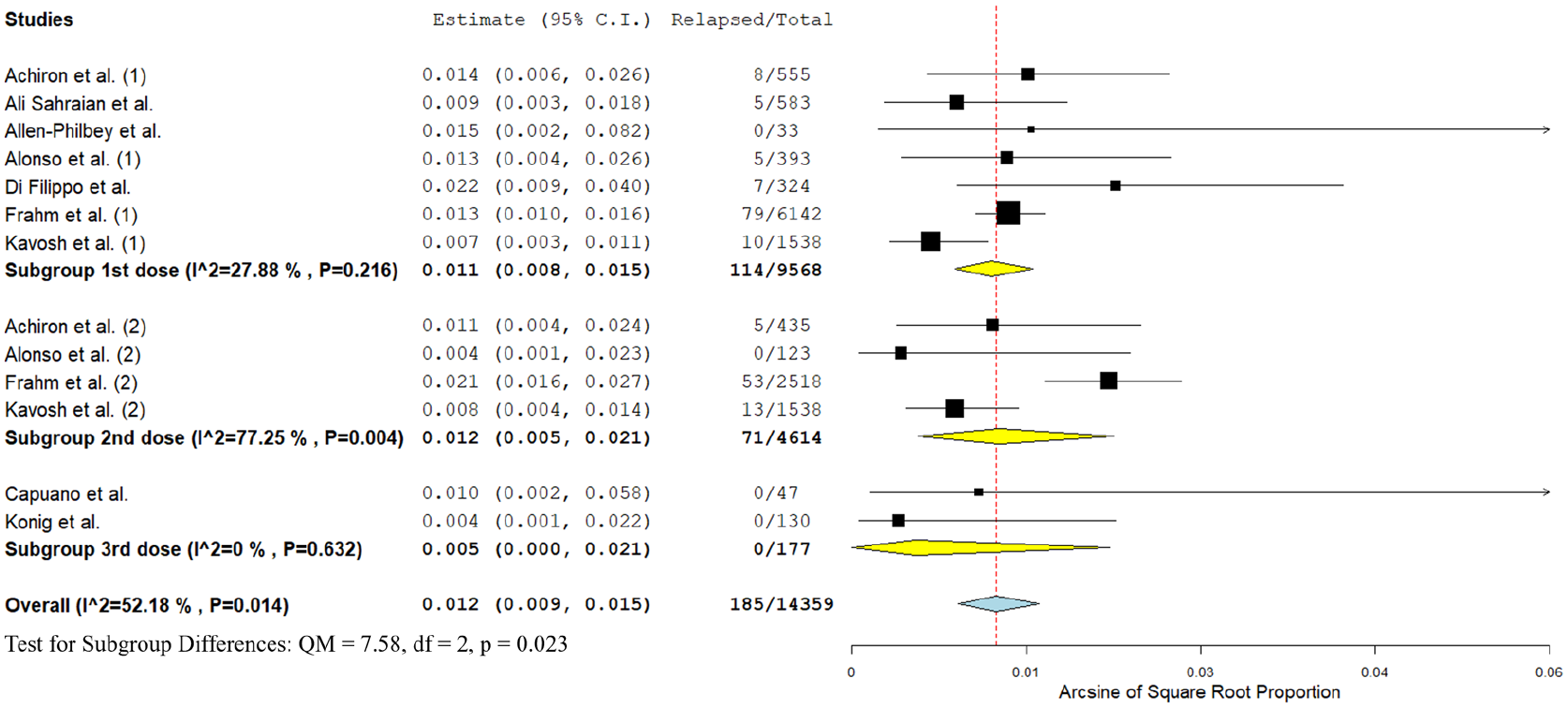
Forest plot presenting the pooled proportion of patients experiencing relapses among the total MS patients having received COVID-19 vaccination, stratified by vaccine dose.
Secondary outcomes
Among MS patients receiving COVID-19 vaccination, 4.8% presented transient neurological worsening after vaccination (95% CI: 2.3%–8.1%; seven studies; I2 = 95%; p for Cochran Q < 0.001; Supplemental eFigure 12). No subgroup differences were disclosed among different vaccines types (p for subgroup differences = 0.494; Supplemental eFigure 13). However, more patients reported transient neurological worsening following the second versus the first dose of vaccination (p for subgroup differences = 0.023; Supplemental eFigure 14).
An adverse event was reported following 52.8% of any COVID-19 vaccine dose (95% CI: 46.7%–58.8%; 15 studies; I2 = 98%; p for Cochran Q < 0.001; Supplemental eFigure 15). Significant differences were disclosed after stratification by vaccine type, with more adverse events being reported after vaccination using adenovectors vaccines (Supplemental eFigure 16). No subgroup differences were disclosed after stratification for vaccine dose (Supplemental eFigure 17). Serious adverse events were reported following 0.1% of any COVID-19 vaccine dose (95% CI: 0%–0.2%; eight studies; I2 = 0%; p for Cochran Q = 0.635; Supplemental eFigure 18). Again, there were no subgroup differences after stratification for vaccine type (Supplemental eFigure 19) or for vaccine dose (Supplemental eFigure 20).
An overview of analyses for primary and secondary outcomes is presented in Table 2.
Overview of analyses for primary and secondary outcomes.
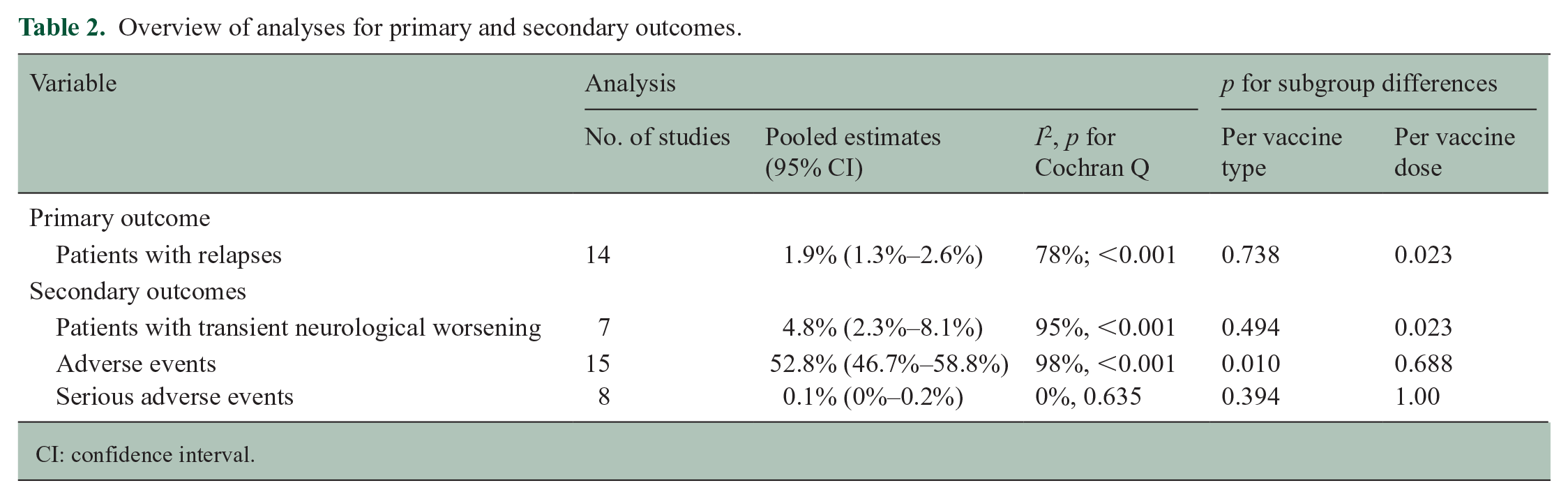
CI: confidence interval.
Publication bias
Publication bias was evaluated using funnel plots for every outcome of the analysis. Asymmetry or evidence of small study effects (i.e. publication bias) were detected for relapses, transient neurological worsening, and adverse events, but not for serious adverse events (Supplemental eFigures 21–24).
Discussion
The present systematic review and meta-analysis, including data from 14,755 MS patients who received a cumulative number of 23,088 doses of any SARS-CoV-2 vaccine has documented the following findings in summary. First, the pooled proportion of patients experiencing MS relapse at a mean time interval of 20 days (95% CI: 12–28.2) from SARS-CoV-2 vaccination was 1.9% (95% CI: 1.3%–2.6%). These findings are reassuring, as they fall within the range of risk estimates from large case–crossover studies (i.e. comparing vaccinated to unvaccinated MS patients) and meta-analyses, that have shown no excess relapse risk during the post-vaccination period, for vaccines including tetanus, hepatitis B, Bacille Calmette–Guèrin (BCG), and influenza.29,30 Similarly, these findings do not present significant deviations from epidemiological estimates of annualized relapse rates in the MS patient population estimated between 0.3 and 1.7 per year. 31 In addition, these results are aligned with recent evidence from observational studies, that indicate no excess risk for vaccine-induced neuroimmunological responses following SARS-CoV-2 vaccination in patients with neuroimmunological disorders, including MS.32,33
Second, despite the rare implication of mRNA and adenoviral vector-based SARS-CoV-2 vaccines in serious autoimmune adverse events, we found no increased risk for MS relapses after stratification according to SARS-CoV-2 vaccine type. It should be noted that although a lower tendency for MS relapses has been previously reported for mRNA vaccines, this finding was documented by a study conducted in the United Kingdom with significant risk of selection biases causing an overrepresentation of the vector-based AZD1222 (ChAdOx1) vaccine (i.e. and vice versa an underrepresentation of mRNA vaccines) and could not be confirmed in the present meta-analysis. 12 Moreover, as opposed to live attenuated vaccines, that confer not only an increased risk for vaccine-induced infection to immunocompromised MS patients, but also an increased risk for relapse, all assessed SARS-CoV-2 vaccine-types, including mRNA, inactivated virus, and viral-vector based, appeared to have a comparable safety profile.
Third, we found significant differences in relapse rates after stratification based on vaccine dose, with lower risk of relapse following the third vaccine dose (0.5%), compared to the relapse rates following the first and second vaccine doses (1.1% and 1.2%, respectively). These results warrant caution in their interpretation, as large deviations in the number and sample size of included studies can be observed, with an almost twofold higher number of vaccine recipients (14,755) followed up after the first compared to the second vaccine dose (8473), and only 177 MS patients having been followed up after their third SARS-CoV-2 vaccine dose. Although these results are most likely attributable to methodological issues, future longitudinal studies are warranted to examine (1) whether MS relapses after initial immunization may lead to vaccine hesitancy (i.e. drop-out) or switch to different vaccine types in subsequent doses; or (2) whether differences in immune responses (e.g. with respect to type, affinity, and avidity of vaccine-induced humoral responses) could underlie an actual attenuation of the relapse risk in MS patients undergoing booster or repeated SARS-CoV-2 vaccinations.
Fourth, our results show that although adverse events were reported in approximately half of all SARS-CoV-2 vaccinations, these were mild side-effects, which have been reported to be self-limited, including pain at the injection site, fever, malaise, headache, and fatigue. 14 By contrast, serious adverse events were recorded only in 0.1% of all vaccinations. Interestingly, a higher prevalence of vaccine-induced transient neurological worsening was detected in 4.8% of MS patients, which did not differ between different vaccine types but was more frequent following the second versus the first vaccine dose. These results are in accordance with recent evidence pointing toward an increased reactogenicity following administration of the second compared to the first vaccine dose, especially for mRNA vaccines. 34 Besides the presumed molecular mimicry processes underlying vaccine-induced reactogenicity in general, mRNA vaccines exhibit additional properties of self-adjuvantation, with the mRNA acting both as antigen and adjuvant that precipitates overt inflammatory responses. 35 These results lend support to the assumption that immune reactions may trigger “Uhthoff’s phenomenon” in MS patients, that in turn induces transient neurological worsening following immunization, and particularly following exposure to mRNA SARS-CoV-2 vaccines, albeit further research is required to evaluate this hypothesis.
To the best of our knowledge, this is the first systematic review and meta-analysis comprising the sum of the so-far published literature on SARS-CoV-2 vaccine safety. Nonetheless, for an accurate interpretation of our results, certain limitations must be acknowledged. First, due to the presence of selection and publication biases, our meta-analysis cannot yield evidence comparable to results of well-designed epidemiological research. Moreover, the generalizability of our findings is limited due to the substantial heterogeneity of included MS patient populations, comprising differences in DMT type and duration, patient demographics including comorbidities that may affect immune responses, and vaccine-specific parameters such as the timing of SARS-CoV-2 vaccination within treatment cycles. Consequently, large, prospective epidemiological studies are warranted to corroborate our findings. Second, regarding patient characteristics, the mean age of MS patients included in the present meta-analysis was fairly advanced at 43.3 years of age, with a mean disease duration of 10.3 years, with both of these indicators being potentially suggestive of more “stable” MS disease stages. Similarly, as RRMS was overrepresented in comparison to progressive MS types and CIS, future studies are needed to assess the safety of SARS-CoV-2 vaccines in different MS patient populations. Third, due to disparities in definitions of transient neurological worsening and MS relapses, in reported outcomes of included studies and the evidence of small study effects (i.e. publication bias), further prospective validation of our results is required once larger and well-characterized registries have been published. Fourth, the aim of the present meta-analysis was to assess SARS-CoV-2 vaccine safety in MS; no RCTs were identified from our search, thus future RCTs are direly needed to assess the safety and also the efficacy of different SARS-CoV-2 vaccine types in different MS populations and under different DMTs. Fifth, as the landscape of SARS-CoV-2 vaccines continues to evolve rapidly, further evidence should be acquired for emerging vaccine types not included in the present meta-analysis (e.g. DNA-based, protein subunit, or other novel vaccines).2,3
In conclusion, the findings of the present meta-analysis indicate that post-vaccination MS relapses are rare, affecting 1.9% of MS patients exposed to SARS-CoV-2 vaccines, with the relapse risk being independent of the type of administered vaccine. Since an almost threefold higher risk for transient neurological worsening was detected, increased awareness is warranted to differentiate accurately between transient neurological worsening and MS relapse. Weighted against the risks of COVID-related MS exacerbations and complications, this safety evidence provides compelling pro-vaccination arguments in MS patients.
Supplemental Material
sj-docx-1-msj-10.1177_13524585221150881 – Supplemental material for Safety of COVID-19 vaccines in multiple sclerosis: A systematic review and meta-analysis
Supplemental material, sj-docx-1-msj-10.1177_13524585221150881 for Safety of COVID-19 vaccines in multiple sclerosis: A systematic review and meta-analysis by Maria-Ioanna Stefanou, Lina Palaiodimou, Aikaterini Theodorou, Maria Veatriki Christodoulou, John S Tzartos, Dimitrios Tzanetakos, Dimitrios Kitsos, Maria Chondrogianni, Vasiliki Zouvelou, Efthimios Dardiotis, Elias Tzavellas, Ekaterini Syrigou, Vassiliki Benetou, George P Paraskevas, Sotirios Tsiodras, Georgios Tsivgoulis and Sotirios Giannopoulos in Multiple Sclerosis Journal
Footnotes
Author Contributions
M.I.S., L.P., G.T., and S.G. contributed to conception and study design. M.I.S., L.P., A.T., M.V.C., and G.T. contributed to acquisition and analysis of data. M.I.S., L.P., G.T., and S.G. contributed to drafting a significant portion of the manuscript or figures. J.S.T., D.T., D.K., M.C., V.Z., E.D., E.T., E.S., G.P.P., S.T., and V.B. contributed with critical comments during manuscript revision. All authors approved the submitted manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Protocol Registration
The protocol of this systematic review and meta-analysis has been registered to the International Prospective Register of Ongoing Systematic Reviews PROSPERO (registration no: CRD42021282052).
Data Availability
The data that support the findings of this study are available from the corresponding author (SG), upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.