
Abstract
Background:
Multiple sclerosis patients experience 3–6 times more seizures than the general population, but observations vary among studies. Seizure risk in disease-modifying therapy recipients remains unknown.
Objective:
The objective of this study was to compare seizure risk in multiple sclerosis patients receiving disease-modifying therapy versus placebo.
Methods:
MEDLINE(OVID), Embase, CINAHL, and ClinicalTrials.gov were searched from database inception until August 2021. Phase 2–3 randomized, placebo-controlled trials reporting efficacy and safety data for disease-modifying therapies were included. Network meta-analysis followed Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines, using Bayesian random effects model for individual and pooled (by drug target) therapies. Main outcome was loge seizure risk ratios [95% credible intervals]. Sensitivity analysis included meta-analysis of non-zero-event studies.
Results:
A total of 1993 citations and 331 full-texts were screened. Fifty-six included studies (29,388 patients—disease-modifying therapy = 18,909; placebo = 10,479) reported 60 seizures (therapy = 41; placebo = 19). No individual therapy was associated with altered seizure risk ratio. Exceptions were daclizumab (−17.90 [−65.31; −0.65]) and rituximab (−24.86 [−82.71; −1.37]) trending toward lower risk ratio; cladribine (25.78 [0.94; 4.65]) and pegylated interferon-beta-1a (25.40 [0.78; 85.47]) trended toward higher risk ratio. Observations had wide credible intervals. Sensitivity analysis of 16 non-zero-event studies revealed no difference in risk ratio for pooled therapies (l0.32 [−0.94; 0.29])
Conclusion:
No evidence of association was found between disease-modifying therapy and seizure risk—this informs seizure management in multiple sclerosis patients.
Introduction
The reported prevalence of seizures in multiple sclerosis (MS) patients is 2%–3%, 1 or 3–6 times higher than in the general population (0.5%–1%). 2 In the absence of high-quality prospective studies of such a rare event, the understanding of seizures in MS relies heavily on case series, which often present heterogeneous findings.
Most patients with MS and epilepsy experience a relatively benign course with good seizure control. 3 However, some studies report greater disability, 4 poorer prognosis with worse cognitive performance and lower brain volumes in those with recurrent seizures, 5 low seizure freedom rates, 6 and an association with status epilepticus. 7 One study found that epilepsy in MS is associated with increased mortality. 8
Although seizures in MS are assumed to be provoked by the underlying demyelinating and inflammatory processes, the exact pathophysiological mechanisms implicated in epileptogenesis in MS remain poorly understood and difficult to substantiate.9,10 Seizures are observed across all MS subtypes. Some studies have found no association between seizures and the severity or duration of MS.5,9,11 Others have reported higher epilepsy rates in patients with an earlier onset of MS and higher Expanded Disability Status Score (EDSS).1,6,12
MS therapies potentially influence seizure occurrence. Cortical lesions in MS have been proposed to contribute to epileptogenesis, 11 which suggests that prevention of cerebral lesions with disease-modifying therapies (DMTs) may reduce seizures. However, the true effect of DMTs on seizures in MS is unknown. Seizures have been reported as rare adverse events in clinical trials including cladribine, 13 fingolimod, 14 glatiramer acetate, 15 and interferon-beta.16–18 While there are assumed proconvulsant properties with certain DMTs, others like dimethyl fumarate and, conflictingly, fingolimod are suggested to have potential antiepileptogenic properties in preclinical studies.19,20
It is important to determine whether DMTs, which are proven to be effective in preventing relapses and disability in MS patients, influence seizure occurrence. Addressing this knowledge gap, we performed a systematic review and network meta-analysis (NMA) to identify seizure risk in MS patients on different DMTs.
Materials and methods
Standard protocol approvals and registrations
This study was registered with PROSPERO (CRD42020181687). 21 The completed review was prepared in consultation with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Extension Statement for Network Meta-Analyses.22,23
Data sources
The following databases were used: MEDLINE (OVID), Embase, CINAHL, and ClinicalTrials.gov. Articles from database inception until 21 August 2021 were considered. Additional articles were identified by screening references of identified articles and contacting authors. The MEDLINE search strategy was developed with the assistance of a health science librarian (Supplementary Table 1).
Eligibility criteria
Type of studies
All phase 2 and 3 randomized placebo-controlled trials (RCTs) examining the efficacy and safety of ⩾1 DMT for the treatment of MS were included. Studies written in non-English languages were excluded.
Trials containing arms with combination therapies, non-pharmacological or over-the-counter interventions were excluded. The open-label extension phase of trials was excluded due to the loss of randomization. Also excluded were trials only reporting adverse events at a frequency of ⩾5% and where additional details not otherwise reported in the main article were unavailable from supplementary material or by contacting the authors, given the low prevalence of seizures in MS patients.
The full list of DMT monotherapies considered for inclusion is detailed in Supplementary Table 1.
Type of participants
All adults (⩾18 years) diagnosed with MS according to any accepted diagnostic criteria24–28 were included, regardless of sex, comorbidities, MS subtype (including clinically isolated syndrome (CIS)), prior MS treatment(s), degree of disability, or disease duration.
Article and data extraction
Level 1 (title and abstract) and Level 2 (full-text) screening were performed independently by two reviewers (Y.L.D. and V.T.Y.Y.) using the Covidence Systematic Review Software. 29 Discrepancies were resolved by assessment by a third reviewer (T.K.).
A data extraction form within an Excel spreadsheet was created and completed independently by two reviewers (Y.L.D. and V.T.Y.Y.). Extracted data included article characteristics (authors, country of origin, publication year), study design (placebo-controlled follow-up duration, methodology characteristics relevant to risk of bias assessment), participant characteristics (age, sex, ethnicity, previous DMT use, MS subtype, mean time since first neurological event/diagnosis of MS, baseline EDSS), intervention details, and outcome data (number of seizures, seizure types, annualized relapse rate).
Risk of bias assessment
Risk of bias assessment was performed independently by two reviewers (Y.L.D. and V.T.Y.Y.) using an adapted version of the National Heart, Lung, and Blood Institute (NHLBI) Quality Assessment Tool for Controlled Intervention Studies 30 (Supplementary Table 2). Discrepancies were resolved by a third reviewer (T.K.).
Studies were evaluated on the adequacy of the following variables: study description, randomization methods, treatment allocation concealment, participant and provider blinding, assessor blinding to outcomes, comparability of baseline group characteristics, overall and differential dropout rates, treatment protocol adherence, avoidance of co-interventions, outcome measure assessment, power calculation, prespecified outcomes, and intention-to-treat analysis. Based on these variables, studies were given overall quality ratings of “good,” “fair,” or “poor.”
Studies with any of the following fatal flaws 30 were assessed to be “poor”: high (>20%) non-adherence rate to randomized treatment, high (>20%) total dropout rate, high differential dropout rate (> 15% between treatment groups), lack of assessor blinding, or non-intention-to-treat-analysis studies. Studies assessed as “good” fulfilled all the following criteria: clear description of a randomized trial, comparable baseline group characteristics, pre-specified outcomes, valid outcome measures, and absence of any fatal flaws. Studies which did not fall into the “good” or “poor” categories were assessed as “fair.”
Statistical analysis
All included studies were scrutinized for important differences to ensure that the transitivity assumption was upheld prior to performance of the NMA.
Assessment of between-study heterogeneity was reported as the value of I2. A funnel plot and Peters test 31 were used to assess for publication bias and small-study effects.
NMA was performed using “gemtc” package under a Bayesian framework with non-informative priors and Markov Chain Monte Carlo (MCMC) simulation,32,33 and the results were plotted using “forestplot” in R (2021.09.0 Build 351). 34 Random effects model was used for primary analysis. A binomial model with a log link function was used for all network meta-analyses. The estimation was run with a burn-in of 150,000 and sampling of 300,000 iterations from four chains of initial values. The adequacy of convergence for the MCMC simulation was visually inspected using trace plots (Supplementary Figure 1) and Gelman-Rubin diagnostics; good convergence was determined by a potential scale reduction factor < 1.05. 35
All included studies were analyzed in the primary NMA. The seizure risk compared with placebo was reported as loge seizure risk ratios (LnSRRs) with 95% credible intervals (CrIs). LnSRR < 0 represents a reduction and LnSRR > 0 represents an increase in seizure risk associated with DMT use, compared with placebo. The primary NMA was performed for individual DMTs (irrespective of dose) compared with placebo. Further analysis was performed with DMTs pooled according to their mechanism of action.
A sensitivity analysis was performed with only “non-zero” studies (i.e. studies reporting ⩾ 1 seizure in the DMT or placebo arms). Another sensitivity analysis was done using meta-analysis to assess the seizure risk in MS patients on DMT compared with placebo. The “meta” package in R was used; all studies were included using Mantel-Haenszel pooling and treatment arm continuity correction for zero studies, with mixed-effects logistic regression modeling with random study effects.
Results
Study and patient characteristics
A total of 1993 titles and abstracts were identified. After removing duplicates, 1509 articles underwent Level 1 screening, resulting in 331 full-text articles which were assessed for eligibility. 275 full-text articles were excluded; the primary reasons for exclusion are detailed in Figure 1. Ten studies were excluded due to only reporting adverse events that occurred at a frequency threshold of ⩾5% and additional details were unavailable.
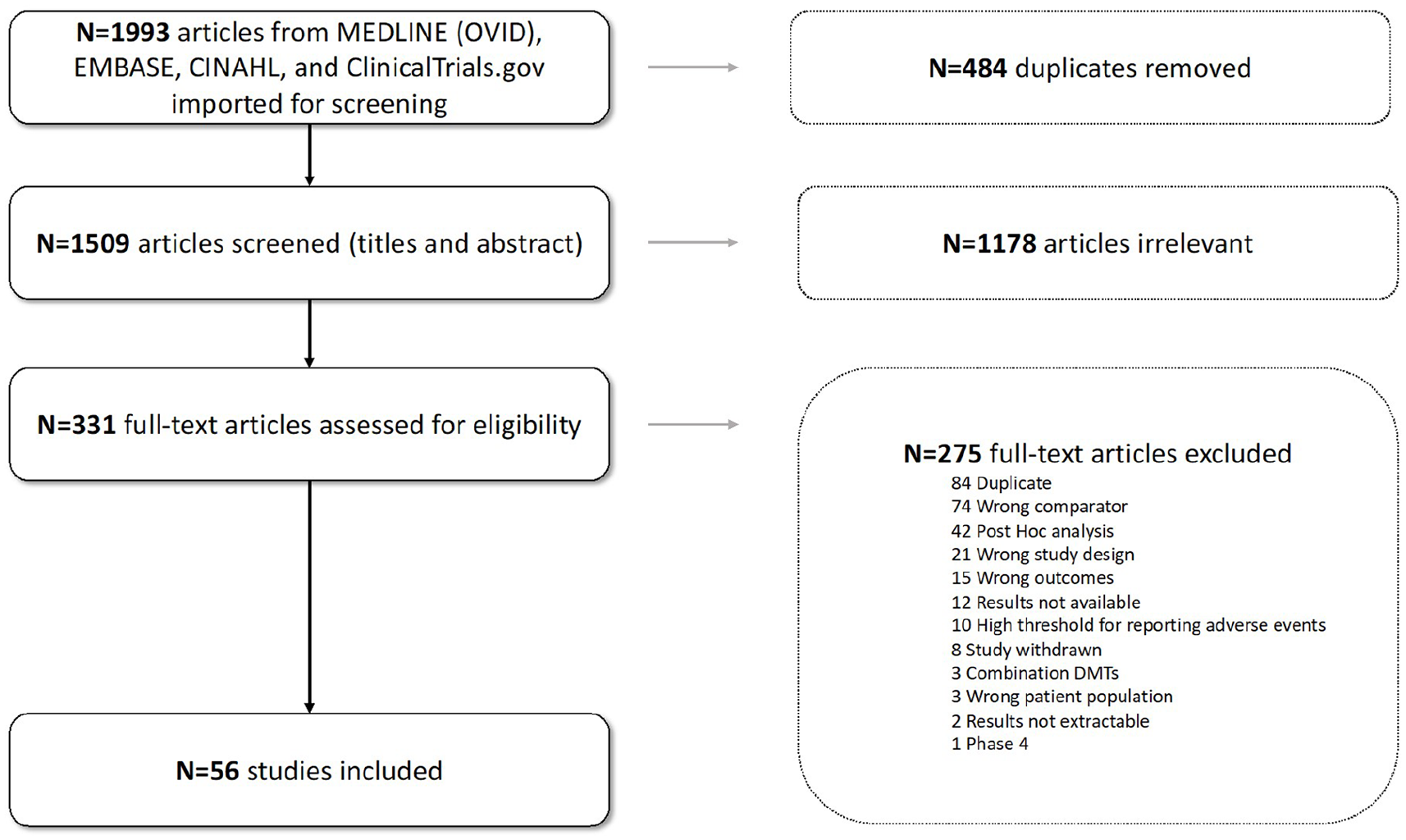
Study flow diagram.
Thus, 56 RCTs were included in the final analysis (Supplementary Table 2), comprising 29,388 patients: 18,909 randomized to DMTs and 10,479 to placebo (Table 1). Forty-five studies (80.3%) were published since 2001. Twenty-nine studies (51.8%) included relapsing-remitting MS patients only, 13 studies included progressive MS only, 4 studies included CIS only, and 8 studies included relapsing-remitting and progressive MS. Forty-six studies (82.2%) included >100 patients. In 34 studies (60.7%), the placebo-controlled follow-up was >48 weeks.
Study and patient characteristics.
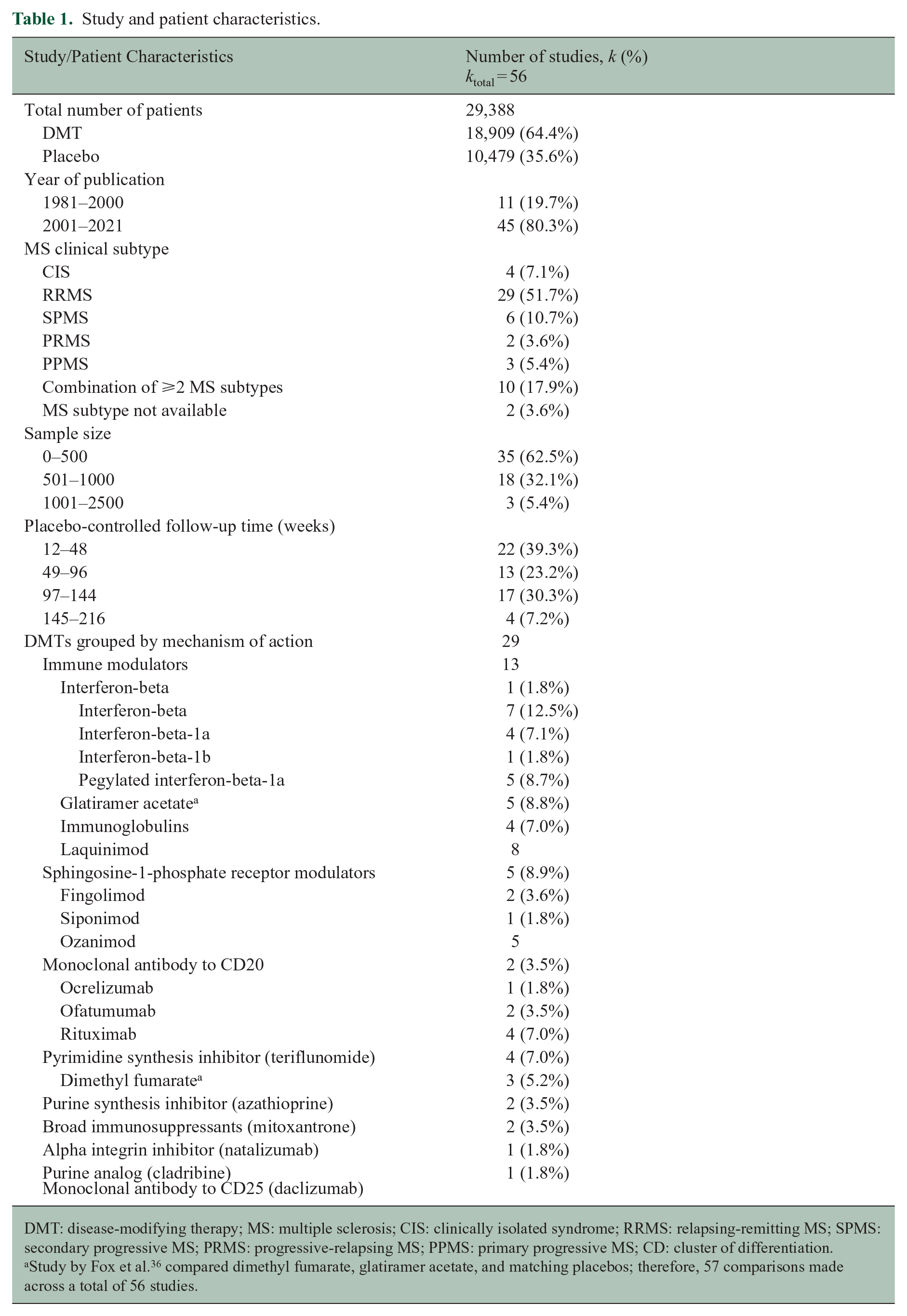
DMT: disease-modifying therapy; MS: multiple sclerosis; CIS: clinically isolated syndrome; RRMS: relapsing-remitting MS; SPMS: secondary progressive MS; PRMS: progressive-relapsing MS; PPMS: primary progressive MS; CD: cluster of differentiation.
Study by Fox et al. 36 compared dimethyl fumarate, glatiramer acetate, and matching placebos; therefore, 57 comparisons made across a total of 56 studies.
When grouped according to mechanism of action, there were 13 studies which included interferons (interferon-beta (1), interferon-beta-1a (7), interferon-beta-1b (4), pegylated interferon-beta-1a (1)), eight which included sphingosine-1-phosphate receptor modulators (fingolimod (5), siponimod (2), ozanimod (1)), and five studies which included CD20 monoclonal antibodies (rituximab (2), ocrelizumab (2), ofatumumab (1)).
Quality assessment
Twenty-five studies were assessed to be of “good” quality, 11 “fair,” and 20 “poor.” Reasons for “poor” study quality included poor adherence to randomized treatment (15), high total dropout rate (8), high differential dropout rate (4), inadequate efficacy evaluator blinding (1), and non-intention-to-treat analysis (2) (Supplementary Table 2).
Between-study heterogeneity and small study effects
The I2 value for the included studies was 0% (95% confidence interval 0.0%–31.0%).
The funnel plot did not demonstrate asymmetry and Peters test (intercept = −553.10, t = −1.01, p = 0.32) suggested against any significant between-study heterogeneity or small-study effects (Supplementary Figure 2).
Seizure risk: individual DMTs
Sixty seizures were reported over 53,443 patient-years (DMT = 41; placebo = 19) across all included studies, representing a seizure incidence of 112.27 seizures per 100,000 patient-years.
The NMA included 56 RCTs comparing ⩾ 1 DMTs with placebo (Figure 2). One study included two arms of DMT monotherapy—dimethyl fumarate and glatiramer acetate. 36
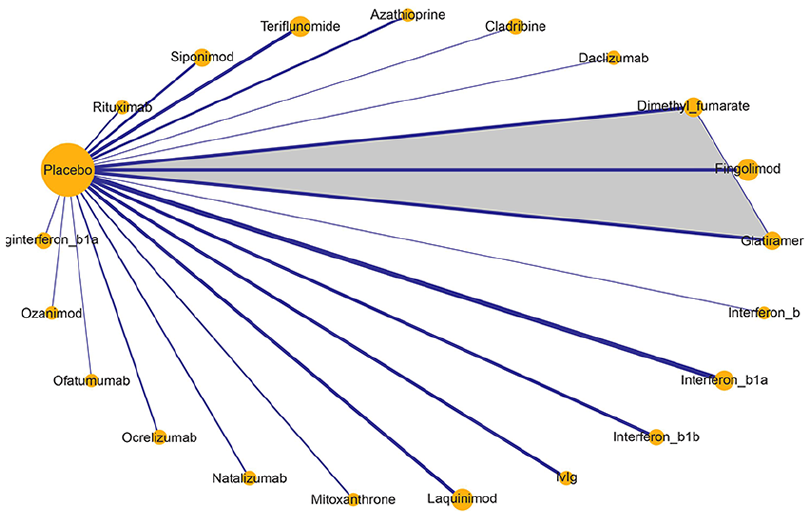
Network plot for disease-modifying therapies (DMT) (individual doses pooled) versus placebo.
None of the DMTs were associated with significant change in LnSRR (Figure 3). The exceptions were daclizumab (−17.90 [95% CrI −65.31; −0.65]) and rituximab (−24.86 [95% CrI −82.71; −1.37]), which trended toward lower LnSRR. Only one study contributed to the result for daclizumab. 37 Two DMTs trended toward higher LnSRR—cladribine (25.78 [95% CrI 0.94; 84.65])) and pegylated interferon-beta-1a (25.40 [95% CrI 0.78; 85.47]), with only one study for each.38,39 It should be noted that the 95% CrIs were wide for all observed potential associations.
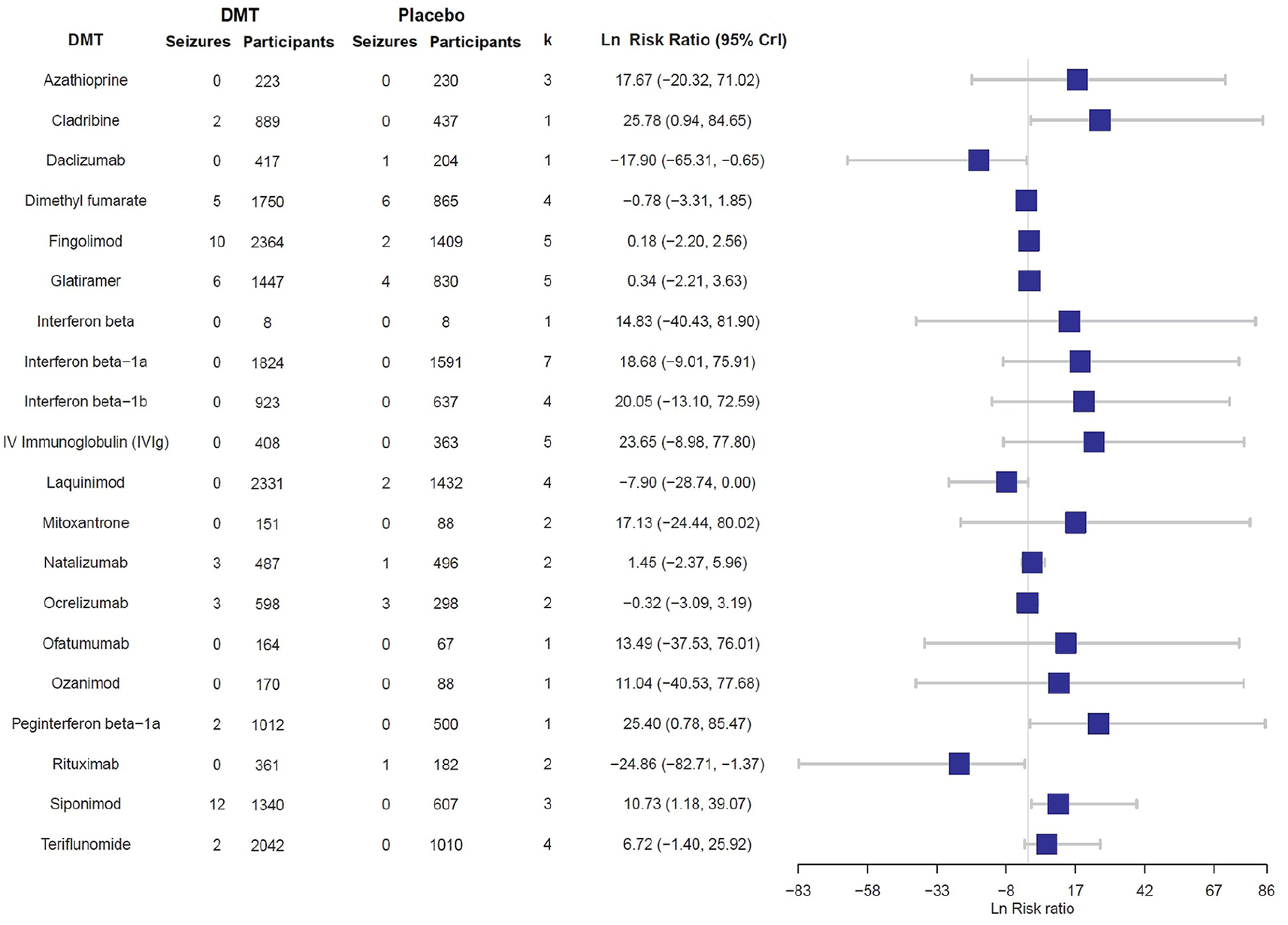
NMA forest plot for LnSRR in MS patients on DMT compared with placebo.
Twelve seizures occurred in one trial which includes siponimod 2 mg daily, 40 corresponding to one seizure in 276.25 patient-exposed-years. No seizures were reported in another study investigating siponimod at doses up to 10 mg daily. 41 Together, the studies of siponimod did not find evidence for association between siponimod and the risk of seizures.
Seizure risk: pooled DMTs
NMA for DMTs pooled by mechanism of action was performed (Figure 4). The apparent reduced seizure risk associated with rituximab was no longer observed—the LnSRR for CD20 monoclonal antibodies was −1.04 [95% CrI −4.05; 1.97]. The LnSRR for interferon-beta was 21.46 [95% CrI 0.85; 71.22]. However, this observation needs to be interpreted with caution because the 95% CrI for this observation was very wide, and seizures were only observed in one out of the 13 included studies—of pegylated interferon-beta-1a. 39
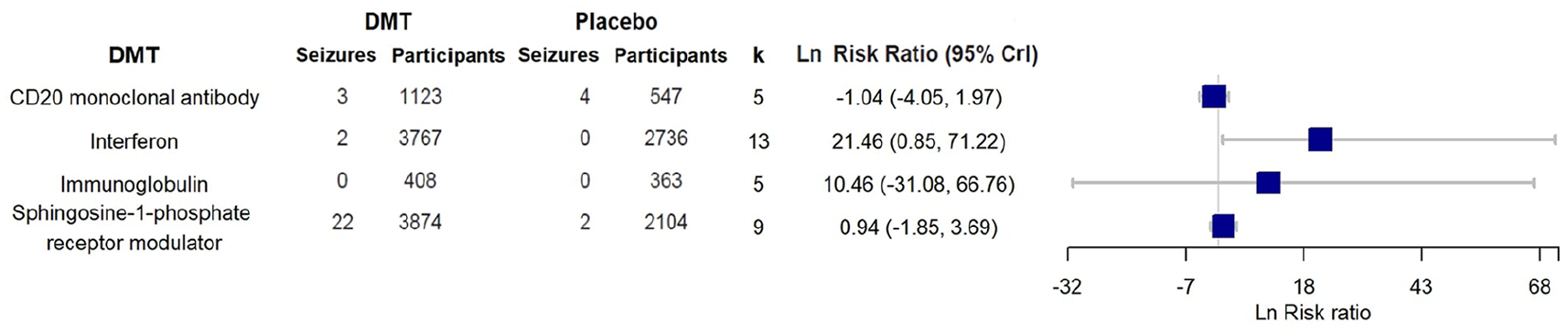
NMA forest plot for LnSRR according to DMT mechanism of action groups compared to Placebo.
Sensitivity analyses
Standard meta-analysis (all studies)
Meta-analysis with random effects model was performed for all studies comparing DMTs with placebo (Figure 5). As a group, the studies did not find evidence for association between DMTs and seizure risk (−0.15 [95% CrI −0.59; 0.30]).

Meta-analysis using random effects model for seizure risk in DMT versus placebo, all studies.
Meta-analysis of “non-zero” studies
Meta-analysis with random effects model performed for 16 “non-zero” studies found no evidence of difference in the LnSRR between the pooled DMTs and placebo (−0.28 [95% CrI −0.90; 0.33]) (Figure 6). In addition, none of the individual DMTs in the “non-zero” studies were found to have an altered LnSRR compared with placebo. Notably, this included pegylated interferon-beta-1a (0.90 [95% CrI −2.13; 3.93]).
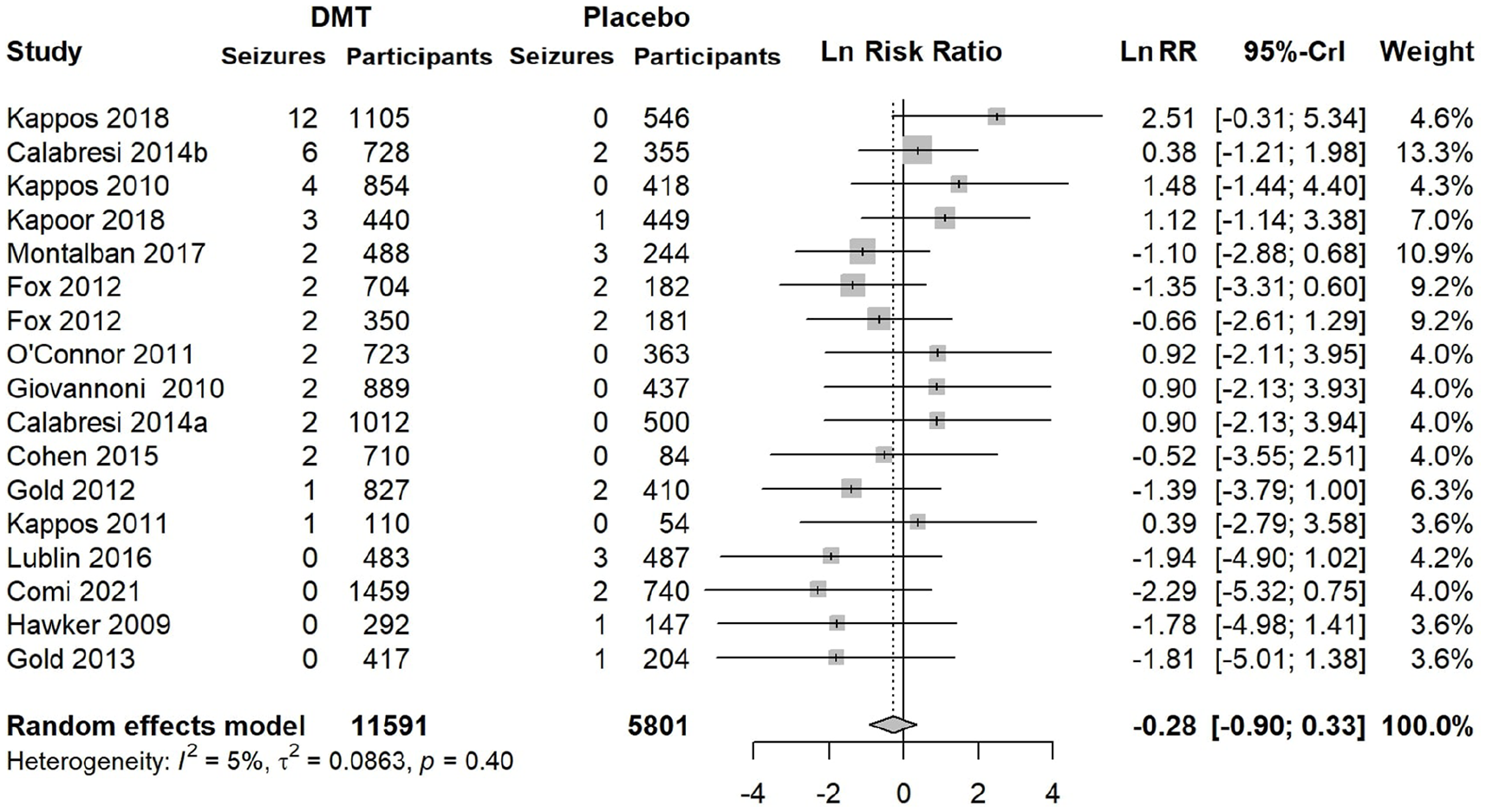
Meta-analysis using random effects model for seizure risk in DMT versus placebo, non-zero studies.
Discussion
This systematic review and NMA of 56 RCTs of 20 DMTs (totaling 29,388 patients) did not find any compelling evidence of altered seizure risk in patients treated with DMTs compared with placebo, either as individual or pooled therapies. A potential exception to this is pegylated interferon-beta-1a, where the risk of seizures may be higher among the treated patients, but this was only seen in one trial and was not observed for other interferon formulations.
Seizures are rare events, and the reported incidence depends on reporting standards and is likely to vary among trials. Incidence rates of 61.44 seizures per 100,000 person-years 2 in the general population and 349 per 100,000 person-years in MS patients have been described elsewhere. 42 From the trials included in this NMA, the seizure incidence was 112.27 per 100,000 person-years in MS patients.
In this study, four DMTs trended toward an altered seizure risk. Daclizumab and rituximab trended toward a reduced seizure risk, whereas cladribine and pegylated interferon-beta trended toward an increase in seizure risk. However, these results need to be interpreted with caution as they were derived from single studies in all cases except rituximab. Other studies of interferon-beta did not show an association with seizure risk. Nevertheless, the Food and Drug Administration (FDA) has issued a caution of seizure being a rare adverse event in treatment with interferon-beta.16–18,43 This is in keeping with results from a retrospective analysis of seizures in a cohort of 1267 MS patients, in which 45% of the 22 individuals identified with epilepsy were previously treated with interferon-beta. 44 However, the temporal relationship between interferon-beta use and seizures in this study was unclear, and the relationship between recipients of other DMTs in this study and seizures was not mentioned. Of note, daclizumab has since been withdrawn from the global market due to significant post-marketing reports of side effects including liver toxicity and severe inflammatory brain disorder.45,46
The trend for reduced seizure risk initially seen with rituximab was not reproducible when the analysis was repeated with rituximab pooled with other CD20 monoclonal antibodies. There were no baseline patient factors in the included trial cohorts that would account for this difference. Conceivably, rituximab, a murine-human chimeric and the first CD20 monoclonal antibody developed for MS, may have subtle differences compared with newer generations of CD20 monoclonal antibodies such as the humanized (ocrelizumab) and the fully human (ofatumumab) therapies, 47 which could account for the different seizure risk. In limited published case series and reviews, rituximab has demonstrated efficacy in the treatment of specific drug-refractory seizures with implicated immune mechanisms such as Rasmussen’s encephalitis and new-onset refractory status epilepticus.48,49
Cladribine was found to have an increased LnSRR, but this finding was only derived from a single study which included 870 participants randomized to either oral cladribine 3.5 or 5.25 mg/kg and 456 participants randomized to placebo. 38 Two seizures were recorded in the cladribine groups—one described as “convulsion” on 3.5 mg/kg oral cladribine and one as “epilepsy” on 5.25 mg/kg oral cladribine—whereas no seizures occurred in the placebo arm. The occurrence of seizure in cladribine-treated patients at 0.3% compared with 0% in placebo in clinical studies was noted by the FDA; however, it concluded that it remains unknown whether the recorded seizures were related to the effects of MS, to cladribine, or to a combination of both. Furthermore, seizures have also been identified as a rare adverse event in non-neurological use of parenteral cladribine and other purine analogs. 50
Some studies have suggested an association between MS cortical or subcortical lesions with epilepsy. If MS lesions and active inflammation are implicated in the pathogenesis of seizures in MS, then reduction of cortical lesions and inflammation by use of DMTs may reduce seizure risk. However, this relationship has not been described in any human studies. When comparing all DMTs as a group with placebo, both the NMA and meta-analysis did not find a statistical difference in the seizure risk.
Aside from multiple sclerosis and DMT use, other comorbidities and co-medication use may alter seizure risk. However, the limited scope of the RCTs included meant that information about other baseline risk factors for seizures was not available. The reporting of seizure events was not harmonized among the included trials, with varied terminology used such as “grand mal seizure” and “convulsions”—at times, the term “epilepsy” was used. However, it was not possible to determine whether this truly represented the occurrence of seizure in a patient who had epilepsy prior to intervention versus an incident seizure during the RCT. In addition, it was not clear whether the reported seizures were unprovoked or acute symptomatic.
Strengths and limitations
Seizure risk in MS patients treated with DMTs has not been previously investigated in a systematic manner, mainly due to its rarity. The use of high-quality data pooled from a large number of RCTs provides an ideal setting for investigating this rare but clinically relevant phenomenon. We chose to base this search on an a priori published protocol in accordance with PROSPERO guidelines. The use of NMA allowed for comparison across multiple studies included on objective criteria, including data from almost thirty-thousand patients, enabling incorporation of indirect evidence based on the assumption of transitivity with a single reference category (placebo).
Incomplete reporting of adverse events may render this meta-analysis vulnerable to reporting bias. Therefore, we applied lenient inclusion of trials which reported adverse events, unless it was explicitly stated that adverse events were only reported at a threshold frequency above that in which seizures would be unreliably captured and additional information was otherwise unavailable. Only 10 studies were excluded for this reason.
Furthermore, we have carried out a sensitivity analysis with non-zero-event studies. In addition, our analysis excluded non-randomized post-marketing data. Some consumer information for interferons mention “a high incidence of seizures,” potentially suggesting that longer follow-up is required before an effect of DMTs on seizure frequency can be observed.
Finally, for many DMTs, the seizure risk ratio was based on a small number of trials—including cladribine and daclizumab. Because these trials were not powered to identify differences in seizure frequency, such results should be cautiously interpreted.
Conclusion
No evidence of association was found between DMT use and seizure risk in MS patients. This suggests DMTs’ effects on central nervous system inflammation do not correspond to seizure risk reduction, at least in the intermediate term. Whether seizures are preventable over the long-term remains unclear. Regardless, DMTs are not associated with increased seizure risk, which is an important message for managing seizures and counseling patients treated with DMT.
Supplemental Material
sj-docx-1-msj-10.1177_13524585231151400 – Supplemental material for Seizure risk in multiple sclerosis patients treated with disease-modifying therapy: A systematic review and network meta-analysis
Supplemental material, sj-docx-1-msj-10.1177_13524585231151400 for Seizure risk in multiple sclerosis patients treated with disease-modifying therapy: A systematic review and network meta-analysis by Yew Li Dang, Vivien TY Yong, Sifat Sharmin, Piero Perucca and Tomas Kalincik in Multiple Sclerosis Journal
Footnotes
Author contributions
Dr Dang and Dr Yong contributed equally as co-first authors. Dr Dang and Dr Yong had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Conception and design of the study: Dang, Perucca, and Kalincik. Acquisition of data: Dang and Yong. Statistical analysis: Dang, Yong, and Sharmin. Drafting of the manuscript: Dang and Yong. Critical revision of the manuscript for intellectual content: Dang, Yong, Sharmin, Perucca, and Kalincik. Study supervision: Perucca and Kalincik.
Data availability
Primary data extracted from included studies, data used for analyses, and analytic codes are available on reasonable request from the corresponding author.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Dang is supported by the National Health and Medical Research Council (NHMRC) of Australia and has received speaker honoraria from Eisai, outside the submitted work. Dr Yong is supported by the Neurological Foundation (registered New Zealand charitable entity) and has no conflicts of interest to disclose. Dr Sharmin has no conflicts of interest to disclose. Dr Perucca is supported by an Early Career Fellowship from the NHMRC (APP1163708), the Epilepsy Foundation, the Royal Australasian College of Physicians, The University of Melbourne, Monash University, the Weary Dunlop Medical Research Foundation, Brain Australia, and the Norman Beischer Medical Research Foundation. He has received speaker honoraria or consultancy fees to his institution from Chiesi, Eisai, LivaNova, Novartis, Sun Pharma, Supernus, and UCB Pharma, outside the submitted work. He is an Associate Editor for Epilepsia Open. Dr Kalincik served on scientific advisory boards for MS International Federation and World Health Organization, BMS, Roche, Janssen, Sanofi Genzyme, Novartis, Merck and Biogen, steering committee for Brain Atrophy Initiative (Sanofi Genzyme), received conference travel support and/or speaker honoraria from WebMD Global, Eisai, Novartis, Biogen, Roche, Sanofi Genzyme, Teva, BioCSL, and Merck and received research or educational event support from Biogen, Novartis, Genzyme, Roche, Celgene, and Merck.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.