
Abstract
Background:
Multiple sclerosis misdiagnosis remains a problem despite the well-validated McDonald 2017. For proper evaluation of errors in the diagnostic process that lead to misdiagnosis, it is adequate to incorporate patients who are already under regular follow-up at reference centers of demyelinating diseases.
Objectives:
To evaluate multiple sclerosis misdiagnosis in patients who are on follow-up at a reference center of demyelinating diseases in Brazil.
Methods:
We designed an observational study including patients in regular follow-up, who were diagnosed with multiple sclerosis at our specialized outpatient clinic in the Hospital of Clinics in the University of Sao Paulo, from 1996 to 2021, and were reassessed for misdiagnosis in 2022. We evaluated demographic information, clinical profile, and complementary exams and classified participants as “established multiple sclerosis,” “non-multiple sclerosis, diagnosed,” and “non-multiple sclerosis, undiagnosed.” Failures in the diagnostic process were assessed by the modified Diagnostic Error Evaluation and Research tool.
Results:
A total of 201 patients were included. After analysis, 191/201 (95.02%) participants were confirmed as “established multiple sclerosis,” 5/201 (2.49%) were defined as “non-multiple sclerosis, diagnosed,” and 5/201 (2.49%) were defined as “non-multiple sclerosis, undiagnosed.”
Conclusions:
Multiple sclerosis misdiagnosis persists in reference centers, emphasizing the need for careful interpretation of clinical findings to prevent errors.
Keywords
Introduction
Multiple sclerosis (MS) is the most common demyelinating autoimmune disease of the central nervous system (CNS) and is one of the leading causes of non-traumatic neurological disability in the young population. 1 In 2016, there were 2,221,188 estimated cases of MS globally. 2 In Brazil, the estimated prevalence of MS has been reported to range from 1.36/100,000 inhabitants in the northeast region 3 to 27.2/100,000 inhabitants in the southern region. 4 In the city of Sao Paulo (southeast region), the estimated prevalence is 15/100,000 inhabitants. 5
Efforts to develop MS diagnostic criteria, including McDonald 2017 revisions, 6 have enabled earlier diagnosis of MS. However, misdiagnosis remains a problem that has significant implications for patients, their providers, and healthcare systems.7,8 There are recent studies discussing a series of patients who were diagnosed with MS earlier in their lives, but after being referred to specialized centers, their diagnoses were revised to other conditions or reconsidered as a possible diagnosis of MS. Before MRI was integrated into the MS diagnostic criteria, Poser 9 described an erroneous diagnosis of MS in 35% of cases referred to his clinic. After the development of the McDonald criteria, studies that included patients referred to specialized centers of demyelinating diseases with an established MS diagnosis8,10–12 or suspected MS diagnosis8,13 for evaluation had misdiagnosis rates ranging from 7.1% to 26%.
However, there is a notable lack of reports that assess misdiagnosis rates among patients who are already under regular follow-up at reference centers of demyelinating diseases with the diagnosis of MS. Adequate evaluation of errors in the diagnostic process that lead to misdiagnosis should include patients who are under regular follow-up at reference centers. In addition, most of the prior MS misdiagnosis studies were predominantly conducted in North America,7,10 Europe,11,13 and Asia. 8 We found only one study carried out in Buenos Aires, Argentina, 12 reemphasizing that misdiagnosis data is less known in South America, a region with higher prevalence of non-MS demyelinating diseases such as anti-aquaporin 4 antibodies (anti-AQP4) positive neuromyelitis optica spectrum disorders (NMOSD) 14 and tropical infectious diseases that may mimic demyelinating diseases such as schistosomiasis and human T-lymphotropic virus type 1 (HTLV-1).15,16 We aimed to evaluate the prevalence, clinical, radiological, and laboratory predictors of MS misdiagnosis in patients who are regular on follow-up at a reference demyelinating diseases center in Brazil.
Materials and methods
We designed an observational study including patients who were diagnosed with MS at our specialized center in the Hospital of Clinics at the University of Sao Paulo from 1996 to 2021 and who were still undergoing regular follow-up at our clinic during the study period in 2022. Our neuroimmunology MS center comprises five outpatient clinics. There are no epidemiological or clinical differences among the profiles of these clinics. We randomly chose one of the five clinics and reassessed misdiagnosis in patients in 2022. The study received the approval of the local ethics committee, and it was conducted in accordance with the ethical principles outlined in the World Medical Association Declaration of Helsinki.
Inclusion criteria comprised diagnosis of MS, minimum age of 18 years old, and regular follow-up for at least 1 year. Patients who were never diagnosed with MS at our center were excluded.
At least two neurologists (EMST, GDS, MBO, MGPS, GAP, IGC, BBC, NTM, LST, TA, SLAP, and DC) who have received fellowship training in neuroimmunology and demyelinating diseases evaluated each participant in person during the patient’s own scheduled routine consultation, between April 1, 2022, and September 30, 2022. All participants were submitted to evaluation through clinical history, neurologic examination with Extended Disability Status Scale, and laboratory examinations including complete blood count, aspartate transaminase, alanine transaminase, γ-glutamyltransferase, kidney profile, antinuclear antibodies, extractable nuclear antibodies, homocysteine, antithyroid antibodies, antiphospholipid antibodies, vitamin B12, folate, erythrocyte sedimentation rate, C-reactive protein and urine examination, and cerebrospinal fluid (CSF) examinations including cell count, total proteins, and immunoglobulin G oligoclonal bands (IgG-OCB) according to the RIREMS (Rising Italian Researchers in Multiple Sclerosis) protocol. 13 If a participant exhibited clinical and/or radiological characteristics with potential overlap between MS, NMOSD, and myelin oligodendrocyte glycoprotein (MOG) associated disease, tests for anti-AQP4 and anti-MOG antibodies using the cell-based assay into live HEK-293 cells 17 were performed. Visual evoked potentials (VEP) were performed only if there was doubt between optic neuritis and other conditions causing visual symptoms. The attending neurologists were responsible for determining whether to do these tests or not.
Patients also underwent an assessment through magnetic resonance imaging (MRI), which was interpreted and reported by 2 MS neuroradiologists with 7 (DMN) and 14 (CMR) years of experience. Both were blinded to the clinical diagnosis and serological data. MRI was acquired using 1.5-tesla scanners. The brain protocol comprised fluid-attenuated inversion recovery (FLAIR) with sagittal 3D-FLAIR sequences and axial T1- and T2-weighted imaging (WI) fast spin echo (FSE) sequences. The orbit protocol comprised axial, coronal T1WI, T2WI FSE, and a coronal T2 short-tau inversion recovery (STIR) sequence. The spinal cord protocol comprised axial, sagittal T1WI, T2WI FSE, and a sagittal T2 STIR sequence. Finally, T1WI FSE postcontrast imaging of the brain, spinal cord, and orbit was acquired.
Participants were classified as having “established MS” when McDonald 2017 diagnostic criteria for MS were met after reasonable exclusion of alternative diagnoses, “non-MS, diagnosed,” which included individuals with clinical manifestations and MRI findings not indicative of MS, resulting in a definitive diagnosis, and “non-MS, undiagnosed,” which comprised cases where clinical manifestations and MRI findings did not suggest MS, but, due to the absence of supporting data such as normal or non-specific MRI results, inconclusive MRI findings, or insufficient paraclinical data, a final diagnosis could not be reached.
After the investigation, the frequency of misdiagnosis was assessed, and conditions misdiagnosed as MS were listed. Demographic and clinical data were documented. MRI findings were classified as normal, non-specific lesions, and MS-suggestive lesions. The presence or absence of IgG-OCB was evaluated.
To identify the main causes of failures in the diagnostic process, we utilized the modified Diagnostic Error Evaluation and Research (DEER). This tool is a seven-step taxonomy, developed to delineate stages in the diagnostic process, including access and presentation, history taking/collection, the physical exam, testing, assessment, referral, and follow-up. The taxonomy identifies where in the diagnostic process the failures occur. 18
Results
In total, 207 patients were evaluated and had their clinical history and exams reviewed in our outpatient clinic during the study period. Six participants were excluded because they did not have a diagnosis of MS. Of the 201 individuals left, all of them had received the diagnosis of MS at some point during follow-up in the Hospital of Clinics of the University of Sao Paulo from 1996 to 2021 and were included in the study. The patients were diagnosed at different times using various diagnostic criteria for MS, including the Barkhof criteria and various revisions of the McDonald criteria. Despite differences among these criteria, we believe that they did not significantly impact diagnostic accuracy in our patient cohort.
After extensive analysis, 191/201 (95.02%) participants were confirmed as “established MS.” Of the 10/201 (4.98%) remaining participants, 5/201 (2.49%) were defined as “non-MS, diagnosed” and 5/201 (2.49%) were defined as “non-MS, undiagnosed” (Figure 1). Notably, 4 participants were considered “non-MS, diagnosed” and 3 individuals of the “non-MS, undiagnosed” group were already under investigation for other conditions due to suspected misdiagnosis in the last years (2–8 past years), although these patients continued to receive follow-up care with the diagnosis of MS and were utilizing DMT during the study period. Demographic characteristics, clinical syndromes, complementary exams, fulfillment of McDonald 2017 criteria, and diagnoses of the 10 participants with “non-MS, diagnosed” and “non-MS, undiagnosed” are presented in Table 1.
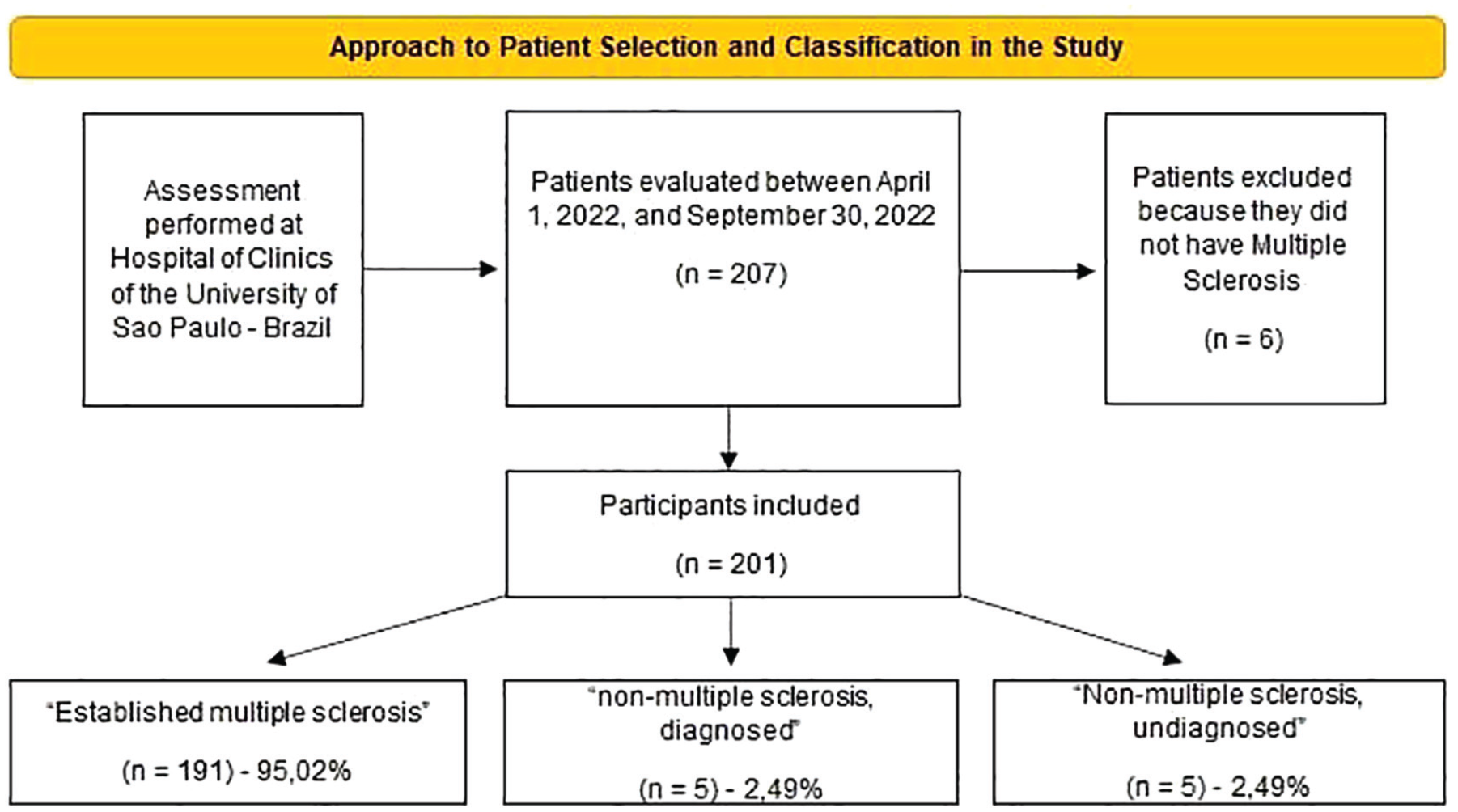
Approach to patient selection and classification in the study.
Demographic characteristics, clinical syndromes, complementary exams, fulfillment of McDonald 2017 criteria, previously diagnosed multiple sclerosis (MS) phenotypes, and final diagnoses of the 10 participants with “non-MS, diagnosed” and “non-MS, undiagnosed.”
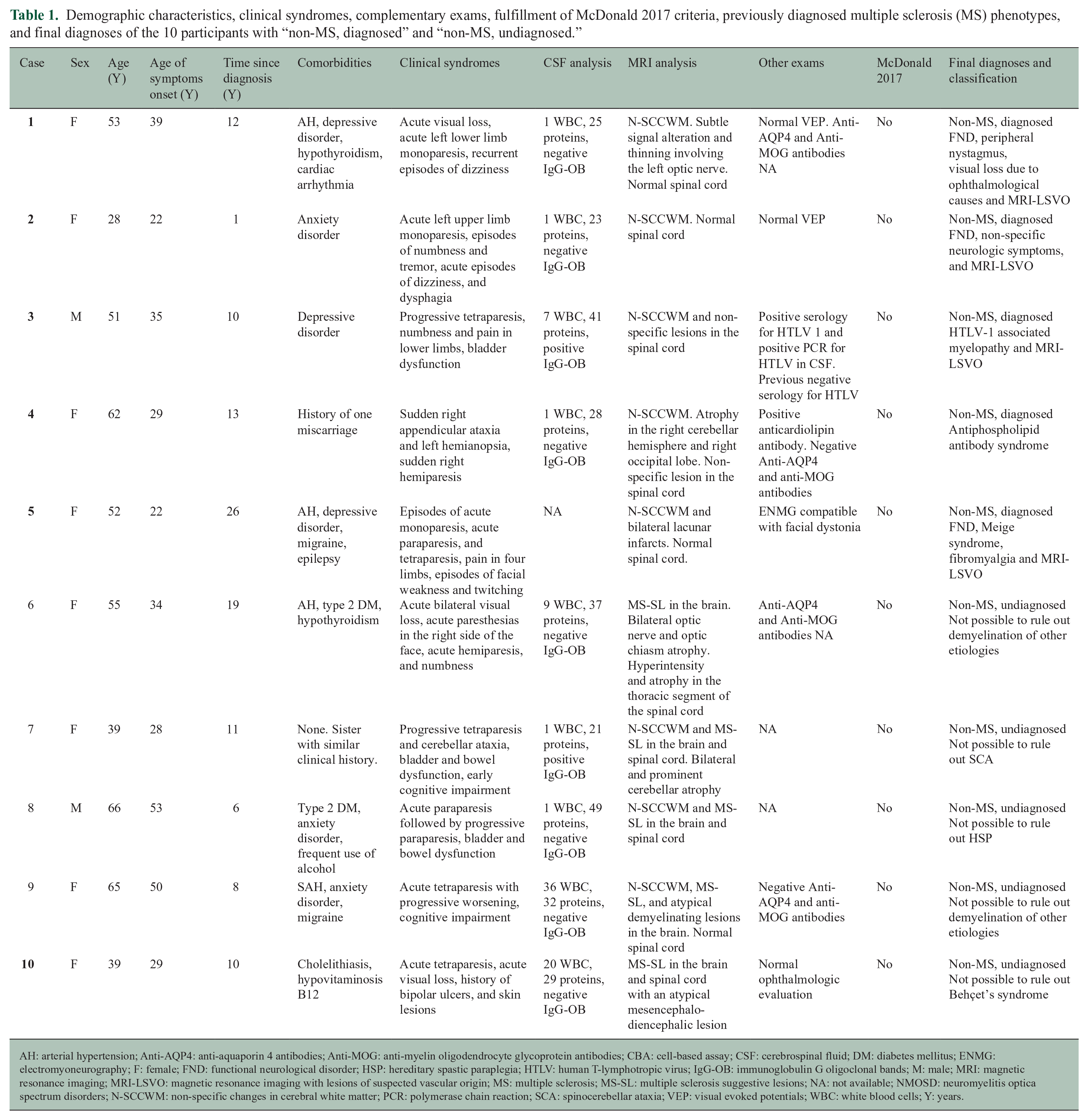
AH: arterial hypertension; Anti-AQP4: anti-aquaporin 4 antibodies; Anti-MOG: anti-myelin oligodendrocyte glycoprotein antibodies; CBA: cell-based assay; CSF: cerebrospinal fluid; DM: diabetes mellitus; ENMG: electromyoneurography; F: female; FND: functional neurological disorder; HSP: hereditary spastic paraplegia; HTLV: human T-lymphotropic virus; IgG-OB: immunoglobulin G oligoclonal bands; M: male; MRI: magnetic resonance imaging; MRI-LSVO: magnetic resonance imaging with lesions of suspected vascular origin; MS: multiple sclerosis; MS-SL: multiple sclerosis suggestive lesions; NA: not available; NMOSD: neuromyelitis optica spectrum disorders; N-SCCWM: non-specific changes in cerebral white matter; PCR: polymerase chain reaction; SCA: spinocerebellar ataxia; VEP: visual evoked potentials; WBC: white blood cells; Y: years.
Participants with misdiagnosis had a mean age of 50.9 years (range: 28–66) and had a female predominance (80%, 8/10). The mean age at symptom onset was 34.1 years (range: 22–53) and 3 participants had symptoms onset after 35 years. Time of misdiagnosis ranged from 1 to 26 years, with an interquartile range of 5 years. Acute limb weakness (80%, 8/10), followed by progressive pyramidal symptoms (40%, 4/10) and acute visual loss (30%, 3/10) were the most common clinical syndromes among the participants with misdiagnosis. The temporal profile of “acute symptoms” was defined to encompass a duration ranging from 6 to 48 hours. 19 CSF pleocytosis was present in 4/9 (44.4%) participants, and IgG-OCB was present only in 2/9 (22.2%) cases. One participant refused to undergo a lumbar puncture due to apprehension regarding the procedure. Non-specific changes in cerebral white matter in the MRI were present in 8/10 participants (80%).
During the assessment of failures in the diagnostic process using the DEER tool, 18 30% (3/10) of patients experienced failure points during the evaluation of clinical history. Among these, two individuals had a misinterpretation of their history data. Case 4 (Figure 2) had sudden clinical events and the first episode was a common vascular syndrome of the posterior fossa, and Case 5 had episodes of facial weakness and twitching that were related to Meige syndrome. In addition, in Case 10, there was a delay in providing a piece of history data once the investigation into bipolar ulcers and skin lesions suggestive of Behçet’s syndrome was performed at a later stage in the progression of the disease.
Brain and spine magnetic resonance imaging (MRI) of Case 4. (a and b) Brain MRI sagittal fluid-attenuated inversion recovery (FLAIR) images showing hyperintense non-specific lesions involving subcortical and juxtacortical regions, probably related to vascular origin. (c) Brain MRI T2 images revealing atrophy in the right cerebellar hemisphere, attributed to a previous cerebrovascular ischemic event. (d) Spinal cord MRI T2 sagittal images showing a single non-specific lesion in the cervical (C5 C6) segment. These findings were later attributed to antiphospholipid syndrome.
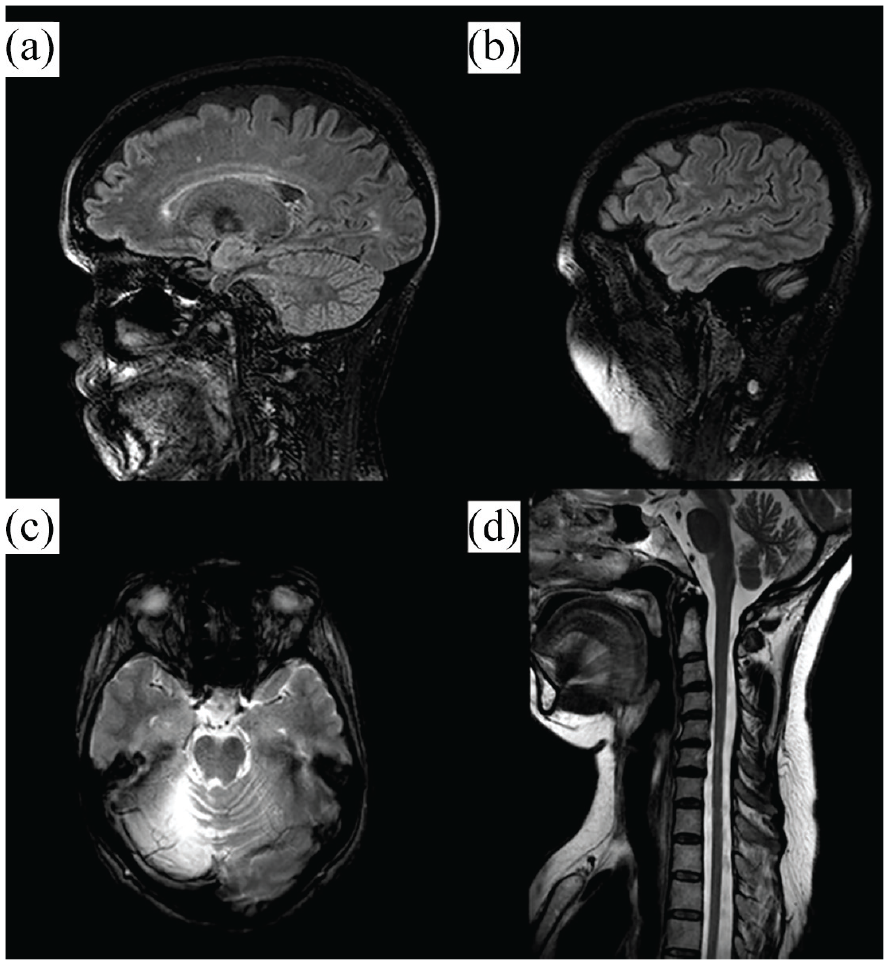
Failure points in physical examination were found in 40% of the participants (4/10). This was primarily attributed to inaccurate or missed physical examination findings in previous assessments. Three individuals had examination findings that were not correlated to lesions on MRI, and all of them had clinical assessments consistent with functional neurological disorder that was initially considered to correspond to an organic pattern. Case 1 (Figure 3) and Case 5 displayed limb falls that were correlated with non-pyramidal patterns. Case 1 also presented peripheral nystagmus that was initially considered to be of a central pattern, along with acute visual loss in the left eye that was attributed to possible optic neuritis at the beginning of follow-up, but after reassessment, an ophthalmological etiology was identified. In addition, oral ulcers observed in Case 10 were not evaluated in previous examinations.
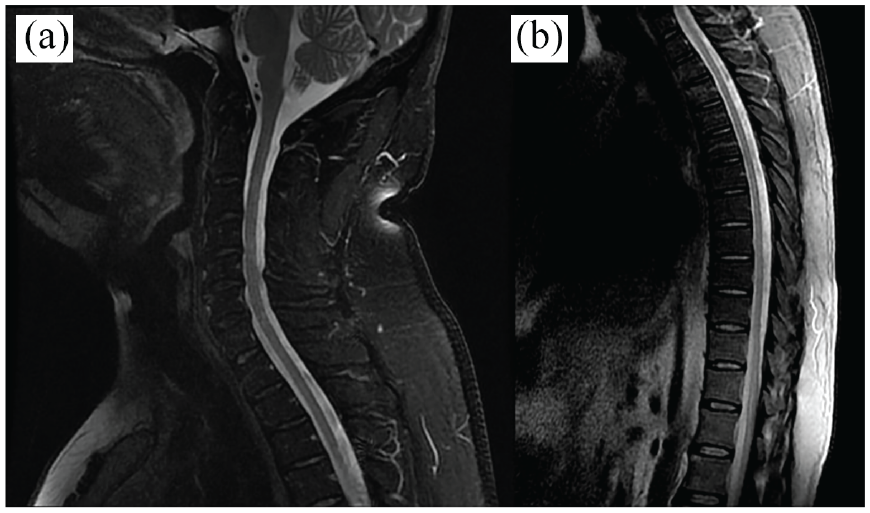
Brain and spine magnetic resonance imaging (MRI) of Case 1. (a) Spinal cord MRI T2-STIR (Short tau inversion recovery) sagittal images revealing the cervical segment without demyelinating lesions. (b) Brain MRI with sagittal fluid-attenuated inversion recovery (FLAIR) images, showing multiple hyperintense non-specific lesions involving periventricular and subcortical regions, probably related to vascular origin. (c) Orbit MRI with coronal T2-STIR images, showing a subtle signal alteration and thinning involving the left optic nerve, which was erroneously overestimated as indicative of optic neuritis in the initial evaluation. The patient received a diagnosis comprising different conditions, namely, peripheral pattern nystagmus, visual loss resulting from ophthalmological conditions, and functional neurological disorder, in association with the observed abnormal MRI.
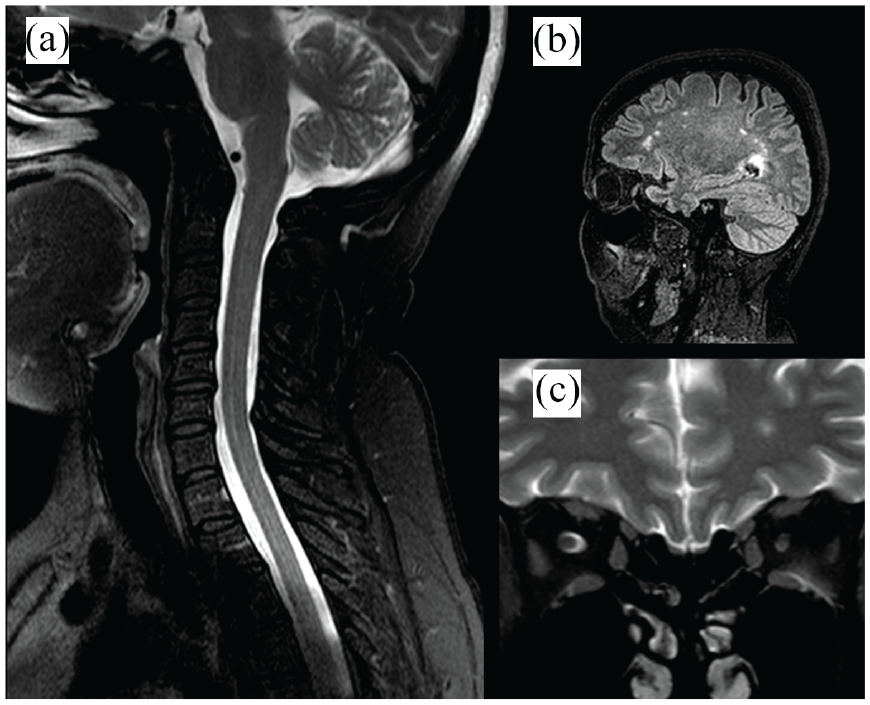
In the assessment of complementary investigations, all patients had failure points during the MRI analysis due to misinterpreted tests. Notably, 8 out of 10 (80%) individuals (except Cases 6 and 10) had non-specific lesions that were earlier considered typical of MS. Three of these patients (Cases 7–9) exhibited both typical MS lesions as well as non-specific lesions. Case 6 had typical lesions, but which could also be related to NMOSD, along with a bilateral optic nerve and optic chiasm atrophy. Case 10 had only typical lesions as well, but which could also be related to Behçet’s syndrome. In the initial MRI evaluation of Case 1, an overestimation of a subtle signal alteration and thinning involving the left optic nerve was observed. Of note, the medical request was formulated based on the hypothesis of optic neuritis, which potentially contributed to a misinterpretation. Moreover, four participants did not undergo all the necessary workup exams to assess other potential differential diagnoses, as AQP4-IgG and MOG-IgG antibodies were unavailable in two cases where they would be beneficial, and genetic testing was also not available for two other participants. Case 3 (Figure 4) had a false negative result in the first examination of HTLV-1 serology, which was later confirmed as positive during the follow-up, along with a positive polymerase chain reaction result in the CSF.
Spine MRI of Case 3. (a) MRI of the cervical segment of the spinal cord with T2-STIR sagittal images. (b) MRI of the thoracic segment of the spinal cord with T2 sagittal images revealing non-specific and poorly delimitated hyperintense foci, in addition to spinal atrophy. These findings were later attributed to Human T-lymphotropic virus type 1 infection. Unfortunately, MRI brain images were external and unavailable to include in this study.
All cases in our study may have exhibited challenges or delays in hypothesis generation, as it is difficult to ascertain the exact thought process of physicians during the diagnostic evaluation. It is important to note that differential diagnoses may not have been thoroughly considered at the initial stages of evaluation. In addition, all cases presented certain shortcomings during follow-up, regarding the lack of reassessment of the diagnoses. We present the failures in the diagnostic process in Table 2.
Failures in diagnostic process assessed by the diagnostic error evaluation and research tool.
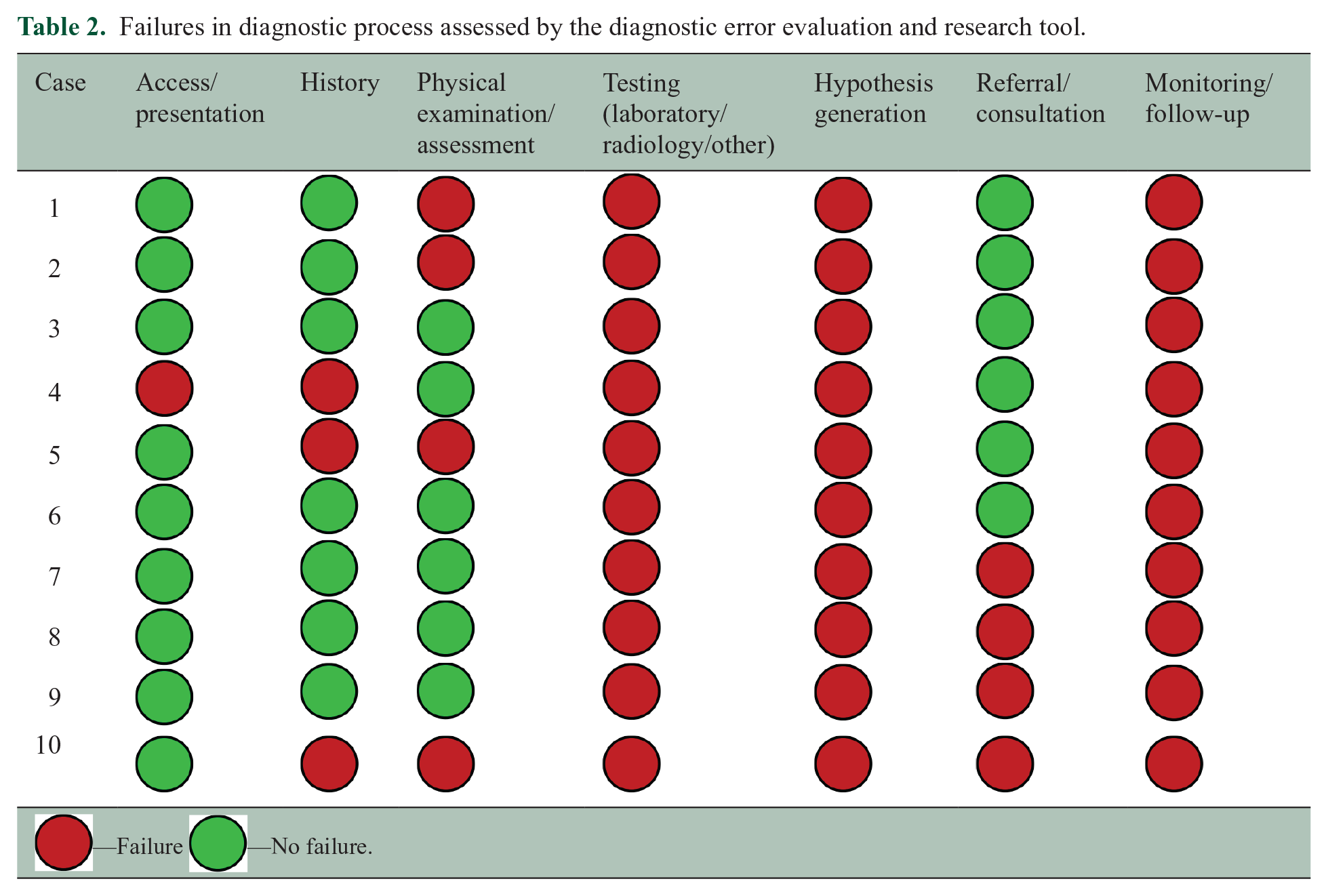
 —Failure
—Failure —No failure.
—No failure.
Discussion
We identified 10 participants of 201 incorrectly diagnosed with MS (4.98%) in a reference center in Brazil. Our study had a lower misdiagnosis rate compared with previous studies.8,10–13 This can be due to evaluating patients already in regular follow-up at a reference tertiary center by different neuroimmunologists, unlike previous studies that relied on referrals from various healthcare professionals, including neuroimmunologists, neurologists, and physicians of other specialties.
The alternative diagnoses obtained or suspected were mainly of autoimmune causes (such as demyelination of other etiologies and Behçet’s syndrome), genetic causes, and functional neurological disorder, all of which were accompanied by an abnormal MRI. Three participants presented a combination of different diagnoses, in addition to an MRI indicating lesions of suspected vascular origin. Case 1 had a combination of nystagmus of peripheral pattern, visual loss due to ophthalmological conditions, and functional neurological disorder, while Case 2 presented functional neurological disorder and non-specific neurologic symptoms. Case 5 had Meige syndrome, functional neurological disorder, and fibromyalgia. We also found one case of HTLV-1 infection, a disease that is more prevalent in South America 16 when compared with other regions globally, such as Europe and North America.
The main failures in the diagnostic process were due to the misinterpretation of the MRI since non-specific lesions were misidentified as typical lesions associated with MS. In addition, there was no early rechecking of the cases during the follow-up period, probably due to the high volume of patients who attend to our demyelinating diseases reference center and the limited time available for consultations. Prior authors have also noted barriers to reexamining established diagnoses of MS and suggested a tendency for MS specialists, after seeing many atypical presentations of MS, to dismiss “red flags” as being within the spectrum of MS, rather than a clue to an alternative condition.20,21
The low positivity rate of CSF IgG-OCB in our study (absent in 7/9—77.7%) was also a contributing factor to the misdiagnosis, although this test may have limited use for MS diagnosis in Brazil since the positivity of CSF IgG-OCB in our country is about 54.4%, 22 a lower rate compared with other regions of the world, such as in Sweden where the positivity rate of CSF IgG-OB in MS patients can reach 93%. 23 This can be due to genetic variations among populations, Brazil’s ethnic diversity resulting from the intermixing of different groups, variations in immune system profiles, and disease susceptibilities. In addition, regional discrepancies in environmental factors, diagnostic practices, and laboratory techniques can result in different OCB prevalence rates.
In a multicenter study, 7 Solomon described the main syndromes and alternative diagnoses obtained after extensive evaluation which were previously mistaken with MS. The most common diagnoses were migraine alone or in combination with other diagnoses 24/110 (22%), fibromyalgia 16/110 (15%), non-specific or nonlocalizing neurologic symptoms with abnormal MRI 13/110 (12%), functional neurological disorder 12/110 (11%), and neuromyelitis optica spectrum disorder 7/110 (6%). Other causes of misdiagnosis were also reported, contemplating autoimmune, vascular, nutritional, infectious, and genetic etiology. Our findings did not differ from Solomon (2016) except for one case related to HTLV infection. Despite the presence of migraine as a comorbidity among certain of our patients, the role of this diagnosis as a potential cause for the misdiagnosis was not considered. This can be due to the uncommon association of migraine-like pattern headaches with typical MS relapses, despite the presence of auras resembling MS symptoms. Thus, migraine may be less confused with MS in reference centers, under the evaluation of professionals with experience in MS.
A previous review reported the main differential diagnoses of MS that can be found in Latin America, 16 although the review did not aim to evaluate the rate of misdiagnosis of MS with the reported conditions. Among infectious diseases, neurosyphilis, neurotuberculosis, tropical spastic paraparesis, neuroschistosomiasis, and some arboviruses such as Dengue, Chikungunya, and Zika, have a high prevalence in South America and can mimic MS. 24 Apart from one participant in our study who had a final diagnosis of tropical spastic paralysis due to the HTLV-1 virus infection, we did not find other misdiagnosis cases of diseases that occur more frequently in Latin America. This may be due to the acute and aggressive clinical course of many of these diseases without proper treatment and a high probability that these conditions were ruled out as MS in the screening appointments for demyelinating diseases, being unlikely that these patients would be in an outpatient follow-up for a long period of time.
Our manuscript has some limitations. First, the study is unicentric which can lead to generalization of the results and our findings may not necessarily be representative of other regions of South America. While contributors to misdiagnosis may be inferred from available patient records and the specific alternative diagnosis identified, in most instances, our neurologists did not participate in making the initial incorrect diagnosis of MS. The assessment of some patients later in their disease course may have facilitated recognition of a misdiagnosis, and hindsight bias may have influenced opinions regarding earlier opportunities for a correct diagnosis.
Our study demonstrated a confirmed misdiagnosis rate of 4.98% for MS in a reference center, highlighting the importance of always rechecking whether the MS diagnosis is correct even in specialized centers of demyelinating diseases. To minimize the rate of misdiagnosis in MS, careful assessment of physical examination findings in conjunction with MRI results, prudent interpretation of neuroimaging, attention when CSF IgG-OCB is absent, and appropriate evaluation of functional neurological disorder as an organic pattern are crucial. We also suggest that differential diagnoses of MS that are more prevalent in South America may be commonly misdiagnosed in our region compared with other parts of the world. Nevertheless, it is essential to consider the most frequent etiologies of MS misdiagnosis, as reported in previous studies.7,8,10,11,13
Conclusion
We found a 4.98% prevalence of definitive misdiagnosis in patients previously diagnosed with MS in a reference center for demyelinating diseases. Misdiagnosis of MS remains a problem even in specialized centers, emphasizing the need for careful diagnostic evaluation. Our work may guide future strategies to improve the accuracy of MS diagnosis, particularly in South America.
The misdiagnosis of MS in Latin America may exhibit a stronger correlation with certain diseases that demonstrate a higher prevalence within this region.
Footnotes
Acknowledgements
The authors thank the participants for their involvement in and commitment to the “Misdiagnosis in Multiple Sclerosis in a Brazilian Reference Center: Clinical, Radiological, Laboratory Profile and Failures in the Diagnostic Process—Cohort Study” manuscript and the clinical study team for the conduct of the study.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors Guilherme Diogo Silva, Mateus Boaventura de Oliveira, Tarso Adoni, Larissa Silva Teixeira, Samira Luisa Apóstolos Pereira, and Dagoberto Callegaro receive regular visits of Biogen, Novartis, EMS, and Roche pharmaceutical companies.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.