
Abstract
Background:
Epidemiological data reveal that 45% of persons with multiple sclerosis (PwMS) in France are more than 50 years. This population more than 50 is more susceptible to cancer, and this risk may be increased by frequent use of immunosuppressive drugs. Consequently, concerns have arisen about the potential increased risk of cancer in PwMS and how patients should be screened and managed in terms of cancer risk.
Objective:
To develop evidence-based recommendations to manage the coexistence of cancer and multiple sclerosis (MS).
Methods:
The French Group for Recommendations in MS collected articles from PubMed and university databases covering the period January 1975 through June 2022. The RAND/UCLA method was employed to achieve formal consensus. MS experts comprehensively reviewed the full-text articles and developed the initial recommendations. A group of multidisciplinary health care specialists then validated the final proposal.
Results:
Five key questions were addressed, encompassing various topics such as cancer screening before or after initiating a disease-modifying therapy (DMT), appropriate management of MS in the context of cancer, recommended follow-up for cancer in patients receiving a DMT, and the potential reintroduction of a DMT after initial cancer treatment. A strong consensus was reached for all 31 recommendations.
Conclusion:
These recommendations propose a strategic approach to managing cancer risk in PwMS.
Introduction
Multiple sclerosis (MS) is a chronic demyelinating and neurodegenerative disease of the central nervous system (CNS). Age at onset of the disease is generally between 20 and 40 years, and today, in France, approximately 45% of persons with multiple sclerosis (PwMS) are 50 years or older. 1 Epidemiological studies show that the age of peak prevalence increased from 50 to 54 years in 1984 to 55 to 59 years in 2006. 2 In Italy, 18% of PwMS were reported to be 65 years or older. 3 In addition, comorbidities are overrepresented in PwMS. 4 Managing individuals aged 50 years or older is now standard practice in MS clinics. Usually, disease-modifying therapies (DMTs) are initiated at disease onset and maintained throughout the lifespan. Stopping them, even after 55 years of age could expose the patient to a reactivation of the disease. 5 These observations raise questions about the risk of cancer in PwMS—whether the risk is inherent in the disease itself or the result of DMT use. Another unresolved issue is the impact of cancer treatments on the course of MS and the management of DMTs in this context. Data extracted from the literature are scarce because cancer patients are systematically excluded from randomized trials on DMTs and epidemiological studies are inadequately documented, depending on the type of cancer and the specific management of treatments. In view of the current lack of high-level evidence literature concerning the management of cancer in PwMS, the Société Francophone de la Sclérose En Plaques (SFSEP) and its Multiple Sclerosis Recommendations Group (France4MS) decided to issue updated recommendations on cancer and MS. In formulating their recommendations, they considered information from the international scientific literature, existing recommendations on cancer in the general population, and the official summary of product characteristics for DMTs. The aim of these recommendations is to help clinicians make decisions regarding the management of the PwMS and cancer.
Methods
Process for recommendations by formalized consensus
The methodology employed in this study was previously discussed when recommendations relating to immunizations, infections, and pregnancy in MS were published.6–9 In summary, we generated recommendations through formalized consensus (RAND/UCLA) 10 in accordance with the guidelines issued by the French High Authority of Health (Haute Autorité de Santé (HAS)). 11 The primary aim of this approach was to establish a standardized level of agreement among experts. This was achieved by identifying and selecting points of consensus through iterative ratings with feedback as follows: (1) A reading group conducted a systematic analysis of the literature using reading grids and wrote a critical and hierarchical synthesis of the literature, including a referenced text and summary tables mentioning the levels of evidence of the studies, and (2) the steering committee of France4MS and the reading group then met to discuss the reported proof and prepare the list of proposals to be submitted to the rating group. Proposals were classified into levels A, B, or C according to the HAS guidelines. In addition, points of disagreement or uncertainty among experts were identified to provide professionals and patients with guidance in making informed decisions regarding appropriate care within specific clinical circumstances.
The steering committee defined five clinical questions within the scope of the following recommendations:
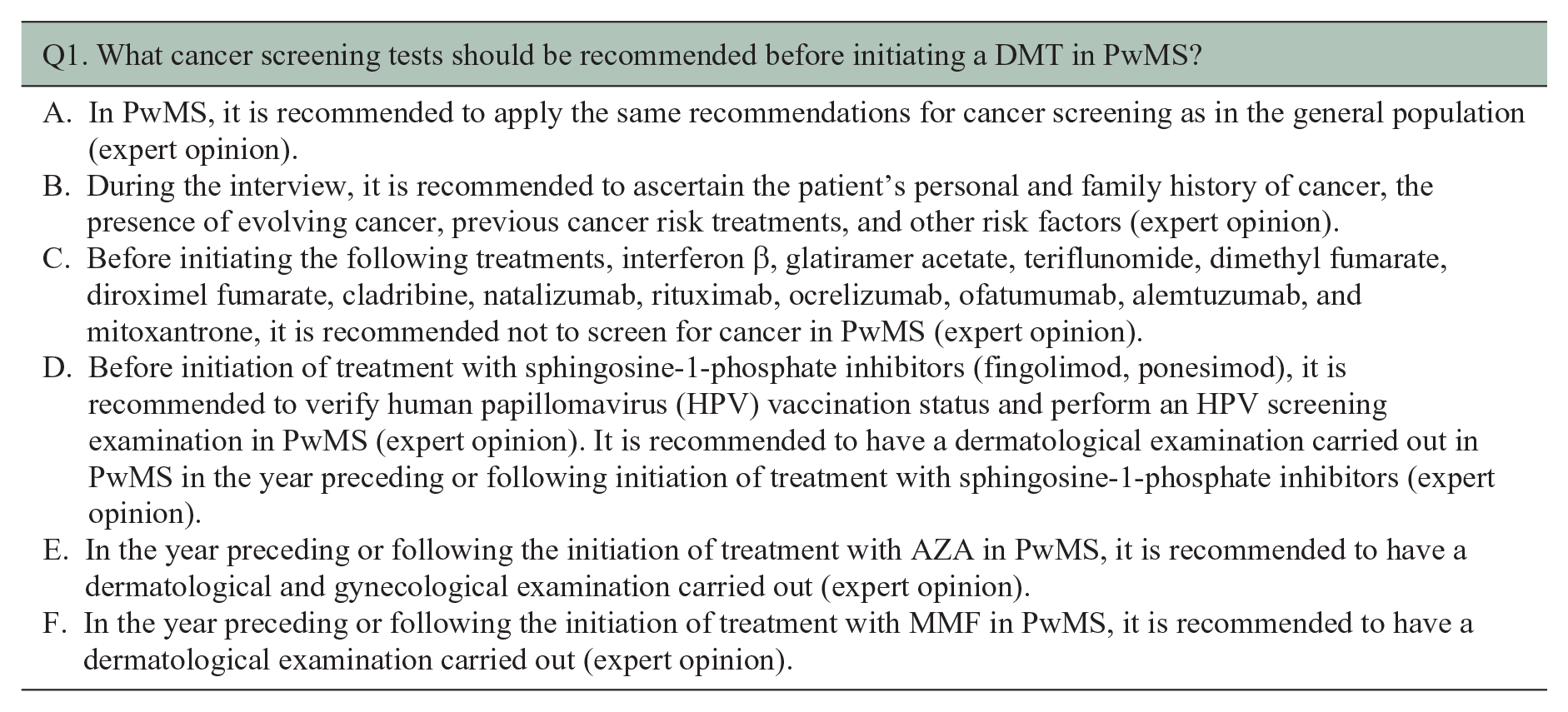
Q1. Which cancer screening tests should be recommended before initiating a DMT in PwMS?
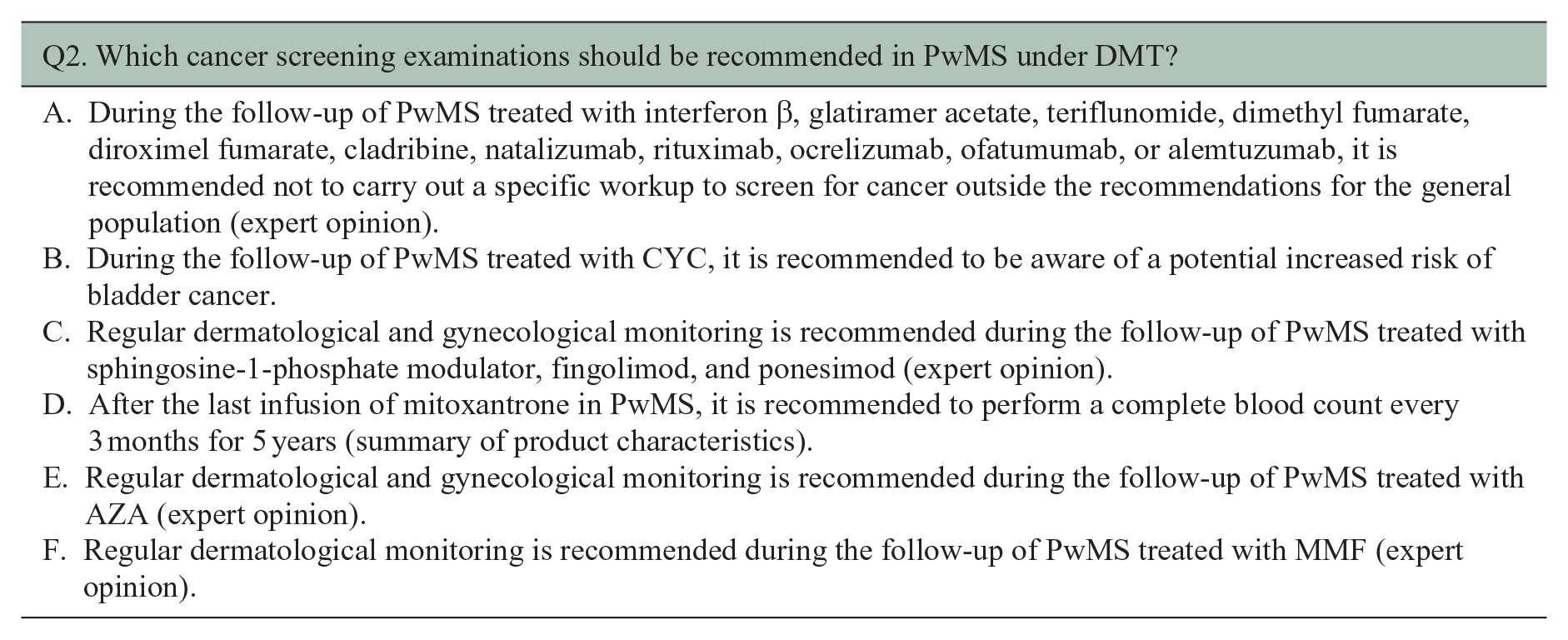
Q2. What cancer screening examinations should be recommended for PwMS receiving DMT?
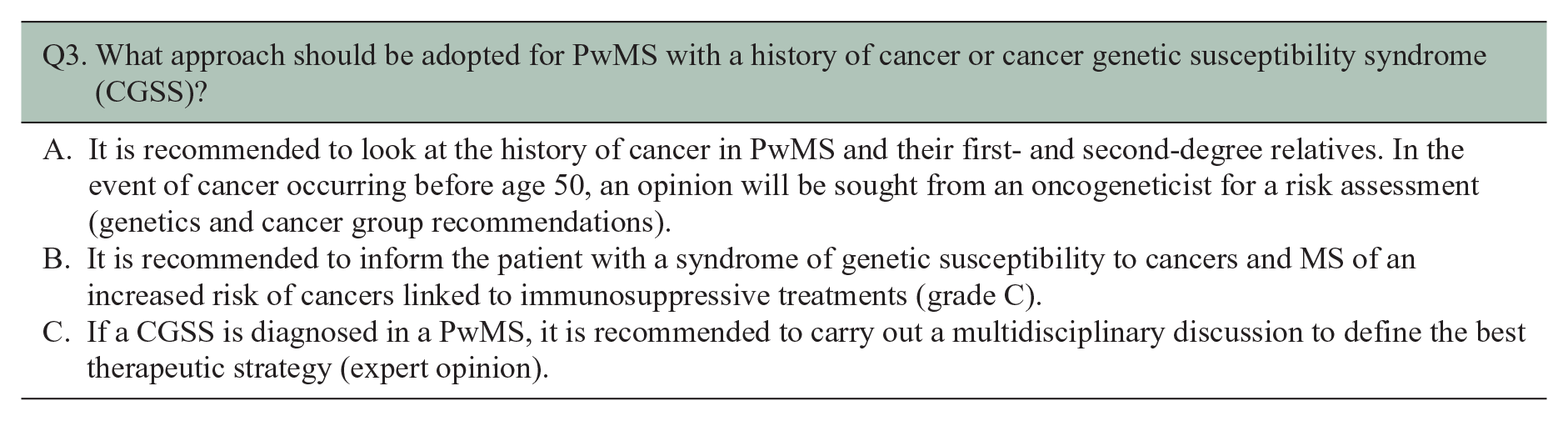
Q3. How should PwMS with a history of cancer or genetic susceptibility to cancer be managed?
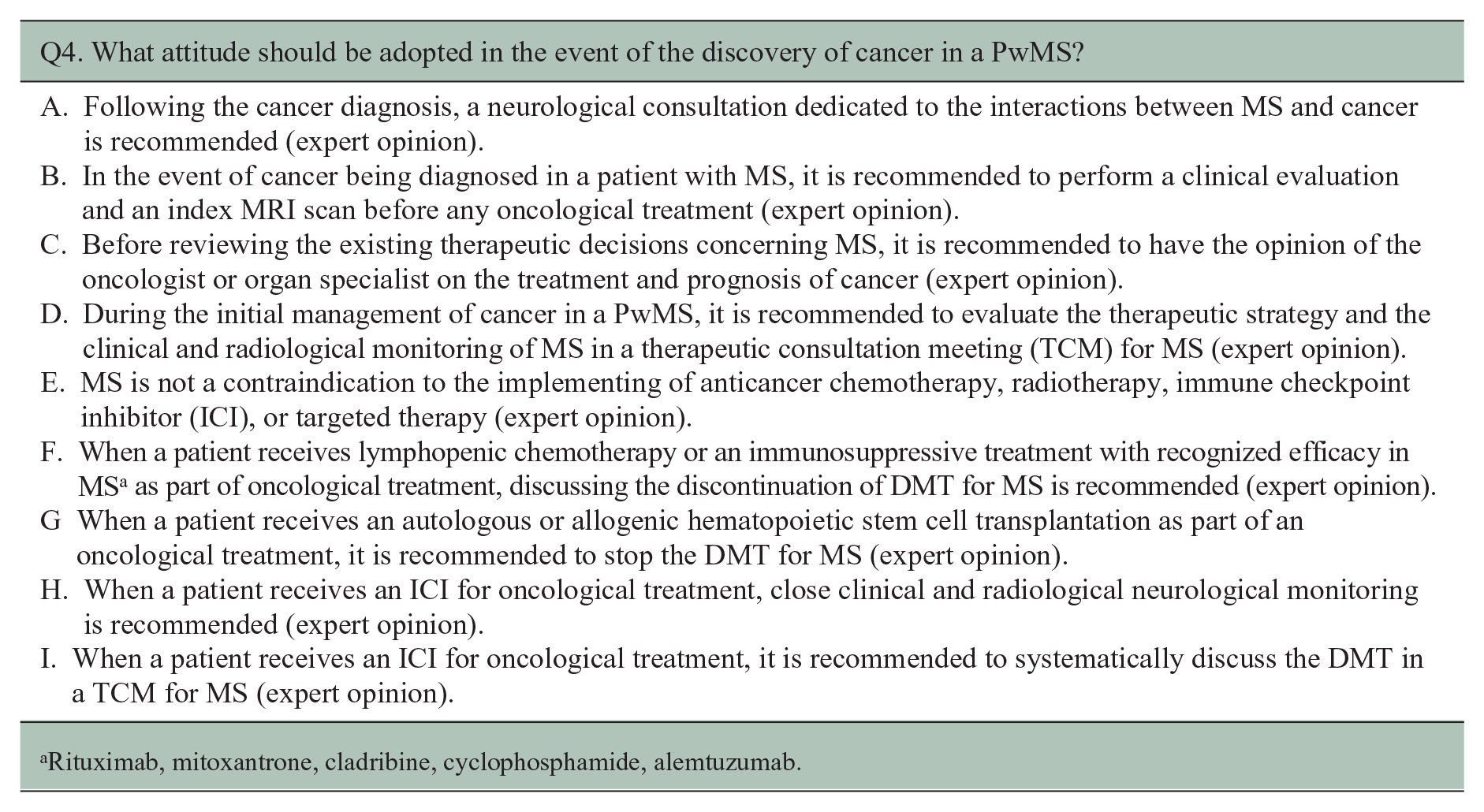
Q4. What approach should be taken upon the diagnosis of cancer in a PwMS?
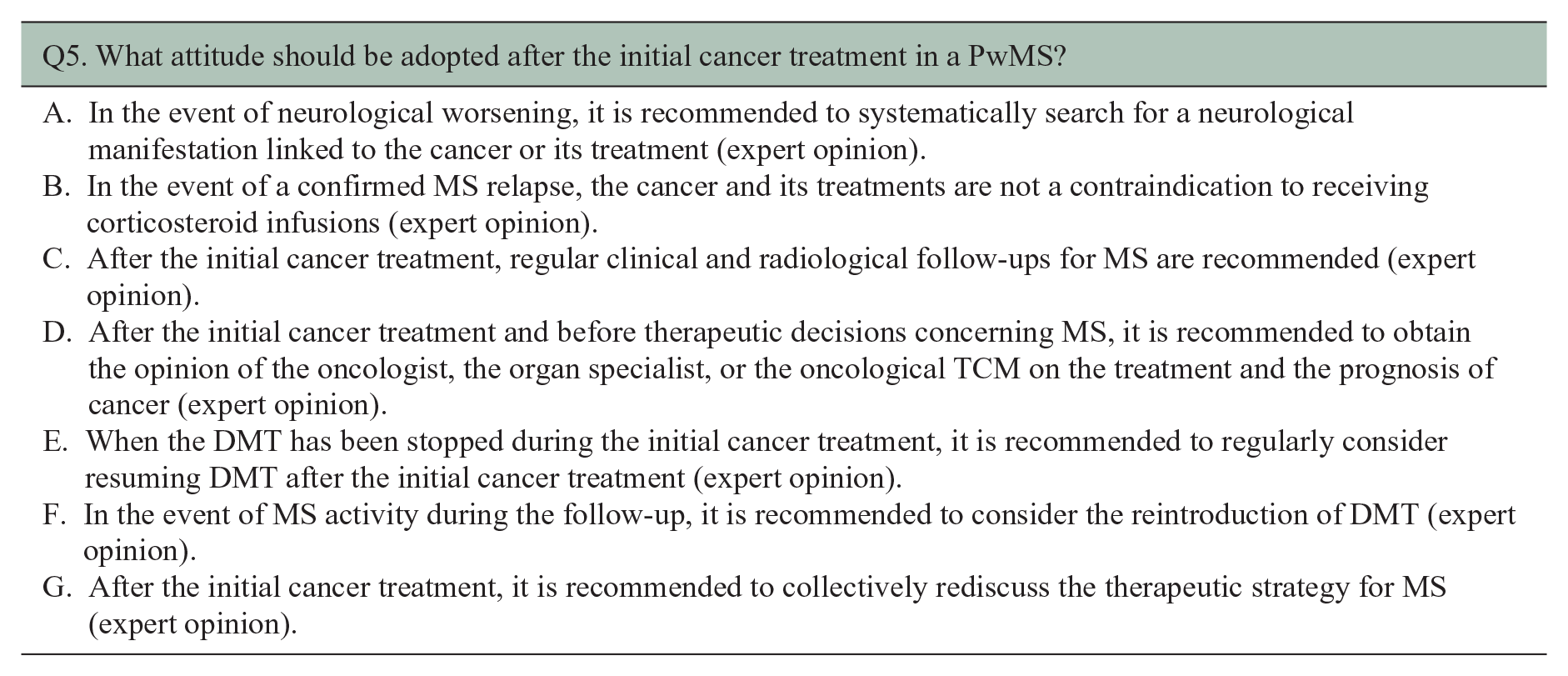
Q5. What approach should be adopted after the initial cancer treatment in a PwMS?
To address these questions, further clarification of the scientific context was necessary, leading to the emergence of additional inquiries:
Does MS increase the risk of cancer?
Do DMTs for MS increase the risk of cancer?
Does cancer increase the risk of developing a first demyelinating event suggestive of MS?
Is cancer associated with an increased risk of relapse or disability progression in PwMS?
Do cancer treatments increase the risk of developing a first demyelinating event suggestive of MS?
Are cancer treatments associated with an increased risk of relapse or disability progression in PwMS?
Data source
PwMS were not directly involved in the editing process of these recommendations, which are mainly based on analysis of the scientific literature and the data used to grant marketing authorization. A literature search for publications in English and French was performed with the help of professional librarians, using the Medline database (http://www.ncbi.nlm.nih.gov/pubmed), the leading websites referencing publications on recommendations and consensus conferences, and gray literature, from January 1975 through June 2022. An initial search was done with the following keywords: MS, cancer incidence, cancer risk, cancer review, neoplasm, immunotherapy, checkpoint inhibitors, anti-Programmed cell death protein 1 (PD1), anti-Programmed cell death protein ligand 1 (PDL1), anti-Cytotoxic T-lymphocyte-associated protein 4 (CTLA4), chemotherapy, hormonotherapy, hormone therapy, estrogen, progesterone, sex hormones, gonadotropin-releasing hormone (GnRH) agonist, GnRH antagonist, anti-androgen, aromatase inhibitors, estrogen inhibitors, tamoxifen, radiotherapy, interferon beta, glatiramer acetate, teriflunomide, dimethyl fumarate, diroximel fumarate, fingolimod, ozanimod, ponesimod, siponimod, natalizumab, ocrelizumab, rituximab, ofatumumab, cladribine, alemtuzumab, mitoxantrone, cyclophosphamide (CYC), azathioprine (AZA), and mycophenolate mofetil (MMF). The whole population of PwMS described in the literature was included in the analysis, irrespective of age or disease characteristics. All types of papers were selected, including case reports. The groups of readers subsequently performed a systematic analysis of the literature with tests and checklists giving arguments referring to the appropriate references. A total of 7569 references were screened and at 259 were retained for our study based on their relevance and quality. Re-reading and grading were performed by all members of the working groups during virtual meetings, and the written version elaborated by the coordinator reflected the many readings/re-readings of the working groups.
Analysis of the data
Recommendations were formulated based on a high level of evidence (level A or B) by considering relevant comments to enhance their clarity and modifying the content as necessary, taking into account the data provided. If necessary, the level of the recommendation could be adjusted. For recommendations based on a low level of evidence (level C) or a low level of agreement within the rating group, the following approach was followed: if the reading group agreed with the recommendation, with responses from at least 90% of the group falling within the range of 5–9, the proposal was retained. Relevant comments were taken into consideration to improve the wording of the recommendation. However, if the reading group was more broadly uncertain or disagreed with the initial recommendation, with fewer than 90% of the group’s responses falling within the 5–9 range, further discussions and revisions were undertaken to reach a consensus.
Results
The list of recommendations for each question is provided, and each recommendation is graded. All recommendations were considered appropriate, with a strong agreement.
Additional inquiries related to question 1: Does MS increase cancer risk?
The literature lacks consensus on the overall cancer risk in PwMS compared with the general population. Various studies present inconsistent findings regarding the overall change in cancer risk among PwMS. We identified five literature reviews and/or meta-analyses, summarized in supplementary data 1.12–17 While some studies report an overall increase in risk, others report a decrease and many report no significant change, as mentioned in supplementary data 2.18–30 These discrepancies in results may be attributed to differences in study populations (variations in recruitment methods, demographic characteristics, age, sex, and comorbidities, all of which can influence cancer risk), diverse methods of collecting cancer occurrence information (patient questioned by neurologists, patient self-administered questionnaires, which may underestimate cases, vs. comprehensive registry linkage), different periods associated with the use of various DMTs, and diverse risk management strategies.
When analyzing the risk of specific cancer subtypes in PwMS, contradictory results arise due to the aforementioned factors. Overall, there is no clear evidence of a significant change in the risk of most cancer subtypes in PwMS compared with the general population. However, uncertainties remain regarding some specific cancer subtypes. There appears to be a tendency toward an increase in breast cancers,17–20,22,24–29,31–38 a possible increase in the risk of CNS cancers (potentially due to overdiagnosis linked to magnetic resonance imaging (MRI) follow-up),17,19,21,24,26,34–38 a trend toward an increase in bladder cancers (which could be influenced by confounding factors such as chronic urinary catheterization, neurological bladder complications, or treatment with CYC),17,19,21,24,26,34–37,39 and a potential reduction in the risk of colorectal cancer in PwMS.17,19,20,24–26,34–37,39 No specific signal was reported for respiratory cancer,17,19,20,26,29,34–39 male and female genitalia cancer,17,19,20,24,26,34,36,37,40 skin cancer,17,19,24–28,34–37,39 hematological and lymphatic cancers,17,19,24,26,34–39 endocrine gland cancer,17,19,21,24,26,34 bone cancer,24,34,35 and other, rarer cancers.19,26,34,37 Studies on the risk for cancer subtypes in MS that included more than five patients are summarized in supplementary data 3.
Additional inquiries related to question 2: Do DMTs increase cancer risk?
Glatiramer acetate
In 2021, Doladille et al. conducted a study using the World Health Organization database (Vigibase) to investigate all cancers reported in PwMS. Among the 15,966 cases of cancer collected, 1170 patients were using glatiramer acetate. The study did not find evidence of an increased cancer risk in patients taking glatiramer acetate. 41 In 2011, Lebrun et al. examined the French cohort of PwMS through the European Database for Multiple Sclerosis (EDMUS) to identify cancer cases. They identified 253 patients with cancer but did not observe an elevated risk of cancer in patients receiving immunomodulators. 42 In 2005, Achiron et al. 18 reported a higher incidence of breast cancer in a study involving 992 patients taking glatiramer acetate. However, this increase was not statistically significant due to the limited number of reported cases (15 cases).
β-interferons
One study used safety data from significant interferon studies and data from Global Drug Safety. The study included 3746 patients, of whom 1096 had been exposed to interferon for more than 3 years, and 568 had been exposed for more than 5 years. This study did not identify a significant cancer risk. 43 In a 2014 study by Kingwell et al., 44 which involved 5146 PwMS with a mean follow-up of 9.5 years and receiving interferon, no difference was observed in the number of patients exposed to interferon and the duration of exposure between the 227 patients diagnosed with cancer and a control population.
Bloomgren et al. conducted a study in 2011 using postmarketing data from PwMS receiving intramuscular (IM) interferon, which potentially included 402,250 patients. They compared the cancer incidence rate with the incidence rate in the GLOBOCAN population (GLOBOCAN registry is an online database providing global cancer statistics and estimates of incidence and mortality in 185 countries) and found no increased risk of cancer. In addition, they analyzed US insurance data of PwMS treated with interferon compared with a group of PwMS treated with another drug and an untreated MS population. The study involved 12,894 patients with an average follow-up of approximately 3 years, and no elevated cancer risk was detected. 45
Teriflunomide
No specific correlation with cancer incidence has been observed in phase III trials.46,47 Furthermore, a literature review conducted using PubMed and the Vigibase database found no cancer reports in preclinical and clinical data associated with teriflunomide. 48 The French postmarketing analysis conducted in December 2015, as well as another French study utilizing data from the worldwide Vigibase between 1 January 2000 and 1 September 2019, also did not identify any red flags regarding cancer. 41 As of 31 March 2018, Vigilyze identified 308 cases of cancer, primarily breast (n = 47) and skin (n = 11). Only one case of follicular lymphoma was reported in a 54-year-old patient after 8 months of treatment. 49 An analysis of the Food and Drug Administration Adverse Event Reporting System (FAERS) database from 2004 to 2020 revealed 149 cancer reports associated with teriflunomide, with an adjusted odds ratio (OR) of 0.25 (0.21–0.30) when compared with beta-1a interferons as a reference. These findings indicate that there is no increased risk of cancer detection with teriflunomide. 50
Dimethyl fumarate
No specific correlation with cancer incidence has been observed in phase III trials.51–53 The FAERS database from 2004 to 2020 identified 429 cancer reports associated with dimethyl fumarate, with an adjusted OR of 0.30 (0.27–0.34) when compared with beta-1a interferons as a reference. 50 This finding is in line with a prospective study conducted in 16 Spanish centers, including 15 in the Madrid region, from February 2014 to May 2019. Out of 886 patients, eight cancer cases were found among those using dimethyl fumarate (0.9%). The cancer rate observed was similar to the general population of MS, with a rate of 298.39 per 100,000 patient-years, comparable to the general population in the Madrid region during the same period. The absence of a specific type of cancer and the occurrence of cancer at different times during treatment make a causal relationship between dimethyl fumarate and cancer unlikely, as suggested by the authors. 54 Another Spanish study analyzed 250 PwMS hospitalized in a single center during the period 1981 to 2019. Among them, 60 PwMS (24%) developed cancer, including nine patients (15%) on dimethyl fumarate. The duration of exposure to dimethyl fumarate was found to be protective, with a hazard ratio of 0.725 (95% confidence interval (CI) = 0.507–1.036, p = 0.077), indicating a reduction in cancer risk of 27% for each year of treatment. 55 In contrast, a study using data from the worldwide Vigibase between 1 January 2000 and 9 January 2019 demonstrated a significant association between dimethyl fumarate and the reporting of cancer in the univariate analysis. The association was more pronounced in females (76.9%) and predominantly observed in individuals aged between 45 and 64 years (58.4%), with a median time to onset of 13 months. After adjusting for age, gender, and geographic region, dimethyl fumarate remained associated with cancer reporting (reported OR = 1.35, 95% CI = 1.25–1.46; p < 0.0001). 41 The analysis by type of cancer revealed significant associations with cancers of the upper aerodigestive tract, breast, urinary tract, and nervous system. This study also reported an association between cancer reporting and the use of interferon-β or natalizumab, contrary to the findings of other studies. It is worth noting that this study potentially involved an over-reporting of cancer cases in a middle-aged or elderly population. In addition, the median delay of 13 months between dimethyl fumarate initiation and cancer onset appears relatively short to establish a direct causative role. Furthermore, a literature review conducted using PubMed and the Vigibase database highlighted preclinical carcinogenicity studies, indicating an increased incidence of renal tubular carcinomas, papillomas, and squamous cell carcinomas in the nonglandular stomach (anterior gastric sector) of mice exposed to dimethyl fumarate. 48 On the contrary, a study in mice demonstrated that dimethyl fumarate induced necroptosis in colon cancer cells, suggesting its potential as a candidate treatment for this type of cancer. 56
Sphingosine-1-phosphate modulators
Fingolimod
Data from the pivotal FREEDOMS II study, a double-blind placebo-controlled trial involving 117 centers conducted between June 2006 and March 2009, aimed to compare the efficacy and tolerance of different dosages of fingolimod versus placebo. Among the 358 patients taking fingolimod 0.5 mg, basal cell carcinoma was found in 10 patients (3%), compared with two patients (1%) in the placebo group. The occurrence of other cancers was infrequent and similar between the treatment and placebo groups. 57 In registries, a total of 1864 cases of cancer were reported from 2006 to 2018, with the most common being basal cell carcinomas (n = 272), breast cancers (n = 168), and multiple myelomas (n = 132). 48 While there are reported cases of melanoma, such as a Dutch series of five patients using fingolimod for over a year (12–32 months) without deep lymphopenia (lymphocytes >0.5 G/l), 58 data from the literature generally suggest a warning signal for skin cancers without an increased risk of melanoma in patients followed up for 4.5 years. 59 Data extracted from the FAERS database from 2004 to 2020 were reported to indicate a safety signal concerning skin cancer (adjusted OR = 4.54 (3.86–5.32)) 60 with fingolimod compared with other DMTs, and another retrospective study supported this finding. 41 In 2021, an analysis of the same registry did not find an increased risk of “all-cause” cancer in patients taking fingolimod compared with interferon beta-1a, which served as a reference (adjusted OR = 0.61 (0.53–0.70)). 50 Overall, while some cohort studies based on the cross-analysis of Swedish MS and cancer registries have reported a trend toward an increased risk of invasive cancer under fingolimod compared with the general population (hazard ratio = 1.53, 95% CI = 0.98–2.38), the ORs were not statistically significant. 61 Other cancers have been reported anecdotally, including two cases of Merkel cell carcinoma, 62 one case of cutaneous cluster of differentiation (CD)30 + T-cell lymphoma, 63 a few cases of lymphomatoid papulosis, B and T lymphomas, one case of acute lymphoblastic leukemia,64,65 one case of Kaposi’s sarcoma, 66 and a few cases of pulmonary or cerebral neoplasia. 48 In addition, an increased proliferation of various melanoma cell lines with S1P1 modulators used at therapeutic concentrations for PwMS has been observed in in vitro studies. 67
Based on these data, in 2015 the European Medicines Agency (EMA) recommended a dermatological check-up before initiating fingolimod treatment, followed by annual checkups throughout the duration of treatment. Fingolimod should not be used in patients with a history of skin cancer. The summary of product characteristics also advises a yearly dermatological follow-up.
Regarding HPV-related lesions, limited data are available in the literature regarding a possible link between fingolimod, HPV reactivation, and the occurrence of genital dysplasia. However, case series suggest an increased risk of cancer or lesions related to HPV infection, particularly in cases of lymphopenia. Five patients with chronic, treatment-resistant warts while taking fingolimod have been reported. The lesions appeared between 17 and 58 months after the start of treatment, and all patients experienced prolonged lymphopenia (minimum, 0.2 G/l) that improved after discontinuing or reducing the treatment dose. The outcome was unfavorable in one patient, with progression to metastatic anal squamous cell carcinoma. 68 Another series, published in 2021, included 16 patients without previous lesions who developed HPV-related lesions. These lesions appeared, on average, 4 years after the start of treatment. Among these patients, nine had cervical dysplasias (five low-grade and four high-grade cervical intraepithelial neoplasias), seven had condyloma acuminata, and four had large common warts affecting the hands and feet, resulting in aesthetic damage. In addition, a quarter of the patients had multiple lesions, and the HPV-16 oncogenic subtype was found in three patients. Six patients discontinued treatment, and anti-HPV vaccination was administered to patients with HPV-related lesions that persisted despite treatment (laser ablation, conization, and cryotherapy). All patients had lymphopenia at diagnosis, with lymphocyte counts between 0.14 and 0.86 G/l. 69 More recently, a case was published involving a patient who had been on fingolimod for 6 years and presented with lymphopenia ranging between 0.3 and 0.6 G/l. This patient developed anal and genital HPV-related intraepithelial neoplasia. 70 Finally, a case of squamous cell carcinoma of the tonsil linked to HPV-16 was published involving a 50-year-old man who had been on fingolimod for 6 years; this occurred in the context of moderate lymphopenia (0.53 to 0.7 G/l). 71
Siponimod
The phase III multicenter, randomized, double-blind study EXPAND, conducted in 2018, aimed to evaluate the efficacy and tolerability of siponimod compared with placebo in 1645 patients for up to 3 years or until the occurrence of a prespecified number of patients with confirmed disability progression. No cancer cases were observed during the pivotal study and its extension phase.72,73 Data extracted from the FAERS database covering the period from 2004 to 2020 were reported to indicate a safety signal primarily related to basal cell carcinoma, with an adjusted OR of 22.83 (95% CI = 12.27–38.83). 60
Ozanimod
Ozanimod was evaluated in two randomized, double-blind, active-comparator-controlled, double-placebo, parallel-group phase III clinical trials in patients with relapsing–remitting multiple sclerosis (RRMS). Study 1, SUNBEAM, was a 1-year study involving 1346 patients in which patients continued their assigned treatment beyond month 12 until the last patient had completed the study. 74 Study 2, RADIANCE, was a 2-year study involving 1320 patients. 75 During the pivotal trials and their extension, 38 (1.4%) out of 2787 patients exposed to ozanimod developed malignancies. The most frequent malignancy was basal cell carcinoma, with 11 cases (0.4%), and the incidence was comparable between the combined ozanimod and interferon β-1a groups. Among 1868 women, nine (0.5%) developed breast cancer. In addition, three malignancy-related deaths occurred during the 5-year follow-up, including metastatic pancreatic carcinoma, disseminated cancer with an unknown primary source, and glioblastoma. 76 Data extracted from the FAERS database from 2004 to 2020 did not report any cases of skin cancer among the 52 reported files of patients under ozanimod. 60
Ponesimod
Regarding ponesimod, the phase III multicenter, double-blind OPTIMUM study was published in 2021. The study aimed to compare the efficacy of ponesimod versus teriflunomide among 1133 equally randomized patients. The proportion of serious adverse effects was similar between the two groups. Although treatment discontinuations due to serious adverse effects were more frequent in patients on ponesimod (8.7% vs. 6%), no specific pattern or cluster of severe adverse effects was identified in either group. The authors noted five cutaneous events in the ponesimod group, including two basal cell carcinomas, two excisions of pre-existing naevi, and one melanoma, compared with one basal cell carcinoma in the teriflunomide group. 77
Natalizumab
The phase II and phase III studies of natalizumab in MS provide evidence of the safety of natalizumab use, and there is no signal suggesting an increased risk of oncological pathology.78,79 These findings are further supported by extension studies80,81 and cohort studies.42,61 The available follow-up durations in these studies extend to 10 years. Although case reports of melanoma in patients treated with natalizumab have been documented in the literature,82–85 long-term follow-up studies employing more rigorous methodologies have not found an association between natalizumab use and increased oncological risk. Current literature data do not indicate an elevated cancer risk in patients treated with natalizumab.
Anti-CD20: ocrelizumab, rituximab, ofatumumab and
Ocrelizumab
Phase III studies of ocrelizumab in RRMS revealed nine cancer cases, with four cases occurring in the initial phase of the study and five cases in the extension phase. Among these cases, four were breast cancers. 32 In a phase III study of ocrelizumab in primary progressive multiple sclerosis (PPMS), 2.3% of patients in the treated group presented with neoplasia, including four breast cancers, compared with 0.8% in the placebo group. 31 However, this imbalance in the incidence of breast cancer, specifically, was not observed in the extension studies 86 ; after a maximum follow-up period of 7 years, the incidence rates of cancers, including breast cancer, did not differ significantly from those in the general population.
Rituximab
Rituximab is used off-label in treating PwMS, meaning it is not explicitly approved for this indication. Consequently, there are limited safety data available for rituximab in MS. However, cohort studies conducted on patients with MS have not indicated an increased risk of cancer associated with rituximab. 61 Similarly, data from other indications, like rheumatoid arthritis, have not shown any elevated cancer risk compared with general population registers, regardless of the treatment duration or the number of administered courses.87,88
Ofatumumab
Regarding ofatumumab, data from phase II and phase III studies with a follow-up period of 30 months have not demonstrated an increased incidence of neoplasia in the ofatumumab group compared with the teriflunomide group.89,90 However, long-term data for ofatumumab are currently unavailable.
Ublituximab
Ublituximab is a new intravenous glycoengineered chimeric anti-CD20 IgG1 monoclonal antibody, approved in December 2022 by the Food and Drug Administration (FDA) for treatment of relapsing forms of MS. Data from phase II and III studies did not show any new safety signals of concern compared with phase III trials of other anti-CD20 monoclonal antibodies.91,92 In particular, no increased incidence of neoplasia in the ublituximab group was observed compared with the teriflunomide group. However, long-term data for ublituximab are currently unavailable.
Alemtuzumab
Available data on an association between alemtuzumab and cancer risk in the literature are limited. However, it should be noted that many thyroid carcinomas have been reported after treatment with alemtuzumab in phase III trials and their extensions.93–95 In the phase III CARE-MS I and CARE-MS II trials, which included 376 patients in the alemtuzumab 12 mg group and 426 and 161 patients in the alemtuzumab 12 and 24 mg groups, respectively, three patients developed thyroid carcinomas. Two cases were in the alemtuzumab 12 mg group, while none were observed in the interferon or alemtuzumab 24 mg groups. During the 5-year extension studies of CARE-MS I and II, two additional cases of thyroid carcinoma were reported. However, data regarding other types of cancer do not provide enough evidence to identify any specific excess risk.
Mitoxantrone
An increased risk of acute promyelocytic leukemia has been reported following treatment with mitoxantrone. The incidence of acute leukemia varies among studies, ranging from 0.25% to 2.82% in studies with an average patient follow-up of at least 3 years after the first infusion of mitoxantrone and including at least 200 patients. One study suggests a relationship between the cumulative dose of mitoxantrone and the risk of acute promyelocytic leukemia, while other studies do not support this association. 96 Notably, a case of acute promyelocytic leukemia has been reported at a very low cumulative dose of 12 mg/m2. The time between the last course of mitoxantrone and the diagnosis of acute promyelocytic leukemia varies widely in the literature, ranging from 1 to 105 months. However, the risk appears to be higher in the first few years after treatment. Seventy-three percent of cases occurred within 4 years in an Italian study. The leukemogenic risk is linked to interactions with topoisomerase 2, an enzyme allowing the repair of single or double DNA fragmentation. Inhibition of topoisomerase 2 predisposes to the risk of secondary leukemia through the occurrence of translocations in genes coding for transcription factors. This explains why the most frequent secondary leukemia is acute promyelocytic leukemia, linked to a mutation of the BRCA29 gene. The presence of leukocytosis, coagulation disorders, or myelemia at the first administration should lead to the suspicion of future chemotherapy-induced leukemia. This risk may be specific to PwMS who carry genetic variants in DNA repair and drug-metabolizing enzymes, leading to impaired chemotherapy detoxification or inefficient repair of drug-induced genetic damage. 97
In a large multicenter French study that combined data from the EDMUS databases of 12 centers and the French cancer registry FRANCIM, 1243 patients treated with mitoxantrone were identified, among whom 28 developed cancers. The study did not find a significantly increased risk of cancer after mitoxantrone compared with no treatment, but a trend toward increased risk (p = 0.06) with a relative risk (RR) of 1.7 was observed. Another retrospective monocentric study found a slightly increased incidence ratio for all types of cancers combined (1.50, 95% CI = 1.05–2.08) in the population treated with mitoxantrone compared with the general population. Specifically, a higher incidence ratio was observed for colorectal cancer (2.98, 95% CI = 1.20–6.14) and acute leukemia (10.44, 95% CI = 3.39–24.36). 98 However, no increase in the incidence ratio of breast cancer was reported. It should be noted that the increase in the incidence of colorectal cancer was not found in another retrospective study. 99
Cladribine
The pivotal phase III CLARITY study identified an oncology risk alert with three cases of cancer (a melanoma and carcinomas of the pancreas and ovary) in the cladribine arm. In contrast, no cases were observed in the control arm. 100 However, the absence of cancer cases in the control group was surprising given the number of patients in that group and the expected incidence of cancers. To further assess the risk, Pakpoor et al. conducted a meta-analysis in 2015 using the CLARITY data, comparing the number of cancers in the cladribine group with a set of control groups from other phase III MS studies. This analysis did not find any excess risk of cancer associated with cladribine. 101 In 2020, Leist et al. 102 conducted a study including all patients treated with cladribine from the phase III studies (CLARITY, CLARITY Extension, and ORACLE-MS) and the prospective PREMIERE registry. The study comprised 923 patients with a mean follow-up of 4.28 years, with 18 patients followed for more than 9 years. Compared with the GLOBOCAN registry, an online database providing global cancer statistics and estimates of incidence and mortality in 185 countries, no increased risk of cancer was observed in the cladribine-treated patients.
Overall, while the initial CLARITY study raised concerns about an oncological risk with cladribine based on the observed cases, subsequent analyses, including meta-analyses and a comprehensive study of cladribine-treated patients, did not find an increased risk of cancer associated with cladribine treatment.
Azathioprine
AZA is used off-label in treating PwMS, meaning it is not explicitly approved for this indication. Consequently, there are limited safety data available for AZA in MS. Data from the literature indicate that using thiopurines after transplantation is associated with a higher risk of nonmelanoma skin cancers, particularly squamous cell carcinoma. This contrasts with the general population, where basal cell carcinomas are more common. 103 The carcinogenic effect of thiopurines is believed to be due to increased genetic mutations induced by UVA rays and increased production of reactive oxygen species (ROS) in skin epithelial cells. Patients should be educated about the importance of strict sun protection measures and avoiding excessive sun exposure. Regular dermatological monitoring, determined by the dermatologist based on individual risk factors like skin type, should be continued, along with self-monitoring. This monitoring is necessary even after discontinuing thiopurines, as the increased risk persists throughout life. 104 It should be noted that the risk of melanoma is not increased with thiopurines. 103
In the context of organ transplants, the use of thiopurines is also associated with an increased risk of cervical cancer linked to HPV. 105 Studies investigating the relationship between immunosuppressants and the increased risk of cervical cancer have produced conflicting results. However, as a precaution, patients should be reminded of the importance of annual gynecological follow-up and adherence to HPV vaccination guidelines.
Regarding MS, retrospective cohorts and case–control studies have not reported a specific correlation between AZA use and overall cancer incidence in PwMS.106–109 However, two observational studies, by Confavreux et al. and La Mantia et al., observed a slight increase in cancer risk in subpopulations receiving high cumulative doses of AZA (>600 g), and with aging. The risk was reported as an OR of 6.7 for high cumulative dose and a standardized incidence ratio (SIR) ranging from 1.11 to 1.21 for age-related risk.107,108
Mycophenolate Mofetil
MMF is used off-label in treating PwMS, meaning it is not explicitly approved for this indication. Consequently, there are limited safety data available for MMF in MS. The data regarding the risk of tumors associated with MMF are conflicting. In vitro studies have shown that MMF has a mutagenic effect, but it has also been used to prevent tumor dissemination in vitro. In addition, MMF has been found to enhance the antiherpetic activity of aciclovir and ganciclovir, potentially reducing the risk of developing Epstein–Barr virus (EBV)-related lymphoproliferative syndrome.
In a randomized trial involving 580 heart transplant patients, comparing AZA with MMF in combination with cyclosporine and prednisone, a similar cancer incidence was observed between the two groups. After 3 years of follow-up, the incidence rates were 15.6% in the AZA group and 12.5% in the MMF group. 110 A review of randomized trials comparing MMF with AZA in kidney transplant patients found no significant difference in the incidence of skin cancers between the two groups. This suggests that the risk of skin cancer is similar for patients receiving MMF and those receiving AZA. 111 A recent meta-analysis that included 32 studies evaluated the risk of cancer associated with MMF. The analysis concluded that exposure to MMF is not associated with an increased risk of cancer and may even be associated with a lower risk than AZA or no treatment. The meta-analysis included both randomized and observational studies, with only four studies having a comparator group of patients without treatment. 112
In PwMS receiving MMF, no specific correlation with cancer incidence has been reported. However, in patients receiving MMF for systemic lupus erythematosus, several cases of primary lymphoma of the CNS have been reported.113–118 Risk factors identified in these cases were prolonged exposure to MMF (more than 2 years) and EBV seropositivity. 113
Despite the overall reassuring data, it is essential to note that prolonged immunosuppressive therapy, including MMF, is associated with an increased risk of certain types of skin cancer, such as squamous and basal cell carcinoma, as mentioned in the summary of product characteristics. Regular dermatological examinations are recommended to aid in the early detection of suspicious skin lesions, allowing for timely referral to a dermatologist for further evaluation or biopsy if necessary.
Methotrexate
Methotrexate (MTX) is used off-label in treating PwMS, meaning it is not explicitly approved for this indication. Consequently, there are limited safety data available for MTX in MS. In the literature, no specific correlation with global cancer incidence has been reported in PwMS receiving MTX.42,48,119–122
However, an increased incidence of EBV-induced lymphomas has been reported among patients receiving MTX for rheumatoid arthritis. The SIR for EBV-induced lymphomas in this patient population ranged from 2.46 to 7.4, indicating an elevated risk compared with the general population. Risk factors associated with the development of these lymphomas include prolonged exposure to MTX, cumulative dose, aging, and the use of other immunosuppressive therapies like infliximab in the context of rheumatologic disorders.42,48,122–124
Cyclophosphamide
CYC is used off-label in treating PwMS, meaning it is not explicitly approved for this indication. Consequently, there are limited safety data available for CYC in MS. CYC is associated with an increased incidence of bladder cancer, as indicated by studies reporting a SIR of 3.6.125–127 These publications highlight several risk factors for bladder cancer, including prolonged exposure to CYC, cumulative dose, aging, repeated urothelial injury such as vesical catheterization and hemorrhagic cystitis, and smoking. On the contrary, the administration of uromitexan, low-dose (<0.7 mg/m2) and limited exposure time to CYC (<3 years) protects against bladder cancer, reducing the risk to levels observed in the general population.48,127–130
CYC use is also associated with an increased risk of myelodysplastic/proliferative syndromes (SIR = 19.6) and cutaneous carcinomas, specifically basal cell carcinoma (SIR = 3.8) and squamous cell carcinoma (SIR = 11.5).126,131 Identified risk factors for these conditions include exposure duration and cumulative dose.126,127,132
However, in the context of MS populations, only a few publications are available, and the data from these studies show no increased incidence of cancer more than a 5-year follow-up period.125,128–130 No consensus for monitoring the risk of bladder cancer after CYC has been elucidated from the literature. To date, no major organization recommends screening asymptomatic adults for bladder cancer. 133
Stem cell transplantation
The available literature in patients with previous cancer treated with autologous hematopoietic stem cell transplantation (aHSCT) suggest that a second cancer risk was modestly increased compared with the general population (SIR = 1.4, 95% CI = 1.2–1.6). 134 Unfortunately, these data should be interpreted with caution as aHSCT conditioning, pre-aHSCT therapies, and risk factors for cancer such as sun exposure history and smoking history in this cohort were not taken into account. However, the occurrence of cancer as a direct consequence of aHSCT in PwMS has not yet been substantiated by scientific research. After an extensive review of the literature on PubMed, no publication supporting an increased risk of developing cancer in PwMS after aHSCT was found. In the largest cohort of 507 patients with MS, no cancer cases occurred after a median follow-up of 2 years. 135 Long-term data for aHSCT are needed to assess the real risk of cancer in the population of PwMS.
Additional inquiries related to question 3: Does cancer increase the risk of developing a first demyelinating event suggestive of MS?
It was relevant to consider cancer genetic susceptibility syndrome (CGSS) cases to study whether a genetic background was shared with MS. The most common CGSSs are breast-ovary syndrome (3% to 4% of breast cancers: 1–5/10,000) and Lynch syndrome (or hereditary nonpolyposis colorectal cancer (HNPCC), 2% to 4% of colon cancer cases; 1/800 in the general population). There are also many other, rarer CGSSs (ataxia-telangiectasia, Cowden syndrome, Von Hippel-Lindau disease, malignant melanoma, neurofibromatosis, polyposis, retinoblastoma, xeroderma pigmentosum). 136 These cancers are due to a deleterious inherited mutation, present from birth in germ cells, in all cells of the body, which alters directly or indirectly DNA repair mechanisms. These GCSSs arise and are transmitted according to the laws of Mendelian inheritance, which, in the cases of breast-ovary syndrome and Lynch syndrome, is autosomal dominant to high penetrating and variable expressiveness, predominant for phenotypic localizations (breast/ovaries for breast cancer (BRCA) or colon for Lynch syndrome) with a triple heterogeneity, allelic, nonallelic, and phenotypic with significant polymorphisms. 137 It is a genetic predisposition that increases the risk of cancer evaluated in relation to the average risk in the general population. Detection of the known inherited family mutation predicts the occurrence of cancer in another healthy relative. More than 80 genetic cancer predisposition genes with hundreds of deleterious mutations have been listed.
For GCSSs, high penetrance makes genetic causality a necessary and sufficient factor to opt for systematic screening and prevention in healthy carriers. The genetic component in MS is a non-Mendelian phenomenon, linked to numerous polymorphisms. 138 Then, complex and infinitely varied association phenomena occur with interactions between polymorphism and environment (exposure factors, contraception, and tobacco) with different levels of expressiveness thresholds for women and men. 139 The role-played by endogenous (gender and endocrine system for BRCA) or exogenous (diet, lifestyle, pollution, and drugs) environmental factors partly explains why there is no exclusive causality in the phenotypic expression of these genes.
No increase in frequency or association with any autoimmune disease has been reported in GCSS patients. A case describing a co-occurrence of MS and cancer in a BRCA1 family raises the question of the involvement of the Signal transducer and activator of transcription 3 (STAT3) gene located in the 17q21.2 region, very close to that of the BRCA1 gene at 17q21.315. 140 The occurrence of MS could be the presumed result of genetic polymorphism, internal and external environmental factors, and a stochastic phenomenon.
Practical issues:
If the patient has a documented CGSS and MS is diagnosed: whatever happens, the patient will have a very close oncogenetic follow-up by organ oncology specialists. The risk of cancer in these patients is extremely high. The current practice is screening or removal surgery. It should be remembered that, because of the numerous possible cancers, ablation surgery does not preclude the need for whole-body surveillance. When prescribing a DMT for MS, it should be noted that the risk of cancer in autoimmune diseases is mainly linked to the treatments. 141 The prescription of immunosuppressive therapy will strengthen patient monitoring with the general practitioner and screening for cancers detectable in prophylaxis (gynecological, lung, digestive, skin, and otorhinolaryngology).
If the biography of a patient followed for MS notes a personal history of cancer or cancers in relatives, the occurrence of cancer before the age of 50 should raise the question of a GCSS. The case must be referred to an oncogeneticist for a risk assessment, which may indicate the need for genetic testing. The family risk is hereditary and transmissible if the genetic result is positive. 142 The recommendations established for the GCSS will then be applicable. Patients benefit from regular monitoring and medical support, to be coordinated with MS monitoring. Sometimes, preventive surgical treatments by removing the organ at high risk of cancer may be recommended to reduce the risk of cancer. If the patient is already being treated with an immunosuppressant at the time of diagnosis of a GCSS and the activity of the autoimmune disease justifies it, the doctors involved in the management will favor the clinical priority (patient’s age or clinical form of MS), with appropriate target organ monitoring.
If a genetic susceptibility to present adverse reactions to certain cytotoxic drugs in MS is suspected, a discussion must take place between the patient and their doctors specializing in neurology, oncology, and oncogenetics. In the case of mitoxantrone, the risk–benefit ratio of its use in aggressive forms of MS remains controversial because of its cardiotoxicity, gonadotoxicity, and the risk of chemotherapy-related leukemia (0.81%). 143
If a genetic susceptibility to radiation is suspected, the situation will arise whether the PwMS treated or not must receive radiotherapy for the treatment of cancer. Several radiation susceptibility syndromes are described: ataxia telangiectasia, xeroderma pigmentosum, hypogammaglobulinemia, and Turcot, Gardner, and Cockayne syndromes. The same irradiation dose will induce lesions 50 to 100 times more numerous than in the general population. This susceptibility concerns 5% to 15% of the general population. 144 It should be remembered that Bruton tyrosine kinase inhibitors (BTKis) are included in the list of radiosensitizing molecules and could influence our future practices.
Rituximab, mitoxantrone, cladribine, cyclophosphamide, alemtuzumab.
Additional inquiries related to question 4: Is cancer associated with an increased risk of relapse or progression of disability in patients with MS?
This question has been discussed above in the case of a CGSS. More generally, however, cancer and its treatment are associated with an increased risk of the onset of a transient or more prolonged aggravation of disability, due to the evolution of the tumor pathology and its impact on the general condition, in the general population and a fortiori in patients with MS. No publications specifically addressing this point have been found in the literature.
Additional inquiries related to question 5: Do cancer treatments increase the risk of developing a first demyelinating event suggestive of MS?
Immune checkpoint inhibitors (ICIs) and targeted therapies
ICIs are monoclonal antibodies that target immune system checkpoint proteins, and they have become a standard treatment for various cancers over the past decade. Commonly treated cancers include melanoma, Hodgkin’s disease, and non-small-cell lung cancer. 140 Neurological complications have been reported with ICIs, occurring at a frequency ranging from 1% in monotherapy to 12% in combination therapy. 145 The question arises as to whether the use of these immunotherapies can trigger or exacerbate autoimmune diseases like MS.146,147
Currently, there are no prospective studies specifically designed to identify the occurrence of initial demyelinating events under ICI treatment in the general oncology population. Literature reviews attempting to assess the occurrence of such events mainly focus on reporting the incidence of neurological side effects associated with ICIs and reviewing various clinical cases with varying levels of documentation. Reported symptoms may sometimes be imprecise, and incomplete complementary assessments make it challenging to establish or discuss a diagnosis of MS.145,147,148 While many published cases describe encephalitis, these cases are often far from meeting the diagnostic criteria for MS.149–151
However, the occurrence of inflammatory myelitis following ICI treatment is worth noting. A series of seven cases and a literature review have been published. Three of the seven cases presented hypersignals without contrast enhancement on brain MRI; one of the three cases had oligoclonal bands in the cerebrospinal fluid, but the diagnosis of MS was not discussed. 152 It should be noted that most patients in this series had received thoracic radiotherapy, which could represent a predisposing factor for developing myelitis.
Recently, targeted therapies tailored to specific mutations and signaling pathways have been developed in cancer treatment. These therapies have also been associated with demyelinating neurological events. 153 Isolated cases suggesting the onset of demyelinating episodes resembling MS have been reported with imatinib, a tyrosine kinase inhibitor (TKi).154,155 The case reported by Govind Babu et al. 155 is particularly convincing as it involves a bilateral and progressive decrease in visual acuity that recurred upon re-administration of the treatment. In the cases described by Rostein et al., 154 two patients were being treated for myeloproliferative syndrome and a digestive tumor, respectively. The first case presented with a severe seronegative neuromyelitis optica phenotype 8 weeks after receiving imatinib at a dose of 400 mg/day. Uhthoff’s phenomenon revealed the second case after 8 months of TKi treatment for the digestive tumor. This patient had oligoclonal bands in the cerebrospinal fluid and demyelinating lesions on brain MRI. Despite the TKi treatment being maintained, no other events were observed. However, new lesions were detected during MRI follow-up after 1 year, which prompted the introduction of DMT. Three additional cases that rapidly occurred after the introduction of another TKi, nilotinib, have only been presented in abstract form.122,156 Furthermore, there have been reported cases of demyelinating manifestations associated with another TKi, tofacitinib, used in treating other systemic autoimmune diseases.157,158
The situation becomes even more complex when considering that these targeted therapies are sometimes administered after ICI treatment in cases where ICIs have been ineffective.
Radiotherapy
Radiation therapy can have detrimental effects on the CNS, and the extent of these effects depends on factors such as the volume of tissue irradiated, the specific area targeted for radiation, and the dose administered. Neurotoxicity resulting from radiation therapy is typically categorized as acute (occurring within days to weeks after treatment), subacute (lasting for weeks to months), or long-term (persisting for months to years). At a microscopic level, subacute or long-term manifestations of neurotoxicity often exhibit demyelination as the predominant characteristic. 159 The damage to myelin is believed to be related to the impact of radiation on various components, including oligodendrocyte-2 astrocyte progenitors, mature oligodendrocytes, the blood–brain barrier, microglia, and the expression of circulating cytokines. These mechanisms contribute to the disruption of myelin and the subsequent neurological consequences.159,160
The available literature on the association between ionizing radiation and the development of MS is primarily based on isolated case reports or retrospective studies with insufficient evidence. As a result, the data are insufficient to draw definite conclusions regarding an increased risk of developing MS after exposure to ionizing radiation. The earliest case report describing a temporal connection between cerebral radiotherapy and the onset of acute demyelination in a patient without a known history of MS dates back to 1959. 161 However, this case analysis needs more documentation to provide informative insights. An Iranian case–control study reported a higher prevalence of a history of radiotherapy in PwMS compared with control cases. 162 According to that study, 15% of PwMS had a history of radiotherapy, while only 2% of controls did. However, the observed rate of 15% appears implausible and far exceeds what is typically observed in clinical practice. The study also suffered from significant methodological biases, including selection and recall biases. It is also worth noting that the collection of exposure history to X-rays encompassed radiotherapy history and exposure to ionizing radiation in occupational settings and medical procedures involving X-rays. Another retrospective case–control study, published in 1993, investigated the history of exposure to various environmental factors, including X-ray exposure for therapeutic or occupational reasons, both in controls and in cases within 5 years before the MS diagnosis. 163 Among the 91 PwMS (diagnosed between 1983 and 1988), five had a history of X-ray exposure, while none of the 248 controls had such a history. However, this study also suffered from notable methodological biases. In addition, several case reports suggest a potential link between the occurrence of a first central demyelinating event, within the radiation field of radiotherapy, in patients without a history of demyelinating disease. However, these reports primarily describe cases of acute demyelination that do not meet the criteria for a diagnosis of MS.164–168
In summary, the current evidence regarding the association between ionizing radiation and the development of MS is limited and inconclusive due to the reliance on isolated cases and retrospective studies with methodological biases. There is, therefore, a need for more comprehensive studies with more substantial evidence.
Chemotherapy and stem cell transplantation
After an extensive review of the literature on PubMed, no publication supporting an increased risk of developing MS related to chemotherapy and stem cell transplantation was found. The available literature does not provide evidence to suggest a causal relationship between these treatments and the development of MS. It is important to note that chemotherapy and stem cell transplantation are commonly used to treat various cancers and hematological disorders, and their potential adverse effects are well-documented. However, the occurrence of MS as a direct consequence of these treatments has not been substantiated by scientific research.
Endocrine therapy
Anticancer endocrine hormone therapies encompass a range of treatments such as synthetic estrogens, progestins, GnRH analogs/GnRH receptor antagonists, aromatase inhibitors (e.g. anastrozole and letrozole), anti-estrogens including selective estrogen receptor modulators (SERMs) such as tamoxifen, selective estrogen receptor degraders (SERDs), such as fulvestrant, and anti-androgens, such as enzalutamide and abiraterone acetate. After an extensive review of the literature on PubMed, no publications supporting an increased risk of developing MS related to any of these hormone therapies were found. The available evidence does not suggest a causal link between the use of these treatments and the development of MS.
Furthermore, there is a lack of specific research examining the potential impact of aromatase inhibitors or anti-androgens on MS. The literature does not currently include publications investigating the association between these particular endocrine therapies and MS development or progression.
Additional inquiries related to question 5: Are cancer treatments associated with an increased risk of relapse or progression of disability in patients with MS?
ICIs and targeted therapies
No data are available from pivotal ICI studies because the presence of a pre-existing autoimmune condition, including MS, was an exclusion criterion for therapeutic trials. However, a multicenter retrospective study specifically investigated the risk of exacerbation under ICI in 56 patients with autoimmune diseases, including two patients with MS who did not experience a relapse. 169 In addition, two case reports described patients who had their first relapse of MS after a radiologically isolated syndrome (RIS) at 4 and 10 months, respectively, following the initiation of ipilimumab.170,171 Two other case reports noted relapses in patients with pre-existing MS that occurred 3–4 weeks and 6 months, respectively, after the introduction of ipilimumab (anti-CTLA4).172,173 In one of these cases, glatiramer acetate and MTX were discontinued before initiating ipilimumab; in the other case, no information was provided regarding the course of fingolimod. However, no data are available in the literature regarding the exacerbation of disability, as measured by the expanded disability status scale (EDSS) score, following the introduction of ICI in PwMS. In three cases, the neurological outcomes were described as favorable after administrating corticosteroids, and there were no recurrences under DMT for MS despite continued ICI treatment.170–172 The article by Garcia et al. theoretically reports 13 cases of MS patients treated with ICI. 174 However, the methodology is open to criticism, since this work combines an observation by the authors whose semiology is dubious, since it mentions fever and confusion, with cases taken from the literature and/or a pharmacovigilance database (with duplications between the two). First central demyelinating episodes and relapses in patients with previous MS are also mixed. Thus, we can assume that there are at most 5 additional cases of MS patients worsening on ICI mentioned in this article, but poorly documented, as no data are available on clinical presentation or MRI activity, and data are lacking on background MS treatment and its eventual discontinuation. Furthermore, no published cases have reported a worsening of progressive forms of MS following the use of ICI.
Regarding other targeted therapies used in the treatment of certain cancers, particularly TKis, to the best of our knowledge no cases of MS exacerbation related to the introduction of such therapies have been published to date. It is worth noting that BTKis are currently under investigation in MS, with promising results from phase II studies. 175
Radiotherapy
The available data in the literature primarily consist of descriptions of isolated cases, which are insufficient to draw definite conclusion regarding an increased risk of relapse or worsening of disability after cerebral radiotherapy in patients with MS. There is only one methodologically helpful article that has investigated the risk of neurotoxicity following ionizing radiation in patients with MS. 176 This retrospective, single-center study conducted at the Mayo Clinic included all patients with known MS who received external cerebral radiotherapy between 1976 and 2004. Among the 15 patients in the cohort, none experienced a worsening of MS symptoms during the radiotherapy treatment. However, six patients (40%) developed grade 4 or higher neurotoxicity due to radiotherapy within a median period of 1 year. Grade 4 neurotoxicity refers to life-threatening conditions or those associated with disability. The cumulative incidence of grade 4 or higher neurotoxicity in these patients was 25% at 1 year and 57% at 5 years. The authors concluded that cerebral radiotherapy may be associated with a higher risk of neurotoxicity in PwMS than in those without demyelinating disease. It should be noted that radiotherapy was administrated in five out of six patients before 1995; therefore, these results cannot be generalized to current management practices and conformal radiotherapy techniques.
In a more recent retrospective study involving 16 PwMS treated for a CNS tumor, no association was found between the risk of MS inflammatory activity (clinical/radiological) and prior exposure to radiotherapy or radiosurgery. 177 Among these patients, 62% had undergone radiotherapy or radiosurgery. Although the occurrence of MS inflammatory activity appeared to be more frequent in patients who had received radiotherapy or radiosurgery than those who had not, this difference was not statistically significant (66.7% vs. 33.3%, p = 0.238). In addition, case reports describe clinical flares accompanied by new brain lesions shortly after cerebral radiotherapy, suggesting that ionizing radiation may have contributed to an episode of focal inflammatory activity in the CNS. These reported cases involve patients with clinically defined MS or those in the clinically isolated syndrome (CIS) or RIS stages.178,179
Chemotherapy and stem cell transplantation
Some cancer treatments have been shown to have a beneficial immunomodulatory effect on the course of MS. Examples of such treatments include anti-CD20 therapies, 180 CYC, 181 mitoxantrone, 182 cladribine, 183 and hematopoietic stem cell transplantation. 184 These treatments can have a prolonged effect on MS, lasting for several years even after the completion of chemotherapy or stem cell transplantation.99,185,186 It is essential to consider this long-lasting effect when deciding whether to resume MS treatment after using these drugs during cancer therapy. This may allow for a postponement of continuing MS treatment, conditioning it on the observation of clinical and radiological signs of inflammatory activity during monitoring. However, it should be noted that the protocols used in cancer treatment may not involve the same doses, regimen, and duration as those used in treating MS, which limits this management strategy.
A retrospective study from Germany reported a cohort of 16 patients with both MS and a CNS tumor, either primary or secondary. The study found that the recurrence of inflammatory activity, whether clinical or observed on MRI, was more frequent in patients who did not receive chemotherapy (83.3%) than in those who did (16.7%). 177
Endocrine therapy
After an extensive review of the literature on PubMed, no publication supporting an increased risk of worsening MS related to the use of endocrine therapy was found. However, there is some indirect evidence worth mentioning. Numerous experimental and clinical studies have provided evidence for the protective role of sex steroids (estrogens, progestagens, and androgens) in the progression of MS, attributed to their immunological, promyelinating, and neuroprotective properties. 187 These findings suggest that sex steroids may benefit MS. Similarly, tamoxifen, a medication with anti-estrogenic properties, has been associated with an immunomodulatory effect. 188 GnRH agonists and antagonists, which are used in assisted reproduction, have been investigated in several studies, with conflicting results. 189 However, a recent study found no evidence of an increased risk of relapse with either GnRH agonists or antagonists in PwMS. 190
While no specific publications directly supporting a risk of worsening MS with these treatments were found, some indirect evidence highlights the potential beneficial effects of sex steroids and the lack of increased relapse risk with GnRH agonists/antagonists in PwMS.
Corticosteroids
Corticosteroids have been extensively used in the field of cancer for various supportive care purposes, such as alleviating fatigue, managing cancer-related pain, improving appetite, and reducing edema in space-occupying lesions (e.g. brain or spinal cord tumors).191–195 While there are no specific studies investigating the risks associated with corticosteroid use during cancer treatment in PwMS, we can speculate that this medication may not have any negative impact on the course of MS.
A specific consideration related to potential therapeutic interactions should be taken into account when using corticosteroids during cancer treatment. First, no clear evidence of an increased risk of infection or interactions affecting the efficacy of cancer chemotherapy has been reported. However, a distinction should be made when using corticosteroids in combination with immunotherapy. The anti-inflammatory and immunosuppressive effects of corticosteroids, particularly on T lymphocytes, 196 can potentially interfere with the mechanism of action of anticancer immunotherapies, including chimeric antigen receptor (CAR) T-cell therapy and ICI. Several retrospective observational studies have been published, some of which suggest a reduction in the effectiveness of ICI in terms of overall cancer survival when corticosteroid therapy is administered (usually orally and over several days, at doses ranging from 10–35 mg/day of prednisone equivalent).197–201 However, these studies often suffer from biases, as patients receiving corticosteroids generally have a poorer prognosis (e.g. presence of brain metastases and cancer-related pain), and not all of these studies employ appropriate statistical methods to address these biases. On the contrary, the use of oral corticosteroid therapy at doses of 10–50 mg/day of prednisone equivalent over a few weeks to manage immune-related adverse events associated with ICI treatment does not appear to be linked to changes in overall cancer survival.202–204 Again, these are retrospective observational studies where comparing patients treated with corticosteroids and those who are untreated may not be the primary focus of the analysis.
In summary, while corticosteroids have been widely used in cancer care, their use during immunotherapy may affect treatment efficacy. Though predominantly retrospective, the available evidence suggests a potential reduction in the effectiveness of ICI when corticosteroids are administered. However, further research using robust study designs is needed to understand better the impact of corticosteroid therapy on cancer treatment outcomes, particularly in immunotherapy.
Discussion
The 2023 recommendations of the French MS Society provide updated guidance on managing patients who have experienced cancer and MS. This pathological context is complex, involving many immunological aspects related to the diseases themselves and the drugs used in both disorders. Neurologists are faced with three main questions when dealing with these cases: (1) What is the impact of the cancer and its treatment on the course of MS? (2) What is the impact of MS and its treatments on the progression of cancer? and (3) What are the neurological toxicities of therapies, unrelated to MS, used in cancer that could add disability to our MS patient? Therefore, these recommendations are an essential step toward better control of MS and cancer and should minimize the risks of reducing the efficacy of anticancer drugs or adding immunoactive medication to treat MS.
From a practical point of view, the literature reports a number of barriers faced by disabled patients, including those with MS, when engaging in the cancer screening process. Some of these potential barriers, such as level of education, age, occupation, and degree of disability, are common to all disabled patients.205,206 Others are more specific to MS, such as fatigue, cognitive impairment, inadequate transportation or inaccessible cancer centers, inappropriate screening equipment, or insensitivity of health care professionals to cancer screening recommendations. 207 As some of these barriers are country-dependent, we believe that our recommendations could be a first step in sensitizing neurologists and oncologists to the need for cancer screening in the MS population. Finally, every neurologist should refer his or her patients, and at every consultation could remind them of the need for screening. In each referral center, the issuing of reminders in the form of letters, cards, phone calls, or e-mails could be a useful way of reducing the number of missed PwMS appointments.
A second practical issue relates to the delay between the introduction of lymphopenic drugs for cancer treatment and DMT discontinuation. This issue is crucial in view of the need to ensure the absence of rebound effects in MS patients, particularly for scavenger drugs such as natalizumab or S1P1 modulators. This timeframe depends on the pharmacodynamics of the lymphopenic chemotherapy used in the cancer. The list of these lymphopenic drugs is fairly long, and each case must be examined individually at a TCM involving at least the oncologist and the referring neurologist.
However, the treatment of MS is rapidly evolving, and drugs in development, such as BTKi in MS and other immunologically active drugs in cancer, will require regular updates to maintain the accuracy of these recommendations. This article emphasizes the necessity of sharing neurological discussions with the oncologist in the cancer setting. In our opinion, a TCM at the local or national level would be the best option to evaluate the prognosis related to cancer or MS, the impact of treatments on the evolution of each pathology, and the neurological toxicities of these therapies.
Supplemental Material
sj-docx-1-msj-10.1177_13524585231223880 – Supplemental material for Cancer and multiple sclerosis: 2023 recommendations from the French Multiple Sclerosis Society
Supplemental material, sj-docx-1-msj-10.1177_13524585231223880 for Cancer and multiple sclerosis: 2023 recommendations from the French Multiple Sclerosis Society by Nicolas Collongues, Françoise Durand-Dubief, Christine Lebrun-Frenay, Bertrand Audoin, Xavier Ayrignac, Caroline Bensa, Kévin Bigaut, Bertrand Bourre, Clarisse Carra-Dallière, Jonathan Ciron, Gilles Defer, Arnaud Kwiatkowski, Emmanuelle Leray, Elisabeth Maillart, Romain Marignier, Guillaume Mathey, Nathalie Morel, Eric Thouvenot, Hélène Zèphir, Julie Boucher, Clémence Boutière, Pierre Branger, Angélique Da Silva, Sarah Demortière, Maxime Guillaume, Benjamin Hebant, Edouard Januel, Anne Kerbrat, Eric Manchon, Xavier Moisset, Alexis Montcuquet, Chloé Pierret, Julie Pique, Julien Poupart, Chloé Prunis, Thomas Roux, Perrine Schmitt, Géraldine Androdias and Mikael Cohen in Multiple Sclerosis Journal
Supplemental Material
sj-docx-2-msj-10.1177_13524585231223880 – Supplemental material for Cancer and multiple sclerosis: 2023 recommendations from the French Multiple Sclerosis Society
Supplemental material, sj-docx-2-msj-10.1177_13524585231223880 for Cancer and multiple sclerosis: 2023 recommendations from the French Multiple Sclerosis Society by Nicolas Collongues, Françoise Durand-Dubief, Christine Lebrun-Frenay, Bertrand Audoin, Xavier Ayrignac, Caroline Bensa, Kévin Bigaut, Bertrand Bourre, Clarisse Carra-Dallière, Jonathan Ciron, Gilles Defer, Arnaud Kwiatkowski, Emmanuelle Leray, Elisabeth Maillart, Romain Marignier, Guillaume Mathey, Nathalie Morel, Eric Thouvenot, Hélène Zèphir, Julie Boucher, Clémence Boutière, Pierre Branger, Angélique Da Silva, Sarah Demortière, Maxime Guillaume, Benjamin Hebant, Edouard Januel, Anne Kerbrat, Eric Manchon, Xavier Moisset, Alexis Montcuquet, Chloé Pierret, Julie Pique, Julien Poupart, Chloé Prunis, Thomas Roux, Perrine Schmitt, Géraldine Androdias and Mikael Cohen in Multiple Sclerosis Journal
Supplemental Material
sj-docx-3-msj-10.1177_13524585231223880 – Supplemental material for Cancer and multiple sclerosis: 2023 recommendations from the French Multiple Sclerosis Society
Supplemental material, sj-docx-3-msj-10.1177_13524585231223880 for Cancer and multiple sclerosis: 2023 recommendations from the French Multiple Sclerosis Society by Nicolas Collongues, Françoise Durand-Dubief, Christine Lebrun-Frenay, Bertrand Audoin, Xavier Ayrignac, Caroline Bensa, Kévin Bigaut, Bertrand Bourre, Clarisse Carra-Dallière, Jonathan Ciron, Gilles Defer, Arnaud Kwiatkowski, Emmanuelle Leray, Elisabeth Maillart, Romain Marignier, Guillaume Mathey, Nathalie Morel, Eric Thouvenot, Hélène Zèphir, Julie Boucher, Clémence Boutière, Pierre Branger, Angélique Da Silva, Sarah Demortière, Maxime Guillaume, Benjamin Hebant, Edouard Januel, Anne Kerbrat, Eric Manchon, Xavier Moisset, Alexis Montcuquet, Chloé Pierret, Julie Pique, Julien Poupart, Chloé Prunis, Thomas Roux, Perrine Schmitt, Géraldine Androdias and Mikael Cohen in Multiple Sclerosis Journal
Supplemental Material
sj-docx-4-msj-10.1177_13524585231223880 – Supplemental material for Cancer and multiple sclerosis: 2023 recommendations from the French Multiple Sclerosis Society
Supplemental material, sj-docx-4-msj-10.1177_13524585231223880 for Cancer and multiple sclerosis: 2023 recommendations from the French Multiple Sclerosis Society by Nicolas Collongues, Françoise Durand-Dubief, Christine Lebrun-Frenay, Bertrand Audoin, Xavier Ayrignac, Caroline Bensa, Kévin Bigaut, Bertrand Bourre, Clarisse Carra-Dallière, Jonathan Ciron, Gilles Defer, Arnaud Kwiatkowski, Emmanuelle Leray, Elisabeth Maillart, Romain Marignier, Guillaume Mathey, Nathalie Morel, Eric Thouvenot, Hélène Zèphir, Julie Boucher, Clémence Boutière, Pierre Branger, Angélique Da Silva, Sarah Demortière, Maxime Guillaume, Benjamin Hebant, Edouard Januel, Anne Kerbrat, Eric Manchon, Xavier Moisset, Alexis Montcuquet, Chloé Pierret, Julie Pique, Julien Poupart, Chloé Prunis, Thomas Roux, Perrine Schmitt, Géraldine Androdias and Mikael Cohen in Multiple Sclerosis Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: N. Collongues has received honoraria for consulting or presentation from Alexion, Biogen Idec, Bristol-Myers Squibb, Horizon Therapeutics, Merck Serono, Novartis, Roche, and Sanofi-Genzyme and is a member of the Editorial Board of the Journal de la Ligue Française contre la Sclérose en plaques and the Neurology and Therapy Journal. Françoise Durand-Dubief has received personal compensation for consulting, serving on a scientific advisory board, speaking, or other activities from Biogen, BMS-Celgene, Merck, Novartis, Roche, Sanofi-Genzyme, and Teva. Christine Lebrun Frenay has nothing to disclose. Géraldine Androdias has received personal compensation for consulting, serving on a scientific advisory board, speaking, or other activities from Biogen, Merck, Novartis, Roche, and Sanofi-Genzyme. Bertrand Audoin has nothing to disclose. Xavier Ayrignac has received consulting fees and lecturing fess, travel grants, and unconditional research support from Alexion, Biogen, Genzyme, Janssen, Merck Serono, Novartis, Roche, Sanofi Aventis, and Teva Pharma. Caroline Bensa has received consulting honoraria from Alexion, Sanofi, Merck, Biogen, BMS, and Novartis. Kevin Bigaut has received lecturing fees and travel grants from Biogen, Celgene-BMS, Novartis, Roche, and Sanofi-Genzyme. Julie Boucher has nothing to disclose. Bertrand Bourre serves on the scientific advisory board and has received funding for travel and honoraria from Alexion, Biogen, BMS, Horizon, Janssen, Merck, Novartis, Sanofi, and Roche. Clemence Boutiere has nothing to disclose. Pierre Branger has received personal compensation for consulting, serving on a scientific advisory board, speaking, or other activities from Alexion, Biogen, Bristol-Myers Squibb, Merck, Novartis, and Sanofi-Genzyme. C. Carra-Dalliere has received travel grants and/or consulting fees from Alexion, Biogen, Merck, Novartis, Roche, and Sanofi-Genzyme. Jonathan Ciron has received personal compensation for consulting, serving on a scientific advisory board, speaking, or other activities from Biogen, Novartis, Merck, Sanofi, Roche, Celgene-BMS, Alexion, and Horizon Therapeutics. Angelique Da Silva has received personal fees from Daichi and Leopharma. Gilles Defer has received personal fees from Biogen, Bristol-Myers Squibb, Merck Serono, Novartis, Sanofi-Genzyme, and Teva Pharmaceuticals. Sarah Demortière has nothing to disclose. Maxime Guillaume has received honoraria from Novartis, Merck, and Sanofi. Benjamin Hebant has nothing to disclose. Edouard Januel has nothing to disclose. Anne Kerbrat has nothing to disclose. Arnaud Kwiatkowski has received personal compensation for consulting, serving on a scientific advisory board, speaking, or other activities from Biogen, Merck Serono, Novartis, Sanofi-Genzyme, Roche, and Teva. Emmanuelle Leray has received personal compensation for consulting, serving on a scientific advisory board, speaking, or other activities with Alexion, Biogen, Merck, Novartis, Roche, and Sanofi-Genzyme. Elisabeth Maillart has received research support from Biogen and personal fees for lectures and serving on advisory boards from Biogen, Janssen, Merck, Novartis, Roche, Sanofi, and Teva. Guillaume Mathey has nothing to disclose. Xavier Moisset has received financial support from Allergan-Abbvie, Biogen, BMS, Grünenthal, Lilly, Lundbeck, Teva, Merck Serono, Novartis, Pfizer, Roche, and Sanofi-Genzyme and non-financial support from SOS Oxygène not related to the submitted work. Alexis Montcuquet has received personal compensation for consulting, serving on a scientific advisory board, speaking, or other activities from Alexison, Biogen, Merck Serono, Novartis, Sanofi-Genzyme, Roche, and Teva. Nathalie Morel has nothing to disclose. Romain Marignier has received personal fees from Horizon Therapeutics, Alexion, Roche, and UCB; and nonfinancial support from Horizon Therapeutics, Merck, Biogen, and Roche. Chloe Pierret has nothing to disclose. Julie Pique has received travel grants and personal compensation for consulting, serving on a scientific advisory board, speaking, or other activities from Teva, Biogen, Novartis, Merck, Sanofi-Genzyme, Roche, Celgene-BMS, and Alexion. Julien Poupart has nothing to disclose. Chloe Prunis has nothing to disclose. Eric Thouvenot has received personal fees from Actelion and Teva and grants from Biogen, Merck Serono, Novartis, and Roche. Thomas Roux has received personal compensation for consulting, speaking, or serving on a scientific advisory board from Alexion, Biogen, BMS-Celgene, Merck, Novartis, and Sanofi-Genzyme. Perrine Schmitt has nothing to disclose. Helene Zephir has nothing to disclose. Mikael Cohen has received personal compensation for consulting, serving on a scientific advisory board, speaking, or other activities from Ad Scientiam, Biogen, Merck, Sanofi-Genzyme, Roche, Celgene-BMS, Alexion, and Horizon Therapeutics.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.