
Abstract
Introduction:
One strategy to mitigate progressive multifocal leukoencephalopathy (PML) risk is to switch to other highly effective disease-modifying therapies (DMTs). However, the optimal switch DMT following natalizumab (NTZ) discontinuation is yet to be determined.
Objective:
The objective of the study is to determine the most effective and tolerable DMTs to switch to following NTZ discontinuation due to John Cunningham virus (JCV) antibody positivity.
Methods:
This is a multicenter observational cohort study that included all stable relapsing-remitting multiple sclerosis (MS) patients who were treated with NTZ for at least 6 months before switching therapy due to JCV antibody positivity.
Results:
Of 321 patients, 255 switched from NTZ to rituximab/ocrelizumab, 52 to fingolimod, and 14 to alemtuzumab, with higher annualized relapse rate (ARR) in fingolimod switchers (0.193) compared with rituximab/ocrelizumab or alemtuzumab (0.028 and 0.032, respectively). Fingolimod switchers also had increased disability progression (p = 0.014) and a higher proportion developed magnetic resonance imaging (MRI) lesions compared with rituximab/ocrelizumab (62.9% vs. 13.0%, p < 0.001, and 66.6% vs. 24.0%, p < 0.001, respectively). Mean drug survival favored rituximab/ocrelizumab or alemtuzumab over fingolimod (p < 0.001).
Conclusion:
Our study shows superior effectiveness of rituximab/ocrelizumab and alemtuzumab compared with fingolimod in stable patients switching from NTZ due to JC virus antibody positivity.
Introduction
Natalizumab (NTZ) is a monoclonal antibody approved for treating relapsing-remitting multiple sclerosis (RRMS). It blocks α4β1 integrin on leukocytes, preventing mononuclear cell trafficking across the blood–brain barrier (BBB). 1 Phase III clinical trials2,3 and observational studies4–6 have confirmed its long-term efficacy and safety in RRMS.
The most significant risk with NTZ is progressive multifocal leukoencephalopathy (PML), especially in patients treated for over 2 years, those with prior immunosuppressive therapy exposure, or those who are John Cunningham virus (JCV) antibody–positive with a high index.7,8
With the availability of high-efficacy disease-modifying therapies (DMTs), the risk of PML in NTZ-treated patients can be mitigated by switching treatments. However, NTZ is associated with a rebound phenomenon and severe disease reactivation risk. 9 The RESTORE trial showed that switching from NTZ to less efficacious DMTs, such as interferons, glatiramer acetate, or methylprednisolone, led to clinical relapses in 15%–29% of patients, with magnetic resonance imaging (MRI) activity detected as early as 12 weeks post-treatment cessation. 10 Similarly, real-world studies found breakthrough disease in patients switched from NTZ to dimethyl fumarate 11 or teriflunomide. 12
Only few small observational studies13–16 looked at efficacy and safety of fingolimod, ocrelizumab (OCR), rituximab (RTX), or cladribine after NTZ cessation.
The aim of this study was to compare the effectiveness, safety, and drug survival of switching from NTZ to other high-efficacy DMTs due to JCV Ab positivity.
Methods
Study setting and population
We conducted a multicenter retrospective observational study of patients with RRMS treated with NTZ for at least 6 months before switching to high-efficacy DMTs due to JCV Ab positivity. Patient data were obtained from the MENACTRIMS registry, the largest regional MS registry, 17 and local national registries from different countries in the MENA region, including Kuwait, Lebanon, United Arab of Emirates (UAE), Iraq, Oman, Algeria, and Tunis. Data were extracted and analyzed between October 2022 and March 2023. All patients diagnosed with RRMS according to the 2010 18 or 2017 19 McDonald criteria and fulfilling the following inclusion criteria were included in the study: age between 18 and 65 years, Expanded Disability Status Score (EDSS) between 0 and 6, treated with NTZ for at least 6 months before switching to another DMT due to positive serum JCV Ab or high antibody index (AI), and a follow-up period on the new DMT of at least 1 year or until drug discontinuation whichever comes first. Patients who discontinued NTZ treatment for other reasons than a positive JCV Ab or shifted to other DMTs after a wash out period longer than 3 months were excluded.
Outcomes
The study outcomes were annualized relapse rate (ARR), time to first relapse, confirmed disability progression (CDP), new MRI activity after switching to the new DMT, no evidence of disease activity (NEDA-3) defined as absence of relapses, new MRI lesions or disability progression, drug survival, and adverse events. The study baseline was defined as the date of initiation of the new DMT.
Relapse was defined as new or recurrent neurological symptoms lasting for more than 24 hours without fever or infection. 20 ARR was calculated by dividing the total number of relapses by the total number of person-years at risk. 21
The Expanded Disability Status Scale (EDSS) obtained within 6 months before or 3 months after switching to the new DMT was chosen as baseline. Disability progression was defined as 3 or 6 months sustained EDSS increase by ⩾1 point for a baseline EDSS between 2 and 5.5, or 0.5 points for an EDSS above 5.5, or 1.5 points for an EDSS between 0 and 1.5. 22
Baseline MRI was defined as the MRI scan performed at least 3 months after initiating the new DMT. Enhancing lesions and new T2 lesions on MRIs were calculated as proportion of patients with positive scans among patients with valid baseline and follow-up MRIs.
Registered adverse events were severe infections requiring medications, persistent lymphopenia for >3 months, increased liver enzymes ⩾3 times upper limit of normal, bradycardia, autoimmune disorders, hypersensitivity reactions, PML, and malignancies. The date of discontinuation of the new DMT was recorded as the date of last administration. Drug survival was defined as persistence on the new DMT during the observational period. Alemtuzumab treatment discontinuation was defined as beginning of an alternative DMT within the first year or when the decision against administration of the second treatment course was made. 23
Data collection
Patient data were recorded during routine clinic visits at participating centers via the locally installed iMed or MDS software programs. Data were collected from the MENACTRIMS and local MS registries using a standardized data collection sheet.
Standard protocol approvals
Ethical approval for the MENACTRIMS registry was granted by the American University of Beirut Ethics Committee. Approvals from local ethical committees in participating centers were also obtained.
Statistical analyses
Patient data were coded and entered for analysis in SPSS V28. Sample characteristics were summarized using frequency, proportion for categorical variable, mean and standard deviation or median and interquartile range for numerical data.
Number of relapses were counted and normalized per year duration to produce ARR, followed by multivariable modeling using the Poisson distribution to produce relative risk (RR), 95% confidence intervals (CIs), and p value.
Kaplan–Meier survival analysis was utilized to look at time for first relapse after switching to the new DMT. Log rank test produced p value comparing the different DMT.
CDP at 3 and 6 months was computed. Crude and adjusted odds ratio (OR) were computed using univariate and multivariable regression models adjusting for other statistically significant covariates.
MRI activity outcomes, new T2 lesions, and gadolinium-enhancing lesions were also counted and compared between the different DMT using the Pearson chi-square, and subsequently followed by the multivariable logistic regression to compute OR, 95% CI adjusted for the following confounding variables: age, sex, disease duration, washout period, baseline EDSS, EDSS upon initiating NTZ, ARR in the year preceding NTZ treatment, and duration of follow-up on the new DMT. All analyses were carried out at the 0.05 significance level.
Results
Study population
In total, 342 patients switched from NTZ due to JCV Ab positivity. We excluded 15 patients switching to low-efficacy DMTs (13 to interferon beta and 2 to teriflunomide and dimethyl fumarate). Six patients switching to cladribine and one to ofatumumab were also excluded due to small numbers. A total of 321 patients were included in the final analysis: 255 on RTX/OCR, 52 on fingolimod, and 14 on alemtuzumab (Figure 1).
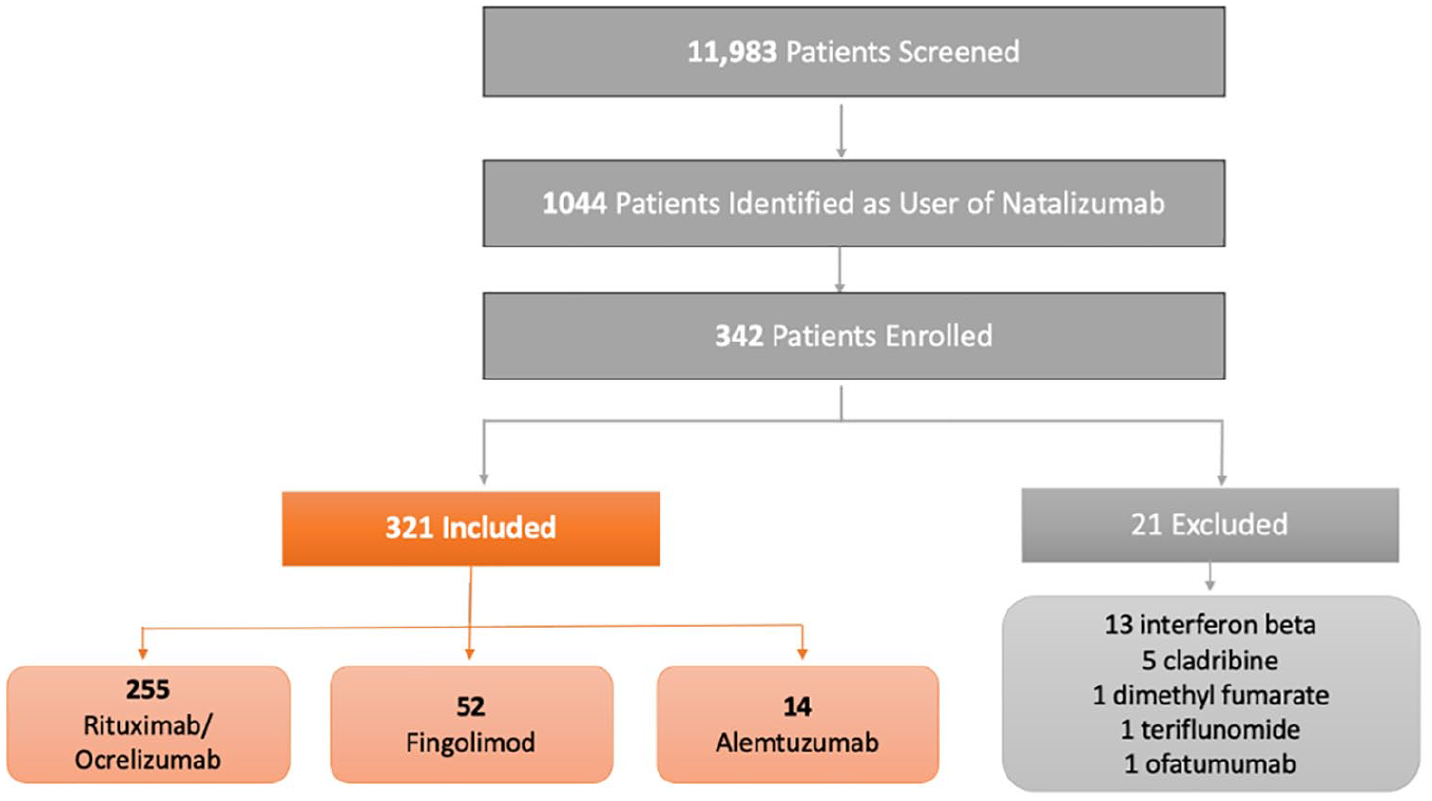
Flow chart of the included/excluded patients.
Baseline characteristics of the study population are shown in Table 1. The mean duration of follow-up on the new DMT was 2.4, 4.3, and 4.0 years on RTX/OCR, fingolimod, and alemtuzumab, respectively.
Baseline characteristics of the study population.
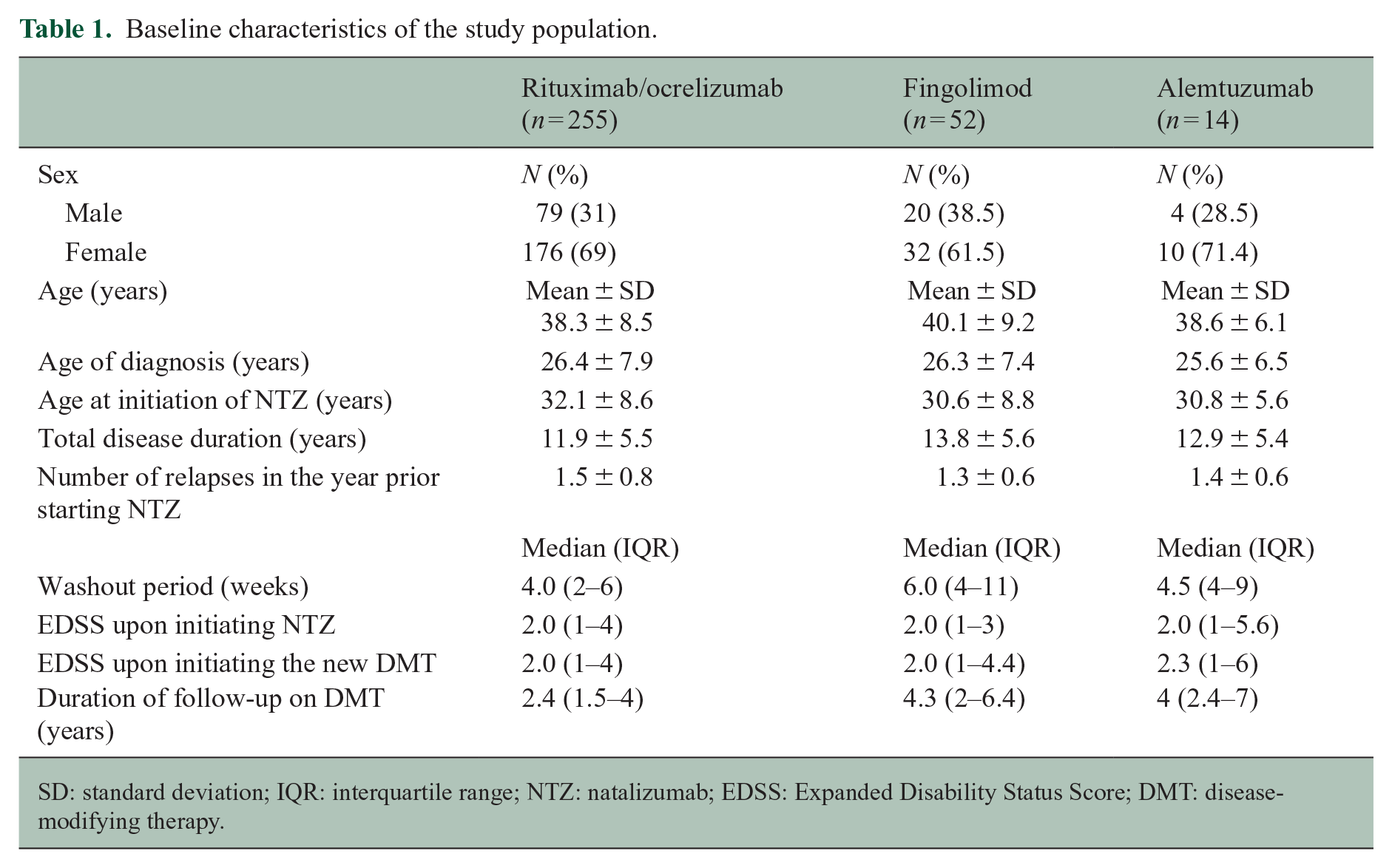
SD: standard deviation; IQR: interquartile range; NTZ: natalizumab; EDSS: Expanded Disability Status Score; DMT: disease-modifying therapy.
Effectiveness
Clinical relapses
Switching to RTX/OCR was associated with a statistically significant reduction in ARR compared with fingolimod (0.028 vs. 0.193; p value < 0.001). No significant difference in ARR was found between patients shifting to RTX/OCR versus alemtuzumab (0.028 vs. 0.032; p value = 0.987). Similar results were obtained when adjusting for the following confounding variables: age, sex, disease duration, washout period, baseline EDSS, EDSS upon initiating NTZ, ARR in the year preceding NTZ treatment, and duration of follow-up on the new DMT. The time to first relapse was significantly shorter in patients switching to fingolimod as compared with RTX/OCR, with a mean time of 6.7 ± 0.6 and 8.7 ± 0.1 years (p value < 0.001), respectively (Figure 2). There was no significant difference in time to first relapse between patients switching to RTX/OCR versus alemtuzumab. Only one patient had a relapse on the latter. The results were similar after adjusting for the selected confounding variables.
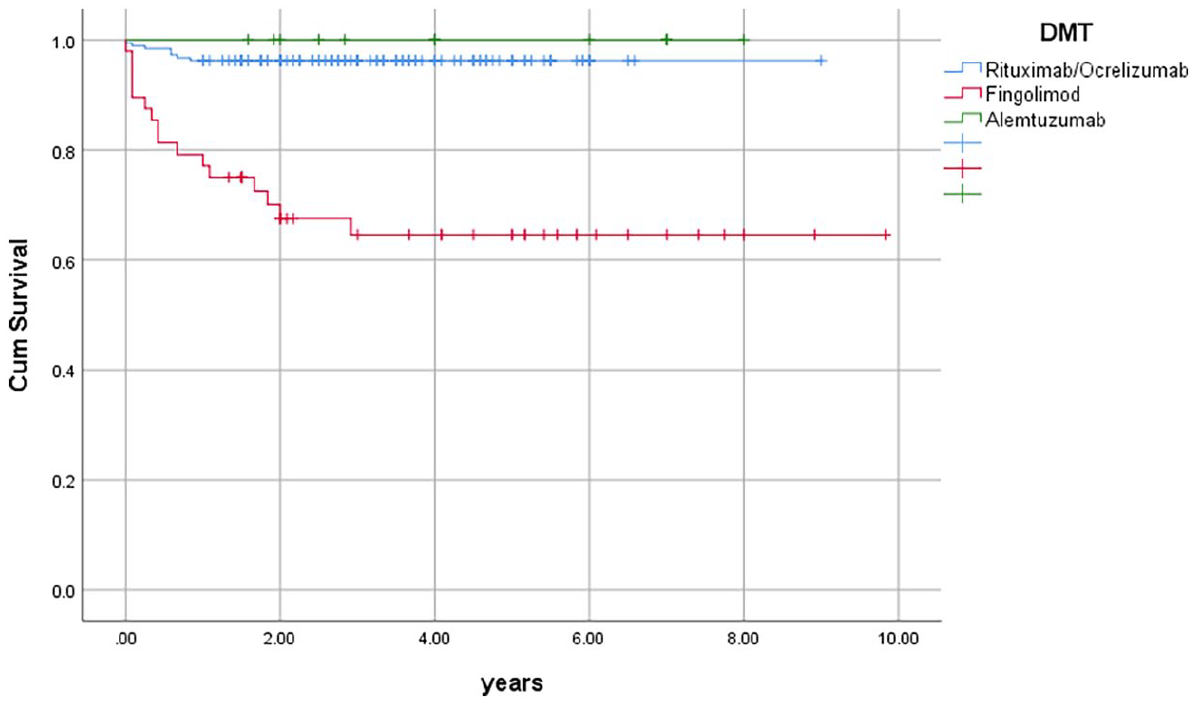
Time to first relapse on the new disease-modifying therapy.
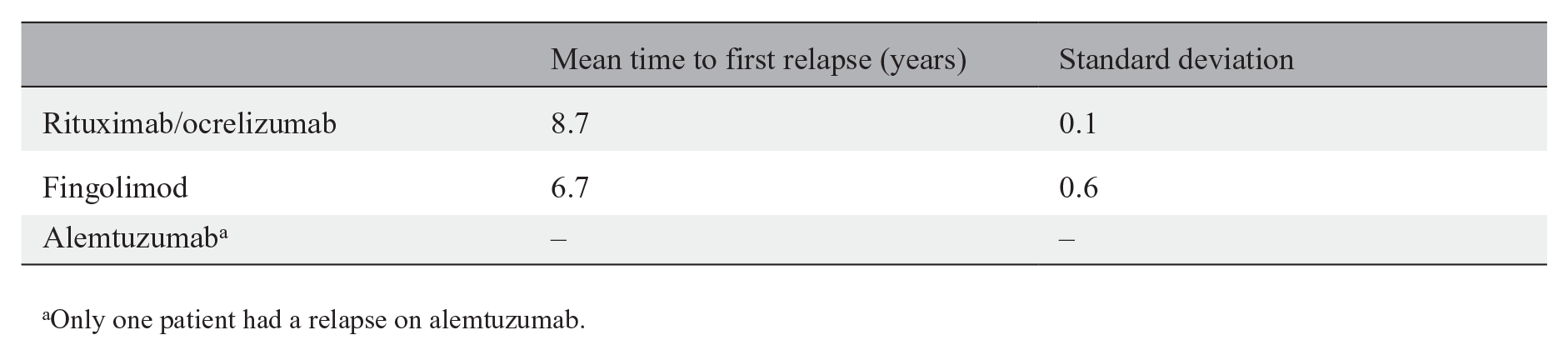
Only one patient had a relapse on alemtuzumab.
Disability progression
Compared with RTX/OCR, switching to fingolimod was associated with a significant increase in risk of 3- and 6-month CDP, even after adjusting for confounding variables (adjusted OR = 3.28; 95% CI = 1.06%–10.09% and 2.89; 95% CI = 1.06–7.87, respectively). Patients switching to alemtuzumab were not included in the disability progression analysis due to the small sample size (Table 2).
Confirmed 3- and 6-month disability progression on the new DMT.
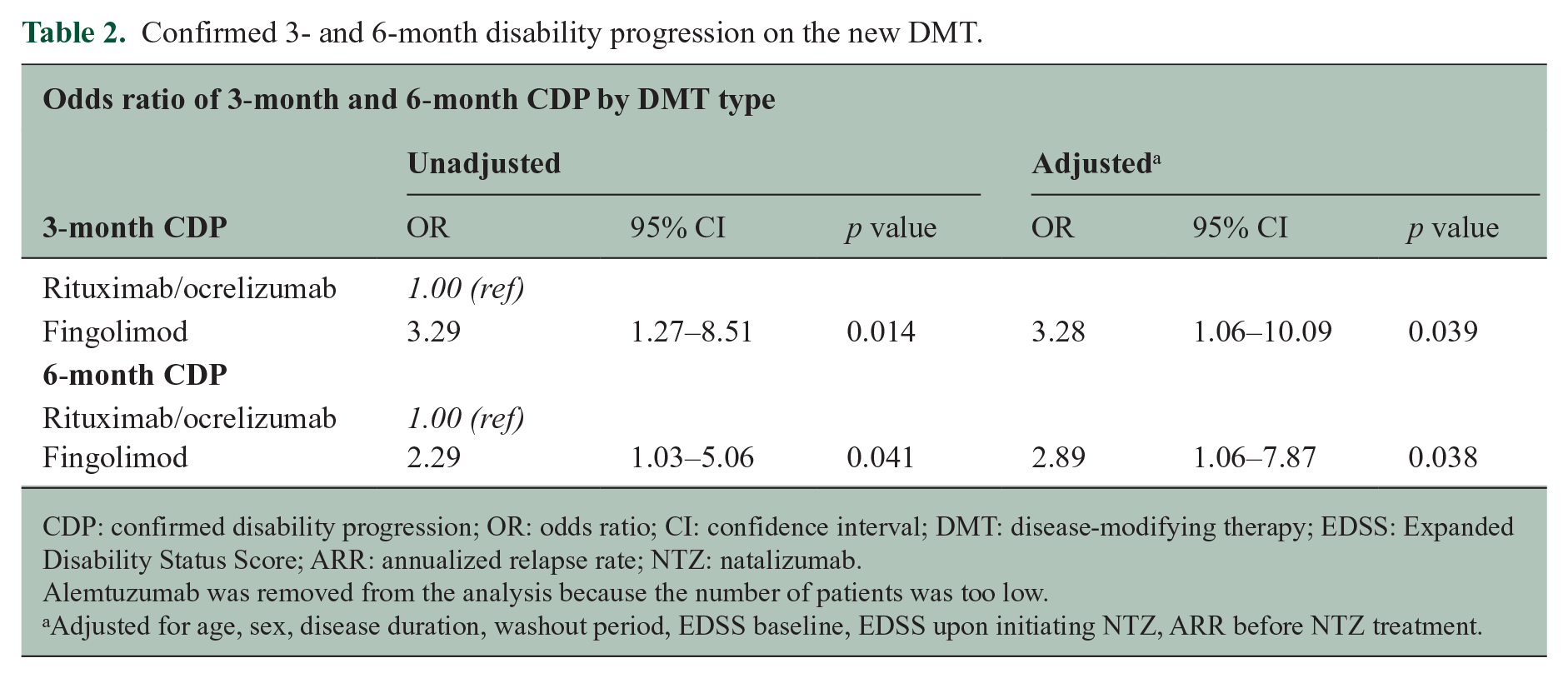
CDP: confirmed disability progression; OR: odds ratio; CI: confidence interval; DMT: disease-modifying therapy; EDSS: Expanded Disability Status Score; ARR: annualized relapse rate; NTZ: natalizumab.
Alemtuzumab was removed from the analysis because the number of patients was too low.
Adjusted for age, sex, disease duration, washout period, EDSS baseline, EDSS upon initiating NTZ, ARR before NTZ treatment.
MRI activity
Due to the small number of patients with valid MRI scans in the alemtuzumab group (n = 3), alemtuzumab was not included in the MRI analysis. A higher proportion of new T2 lesions were detected in patients shifting to fingolimod compared with RTX/OCR (66.6% vs. 24.0%; p value < 0.001) (Table 3). Similar results were obtained for Gd+ lesions with a higher proportion of patients with Gd+ lesions on fingolimod compared with RTX/OCR (62.9% vs. 13.0%, p value < 0.001). Figure 3 shows that after adjusting for confounding variables, the proportion of patients with new T2 or Gd+ lesions was still lower on RTX/OCR compared with fingolimod (OR = 0.58; 95% CI = 0.35%–0.80% and 0.54; 95% CI = 0.33–0.76, respectively).
MRI outcomes on the new DMT.
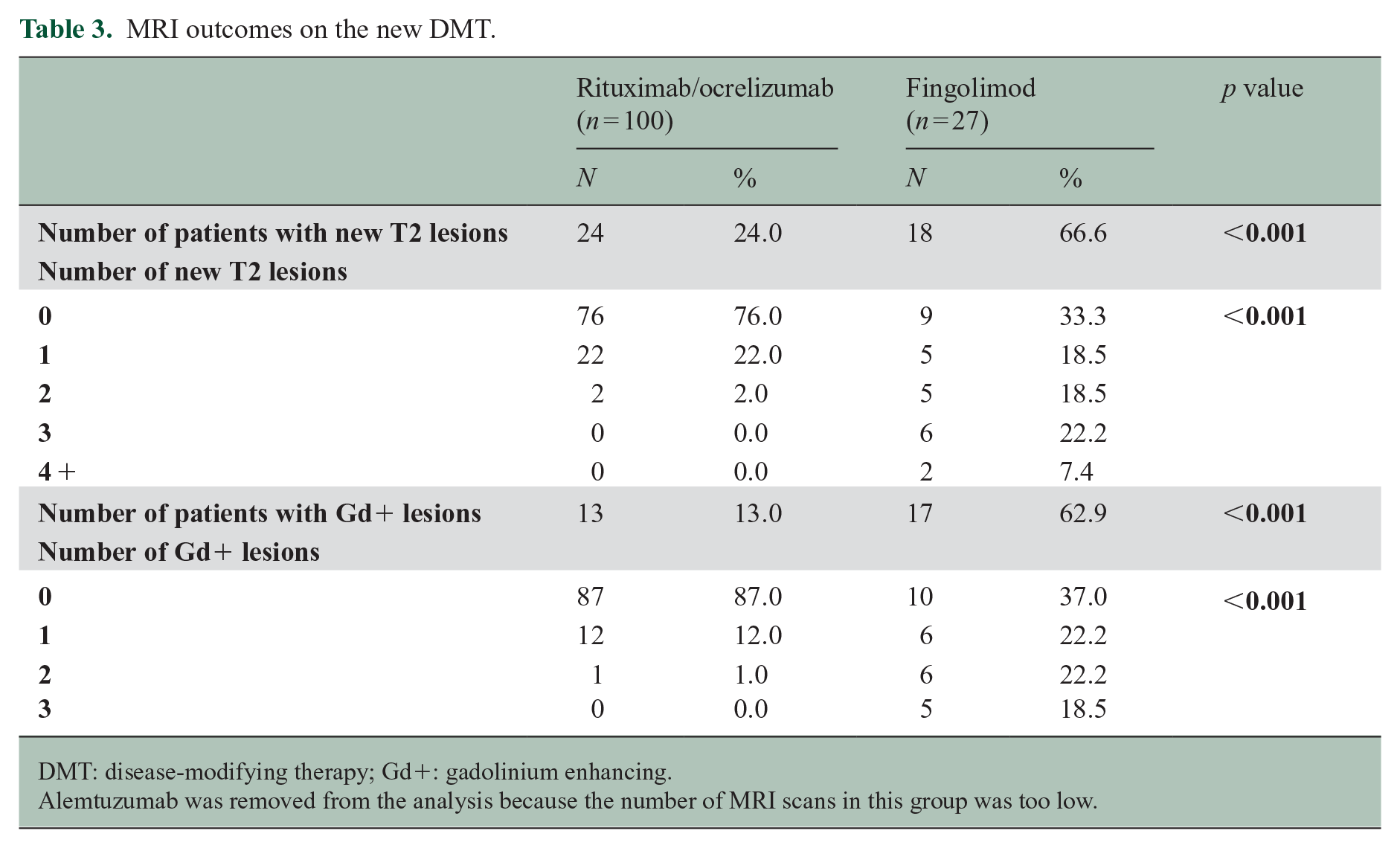
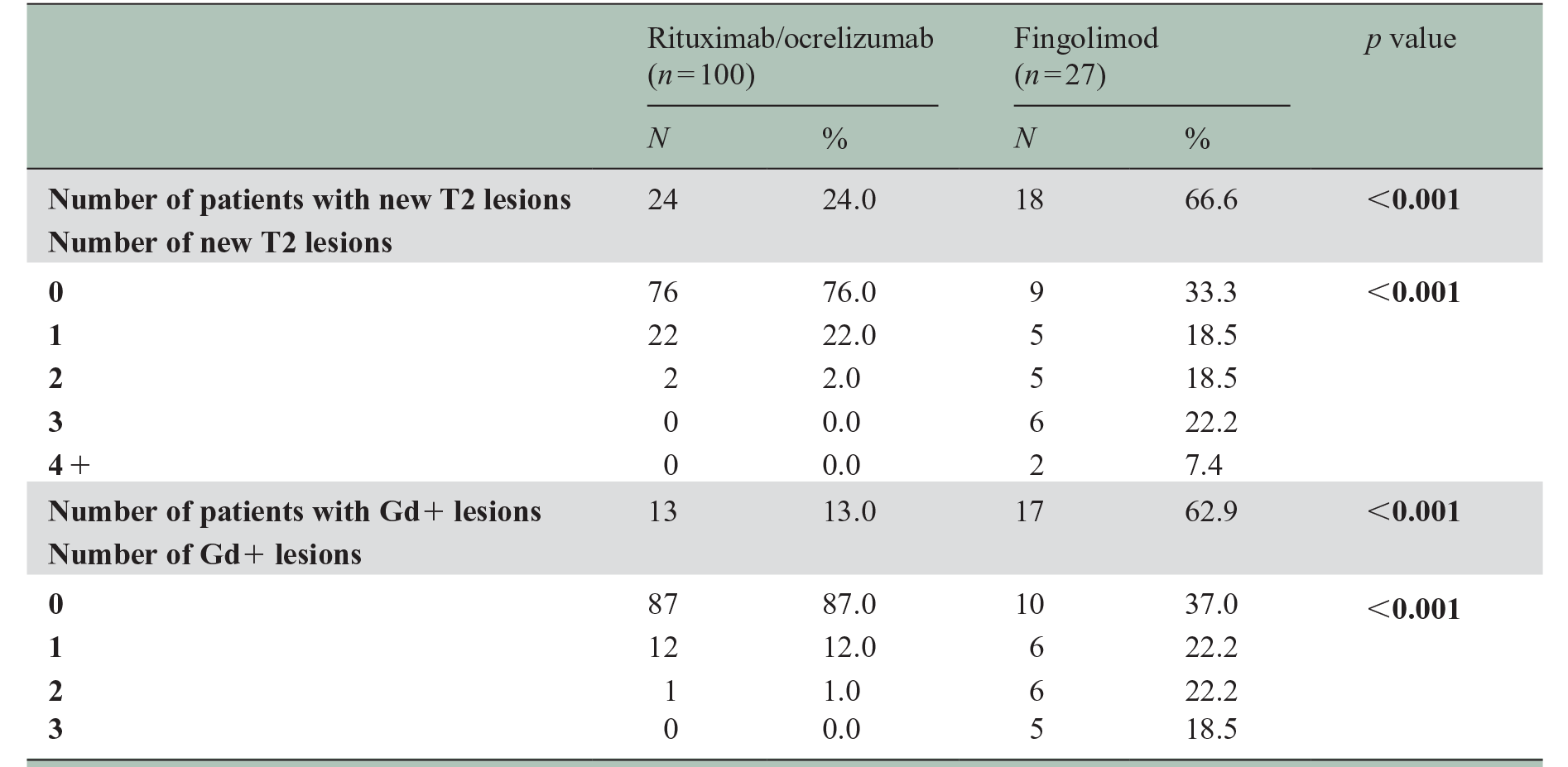
DMT: disease-modifying therapy; Gd+: gadolinium enhancing.
Alemtuzumab was removed from the analysis because the number of MRI scans in this group was too low.
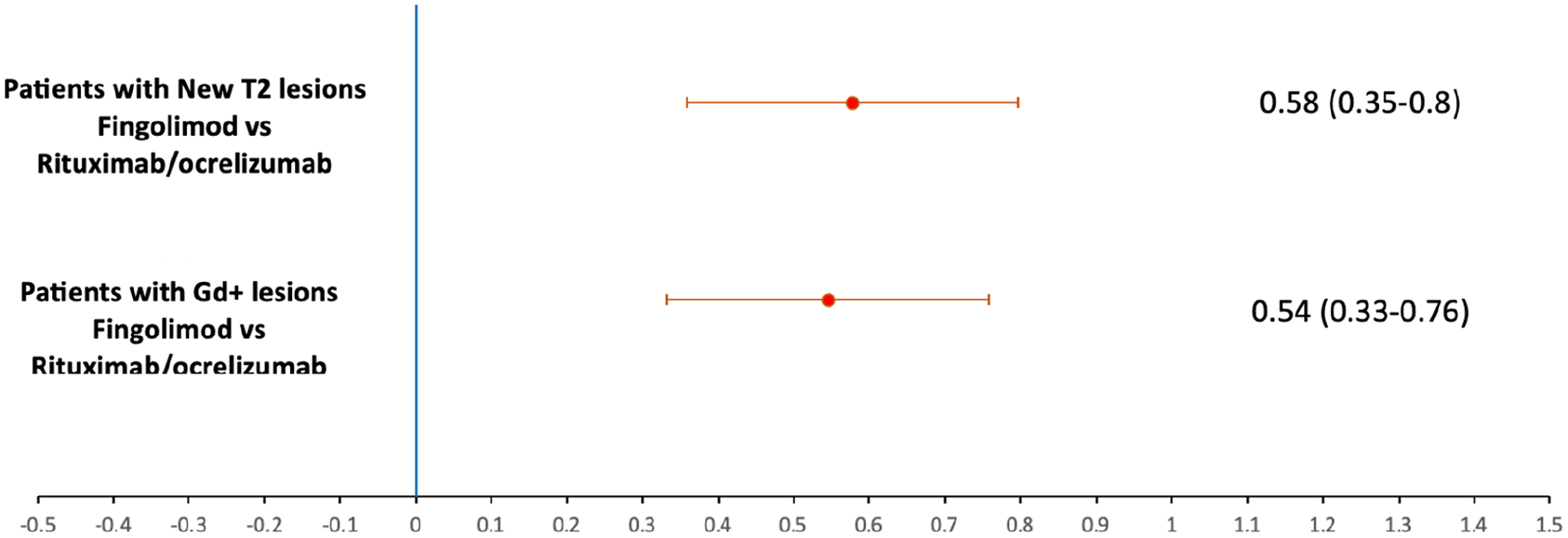
Forest plot for MRI activity after adjusting for confounding factorsa.
The alemtuzumab group was not included in the NEDA-3 analysis due to the small number of patients with MRI. A higher proportion of patients on RTX/OCR achieved NEDA-3 compared with fingolimod: 74.9% (191/255) versus 40.4% (21/52); p value < 0.001.
Safety
Patients on alemtuzumab experienced the highest frequency of adverse events (4/14 patients with autoimmune thyroiditis) compared with fingolimod and RTX/OCR (28.6%, 21.2%, and 8.6%, respectively). Lymphopenia, increased liver enzymes, and bradycardia were more commonly seen in patients on fingolimod. There was one case of PML (considered a carry-over from NTZ) and one case of breast cancer on RTX and OCR, respectively (Table 4).
Adverse events.
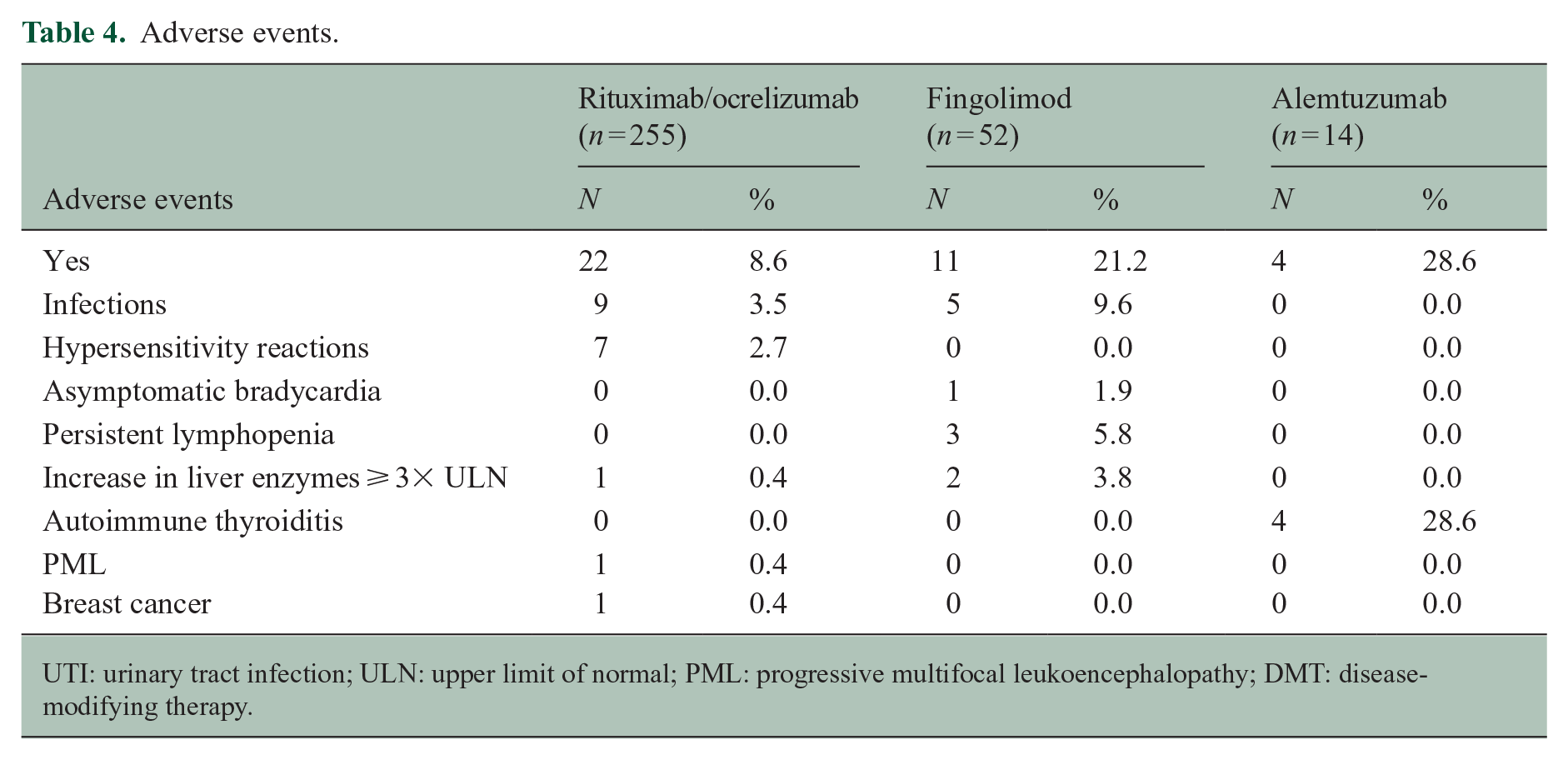
UTI: urinary tract infection; ULN: upper limit of normal; PML: progressive multifocal leukoencephalopathy; DMT: disease-modifying therapy.
Drug survival
A total of 31/52 patients (59.6%) on fingolimod discontinued treatment compared with 8/255 (3.1%) on RTX/OCR. The mean drug survival was 8.5 years on RTX/OCR compared with 5.6 years on fingolimod (p value < 0.001) (Figure 4). The reasons for discontinuation of fingolimod were treatment failure (20/31 (64.5%)), adverse events (7/31 (22.6%)), and pregnancy (4/31 (12.9%)), and for RTX/OCR, patient preference (3/8 (37.5%)), treatment failure (2/8 (25%)), adverse events (2/8 (25%)), and pregnancy (1/8 (12.5%)). None of the patients on alemtuzumab fulfilled the criteria for treatment discontinuation, but three patients received a third cycle due to breakthrough disease.
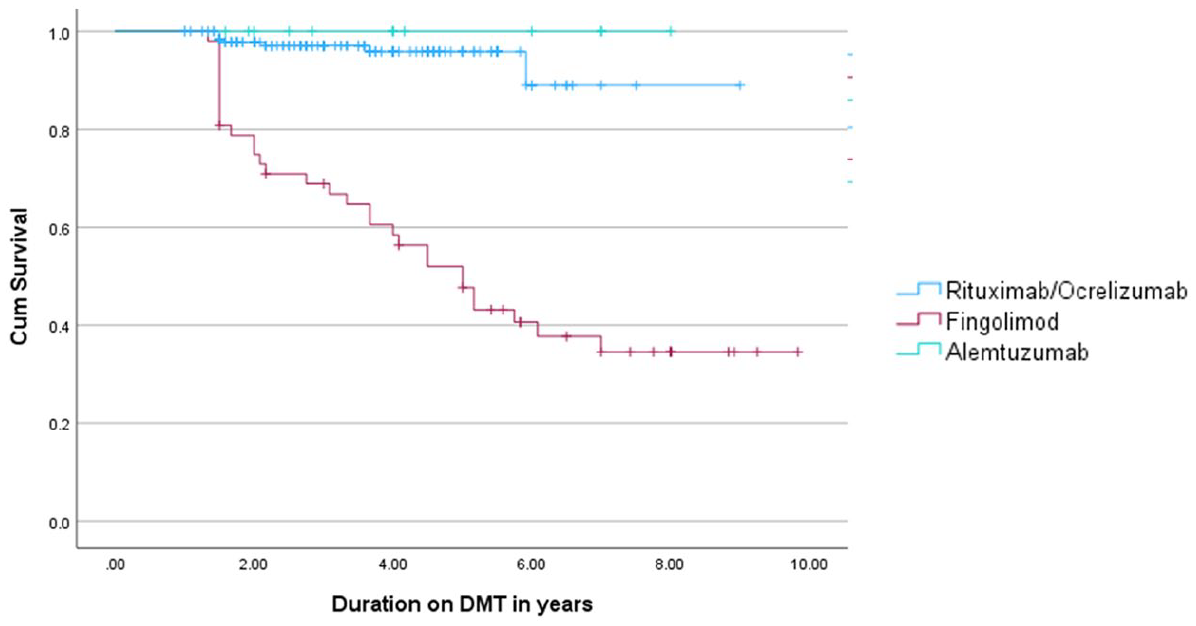
DMT survival.
Discussion
In this observational retrospective cohort study, we compared the effectiveness, safety, and drug survival of RTX/OCR, fingolimod, and alemtuzumab after switching from NTZ due to JCV Ab positivity. Compared with fingolimod, RTX/OCR and alemtuzumab were associated with significant reduction in ARR and time to first relapse and had a longer drug survival. Patients switching to RTX/OCR had less disability progression, fewer new T2 and Gd+ lesions, and higher rates of NEDA-3 compared with fingolimod. The results were similar after adjusting for the selected confounding variables. Due to the low number of patients switching to alemtuzumab, the latter was not included in the disability progression, NEDA-3, and MRI activity analyses. The safety profile also favored RTX/OCR versus both fingolimod and alemtuzumab with higher rate of infections, liver toxicity, and lymphopenia on fingolimod and autoimmune thyroiditis on alemtuzumab. It is of note, however, that there was one case of PML and one case of breast cancer on RTX and OCR, respectively. The better drug survival of RTX/OCR and alemtuzumab compared with fingolimod was mainly due to a higher rate of treatment failure on fingolimod.
To our knowledge, this is the first study comparing the effectiveness, safety, and drug survival of RTX/OCR, alemtuzumab, and fingolimod after switching from NTZ. It is of note that to date, no randomized controlled trial comparing the efficacy and safety of switching from NTZ to high-efficacy DMTs due to JCV Ab positivity has been performed.
In a Swedish multicenter study of 256 patients switching from NTZ to RTX or fingolimod due to JCV Ab positivity, RTX was associated with significantly lower relapse rates (1.8% vs. 17.6%), Gd+ lesions (1.4% vs. 24.2%), and treatment discontinuation rates (1.8% vs. 28.2%) during 1.5 years of follow-up. 24 Our study showed similar results when comparing RTX/OCR with fingolimod over a longer follow-up period (2.4–4.3 years). 25 Similar outcomes were reported in a large retrospective observational MSBase registry study 25 comparing the effectiveness and treatment discontinuation rates in patients switching from NTZ to dimethyl fumarate, fingolimod, or OCR. Patients on fingolimod had higher ARRs (OR = 4.33; 95% CI = 3.12–6.01), increased risk of disability progression (49%), and higher treatment discontinuation rates (OR = 2.57; 95% CI = 1.74–3.80) compared with OCR.
In a retrospective French study, 26 48 patients on OCR were compared with 54 on fingolimod after NTZ cessation. Patients on OCR had a significantly lower ARR after 1 year (0.12 vs. 0.41, p = 0.026), similar to our findings.
In a retrospective multicenter German study, 27 101 patients receiving fingolimod were compared with 42 patients receiving alemtuzumab after NTZ cessation. Similar to our study, patients on fingolimod had higher relapse rate (OR = 2.24; 95% CI = 1.12–4.50), disability progression (OR = 4.84; 95% CI = 1.74–13.47), and MRI progression (OR = 2.41; 95% CI = 1.26–4.60). Unlike our study, adverse events were much more common in patients receiving fingolimod compared with patients receiving alemtuzumab (OR = 7.78; 95% CI = 1.04–57.95). Patients, however, were only followed for 1 year, knowing that the most common adverse events of alemtuzumab, namely, autoimmune disorders, peak in the third year of treatment.
In a recent study, Santiago-Setien et al. assessed clinical outcomes in 30 patients maintained on NTZ extended interval dosing or shifted to OCR. There were no significant differences in ARR, radiological activity, or disability progression between the two groups. 28
Our study has several limitations. The retrospective observational design could have introduced a selection bias. However, adjusting for multiple confounding variables did not alter the outcomes. Combining both B-cell-depleting therapies (OCR and RTX) into a single group might have obscured any differential effects between them, but most studies have shown similar effectiveness and safety profiles for both DMTs. For instance, a retrospective multicenter Italian study found that OCR and RTX had similar reductions in ARR and MRI activity in patients switching from NTZ. 29 In addition, we could not determine the JCV Ab index due to inconsistent reporting in the registries. We also lacked detailed information on the dosage and interval dosing of NTZ and the B-cell-depleting therapies. Some patients on RTX received doses ranging from 500 to 1000 mg at intervals of 6 to 12 months, a common practice in the MENA region. However, previous studies have indicated that such variations in dosing or treatment interval did not affect the effectiveness of RTX.30–32
The strengths of this study include the large number of patients and long follow-up duration compared with most previous studies. It is also, to our knowledge, the first study to compare RTX/OCR, fingolimod, and alemtuzumab as potential exit strategies in patients on NTZ and JCV Ab positivity.
Conclusion
Our study showed that in patients switching from NTZ due to JCV Ab positivity, RTX/OCR showed higher effectiveness and better safety profile compared with fingolimod. Compared with alemtuzumab, RTX/OCR had similar effectiveness but better safety profile.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: M.Z. has received honoraria for lectures from Biologix, Biogen, Janssen, Hikma Pharmaceuticals, Novartis, Merck, Roche, and Sanofi-Genzyme. She received travel grants from Novartis, Merck, and Roche and a research grant from Biogen. She received two research grants from Biogen, one research grant from Merck, and two research grants from MENACTRIMS. She has no conflict of interest related to this study. B.Y. has received speaker honoraria from Bayer, Biogen, Merck, Novartis, Roche, and Sanofi; research grants from Bayer, Biogen, Merck, Novartis, and Pfizer; and advisory board honoraria from Bayer, Biogen, Merck, Novartis, Roche, and Sanofi. He has no conflict of interest related to this study. A.A.-A. has received honoraria from Novartis, Sanofi, Biologix, Merck, Roche, Biogen, and Bayer. He serves on the scientific advisory boards of Novartis, Merck, and Roche. He has no conflict of interest related to this study. R.G. has received research grant from Roche and advisory board honoraria from Biogen, Hikma, Merck, Roche, and Sanofi. He has no conflict of interest related to this study. S.M. received a MENACTRIMS clinical research grant (2020) but has no conflict of interest related to this study. R.A.-R., S.F.A., S.K., N.E.-A., A.A.-M., J.A.-K., A.C., J.I., N.S., J.M., F.M.R.H.M., A.A.-H., P.S., H.D., and F.B. declare that there is no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a research grant from Biogen. The funder had no role in study design, data collection and analysis, decision to publish, or preparation of this presentation.