
Abstract
Background:
A latent period of variable length elapses between multiple sclerosis (MS) biological onset and the occurrence of the first clinical episode reflecting a central nervous system (CNS) demyelinating event. Factors affecting the duration of such interval are unknown.
Objective:
To explore whether brain reserve, which moderates the impact of structural damage along MS course, could also affect the timing of MS clinical onset.
Methods:
We conducted a time-to-event analysis in 326 relapsing-onset multiple sclerosis patients to ascertain the effect of brain reserve, that is, larger maximal lifetime brain growth (MLBG) estimated as intracranial volume, on the risk of an earlier disease onset. For this purpose, we carried out a Cox proportional hazards regression model stratified by sex and adjusted by site and pre-morbid MS risk factors. All patients reached the event (i.e. the disease onset) with no censored case; the age (years) at disease onset was set as the main time variable.
Results:
We identified a protective effect of brain reserve on the time to disease onset (HR = 0.11, 95% CI = 0.02–0.83, p = 0.032), unchanged when accounting for MS risk factors.
Conclusion:
Brain reserve might counteract the pathological mechanisms ongoing after biological initiation, thus delaying the disease overt clinical manifestation.
Keywords
Introduction
Brain reserve, that is, larger maximal lifetime brain growth (MLBG; determined by genetics) moderates the impact of structural damage on clinical disability in multiple sclerosis (MS), counteracting cognitive efficiency decline and motor disability progression.1,2 Indeed, over a medium-term follow-up (4.5 and 5 years, respectively), larger MLBG protected against decline in Symbol Digit Modalities Test and Paced Auditory Serial Addition Task performance 1 and predicted lower risk for Expanded Disability Status Scale progression, independently of cerebral atrophy and demyelinating lesion burden. 2 Considering that brain tissue damage occurs since the very early stages of the MS continuum,3–5 we explored whether MLBG protective effect against the impact of structural damage, which has been reported after MS clinical onset, 2 could also extend to the period predating MS overt clinical manifestation, thus affecting the timing of MS onset. Indeed, so far, few individual risk factors for MS have been identified, 6 and no data are available on features that might modulate the relationship between MS biological and clinical onset. Over the past years evidences drawn from population studies have supported the need for a revision of MS natural history, suggesting that a subclinical phase, potentially followed by the occurrence of non-specific clinical signs and symptoms (prodromal stage), intervenes between the disease biological onset in susceptible individuals and its classical clinical presentation. 7 Prodromal symptoms, although might not develop in all individuals, might connotate subjects who are at high risk of developing classical MS. 7 Here, we explored whether (1) brain reserve might exert an impact on age at disease onset and (2) the impact of brain reserve on age at disease onset might still be observed when accounting for individual MS risk (susceptibility related to exposure to risk factors and occurrence of prodromal symptoms).
Methods
Study population
Clinical and magnetic resonance imaging (MRI) data were retrospectively retrieved from the MS Centre databases of S. Andrea and S. Camillo Forlanini Hospitals in Rome. Inclusion criteria were (1) diagnosis of MS according to the 2017 McDonald criteria, (2) relapsing-onset MS and (3) availability of a 3D T1-weighted image, acquired at 1.5 Tesla (GE Signa n = 154, Siemens Avanto n = 172) at any time during the disease course. Indeed, as MLBG is genetically determined and independent from MS disease burden,1,8 its estimation can be carried out at any point during MS course.
We excluded (1) patients with missing information about known/putative risk factors for MS in the clinical databases and (2) patients experiencing an insidious development of neurological symptoms with subsequent irreversible disability, whose exact onset date cannot be determined, suggesting a primary progressive disease course.
Demographic and clinical data
Demographic and clinical data included sex, age at disease onset, that is, the date of the first demyelinating event as reported by patients or their relatives. We also collected pre-morbid known or putative risk factors according to previous literature 6 including pre-onset childbirths, pre-onset smoking (pack/year), adolescent overweight (BMI > 25 kg/mq) or obesity (BMI > 30 kg/mq), 9 familial history of MS, adolescent coastal proximity (https://gisportal.istat.it/sezionilitoranee/) as proxy of 25(OH)D level 10 and self-reported prodromal symptoms (e.g. fatigue, anxiety, depression, pain, urinary hesitancy, constipation). 7 Information about prodromal symptoms was entered in the MS Centre database as part of the patient’s history. Specifically, questions about prodromal symptoms were asked during the first encounter/periodic follow-up with the patient at the treating MS Centre, using a prespecified check list (see Supplemental material for details). The mean interval between MS onset and collection of information about prodromal symptoms in our population was 4.44 ± 5.99 years, with a trend towards shorter interval in patients reporting than in not reporting prodromal symptoms (3.22 ± 4.60 vs 5.53 ± 6.26, p = 0.06). As the length of the prodromal phase in MS is unknown and prodromal symptoms have been reported up to 17 years before MS onset, 11 no specific time-frame was indicated when collecting information about self-reported prodromal symptoms.
MLBG estimation
Individual 3D T1-weighted images were analysed with SIENAX (https://fsl.fmrib.ox.ac.uk/fsl/fslwiki/SIENA). MLBG was expressed as the reciprocal of the SIENAX volume scaling factor (driven by registration of the external surface of the skull), so that larger values correspond to larger intracranial volume (ICV), regression-adjusted for sex. 2
Statistical analysis
A time-to-event analysis was conducted to ascertain the effect of ICV on the risk of an earlier disease onset. For this purpose, we carried out a Cox proportional hazards regression model stratified by sex and adjusted by site to account for between-scanner difference in ICV estimation. All patients reached the event (i.e. the disease onset) and there was no censored case; the age (years) at disease onset was set as the main time variable. We explored the impact of MLBG on age at disease onset by a univariate Cox analysis. Given that MLBG is reached at age 15 12 and that the onset of MS during childhood affects the age-expected brain growth, 13 we then repeated the Cox models after removing cases with early-onset MS (<16 years) and, in another analysis, cases with disease onset <20 years to account for gap between the biological and clinical disease onset. 14 Finally, we ran a multivariable Cox analysis by entering pre-morbid known or putative MS risk factors as covariates to confirm the influence of MLBG on disease onset, regardless of other variable potentially influencing the clinical MS onset; pre-onset childbirths and smoking were handled as time-varying covariates, with a value of 0 until either pregnancy or starting smoking, and changes to 1 thereafter. Self-reported prodromes were entered in the model as dichotomous variable.
Ethics statement
All data were gathered after obtaining an informed consent from each participant, and after notification to our institutional ethical committee (Comitato Etico Lazio 1; email: comitatoeticolazio1.it) that provided exemption of approval for non-interventional retrospective studies. In no way did this study interfere in the care received by patients.
Results
We analysed data of 326 MS patients (Table 1). Mean (standard deviation) ICVs were 0.69 (0.05) and 0.79 (0.06) for females and males, respectively. We found no difference in estimation of ICV across the two sites.
Clinical and demographic features of the study population (n = 326).
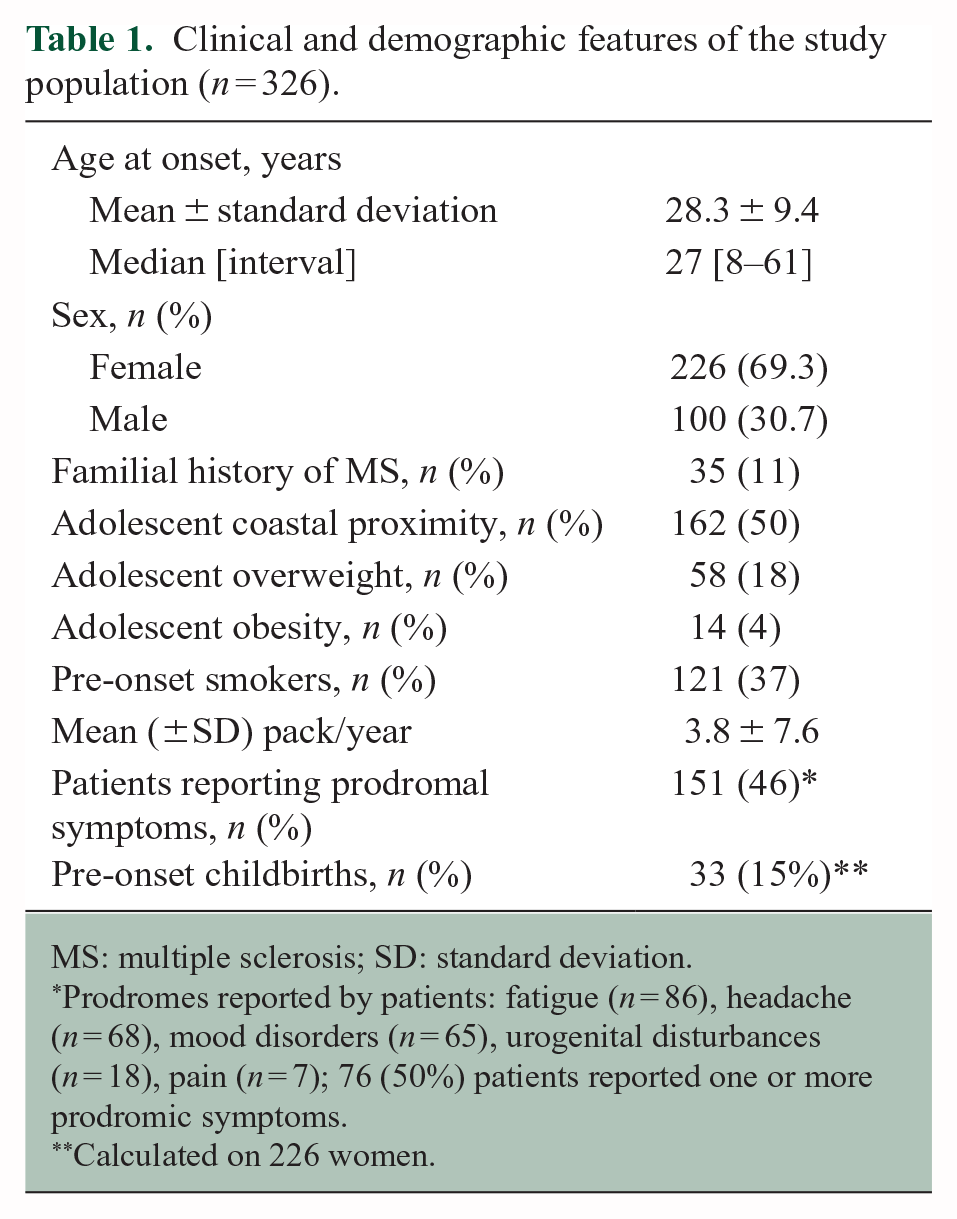
MS: multiple sclerosis; SD: standard deviation.
Prodromes reported by patients: fatigue (n = 86), headache (n = 68), mood disorders (n = 65), urogenital disturbances (n = 18), pain (n = 7); 76 (50%) patients reported one or more prodromic symptoms.
Calculated on 226 women.
We found a protective effect of larger ICV on the time to disease onset: hazard ratio (HR) = 0.11, 95% confidence intervals (CIs) 0.02–0.83, p = 0.032 (Figure 1); we obtained similar results by using a Spearman Rank correlation analysis (rho = 0.17, p = 0.003).
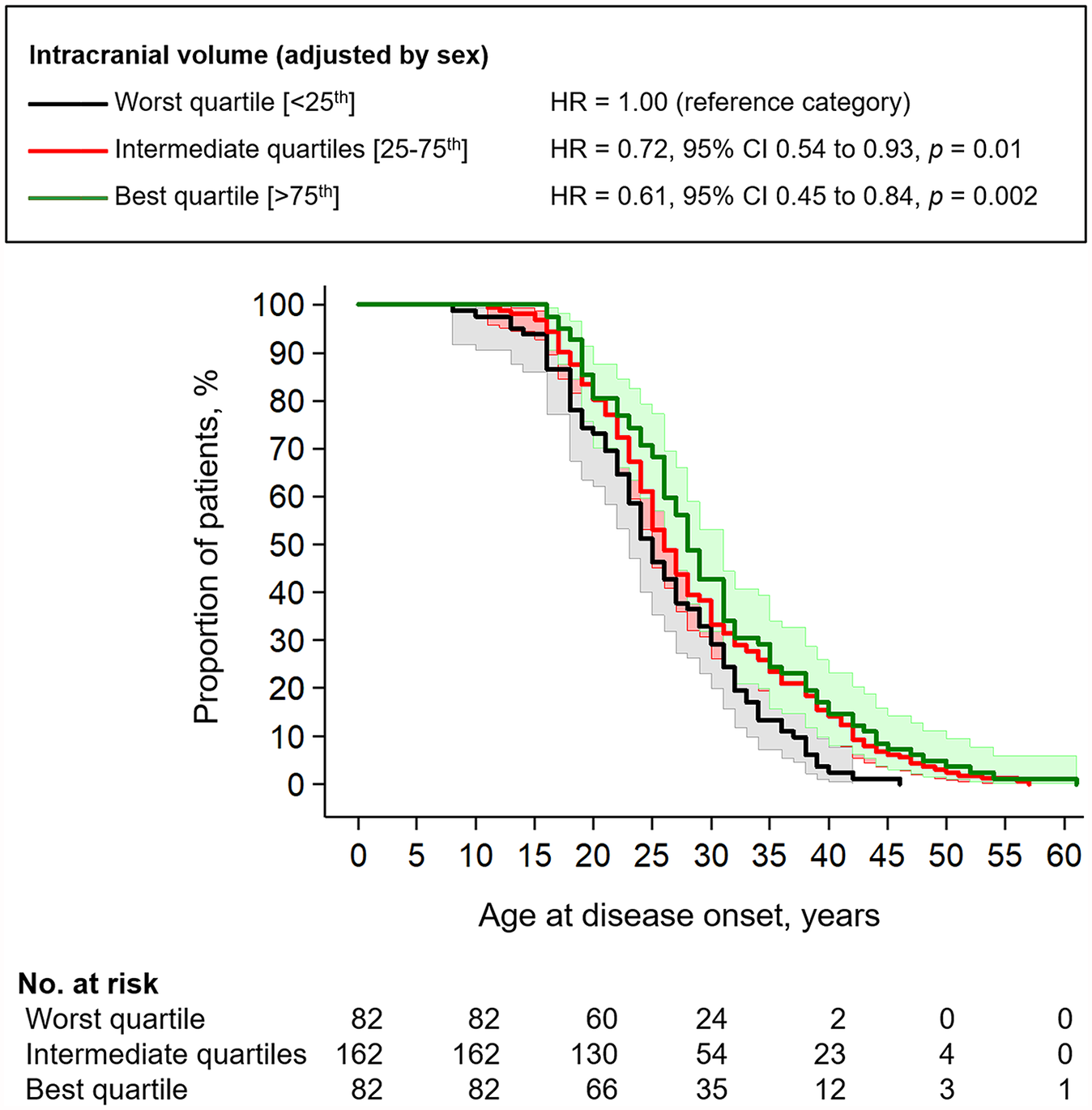
Kaplan–Meier curve, with 95% confidence intervals, for the age at disease onset according to intracranial volume; p = 0.005 by the Log-Rank test.
We obtained quite consistent findings after removing 10 patients with early-onset MS (<16 years; HR = 0.10, 95% CI = 0.01–0.86, p = 0.038) and even after removing 38 patients with disease onset <20 years (HR = 0.15, 95% CI = 0.02 to 1.15, p = 0.068). Similar findings were found by using a Spearman Rank correlation analysis (rho = 0.13–0.14, p < 0.02).
Notably, the association between older age at disease onset and larger ICV remained significant even in a multivariable model where known and putative risk factors were inserted as covariates (HR = 0.05, 95% CI = 0.01–0.98, p = 0.048). In the meanwhile, we found an association between self-reported prodromes and older age at disease onset: HR = 0.65 (95% CI = 0.47–0.90), p = 0.010. The number of pre-onset childbirths was also related with an older age at disease onset when compared with nulliparous women: HR for two pre-onset childbirths (n = 9) = 0.98 (95% CI = 0.96–0.99, p = 0.008); HR for one pre-onset childbirth (n = 33) = 0.99 (95% CI = 0.97–1.01, p = 0.11). There was no association between age at disease onset and the other explored factors, including adolescent overweight or obesity, familial history of MS, and adolescent coastal proximity.
Discussion
MS clinical onset is preceded by a latent period intervening between the biological onset of the pathology and the manifestation of typical symptoms allowing MS diagnosis.7,14–16 Health-care usage in adults and children is greater in the years before their first demyelinating event,17,18 with reasons for seeking medical attention including headache and other pain-related disorders, fatigue, urinary symptoms and psychiatric symptoms.19–23 Studies resorting to patients questionnaires have confirmed these data, identifying a mixture of specific symptoms, possibly related to a first demyelinating event, and non-specific symptoms in the years preceding MS diagnosis. 11 Given the current impossibility to identify the initiation of MS pathobiology, factors affecting the duration of MS prodromal stage are unknown. Larger MLBG is expression of larger neuronal count and synaptic density,24,25 which provide an efficient substrate to functional connections and result in higher threshold of susceptibility and higher compensation capability towards the accrual of structural damage.26,27 Here, we hypothesize that reserve might affect the individual course of MS not only during the symptomatic phase, 28 but also in the period predating the occurrence of the first clinical episode reflecting a central nervous system (CNS) demyelinating event, counteracting the ongoing pathological mechanisms and delaying their clinical manifestation. Our findings support this hypothesis, showing an association between larger brain reserve and greater age at MS onset that, despite the relatively small sample size, was confirmed after excluding early-onset patients (age at onset <16 years). When removing patients with age at onset <20 years a similar trend was identified, although results did not reach the statistical significance due to insufficient power.
The association between MLBG and age at onset remains significant when accounting for known and putative risk factors for MS. Among these, only self-reported prodromes and pre-onset childbirths seem to modulate MS onset time; on the contrary, there is no association with adolescent overweight or obesity, familial history of MS and adolescent coastal proximity. Although biological mechanisms sustaining non-specific symptoms occurring during MS prodromal stage are unknown, 7 these might represent the clinical counterpart of diffuse neuroaxonal damage 15 preceding, for a length of time modulated by other individual end environmental factors, the overt inflammatory disease onset. Although prodromal symptoms occur both in paediatric and adult-onset MS, 7 we cannot exclude that patients experiencing a longer prodromal phase (people with later clinical onset, i.e. higher age at onset) could be more likely to experience prodromal symptoms, suggesting a reverse causality as driver of the association between prodromal symptoms and onset time.
A reverse causality phenomenon cannot be excluded also for the protective effect of pre-onset childbirths, with patients experiencing a later clinical onset more likely to have had children before the occurrence of the first demyelinating event.29,30 In addition, pre-onset childbirths might not play a protective role in all women, as pregnancy does not seem to modify MS risk in genetically susceptible women. 31 Finally, cumulative duration of breastfeeding is associated with a decreased risk of MS, 32 possibly confounding the association between MS risk and parity/pregnancy.
This work is not free from limitations. We have utilized SIENAX scaling factor, a widely applied proxy of ICV, for MLBG estimation. Although this represents a rough measure of pre-morbid brain resilience and compensation capability, no better proxy is currently available, nor will it be until we will be able to clearly identify patients in MS prodromic stage. Further studies, testing the role of brain reserve in modulating clinical conversion in patients with radiologically isolated syndrome, might help strengthen our hypothesis. The lack of data on the Epstein–Barr virus (EBV) infection status is another limit, given its role as risk factor for MS. 33 To date, no standardized criteria for prodromal MS identification exist and previous works on the topic have drawn information from either health-care records or patient questionnaires. 7 Here, as no standardized questionnaire has been developed so far, we relied on a self-checklist of possible prodromal symptoms according to the existing literature. 6 This approach, however, intrinsically suffers from recall bias, as prodromal symptoms may occur many years before MS clinical onset and subsequent diagnosis. 11 Indeed, patients reporting prodromal symptoms in this study had shorter disease duration that patients denying prodromal symptoms. Finally, although the lack of association between age at disease onset, adolescent overweight or obesity, familial history of MS, and adolescent coastal proximity seem to suggest that these factors, while representing a risk for MS, do not modulate the length of MS latent period, the relatively small sample size of our study does not allow to reach a definite conclusion.
Despite these limitations, our findings suggest a role for brain reserve in modulating timing of clinical onset in MS, contributing to the recently growing body of knowledge on the period between MS biological onset and first overt manifestation. In prospect, gaining insight into such phase might favour the application of preventive strategies or early treatments limiting the accrual of irreversible damage.
Supplemental Material
sj-docx-1-msj-10.1177_13524585241272046 – Supplemental material for Brain reserve and timing of clinical onset in multiple sclerosis
Supplemental material, sj-docx-1-msj-10.1177_13524585241272046 for Brain reserve and timing of clinical onset in multiple sclerosis by Maria Petracca, Serena Ruggieri, Riccardo Nistri, Ilaria Tomasso, Elena Barbuti, Valeria Pozzilli, Shalom Haggiag, Carla Tortorella, Claudio Gasperini, Carlo Pozzilli and Luca Prosperini in Multiple Sclerosis Journal
Supplemental Material
sj-pdf-2-msj-10.1177_13524585241272046 – Supplemental material for Brain reserve and timing of clinical onset in multiple sclerosis
Supplemental material, sj-pdf-2-msj-10.1177_13524585241272046 for Brain reserve and timing of clinical onset in multiple sclerosis by Maria Petracca, Serena Ruggieri, Riccardo Nistri, Ilaria Tomasso, Elena Barbuti, Valeria Pozzilli, Shalom Haggiag, Carla Tortorella, Claudio Gasperini, Carlo Pozzilli and Luca Prosperini in Multiple Sclerosis Journal
Footnotes
Author contributions
M.P.: conception and design of the study, acquisition and analysis of data and drafting of the manuscript. S.R.: conception and design of the study, acquisition and analysis of data and drafting of the manuscript. R.N.: acquisition and analysis of data. I.T.: acquisition and analysis of data. E.B.: acquisition and analysis of data. V.P.: acquisition and analysis of data. S.H.: acquisition and analysis of data, and drafting of the manuscript. C.T.: acquisition and analysis of data, and drafting of the manuscript. C.G.: acquisition and analysis of data, and drafting of the manuscript. C.P.: acquisition and analysis of data, and drafting of the manuscript. L.P.: conception and design of the study, acquisition and analysis of data, and drafting of the manuscript and figures.
Data availability statement
Anonymized data not published within this article will be made available by request from any qualified investigator.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.