
Abstract
Background:
Infection by cytomegalovirus (HCMV) and Epstein–Barr virus (EBV) play a prognostic role in multiple sclerosis (MS).
Objectives:
To explore whether humoral immune responses to HCMV and EBV at disease onset were associated with changes in serum and cerebrospinal fluid (CSF) levels of inflammatory and neurodegeneration biomarkers.
Methods:
Ninety-eight MS patients with a median follow-up of 20 years were included in the study. The levels of a panel of nine biomarkers were measured in serum (N = 60) and CSF (N = 61) samples of patients at the time of the first demyelinating event.
Results:
Immune responses to HCMV inversely correlated with serum neurofilament light chain (sNfL) levels (rho = −0.367; p = 0.039). sNfL levels were reduced in patients with high immune responses to HCMV (p = 0.006). Elevated sNfL levels were associated with higher risk of Expanded Disability Status Scale (EDSS) 3.0 (p = 0.016), 4.0 (p = 0.009) and 6.0 (p = 0.003), and with higher risk of developing secondary progressive MS (p = 0.003) and to receive treatment (p = 0.032). Serum soluble CD21 levels were increased in patients with high immune responses to EBV nuclear antigen 1 (p = 0.020).
Conclusions:
High immune responses to HCMV are associated with limited disease progression and central nervous system (CNS) injury in MS patients. These findings reinforce the protective role of HCMV infection in MS.
Introduction
Genetic and environmental factors jointly determine the susceptibility to develop Multiple Sclerosis (MS) and microbial infections, have long been associated with MS development. Ubiquitous herpesviruses, a group of large DNA viruses that are capable of establishing latency with potential for reactivation after primary infection, are thought to modulate MS susceptibility. While infection with EBV, HHV-6 and HCMV have particularly been associated with MS, 1 current data suggest that not all of the aforementioned herpesviruses contribute equally to MS risk. 2 There is a strong evidence for a causal relationship between EBV and MS. 3 The role of HHV-6 is less well defined, some studies reported that HHV-6 can infect and activate EBV-infected B cells and suggested cumulative roles for EBV and HHV6 in MS pathogenesis.4,5 In contrast, HCMV seems to play a protective role since sero-epidemiological studies found HCMV infection to be associated with a lower risk of MS development.6,7 However, the role of EBV and HCMV infection as prognostic factors in patients with MS remains less well defined.
In a recent study conducted by our group in patients with a first demyelinating event or clinically isolated syndrome (CIS) and a median follow-up of 20 years, 8 increased humoral immune responses against the EBV viral capsid antigen (VCA) were associated with shorter time to treatment with first-line and second-line therapies during follow-up. In addition, increased humoral immune responses against the EBV-encoded nuclear antigen-1 (EBNA1) correlated with an increased relapse rate during follow-up. In contrast, elevated humoral immune responses against HCMV were protective on long-term disability outcomes such as the time to reach an EDSS of 4.0 and the time to develop a secondary progressive phase of MS (SPMS), and were also associated with shorter time to first-line therapies. 8
Serum and CSF levels of several neuroglial and immune proteins reflecting neuroaxonal damage such as the soluble neurofilament light chain (NfL), microglial and astroglial activation such as chitinase-3-like 1 (CHI3L1/YKL-40) and soluble triggering receptor expressed on myeloid cells 2 (TREM2), immune cell activation, survival and CNS-recruitment such as IL-6, IL-15 and CXCL13, and complement system-associated proteins such as activated complement protein C3a and the soluble complement receptor 2 (CD21), show potential to be sensitive biomarkers of pathologic processes associated with disability accrual in MS and other CNS diseases.
In this study, we aimed to better understand the mechanisms by which the humoral immune responses against EBV and HCMV are associated with long-term prognostic outcomes in MS patients. To achieve this objective, we measured the serum and cerebrospinal fluid (CSF) levels of a panel of inflammatory and neurodegeneration biomarkers previously reported to be associated with MS activity, severity or progression.9,10
Methods
Patients
A total of 98 patients belonging to the initial cohort of CIS patients recruited at the Cemcat (Barcelona) and who participated in the previous studies performed by the group8,11 were included based on the availability of serum and CSF samples collected at the time of the first demyelinating event. Inclusion criteria, clinical, CSF and brain MRI assessments of the CIS patients participating in the study were previously described. 11 Briefly, the main inclusion criterion was a CIS suggestive of demyelination in the central nervous system (CNS) involving the spinal cord, optic nerve, brainstem or other topography that was not attributable to other diseases. Patients having other alternative diagnoses beyond MS confirmed during follow-up were excluded from the study. The serum cohort included 60 patients and the CSF cohort 61 patients. These cohorts were partially overlapped, and only 23 (23.5%) patients had both serum and CSF samples. The study was approved by Comité Ético de Investigación Clínica des Hospital Universitari Vall d’Hebron (EPA(AG)57/2013(3834)). Participants gave informed consent to participate in the study before taking part.
Viral serologies
Humoral immune responses against the EBV antigens EBNA1 and VCA, and against HCMV were measured by ELISA at disease onset as described in the previous study. 11
Quantification of serum and CSF levels of biomarkers
The levels of the following biomarkers were measured in serum and CSF samples from patients included in the study using the ELLA multiplex immunoassay platform: complement component C3a, soluble CD21, CHI3L1, TREM2, IL-6 and 15, NfL, glial fibrillary acidic protein (GFAP), and CXCL13. Samples were sent to the University Hospital of Münster (Münster, Germany) on dry ice. For quantification, samples were thawed at 37°C (water bath), immediately transferred to ice and processed as recommended by the manufacturer (Bio-Techne, Minneapolis, MN, USA).
All biomarkers were measured in both serum and CSF samples except for GFAP (only in CSF) and CXCL13 (only in serum).
Statistical analysis
Multivariable linear regression models were built to assess the association between serum and CSF levels of biomarkers and baseline variables such as age, sex and the number of T2 lesions in brain MRI. Associations between viral IgG responses and serum and CSF biomarkers were evaluated by partial correlation analysis adjusted by age. Patients were classified into ‘high’ and ‘low’ immune responses according to the median values of IgG responses to HCMV, EBNA1 and VCA. Comparison of serum and CSF biomarker levels between patients with high and low immune responses was performed with a Mann–Whitney U test. Univariable and multivariable Cox proportional hazard regression models adjusted for age at CIS, sex, number of T2 lesions in baseline brain MRI, and treatment during follow-up were used to evaluate the association of serum NfL levels and viral IgG responses to HCMV with the time to EDSS 3.0, EDSS 4.0, EDSS 6.0, SPMS, and low-/medium-efficacy and high-efficacy therapies. The association of serum soluble CD21 levels and viral IgG responses to EBNA1 with the number of relapses was analysed using univariable and multivariable Poisson regression models adjusted for follow-up time, age, sex, number of T2 lesions and treatment; results were expressed as rate ratio and 95% CI. Potential interactions between factors were also evaluated.
Results
Patients and antiviral immune responses
Demographic, clinical and radiological information of patients at disease onset is summarized in Table 1. In the serum cohort, mean (standard deviation; SD) age of patients was 29.9 (7.1) years, 46 (76.7%) were women and 38 (63.3%) were positive for oligoclonal bands. Forty-seven percent of patients had nine or more T2 lesions in baseline MRI, 25% between one and eight T2 lesions, and 23% had no T2 lesions. Thirty-two percent of patients had contrast-enhancing lesions. Median (interquartile range) time between disease onset and blood collection was 2.4 (0.9–7.7) months. Mean age of the CSF cohort was 31.2 (7.5) years, 45 (73.8%) were women and 39 (66.1%) were positive for oligoclonal bands. Regarding T2 lesions, 33% of patients had nine or more T2 lesions, 32% between one and eight T2 lesions, and 20% had no T2 lesions. Thirty-three percent of patients had contrast-enhancing lesions. Time between disease onset and CSF collection was 1.5 (0.5–4.7) months.
Demographic, clinical and radiological characteristics of patients included in the study.
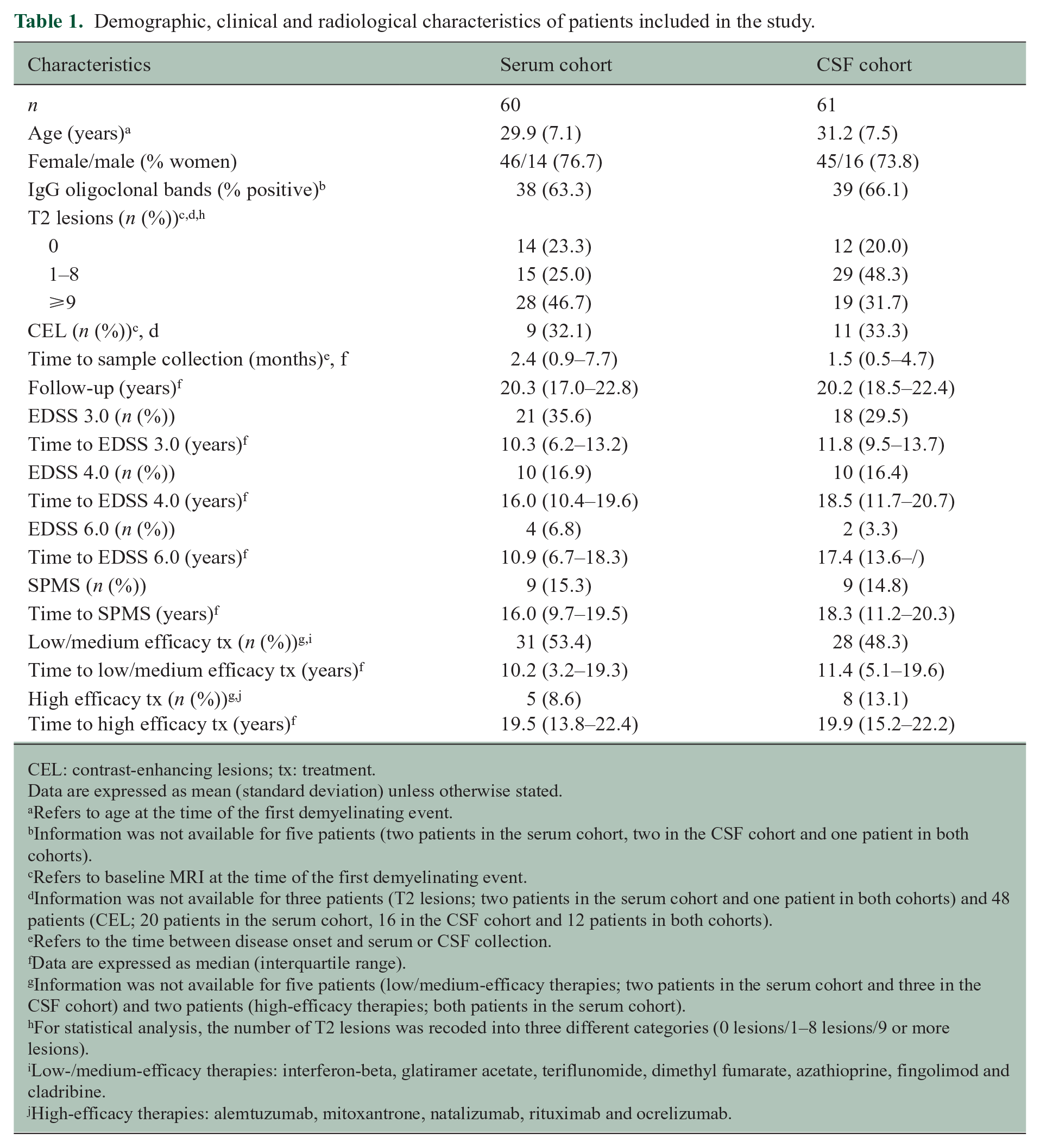
CEL: contrast-enhancing lesions; tx: treatment.
Data are expressed as mean (standard deviation) unless otherwise stated.
Refers to age at the time of the first demyelinating event.
Information was not available for five patients (two patients in the serum cohort, two in the CSF cohort and one patient in both cohorts).
Refers to baseline MRI at the time of the first demyelinating event.
Information was not available for three patients (T2 lesions; two patients in the serum cohort and one patient in both cohorts) and 48 patients (CEL; 20 patients in the serum cohort, 16 in the CSF cohort and 12 patients in both cohorts).
Refers to the time between disease onset and serum or CSF collection.
Data are expressed as median (interquartile range).
Information was not available for five patients (low/medium-efficacy therapies; two patients in the serum cohort and three in the CSF cohort) and two patients (high-efficacy therapies; both patients in the serum cohort).
For statistical analysis, the number of T2 lesions was recoded into three different categories (0 lesions/1–8 lesions/9 or more lesions).
Low-/medium-efficacy therapies: interferon-beta, glatiramer acetate, teriflunomide, dimethyl fumarate, azathioprine, fingolimod and cladribine.
High-efficacy therapies: alemtuzumab, mitoxantrone, natalizumab, rituximab and ocrelizumab.
As shown in Supplementary Table 1, mean/median (range) IgG titers to HCMV were 40.7/40.0 (5–87), to EBV-EBNA1 3.0/3.2 (0.8–3.3) and to EBV-VCA 3.5/3.7 (0.2–5.5). Thirty-seven percent of patients were seronegative for HCMV.
Association between humoral immune responses against EBV and HCMV and serum biomarker levels at disease onset
Supplementary Table 2 shows the results of the multivariable analysis at baseline of serum biomarkers. TREM2 was associated with age, CHI3L1 with sex, and soluble CD21 and IL-6 with the number of T2 lesions. IL-15 was associated with sex and the number of T2 lesions. Viral IgG responses to HCMV significantly correlated with IL-6 serum levels (0.406; p = 0.019) and inversely correlated with serum NfL levels (−0.367; p = 0.039) (Table 2). In contrast, none of the serum biomarker levels significantly correlated with IgG responses to EBV EBNA 1 and VCA antigens (Table 2).
Correlations between blood and CSF biomarkers and humoral immune responses against HCMV and EBV.
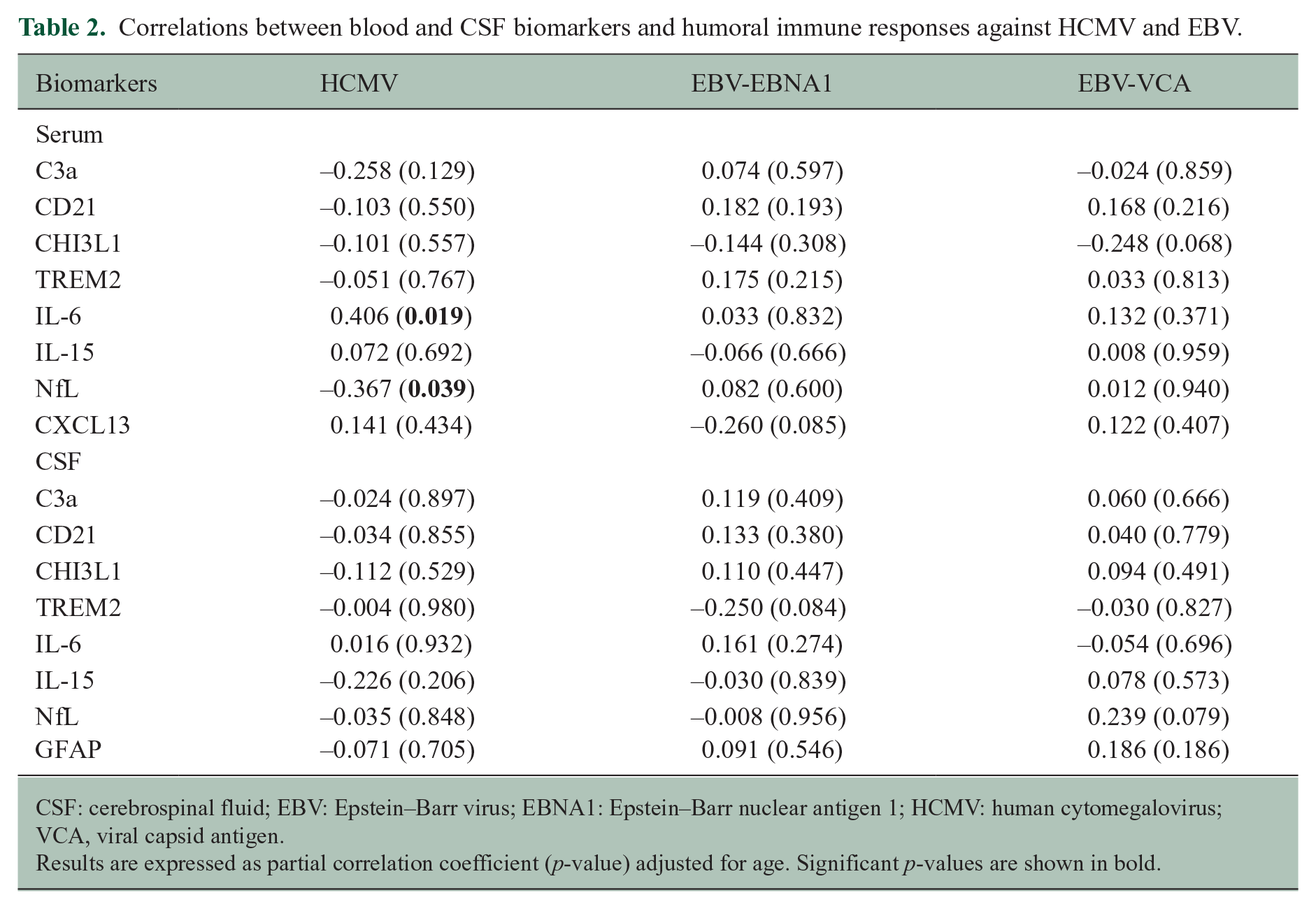
CSF: cerebrospinal fluid; EBV: Epstein–Barr virus; EBNA1: Epstein–Barr nuclear antigen 1; HCMV: human cytomegalovirus; VCA, viral capsid antigen.
Results are expressed as partial correlation coefficient (p-value) adjusted for age. Significant p-values are shown in bold.
Supplementary Table 3 shows the baseline demographic, clinical and radiological characteristics of patients classified according to high and low immune responses to HCMV and EBV-EBNA1 and -VCA. As shown in Figure 1, serum NfL levels were significantly lower in the group of patients with high humoral immune responses to HCMV compared to patients with low humoral immune responses (p = 0.006; p = 0.042 after adjustment for age and number of T2 lesions in multivariable linear regression analysis). Interestingly, a similar distribution of serum NfL levels was observed between seronegative and seropositive patients for HCMV being higher in seronegative patients, although differences did not reach statistical significance (p = 0.121; Supplementary Figure 1).
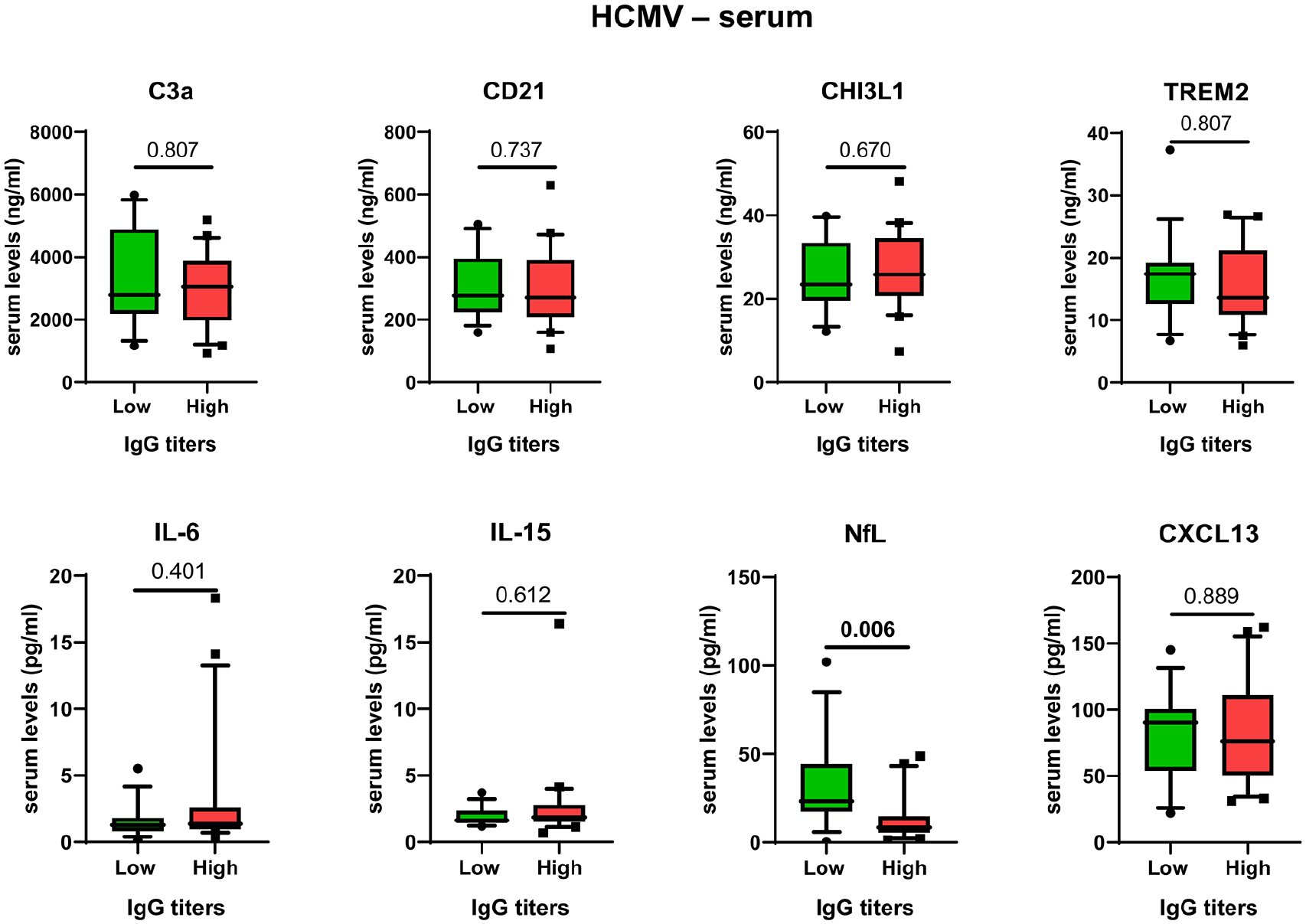
Boxplots showing serum biomarker levels in patients classified according to the median values of IgG immune responses to HCMV.
Comparisons of serum biomarker levels between patients with high and low humoral immune responses to EBV revealed significantly higher serum levels of soluble CD21 in patients with high humoral immune responses to EBV-EBNA1 compared to patients with low immune responses (p = 0.020; p = 0.192 after adjustment for age and number of T2 lesions in multivariable linear regression analysis) (Figure 2). Also, a trend towards higher serum IL-15 levels was observed in patients with low immune responses to EBNA1 compared to patients with high immune responses (p = 0.050; p = 0.639 after adjustment for age, sex and number of T2 lesions) (Figure 2).
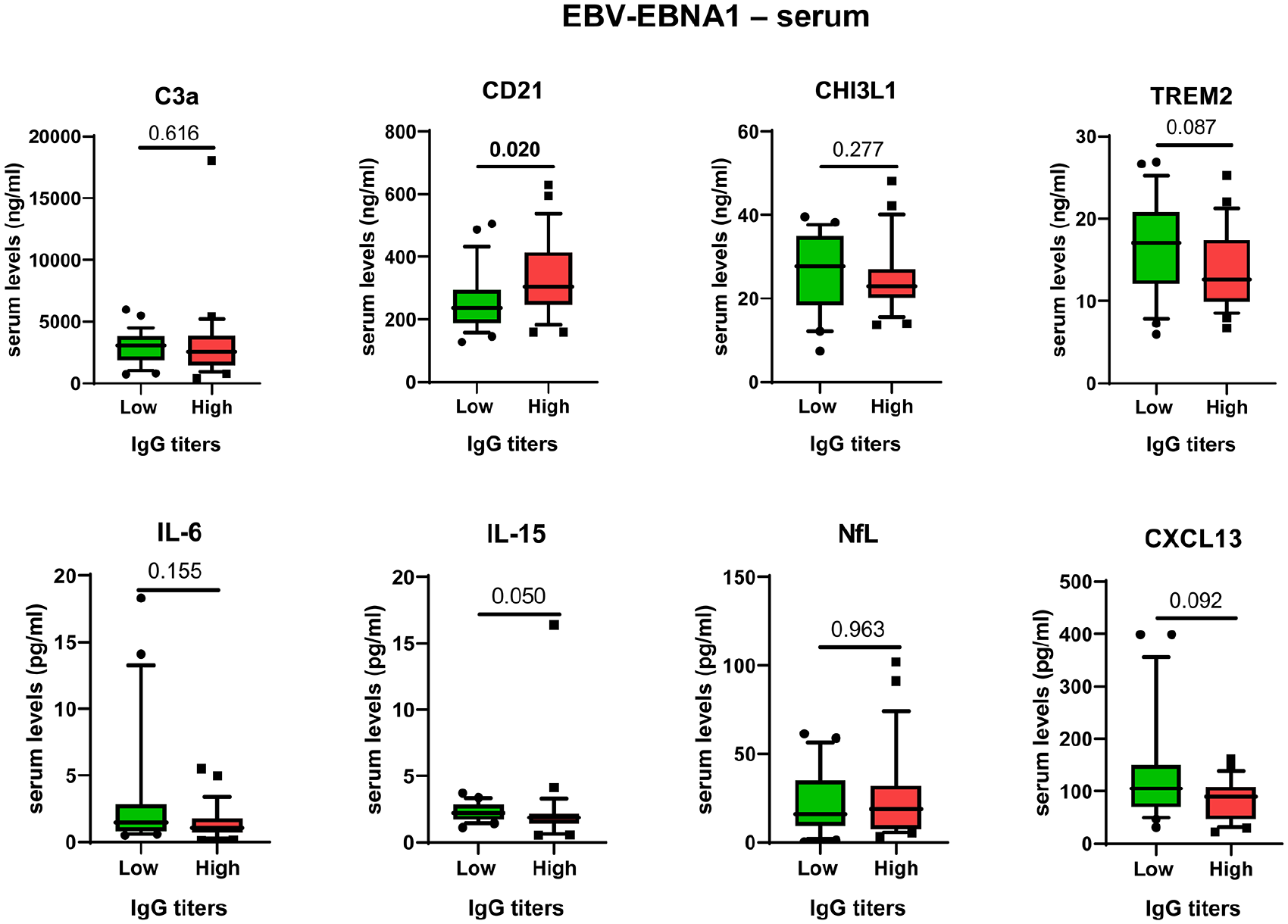
Boxplots showing serum biomarker levels in patients classified according to the median values of IgG immune responses to EBNA1.
Serum biomarker levels were comparable between patients with high and low IgG responses to EBV-VCA (Supplementary Figure 2).
Association between humoral immune responses against EBV and HCMV and CSF biomarker levels at disease onset
As shown in Supplementary Table 2, CHI3L1 and TREM2 were associated with age, and NfL with sex. GFAP was associated with age, sex and the number of T2 lesions. None of the CSF biomarker levels significantly correlated with IgG responses to HCMV or EBV antigens (Table 2). Similarly, no significant differences were observed in CSF biomarker levels between patients with high and low immune responses to HCMV and EBV antigens (Supplementary Table 4).
Effects of serum biomarker levels and humoral immune responses to HCMV and EBNA1 on the different outcomes
Based on the findings of significant differences in the levels of serum NfL and soluble CD21 levels between patients with high and low IgG immune responses to HCMV and EBNA1 respectively, we investigated the effect of these two biomarkers on different study outcomes and explored their potential interaction with the antiviral humoral immune responses. As shown in Table 3, elevated serum NfL levels at disease onset were associated with increased risk for the time to EDSS 3.0 (HR 1.017; 95% CI 1.003–1.031; p = 0.016), EDSS 4.0 (HR 1.024; 95% CI 1.006–1.043; p = 0.009), EDSS 6.0 (HR 1.047; 95% CI 1.015–1.079; p = 0.003), SPMS (HR 1.028; 95% CI 1.009–1.048; p = 0.003) and low/medium-efficacy therapies (HR 1.014; 95% CI 1.001–1.031; p = 0.032). These associations remained significant in multivariable analysis for the outcomes time to EDSS 4.0, EDSS 6.0 and SPMS (Table 3). As expected from the previous study, 8 in univariable analysis, elevated immune responses against HCMV were associated with a lower risk to time to EDSS 4.0, SPMS and low/medium-efficacy therapies (Table 3). Interaction analysis resulted in a loss of the significant effects that serum NfL levels and immune responses against HCMV had individually on the different outcomes (Table 3).
Effects of sNfL and sCD21 levels, IgG titers to HCMV and EBNA1, and their interactions.
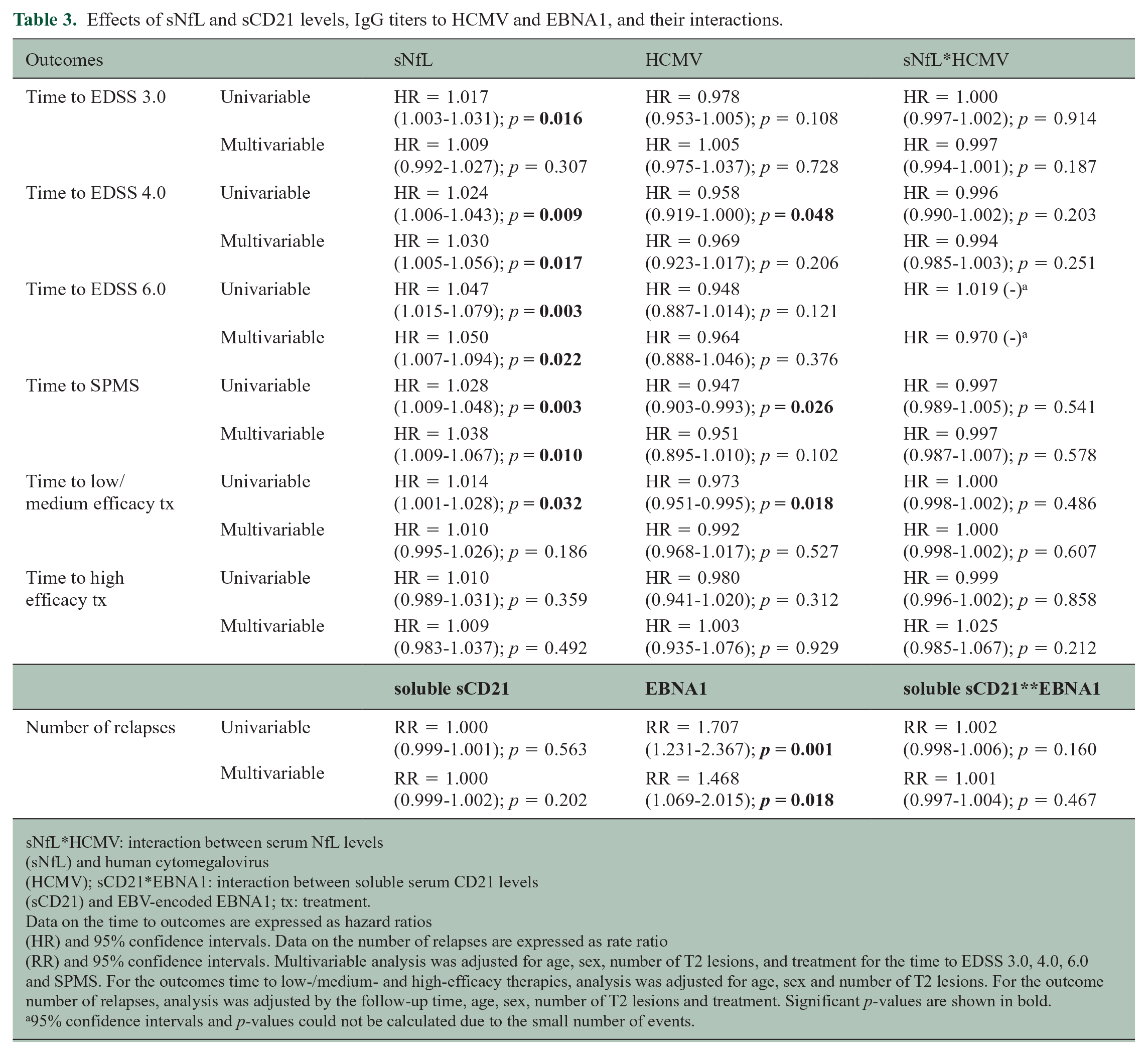
sNfL*HCMV: interaction between serum NfL levels (sNfL) and human cytomegalovirus (HCMV); sCD21*EBNA1: interaction between soluble serum CD21 levels (sCD21) and EBV-encoded EBNA1; tx: treatment.
Data on the time to outcomes are expressed as hazard ratios (HR) and 95% confidence intervals. Data on the number of relapses are expressed as rate ratio (RR) and 95% confidence intervals. Multivariable analysis was adjusted for age, sex, number of T2 lesions, and treatment for the time to EDSS 3.0, 4.0, 6.0 and SPMS. For the outcomes time to low-/medium- and high-efficacy therapies, analysis was adjusted for age, sex and number of T2 lesions. For the outcome number of relapses, analysis was adjusted by the follow-up time, age, sex, number of T2 lesions and treatment. Significant p-values are shown in bold.
95% confidence intervals and p-values could not be calculated due to the small number of events.
Finally, serum soluble CD21 levels at disease onset had no effect on the relapse rate of patients during follow-up (Table 3). As expected from the previous study, 8 EBNA1-specific IgG levels were associated with an increased relapse rate in both univariable and multivariable analyses; however, as shown in Table 3, serum soluble CD21 levels and humoral immune responses to EBNA1 did not interact with each other.
Discussion
In a previous study, 8 elevated humoral immune responses to EBV antigens such as EBNA1 and VCA measured in MS patients at disease onset were found to influence long-term prognosis based on their associations with inflammation-related outcomes like the time to treatment with first-line and second-line therapies and the relapse rate. In contrast, high immune responses to HCMV at disease onset were found to be protective on disability-related outcomes like the time to reach an EDSS of 4.0 and the time to develop SPMS. Here, we explored whether the abovementioned relationship between antiviral immune responses and prognostic disease outcomes was associated with changes in the blood and CSF levels of a panel of biomarkers measured by a multiplex immunoassay platform.
In the correlation analysis between biomarker levels and humoral immune responses, elevated IgG immune responses to HCMV were associated with high serum levels of the proinflammatory cytokine IL-6. Although IL-6 is known to play a role in the immunopathogenesis of MS, 12 the association found in this study between antiviral immune responses to HCMV and IL-6 serum levels is intriguing and most likely related to the potential described for HMCV to induce IL-6 expression both at the mRNA and protein levels in peripheral blood cells from healthy controls. 13 Interestingly, an inverse relationship was observed between IgG immune responses to HCMV and serum NfL levels. Furthermore, serum NfL levels at disease onset in patients having high immune responses to HCMV were significantly decreased compared to patients with low anti-HCMV immune responses. Several studies have shown that blood and CSF NfL levels play an important prognostic role on a number of inflammation and disability outcomes in patients with MS, particularly those with relapse-onset disease.14–16 Considering that NfL are a highly specific biomarker of CNS injury, the findings of lower serum NfL levels in patients with high humoral immune responses to HCMV support the protective role that HCMV infection seems to play on disease prognosis of MS patients. Of note, high serum NfL levels at disease onset were associated with worse prognosis on all long-term disability outcomes analysed in the study such as the time to reach an EDSS of 3.0, 4.0 and 6.0, and also on the time to low-/medium-efficacy therapies. Similar findings of elevated blood NfL levels and worse disability outcomes have been previously reported in relapse-onset MS patients.17–19 As observed in our initial study, 11 high immune responses to HCMV were associated with lower risk to reach an EDSS of 4.0, to develop SPMS and to be treated with low-/medium-efficacy therapies. However, interactions between anti-HCMV humoral immune responses and serum NfL levels did not improve the effect that each of the factors had individually on the different outcomes, probably owing to the fact that both variables are highly correlated.
Comparisons of serum and CSF biomarker levels between patients with high and low humoral immune responses to EBV antigens only revealed significant results for serum soluble CD21. Human CD21 is a membrane glycoprotein that serves as complement receptor (complement receptor type 2 – CR2) of the complement C3-derived fragments iC3b, C3dg and C3d. 20 CD21 is expressed on B cells and binds to the EBV gp350 surface glycoprotein thus mediating the entrance of the virus into these cells. 21 A soluble form of CD21 exists following shedding of the extracellular part of the protein which is fully functional and has the potential to bind to all of its known ligands. 22 Previous studies have reported significantly lower soluble serum CD21 levels in MS patients compared to healthy controls and patients with other neurological disorders.23,24
EBNA1 has been found to be consistently expressed in proliferating EBV-infected memory B cells, which suggests that high immune responses to EBNA1 are possibly associated with higher B cell activation and proliferation. Although not proven in this study, the finding of higher serum soluble CD21 levels in patients with elevated immune responses against EBNA1 suggests increased B cell activation in these patients.
There is growing evidence that ineffective immune control of Epstein–Barr-virus infection in MS contributes to the formation of elevated EBNA1-specific Ab titers.25,26 Some of these EBNA1-specifc Abs might contribute to the evolution of MS through cross-recognition of glial proteins such as the CNS protein glial cell adhesion molecule (GlialCAM).25,27 B cell activation leads to shedding of CR2 (CD21) 22 and its association with high EBNA1Ab titers is also in line with a less effective control and resulting in higher activation of EBV latency in B cells. However, our data should be taken with caution since serum soluble CD21 levels seem to be largely influenced by the baseline MRI findings like the number of brain T2 lesions. In our study, we investigated whether serum soluble CD21 levels at disease onset influenced the number of relapses during follow-up of patients. We observed that elevated IgG immune responses to EBNA1 significantly increased the relapse rate in patients, a finding already reported in our previous study. 8 However, serum soluble CD21 levels by themselves or via interaction with humoral immune responses against EBNA1 did not have any effect on this inflammation-related outcome. It would have been interesting to explore whether these findings differed between patients positive and negative for the HLA-DRB1*15:01 allele; however, the lack of HLA-DRB1 genotyping is a limitation of the study.
Both EBV and HCMV infect and persist in hematopoietic cells which reside in lymphoid organs. Notably, IgG immune responses to HCMV and EBV antigens had no effect on the CSF levels of the biomarkers investigated in this study, suggesting that antiviral immune responses are being predominantly developed in lymphoid compartments with little involvement of the CNS and that mechanisms underlying the associations with clinical and paraclinical disease severity and progression are confined to or at least initiated in the periphery, that is, outside of the CNS and CSF compartments.
In conclusion, the finding of lower serum NfL levels in patients with high immune responses to HCMV reinforce the protective role of HCMV infection in long-term MS disease prognosis, and probably reflects a lower inflammatory environment in these patients. The finding of higher serum soluble CD21 levels in patients with high immune responses to EBNA1 is probably associated with increased CD21 shedding and may suggest a higher activation status of B cells in these patients.
Supplemental Material
sj-docx-1-msj-10.1177_13524585241274571 – Supplemental material for Cytomegalovirus immune responses are associated with lower serum NfL and disability accumulation risk at multiple sclerosis onset
Supplemental material, sj-docx-1-msj-10.1177_13524585241274571 for Cytomegalovirus immune responses are associated with lower serum NfL and disability accumulation risk at multiple sclerosis onset by Jan D Lünemann, Augusto Sao Avilés, Mar Tintoré, Luciana Midaglia, Nicolás Fissolo, Lucía Gutiérrez, Heinz Wiendl, Xavier Montalban and Manuel Comabella in Multiple Sclerosis Journal
Footnotes
Data Availability Statement
Anonymized data not published within this article will be made available by request from any qualified investigator.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was funded by grants of the Deutsche Forschungsgemeinschaft (DFG) (grant numbers LU 900/3-1, LU 900/4-1 and SFB-TR128/Teilprojekt A11) and a grant by the European Commission (BEHIND-MS, 101137235).
Ethical Approval
This study involves human participants and was approved by Comité Ético de Investigación Clínica des Hospital Universitari Vall d’Hebron (EPA(AG)57/2013(3834)). Participants gave informed consent to participate in the study before taking part.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.