
Abstract
Objectives:
The objectives were to understand the employment impacts of myelin oligodendrocyte glycoprotein–associated antibody disease (MOGAD) on adults in an international cohort by determining lost employment, work hours, and wages.
Background:
Clinically, MOGAD can be associated with significant disability; however, its socioeconomic consequences for adults are barely reported.
Methods:
Participants of potential working age (18–70 years old) with neurologist-diagnosed MOGAD were recruited from clinical sites in 13 countries, April 2022 to August 2023. Each participant completed a one-time survey. Regression models assessed associations with post-MOGAD (1) unemployment and (2) work hours.
Results:
A total of 117 participants (66.7% female), mean age 39.7 years, median disease duration 3 years (25th, 75th percentile: 1, 7) were analyzed. Employment post-MOGAD reduced from 74 (63.2%) to 57 (48.7%) participants. Participants employed pre-diagnosis reduced their work hours, on average, from 31.6 hours/week to 19.5 hours/week post-diagnosis. Residence in a high-income country was statistically significantly associated with post-diagnosis employment and higher weekly work hours. Depressed mood was associated with unemployment. MOGAD-related pain and history of myelitis were independently associated with lost work hours.
Conclusion:
MOGAD can have significant impacts on adult employment, particularly in non–high-income countries. Depressed mood and pain are potentially modifiable factors related to socioeconomic status in MOGAD.
Keywords
Introduction
The impact of myelin oligodendrocyte glycoprotein–associated antibody disease (MOGAD) on adult livelihoods is not well known, especially internationally. Clinically, MOGAD can be associated with significant disability through its attacks on the optic nerve, spinal cord, and/or brain, leading to blindness, spinal cord dysfunction, and possibly cognitive changes, alongside the need for recurring medical visits.1–6 Because MOGAD often first presents in adolescence and young adulthood, there is a risk of disrupting a person’s ability to work and gain a meaningful income over the lifespan; however, the socioeconomic consequences of MOGAD, particularly in adults, are not reported. Because the identification of MOGAD as a distinct disorder is relatively recent, outcomes of MOGAD in adults are timely to report, given the growing number of adults now recognized to live with MOGAD internationally.
In this international, observational, convenience-sampled cohort study, we surveyed adults in countries of multiple country income levels and geographic regions for the socioeconomic impact of MOGAD. 7 We provide an analysis of patient-perceived impact of MOGAD on employment, collectively from multiple countries, in relation to employment, work hours, and wages. We ask the following main questions: (1) What is the prevalence of un- and under-employment in MOGAD? and (2) What are the demographic, clinical, and country income-level associations of lost employment and work hours in MOGAD? We further report the self-perceived impact of MOGAD on personal wages post-diagnosis.
Materials and methods
Ethics approvals
The Massachusetts General Brigham Institutional Review Board reviewed and approved the study protocol. Each participating country also had local ethics board reviews and approvals, as needed, to collect de-identified survey-based data. Completion of the survey by an adult with MOGAD implied their consent to participate in the study in most settings.
Survey design
A survey was designed to characterize (1) present demographic variables, (2) clinical history, (3) current symptoms related to MOGAD including pain, mood, and fatigue, (4) treatment, (5) comorbidities, (6) pre- and post-diagnosis employment, (7) pre- and post-diagnosis work hours, and (8) pre- and post-diagnosis income.
The survey was initially drafted in English, based on focus group discussions in US patients with NMOSD and MOGAD. 7 The US patients have been previously reported within a larger cohort focused on NMOSD patients. 8 The English survey was then translated by local neurologists and research staff into multiple languages (Hindi, Mandarin, Malay, Brazilian Portuguese, Spanish, Indonesian, and Thai) for global recruitment of MOGAD patients.
Data collection
Patients with MOGAD were recruited through neurologists in each country and were either interviewed in person at a neurologist’s clinic, contacted by telephone and given an online survey link by study staff. Adults of broad potential working age, 18 to 70 years old at the time of enrollment, were eligible for inclusion. Answers were recorded in RedCap™ and responses were required on each page to continue the survey to avoid overlooked or missing responses. Participants who needed assistance to complete the study, for example, due to visual impairment, were offered that option. Each survey took approximately 30 minutes for a participant to complete. Responses were anonymous, and each participant was surveyed once.
Data collection occurred between April 2022 and August 2023. Invitations for participation were extended to multiple countries and the consortium had 23 participating countries to gather data on NMOSD.
Definitions
Employment was defined as participants who reported being employed full time (at least 40 hours/week) and included participants who identified as self-employed. Students, part-time employees, homemakers, and other designations were categorized as not employed.
The economic vantage point for reporting employment, work hours, wages, and caregiving was the participant’s with MOGAD. Currency was specified by the participant. International dollars, a hypothetical currency that is tied to the US dollar at a particular point in time for exchange (in this case 1 January 2022), were used to standardize across all currencies.
There were 23 countries in the consortium of all income levels invited. The 13 countries who recruited MOGAD participants were categorized as high- (Australia, Italy, Singapore, the United Kingdom, the United States), upper middle- (Argentina, Brazil, China, Colombia, Dominican Republic, Malaysia, Turkey), or lower middle- (India) income, based on the World Bank’s categorization of countries’ income level, assessing gross national income per capita, using the year of study commencement, 2022.
Data analysis
Survey data were reviewed by the authors (A.S.H., I.G.H., and F.J.M.) for quality control. Responses wwere clarified when needed at each site. Missing responses were considered missing completely at random when forced responses were not required on a question. No data imputation occurred. In countries with <5 participants with MOGAD (Argentina, Brazil, Colombia, the Dominican Republic, Italy, Malaysia, Turkey, and the United Kingdom), reporting was done in the context of country-level income but not individually by country which occurred for eight countries.
Certain clinical variables were conditioned for analysis and binarized given the cohort’s sample size. Pain level, which was reported on a 11-point scale from 0 to 10 (worst possible pain), was binarized as more/less pain for people rating pain intensity as a 5 or above or not. The survey also assessed how often depressed mood impeded a participant’s ability to complete job-related duties over the prior week on a 4-point scale, with 0 indicating not at all, 1 for several days, 2 for more than half the days, and 3 for nearly every day. Participants indicating a 2 or 3 on this scale were placed into one bin, compared to those answering 0 or 1. A similar methodology was utilized to binarize fatigue frequency, with those answering often or almost always for fatigue impact being placed in one category. For results written in by participants, such as one’s current job, categorization was done by the authors.
Descriptive statistics, including means, medians, ranges, and percentages, were used to depict the group’s characteristics. The prevalence of particular outcome variables of interest (e.g. employment) are reported pre- and post-MOGAD diagnosis and by gender and by country income category. The distribution of work hours was graphed. A test of two proportions was used to compare pre- and post-MOGAD diagnosis (1) employment and (2) work hours.
After removing current students from the analysis, generalized linear models were constructed for two major outcome variables of interest: employment and reduced or lost work hours (Table 3). Participants who were unemployed pre-MOGAD diagnosis were removed from the work hours’ analysis. In both regression models, the same demographic and clinical explanatory variables were selected a priori: participant age at study enrollment, gender, years of formal education, country income-level stratum, presence of myelitis or not, unilateral or bilateral visual loss or not, fatigue, depressed mood, pain, and disease duration of MOGAD.
Data analyses were conducted using R (version 4.3.1). A p-value < 0.05 was considered statistically significant. Reporting followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 9
Results
Demographic variables
There were 117 patients with MOGAD (66.7% female, 33.3% male) with a mean enrollment age of 39.7 years (Table 1). Patients were from 5 high-income countries (HICs), 7 upper middle-income countries (UMICs), and 1 lower middle-income countries (LMICs). Most participants (69.2%) were from three countries: China, India, and the United States. Ten countries each contributed fewer than 10 participants, particularly emerging economies. Participants had an average of 13.6 ± 3.9 (standard deviation) years of schooling. The highest level of education achieved was primary school for four participants (3.4%), secondary school for 11 (9.4%), high school for 22 (18.8%), trade school for five (4.3%), college for 55 (47.0%), and professional schools for 21 (17.9%). Seven (6.0%) were current students.
Demographic and clinical characteristics of MOGAD participants.
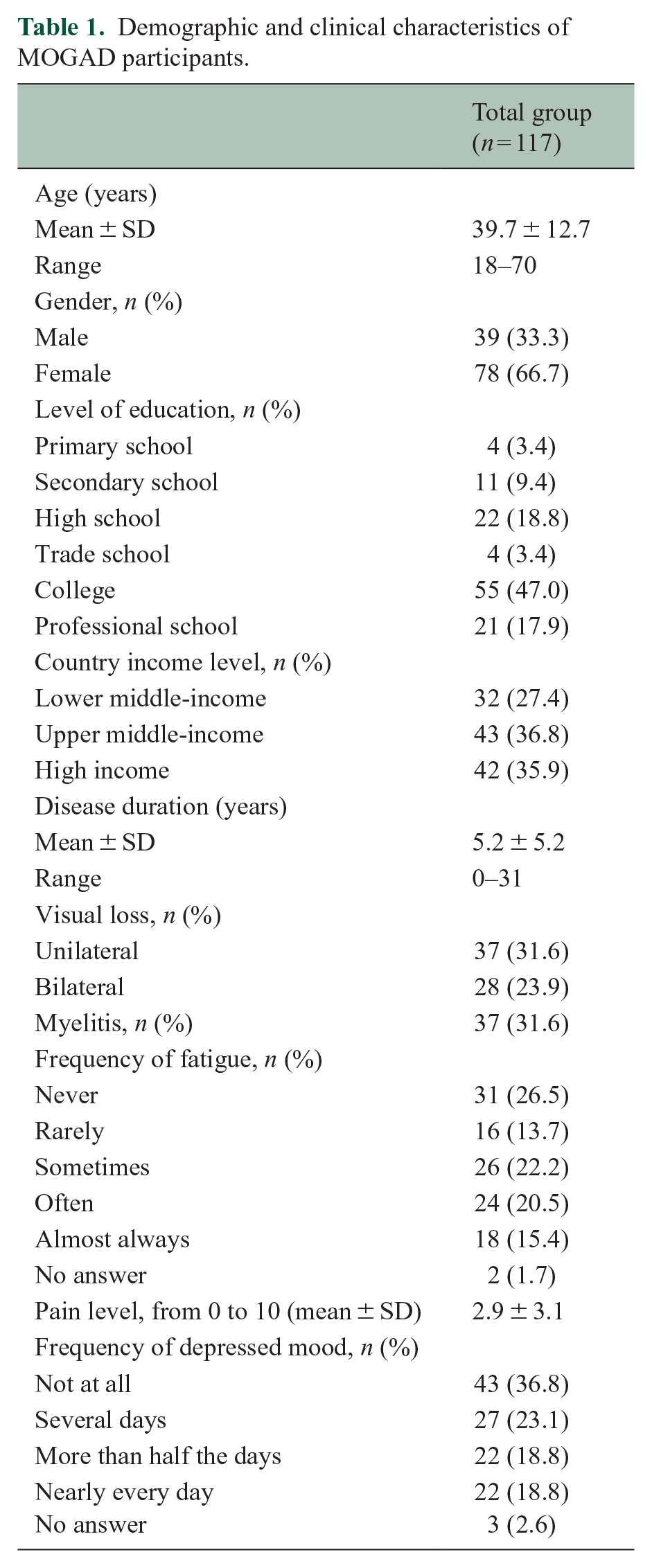
In total, 34 (29.1%) of respondents were single, 78 (66.7%) were married, and 5 (4.2%) were separated or divorced. The average household size was 3.7 ± 1.9, and the average number of income earners per household was 1.9 ± 1.2 people.
Clinical features
The mean age of first disease attack was 32.7 ± 13.0 years. Seven (6.0%) participants experienced their first attack before the age of 18 years. The mean age of MOGAD diagnosis was 34.5 ± 13.1 years and the median duration of disease was 3 years (25th, 75th percentiles: 1, 7). At the time of the survey, 50 (42.7%) participants reported no visual loss, 37 (31.6%) reported unilateral visual loss, and 28 (23.9%) reported bilateral visual loss. Thirty-seven participants (31.6%) had myelitis. Twenty-three participants (19.7%) had both visual loss and myelitis. The most recently reported attack occurred in 10 participants in the prior 90 days and 30 participants in the prior year.
In terms of self-reported comorbidities, 14 (12.0%) participants had obesity (defined as body mass index >30 kg/m2), 10 (8.5%) hypertension, 8 (6.8%) asthma, 8 (6.8%) gastrointestinal disease, and 6 (5.1%) lung disease. Forty-two (35.9%) participants reported moderate to high levels of fatigue, while 41 (35.0%) reported a pain level that was at least 6 of 11 possible points. Forty-five participants (38.5%) reported no pain at all. Forty-four participants (37.6%) stated that their depressed mood interfered with job-related duties for more than half of days or nearly every day. Most participants (n = 95, (81.2%)) were treated for MOGAD, through any combination of immunosuppressive agents, steroids, and immunoglobulins (Table 2).
Therapies used by MOGAD patients.
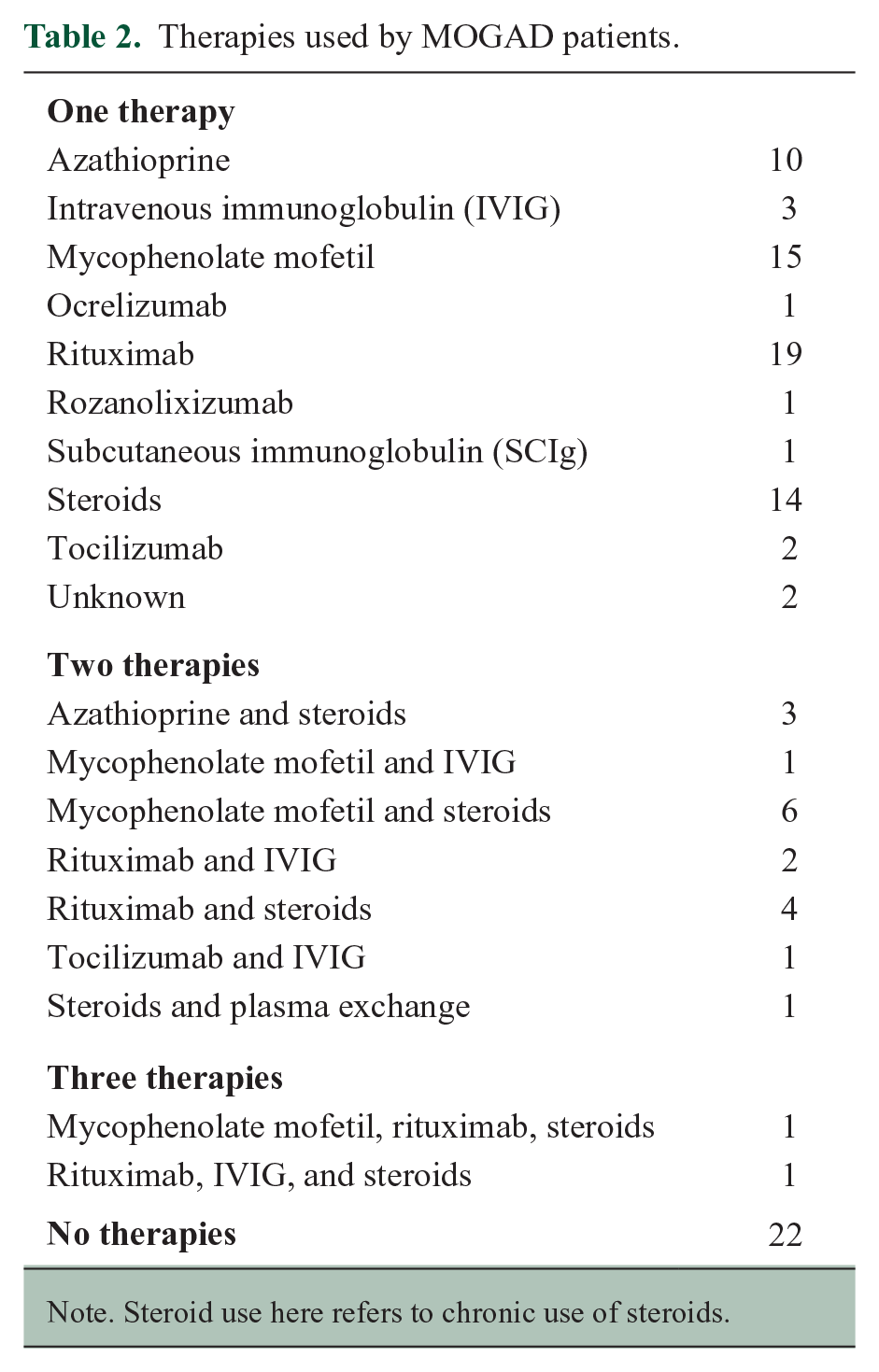
Note. Steroid use here refers to chronic use of steroids.
Employment and wages
Of 117 participants, 74 (63.2%) reported employment before their MOGAD diagnosis, while 42 (35.9%) were unemployed (Figure 1). One participant declined to answer. Post-MOGAD diagnosis, 57 patients (48.7%) were employed. Sixty participants (51.3%) were unemployed, including six students. The reduction in employment post-diagnosis, according to a test of two proportions, was statistically significant (p = 0.029).
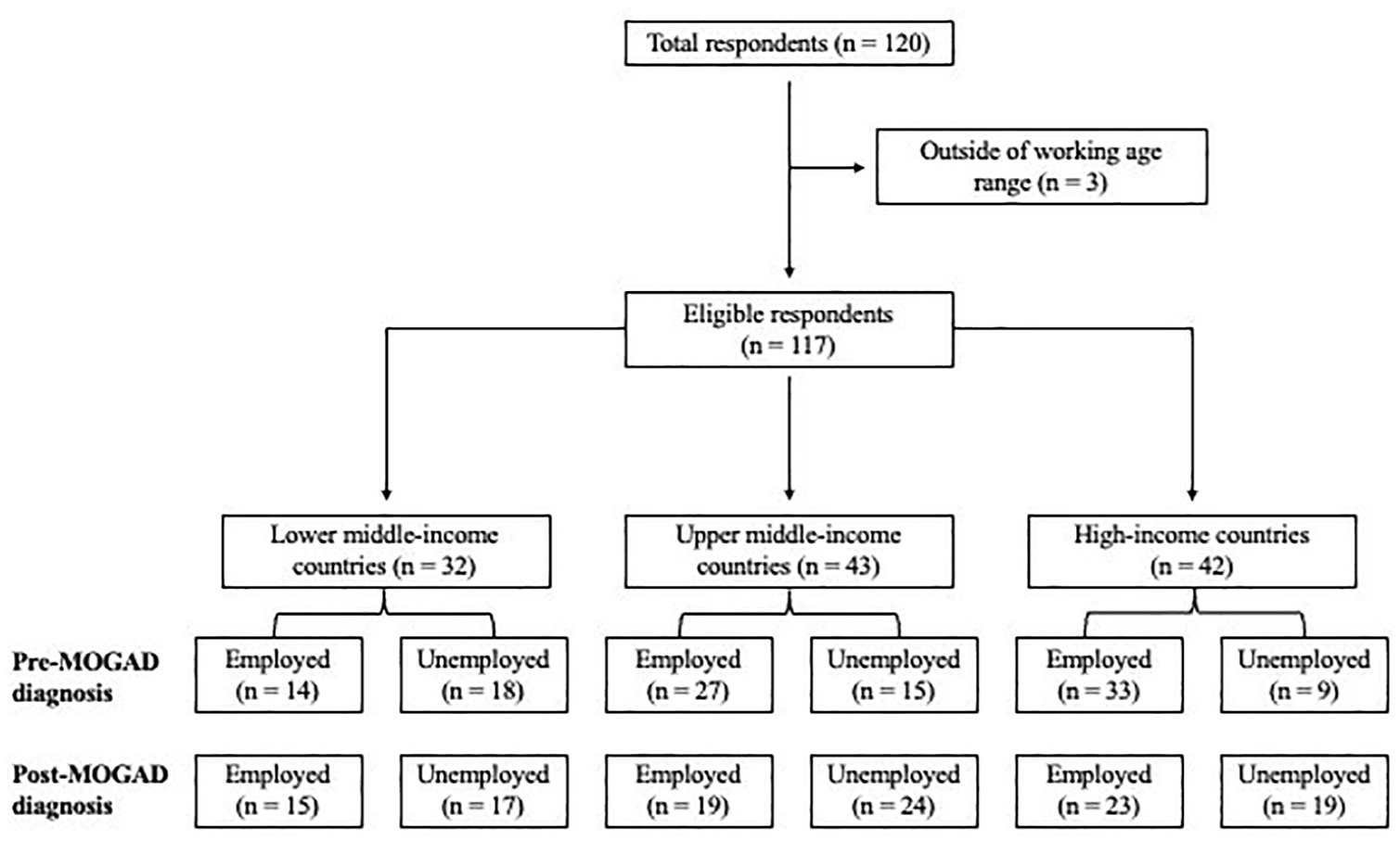
Participant selection, including proportions of participants who are employed or unemployed post-MOGAD diagnosis.
Employment was 66.7% for women and 57.9% for men pre-diagnosis and 43.6% for women and 59.0% for men post-diagnosis. Across country income levels, the proportions employed were 43.8% in LMICs, 64.3% in UMICs, and 78.6% in HICs pre-diagnosis and 46.9% in LMICs, 44.2% in UMICs, and 54.8% in HICs post-diagnosis.
On average, self-employed, part-time, and full-time-employed MOGAD participants were working a median of 40 hours/week (25th, 75th percentiles: 4, 48), before their diagnosis and 12 hours/week (25th, 75th percentiles: 0, 40) afterwards, with a reduction in work hours in addition to a lower overall employment. This reduction in work hours post-diagnosis was statistically significant (p < 0.001). In total, 43 participants (36.8%) reported having lost work directly due to their MOGAD diagnosis at one point, while 63 (53.8%) indicated that they had reduced work hours due to MOGAD. A total of 58 (49.6%) of participants disclosed their diagnosis to employers. A total of 46 participants (19 from China, 11 from the United States, and others from the Dominican Republic, India, Italy, Argentina, Colombia, Singapore, and Turkey) reported receiving health insurance from their place of work, of whom 30 reported that keeping this insurance was a factor in their decision to continue working after their diagnosis.
A total of 51 (43.6%) participants indicated that the COVID-19 pandemic had affected their work, for reasons including having to work at home, physical weakness and fatigue from getting COVID-19, lack of childcare support, and fear of transmission of the virus to them, discouraging them from working in-person. Participants rated the effect of MOGAD on their productivity while working an average score of 3.5 on a scale of 0 (no effect) to 10 (complete prevention).
In total, 50 (42.7%) participants reported losing wages after MOGAD diagnosis. The median annual income for all participants pre-diagnosis was 5335 international dollars, and 5467 international dollars post-diagnosis.
Regression analyses for associations with post-MOGAD employment and loss of work hours
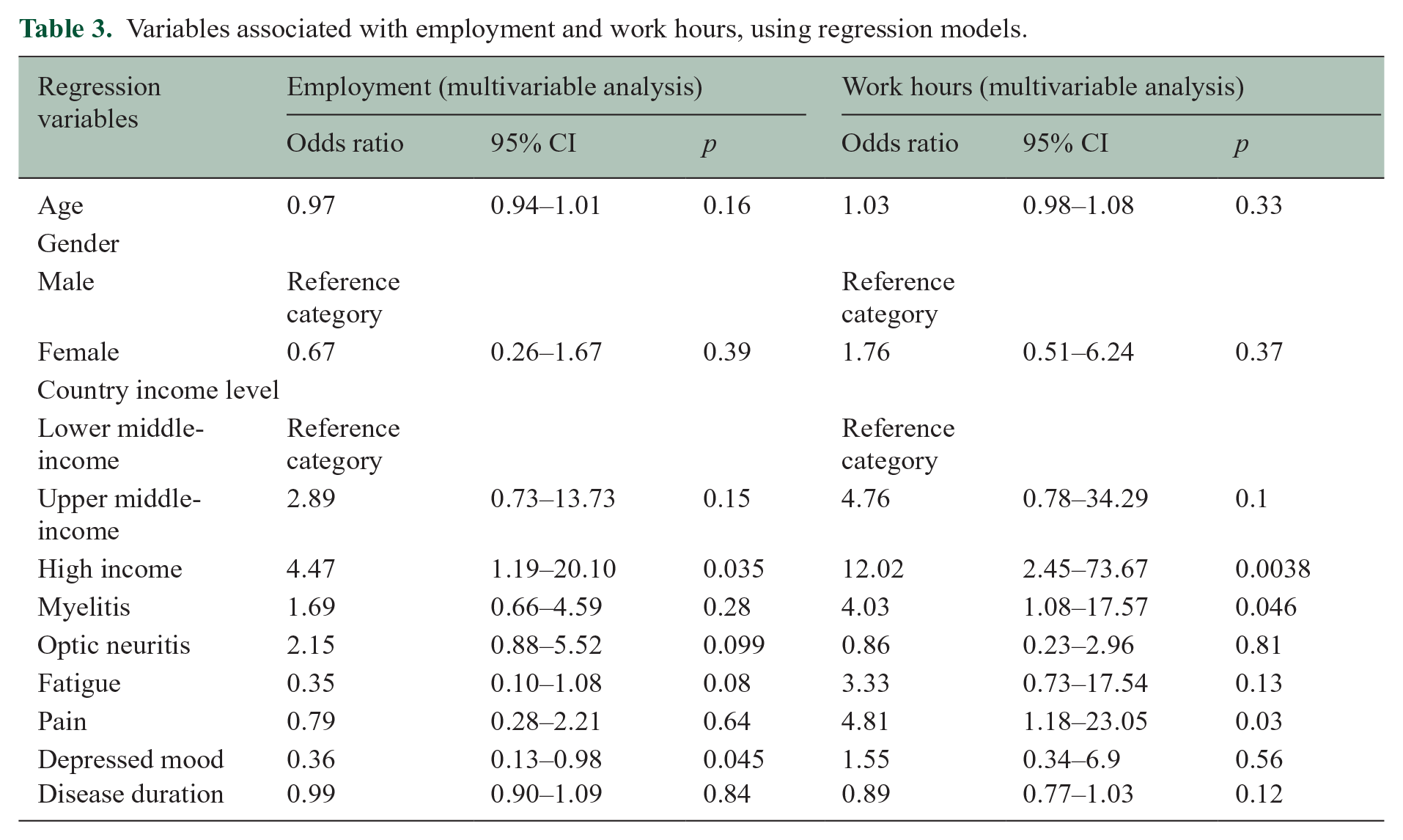
For employment as a dichotomized outcome, residence in an HIC, as opposed to lower middle-income or upper middle-income, was a positive association with employment (odds ratio (OR) = 4.47, p = 0.03), while the presence of depressed mood was a negative association (OR = 0.36, p = 0.045). Myelitis (OR = 4.03, p = 0.046), residence in a HIC (OR = 12.02, p = 0.0038), and pain (OR = 4.81, p = 0.03) were statistically significant positive associations of a participant with MOGAD having lost or reduced work hours since the MOGAD diagnosis (Table 3).
Variables associated with employment and work hours, using regression models.
Discussion
Little has been previously reported on the socioeconomic outcomes of MOGAD in adults, partly due to its relatively recent emergence as a distinct disease entity, separate from multiple sclerosis and aquaporin-4 antibody positive neuromyelitis optica. The number of adults who have diagnosed MOGAD is growing globally due to increasing clinical recognition, improved diagnostic assays, and new consensus diagnostic criteria.10,11 However, MOGAD is still overall rare. In this cohort of 117 adults, including participants from 13 countries, the average age was 40 years old with median disease duration of 3 years. The average age of participants is consistent with a peak working age in most societies. The employment prevalence went from 63% pre-MOGAD to 49% post-MOGAD diagnosis. Moreover, 37% of participants reported losing employment at one point due to MOGAD, implying participants who are working post-MOGAD have had discontinuous employment post-diagnosis. Work hours dropped to 19.5 hours/week from 31.6 hours/week on average (i.e. 60% of pre-diagnosis) among those who continued working. This reflects a subgroup of employed adults who went from close to full-time employment to part-time employment. These findings reflect statistically significant decrements in pre- versus post-MOGAD work. In many countries, retention in work was often due to a stated need to continue receiving health insurance and benefits.
MOGAD is considered to be a clinically variable disease, with the most common presentation being optic neuritis, 12 and a significant but smaller proportion having myelitis. This phenotypic spectrum was also noted in our cohort. However, optic neuritis itself did not predict unemployment or lost work hours.
Our cohort has a predominance of HIC and UMIC participants due to the lack of antibody testing access in many lower-income countries. Three additional lower-income countries were invited but identified no cases. The majority of MOGAD cases, approximately 69%, come from three of the 13 countries: China, India, and the United States. This is related to a combination of factors including access to resources for health, population size, health systems organization, and investigator time spent. Most of our participants were treated with immunosuppressive agents, with a variety of therapeutic approaches reported. Notably, employment, work hour, and wage impacts occurred in this group, who were overall treated with immunosuppression and followed longitudinally for neurological care at mostly academic medical centers.
Our study had several notable limitations. Given the complexity of the study across multiple countries, we did not capture the number of people invited to complete our survey and are unable to calculate a response rate. We cannot rule out that our sample was biased. Our sampling was by convenience. People who had a clinically monophasic disease may not have presented for longitudinal neurological follow-up to clinics and may therefore have been overlooked, underestimating the number of people who are employed. 13 By contrast, people with severe disease such as bilateral visual loss may have been less willing to participate due to barriers to participation in a lengthy survey, overestimating our employment prevalence estimate. Similarly, patients with concerns about employment may have been more motivated to participate in a survey on employment.
Importantly, there are no control participants in this study. Therefore, it is difficult to disaggregate which factors are related exclusively to MOGAD, the country setting, or to some relationship between the two. The LMIC stratum is represented fully by India, while China dominates the upper middle-income stratum and the United States dominates the high-income stratum in participant numbers. Many issues arise with international comparisons of people with the same disease, including heterogeneity in macro-economic factors, such as job availability, political stability, and country-level wealth. Cultural factors also motivate a person’s work environment, including gender roles and biases, the importance of age to employability, and stigma toward people with specific neurological impairments. Variations in public services and laws mean that impairments in some situations may become disabilities in others, making factors such as public transportation, elevators, disability services, health care coverage, and medical leaves likely influential.
An interesting finding in our analysis is that while HIC participants were more likely to be employed post-MOGAD diagnosis compared to UMIC or LMIC participants, they also experienced the highest decrement (24%) in employment loss. Similarly, UMIC participants were more likely to be employed compared to LMIC participants post-MOGAD, but had higher job loss post-diagnosis compared to LMIC.
After the global administration of the survey, we identified several modifications that could be made for future work. We did not ask specifically about the onset clinical presentation of MOGAD or the degree of recovery from the initial attack. This means we did not specifically inquire about acute disseminated encephalomyelitis (ADEM) which is a first presentation of MOGAD, occurring less commonly and predominating in young children and young adults with potential longer-term cognitive effects. 14
Responses are assumed to be accurate, and quality control was done with each site when needed. Indeed, many participants did not know their own antibody status, requiring clarification with the site’s clinical team. We did not inquire whether patients were diagnosed with the live cell-based assay, the current highest standard of testing, or if the antibody was drawn on the serum or cerebrospinal fluid. 15 If participants reported they were double seropositive, they were ultimately excluded given the very low likelihood that these cases’ autoantibodies were correctly reported. Some MOGAD cases were almost certainly excluded for data quality issues alone.
Our study also commenced before the publication of the new MOGAD diagnostic criteria. 10 Therefore, we were unable to use the criteria prospectively in our study design; the criteria would provide a higher standard of diagnostic clarity and should be used in studies moving forward. We deferred to the treating clinical neurologist for the diagnosis of MOGAD. As above, we cannot provide a breakdown of the rarer cortical and brainstem or cerebellar presentations of MOGAD as listed by the new diagnostic criteria (criterion A). Many patients wrote in their presenting features themselves, allowing us to interpret but not formally categorize every initial presentation. As our study design was a patient-facing survey, we did not ask patients about their antibody assays, titers, and magnetic resonance imaging (MRI) features (criterion B). With a wide range of countries participating, some patients may not have fulfilled criterion B as the cell-based assays for MOG antibody are not globally available. As MOGAD patients were recruited through their neurologists, they were considered to have fulfilled criterion C, that is, lacked competing alternative diagnoses.
An important consideration is the COVID-19 pandemic near the time of our survey, declared 2.3 years prior to our data collection. This could have changed the relationship of MOGAD with employment in various ways, some positively (such as the ability to work from home) and some negatively (such as the increased unemployment in some sectors). Since most MOGAD patients were immunosuppressed, the COVID-19 pandemic may serve as an extraordinary circumstance that impacted employment that is not predictive of future years. Since employment is a time-varying variable, and COVID-19 risk varies over time, longitudinal studies would likely better address this inter-relationship.
Regarding wages, we attempted to provide a common currency, standardized across countries, which is the oft-used “international dollar.” The international dollar is very similar to the USD but controls for timing of exchange. In some cases, wages increased, but the extent of wage increase is below expectation given recent inflation. Inflation varies by country but has been significant and globally recognized since the pandemic. Moreover, summary measures in wages may obscure nuanced changes in a group and do not lend insight into how or why wage changes occur, such as through job change, retraining, or demotions/promotions.
Although our study cannot identify all aspects of the environmental components of work and employment, we are able to identify individual-level, self-reported aspects of the mostly treated history of MOGAD and its reported symptoms in the context of employment. We find that there are several associations with employment retention that are relevant, particularly country income level and presence of depressed mood. Of total, 37% of participants reported that depressed mood interfered with their job-related duties. Others have found that 28.8% of people with NMOSD have a diagnosis of depression. 16 Depression is also common in MS, with an estimated prevalence of 30.5% 17 and is associated with job difficulties and reduced quality of life. 18 Factors associated with employment retention in MS and NMOSD in other studies include younger age, less fatigue, a lack mood disorders, lower pain levels, fewer comorbidities, and not using walking aids.8,18,19 In addition, the presence of pain and myelitis has measurable and statistically significant relationships with the degree of work a person with MOGAD participates in.
There are several points of potential intervention. The first is that several symptoms that associate negatively with post-MOGAD diagnosis employment and work hours are potentially modifiable. This includes the prevalent self-reporting of low mood. While this study did not explore causes of low mood, such as repetitive intravenous lines and multiple medical visits, this is a possibly addressable complaint. Similarly, attention to pain management and developing an improved pipeline of medicines for spinal cord pain could likely also improve the socioeconomic status of patients. These less emphasized symptoms appear as an unmet need in MOGAD in our study. Employment counseling, professional retraining opportunities, and provision of useful long-term prognostic information would also be valuable for adults with MOGAD, given the relatively young age of diagnosis in this adult cohort.
Together, our data provide initial assessments of the combined clinical and demographic picture of MOGAD in several countries as it relates to microeconomic outcomes, suggesting that MOGAD has a notable impact on work, with significant associations with potentially treatable symptoms such as pain and mood. These person-level factors occur alongside the more difficult to address macro-level impact of the country-level income of a person’s residence on MOGAD outcomes.
Supplemental Material
sj-docx-1-msj-10.1177_13524585241286671 – Supplemental material for Employment, work hours, and wages in adults with myelin oligodendrocyte glycoprotein antibody disease: An international cohort study
Supplemental material, sj-docx-1-msj-10.1177_13524585241286671 for Employment, work hours, and wages in adults with myelin oligodendrocyte glycoprotein antibody disease: An international cohort study by Andrew Siyoon Ham, Isabella Gomez Hjerthen, Akshatha Sudhir, Lekha Pandit, Y Muralidhar Reddy, Jagarlapudi Muralikrishna Murthy, De-Cai Tian, Hongfei Gu, Wen Gao, Simon A Broadley, Unnah Leitner, Amelia Yun Yi Aw, Kevin Tan, Tianrong Yeo, Saúl Reyes, Jaime Toro, Jairo Gaitán, Deyanira Altagracia Ramírez, Raúl Comme-Debroth, Josmarlin Patricia Medina Báez, Bade Gulec, Ugur Uygunoglu, Melih Tutuncu, Aksel Siva, Raffaele Iorio, Eleonora Sabatelli, Saif Huda, Patricia Kelly, Juan Ignacio Rojas, Edgardo Cristiano, Liliana Patrucco, Enedina Maria Lobato de Oliveira, Raquel Paiva Portugal, Paloma Peter Travassos Zaidan, Shanthi Viswanathan, Karina Koh, Su-Yin Lim and Farrah J Mateen in Multiple Sclerosis Journal
Footnotes
Acknowledgements
The authors are grateful to the American Academy of Neurology’s Neuroscience is Rewarding program for an internship scholarship to I.G.H.
Data Availability Statement
Data sharing not applicable to this article as no data sets were generated or analyzed during this study.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr F.J.M. has received research funding to her institution from Alexion, Amgen, EMD Serono, Genentech, Novartis, and TG Therapeutics and consulting fees from Alexion, EMD Serono, Genentech, and Roche. Dr T.Y. has received honoraria from ASNA, Edanz Pharma, Euroimmun AG, Merck, Novartis, Roche, Terumo BCT for consulting services and speaker’s fees, and research grants from the National Medical Research Council (NMRC Singapore), and Roche. Dr A.S. has received research grants from The Turkish Multiple Sclerosis Society; and research grants from The Scientific and Technological Research Council of Turkey & Istanbul University-Cerrahpasa Research Support Funds.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Sumaira Foundation and Horizon Therapeutics (Amgen). Both sponsors had no role in the study concept, design, analysis, or decision to submit the work for publication.
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.