
Abstract
Background:
Predicting treatment response and disease progression in multiple sclerosis (MS) is challenging. Treatment Response Scoring Systems (TRSS) are potentially useful, but their utility in patients receiving high-efficacy therapies and very high-efficacy therapies (HET/vHET) remains unclear.
Objective:
This study aimed to evaluate the performance of TRSS in patients treated with HET/vHET.
Methods:
We retrospectively studied MS patients treated with HET/vHET in an MS specialized centre. TRSS, including the Rio Score, modified Rio Score and MAGNIMS score, were applied to assess response to treatment. We evaluated the predictive value of the TRSS on disease activity and disability progression.
Results:
TRSS effectively predicted disease activity and progression of disability in patients treated with HET/vHET. Patients with high TRSS scores at 12 months post-HET/vHET initiation had a significantly increased risk of relapses, new lesions on magnetic resonance imaging (MRI) scans and progression of disability at 4 years.
Discussion:
Our findings highlight the importance of personalized treatment strategies in MS. TRSS are valuable tools for monitoring treatment response, guiding clinical decision-making and optimizing patient care.
Keywords
Introduction
Multiple sclerosis (MS) is a chronic, inflammatory demyelinating and neurodegenerative disorder of the central nervous system. Up to 85% of patients present a relapsing–remitting (RRMS) stage at disease onset. Around 50% of untreated patients develop sustained and progressive disability or a secondary progressive multiple sclerosis (SPMS) disease after 10–15 years.1,2 Several disease-modifying therapies (DMTs) are available, with different efficacy in reducing relapse rates, progression of disability, incidence of new T2 or contrast-enhancing lesions (CELs) and development of brain atrophy. DMTs can be classified into low- to moderate-efficacy therapies (interferons, glatiramer acetate, teriflunomide and dimethyl fumarate), high-efficacy therapies (HET) (S1p modulators and cladribine) and very high-efficacy therapies (vHET; anti-CD20 monoclonal antibodies, natalizumab and alemtuzumab).3,4
Accumulated evidence from clinical trials and real-world studies supports that early DMT initiation has a favourable impact on MS prognosis.5–7 Controversies have emerged focusing on the optimal initial treatment strategy, specifically on the dichotomy between induction and escalation approaches. More recently, despite some safety concerns (particularly infections and malignancy risk), different authors suggest the earlier use of HET/vHET, even from the initial stages of MS, the better the long-term outcomes of the disease.8–12
Monitoring of treatment response is one of the most challenging topics in MS management. Several clinical and radiological scores have been designed to predict response to treatment in the long term. These are known as Treatment Response Scoring Systems (TRSS) and include the Rio, Modified Rio and MAGNIMS scores.13–16 Although certain studies have evaluated the MAGNIMS score in patients treated with fingolimod and natalizumab, the predictive utility of TRSS when using HET or vHET remains largely unexplored. In this context, and recognizing that HET and vHET are increasingly employed earlier in the disease course, the availability of validated scores to monitor and early predict therapeutic response is of paramount importance.
The main objective of this study is to evaluate the performance of TRSS in patients treated with HET/vHET.
Methods
Study design
We analysed prospectively collected data of a cohort of MS patients treated with HET at the MS Centre of Catalonia (Cemcat) between 2007 and 2021.
Patient selection
We selected patients with initial diagnosis of RRMS according to the McDonald criteria who received HET/vHET.17–20 Additional inclusion criteria were (1) patients who have received HET/vHET for at least 1 year, either naïve or having received only one platform DMT prior to starting HET/vHET or (2) patients whose first treatment was an HET/vHET but switched to another HET/vHET after 1 year of treatment due to intolerance, adverse effects, or increased risk of progressive multifocal leukoencephalopathy. We excluded patients with progressive MS at HET/vHET initiation, and those who, during follow-up, received a diagnosis different from MS. A flowchart detailing patient recruitment is shown in Figure 1.
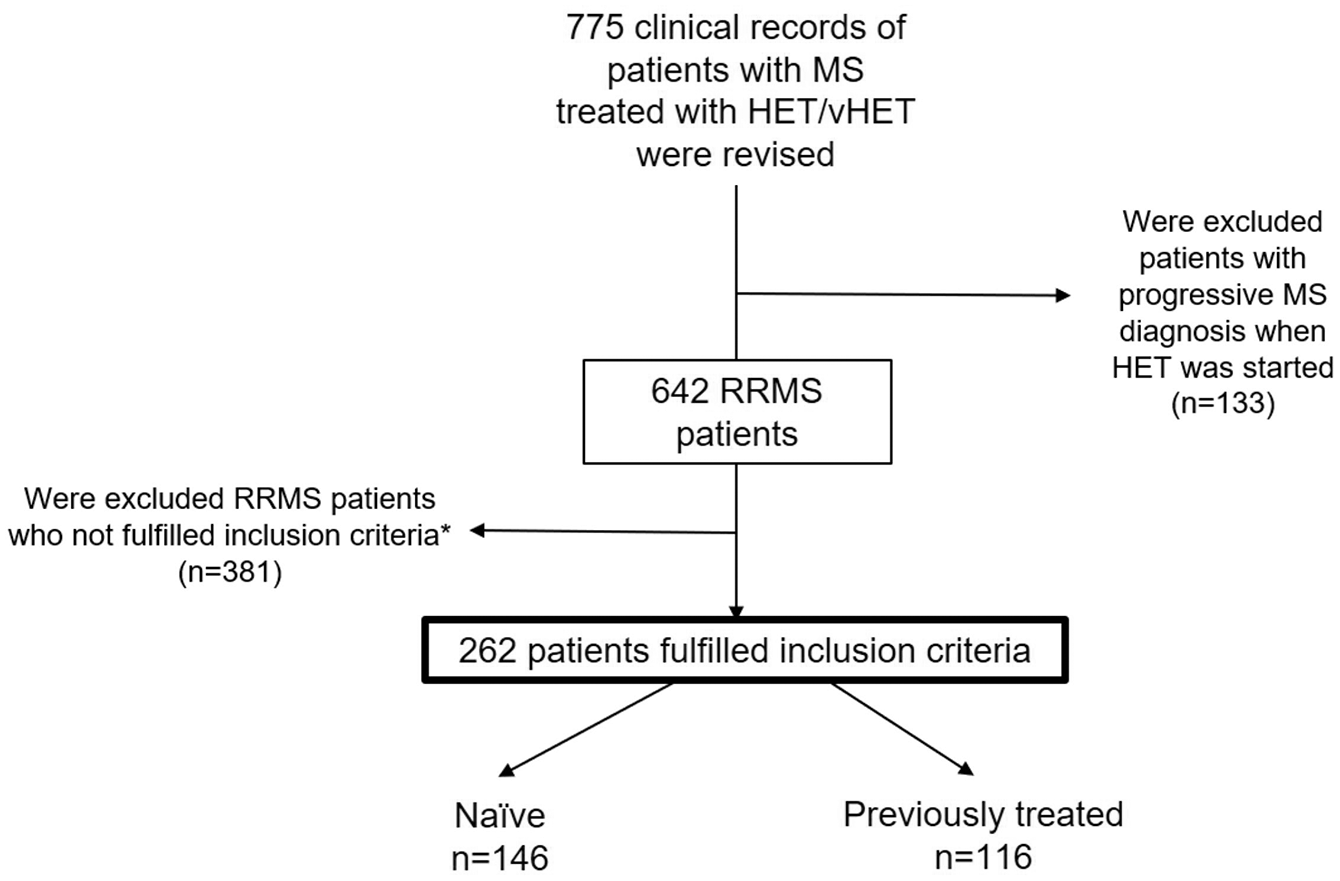
Patients’ selection flowchart. A prospectively followed cohort of 775 MS patients treated with HET/vHET was reviewed.
Fingolimod, cladribine tablets, natalizumab, ocrelizumab, rituximab and alemtuzumab were considered HET/vHET.3,4 Each DMT was used in strict accordance with the approved European Medicines Agency (EMA) guidelines regarding dosage and administration intervals (www.ema.europa.eu).
We collected demographic and clinical variables at the time of diagnosis, including age at disease onset, sex, topography of the first demyelinating event (spinal cord, brainstem and cerebellum, optic nerve, hemispheric and others) and cerebrospinal fluid (CSF) oligoclonal bands (OCBs) status. At the time of HET/vHET initiation, we recorded age, duration of the disease, number of relapses in the prior 12 and 24 months, T2 lesion burden, presence of CELs and expanded disability status scale (EDSS). 21 We also collected the type of HET/vHET prescribed, date of initiation and discontinuation.
A relapse was defined as the presence of a new typical symptom of MS or subacute worsening of existing symptoms, lasting at least 24 hours (with or without recovery), preceded by stability of at least 30 days, and in the absence of fever or infection. 20 Disability accumulation was defined as a confirmed increase in > 1 EDSS point in the absence of relapses for at least 6 months. 13 At the time of applying the TRSS (Month 12), radiological activity was defined as the presence of new T2 lesions or CELs. Beyond the run-in phase, only new T2 lesions were considered as radiological activity.
Each DMT was used in strict accordance with the approved EMA guidelines regarding dosage and administration intervals (www.ema.europa.eu).
Follow-up protocol
The study consisted of an initial run-in phase of 12 months, after which the different TRSS had been applied considering the clinical and radiological activity presented during this period. This stage was followed by an additional clinical and radiological monitoring phase from Months 12 to 48, to assess the potential predictive role of the different scores.
After HET/vHET onset, patients were evaluated in-clinic visits at least twice a year, when EDSS score and presence of new relapses were assessed. Magnetic resonance imaging (MRI) scans were performed on 1.5T or 3.0T up to 6 months before the initiation of HET using a standardized protocol that included the following sequences: (1) transverse 2D dual-echo T2-weighted fast spin echo; (2) transverse 2D T2-weighted fluid-attenuated inversion-recovery (FLAIR); and (3) transverse 2D T1-weighted spin-echo or gradient-echo. For all sequences, 46 interleaved contiguous axial sections were acquired with a 3-mm section thickness covering the whole brain, and with an in-plane spatial resolution of approximately 1 × 1 mm. At first MRI, the transverse T1-weighted sequence was repeated in all patients following administration of a gadolinium-based contrast agent (0.1 mmol/kg; scan delay, 5 minutes). Subsequently, follow-up studies were performed contrast-free annually. Experienced neuroradiologists blind to patients’ clinical status analysed MRI data.
Study outcomes
Performance of TRSS in patients treated with HET/vHET
Rio Score, modified Rio Score and MAGNIMS score were applied 12 months after starting HET/vHET. For the Rio Score, 1 point was considered for > 2 new T2 or CELs, 1 point for clinical relapses and 1 point for sustained EDSS score ⩾ 1. 13 The Modified Rio Score considered 1 point for > 4 new T2 lesions, 1 point for 1 clinical relapse and 2 points for patients experiencing ⩾ 2 relapses. 14 A MAGNIMS score of 0 was determined if patients developed with 0 relapses and < 3 new T2 lesions, 1 if patients developed with 1 relapse or > 3 new T2 lesions, 2 if patients presented 1 relapse and > 3 new T2 lesions or if patients developed with > 2 relapses. 16 A total of 0–3 points was calculated for the Rio Score and modified Rio Score, and a total of 0–2 points was calculated for the MAGNIMS score. Given that after starting HET/vHET, we usually expect minimal disease activity or an optimal response within the initial months of treatment, and to enable a robust statistical analysis, we recategorized patients into two groups: low score if they received between 0 and 1 points, and high score if they received between 2 and 3.
The performance of TRSS for predicting the appearance of new clinical or radiological activity (at least one clinical relapse or one new T2 lesion) or a confirmed increase in at least one EDSS point during the monitoring period was analysed separately for each response variable. Then, the risk of developing evidence of disease activity (EDA) by combining all variables was also calculated for each subcategory score (low score and high score).
As part of a sensitivity analysis, considering that many patients treated with induction drugs (cladribine tablets and alemtuzumab) achieve their maximum efficacy after 1 year of treatment onset, the performance of the TRSS was also examined by applying them at Month 24 after HET/vHET treatment initiation.
Statistical analysis
Demographic and clinical data were used for descriptive analysis. Parametric and non-parametric tests, specifically the chi-square test and Mann–Whitney U test, respectively, were applied according to the distribution of each variable. Quantitative variables were represented as the median and interquartile range (IQR).
Univariate Cox regression analyses were applied to evaluate the accuracy of TRSS for predicting the risk of developing clinical relapses, new T2 lesions, increase in disability and EDA during the monitoring phase.
Propensity scores were calculated using Inverse Probability Treatment Weighting (IPTW) to adjust for differences in disease duration between groups in each calculation. The IPTW approach assumes that the variable used for adjustment – in this case, disease duration – was accurately measured and appropriately modelled. Weights were calculated as w = 1/pw = 1/pw = 1/p for individuals in one group and w = 1/(1−p)w = 1/(1−p)w = 1/(1−p) for those in the other, where p represents the estimated probability of belonging to a specific group based on disease duration. This method ensured that disease duration was balanced across groups, minimizing its confounding effect on subsequent analyses. Given the differences in disease duration, all subsequent calculations were preceded by IPTW adjustments.
All statistical analyses were executed using Stata version 17 (StataCorp).
The study was approved by the local Ethics Committee, and all patients gave written informed consent to be included in the study.
Results
Patients’ characteristics
Among 775 patients with MS, 262 (181 female) fulfilled the inclusion criteria and were included. The median age at the first demyelinating event was 29 (24–36) years, and the median time from disease onset to the last follow-up visit was 8 (4–14) years.
Most patients initially presented with spinal cord syndromes (n = 132, 50.4%), followed by brainstem and cerebellum-related syndromes (n = 60, 22.9%) and optic neuritis (n = 46, 17.6%). The median EDSS at diagnosis was 2.0 (1.5–3), and 80% of patients presented at least one CEL on brain MRI at baseline. CSF-restricted IgG OCB were positive in 181 out of 201 cases tested (90%).
Notably, 146 patients (55%) were treatment-naïve. The reminder had previously received interferons, glatiramer acetate, teriflunomide, or dimethyl fumarate. The median relapse rate was 1 (1–3) and 2 (1–3) in the 12 and 24 months prior to HET and vHET initiation, respectively. The median age at HET/vHET initiation was 35 (28–42) years. HET/vHET were natalizumab (n = 97, 37%), ocrelizumab (n = 50, 19.1%), fingolimod (n = 48, 18.3%), alemtuzumab (n = 26, 9.9%), rituximab (n = 22, 8.4%) and cladribine tablets (n = 19, 7.3%). Patients’ baseline characteristics at the time of HET/vHET initiation are detailed in Table 1.
Characteristics of patients at the initiation of treatment according to the high-efficacy drug used.
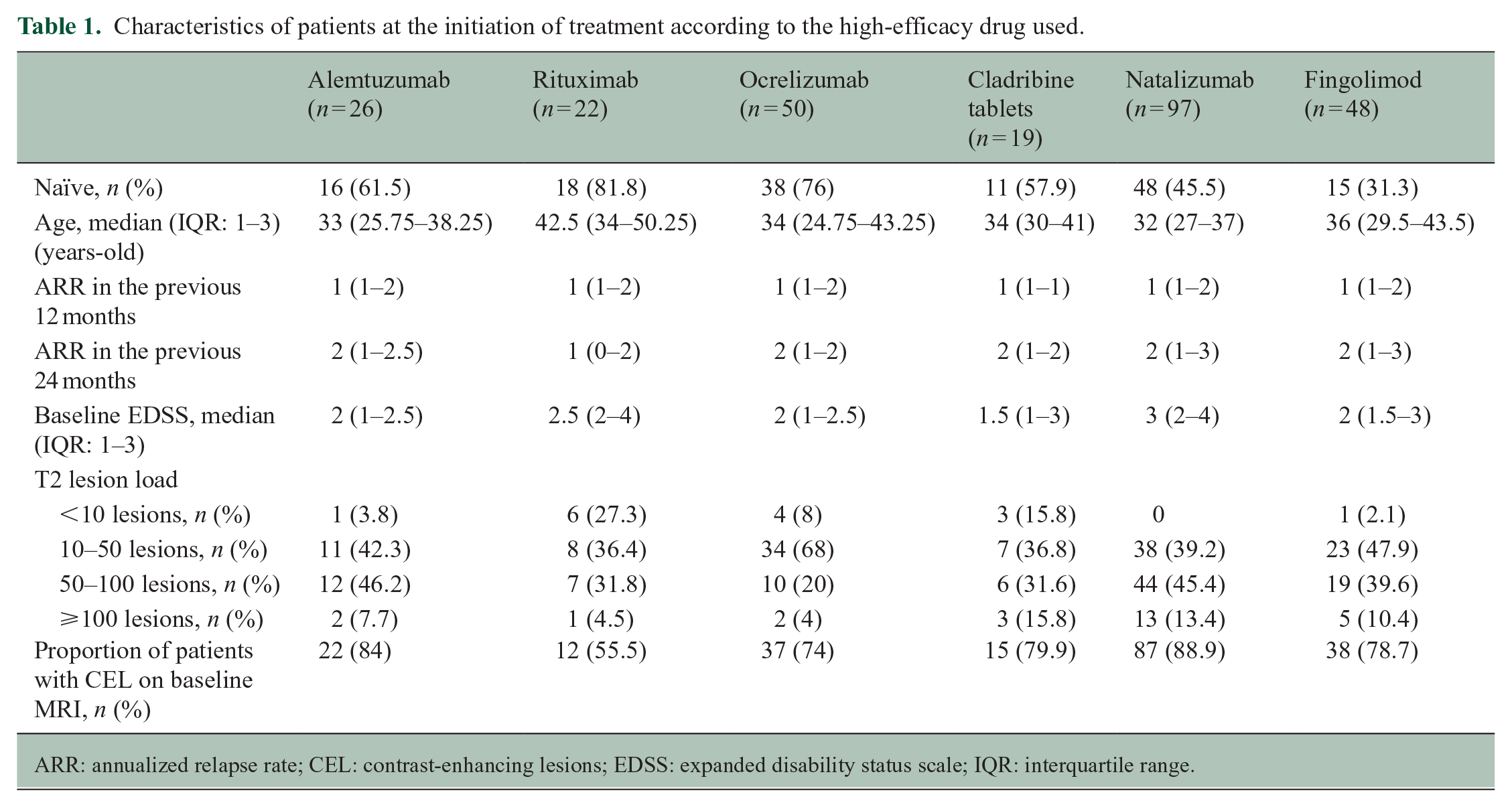
ARR: annualized relapse rate; CEL: contrast-enhancing lesions; EDSS: expanded disability status scale; IQR: interquartile range.
Treatment-naïve patients were older than those patients who switched from a low- to moderate-efficacy drug (31, 24–38.2 vs 28, 24–34 years, p = 0.03) at disease onset but younger (33, 26–41 vs 37, 30–43 years, p = 0.01) with a shorter disease duration (47 months, 31–65 vs 105 months, 61–147, p < 0.001) at the time of HET/vHET initiation. Naïve patients had received treatment in a more recent epoch (median year 2019 vs year 2014), had more CELs, and lower EDSS than those who switched from a platform drug (3.0 vs 2.0, p = 0.01 and 2.0 vs 3.5, p < 0.001). Remarkably, a higher number of patients who had previously received DMTs developed SPMS (26 vs 9, p = 0.002) which could be partially related to a longer disease duration (Table 2).
Comparative analysis between patients who were previously naïve or switched from a first-line drug when HET/vHET was initiated.
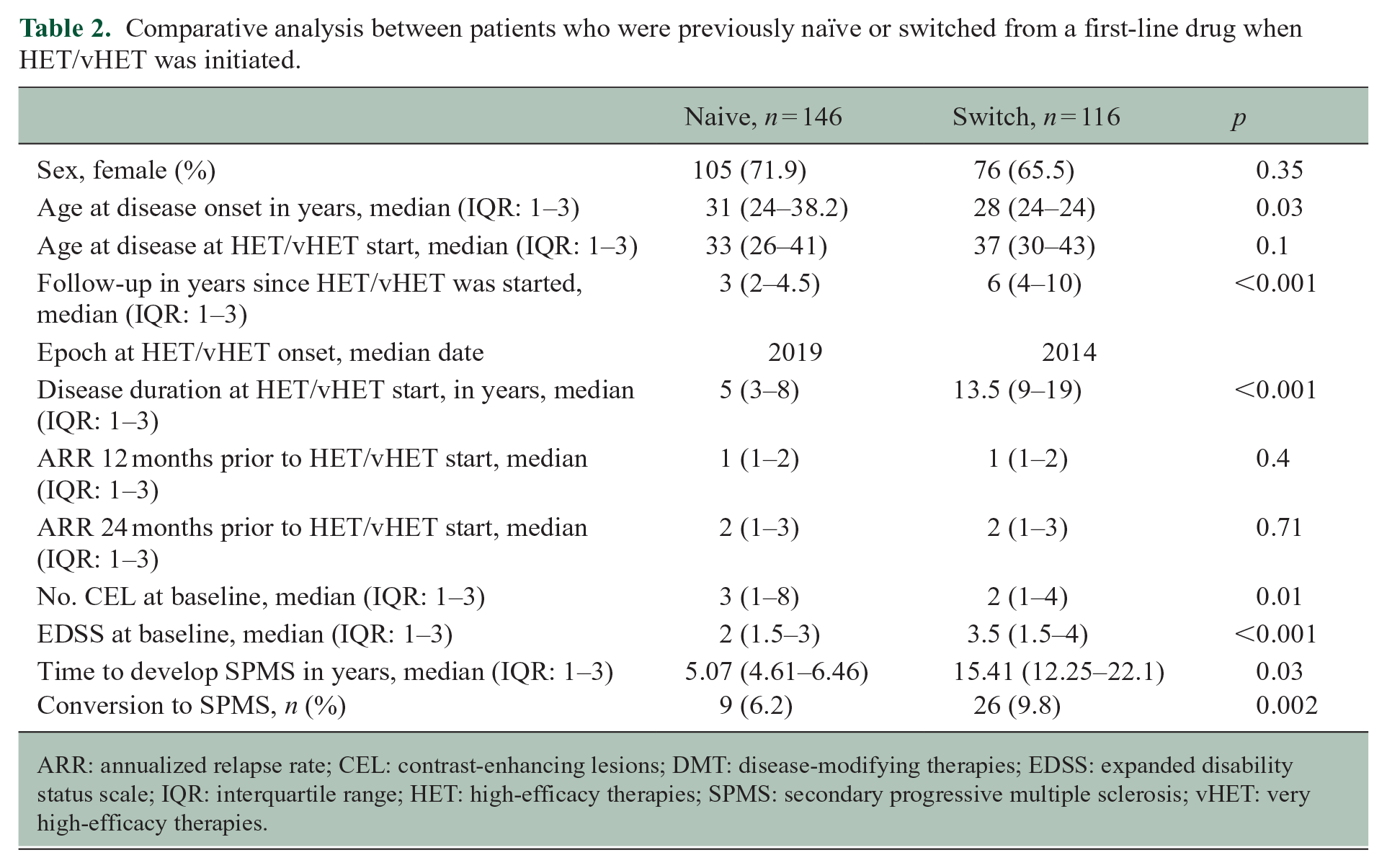
ARR: annualized relapse rate; CEL: contrast-enhancing lesions; DMT: disease-modifying therapies; EDSS: expanded disability status scale; IQR: interquartile range; HET: high-efficacy therapies; SPMS: secondary progressive multiple sclerosis; vHET: very high-efficacy therapies.
TRSS performance evaluation
Considering the difference in disease duration in both groups, all further calculations were preceded by adjustments with IPTW. Detailed matching results are provided in the Supplementary Table 1.
Patients with high Rio and MAGNIMS scores at 12 months after HET/vHET initiation had a statistically significant increased risk of experiencing relapses during the monitoring period (Rio Score HR = 11.11, 95% CI = 2.77–44.51, p < 0.001 and MAGNIMS score HR = 5.96, 95% CI = 1.07–33.35, p = 0.04). High-risk Rio Score patients, also had an increased risk of developing new T2 lesions on subsequent MRI scans (HR = 3.13, 95% CI = 1.23–7.63, p = 0.01) and increasing at least 1 point in the EDSS (HR = 6.86, 95% CI = 1.62–29.11, p < 0.01) (Table 3). High-risk patients in all TRSS at 12 months after HET/vHET initiation had an increased risk of presenting EDA during follow-up (Rio score HR = 10.51, 95% CI = 4.33–25.54, p < 0.0001), modified Rio score (HR = 5.05, 95% CI = 2–12.76, p < 0.0001) and MAGNIMS score (HR = 6.56, 95% CI = 2.92–14.75, p < 0.0001).
TRSS results.
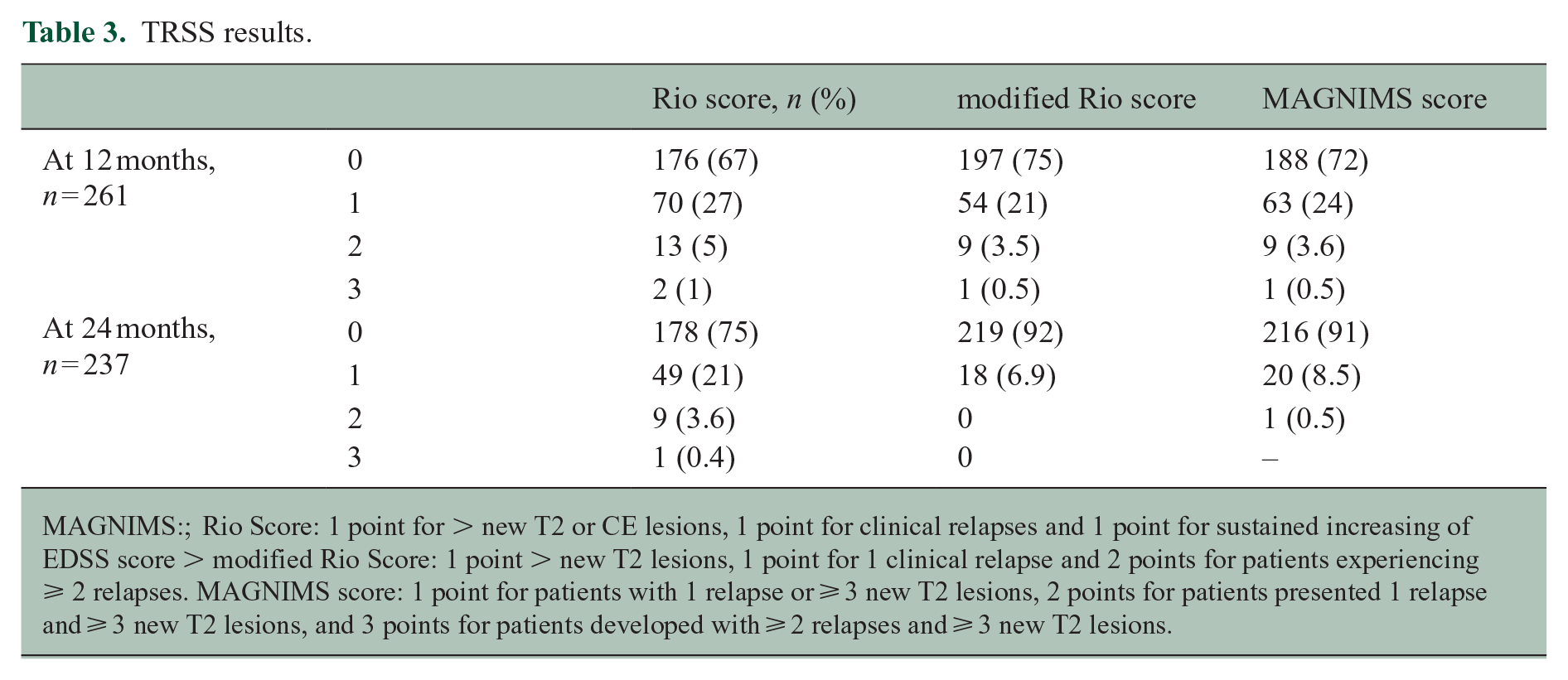
MAGNIMS:;
Rio Score: 1 point for > new T2 or CE lesions, 1 point for clinical relapses and 1 point for sustained increasing of EDSS score > modified Rio Score: 1 point > new T2 lesions, 1 point for 1 clinical relapse and 2 points for patients experiencing ⩾ 2 relapses. MAGNIMS score: 1 point for patients with 1 relapse or ⩾ 3 new T2 lesions, 2 points for patients presented 1 relapse and ⩾ 3 new T2 lesions, and 3 points for patients developed with ⩾ 2 relapses and ⩾ 3 new T2 lesions.
Patients who presented high Rio score at Year 2 developed with a significantly increased risk of developing clinical and radiological MS activity (HR = 35.27, 95% CI = 3.66–340, p = 0.02 and HR = 16.02, 95% CI = 4.61–55.71, p < 0.001, respectively) and tended to have more disability (HR = 4.72, 95% CI = 0.80–24.52, p = 0.08). Considering the small number of patients who had high-risk modified Rio Score and MAGNIMS score after 24 months of treatment, these calculations could not be made (Table 4). Interestingly, patients with high-risk Rio score at 24 months had an increased risk of presenting EDA during the next 2 years (HR = 4.02, 95% CI = 1.37–11.81, p = 0.01). These results are illustrated in Figure 2.
TRSS performance. Cox’s regression analysis results.
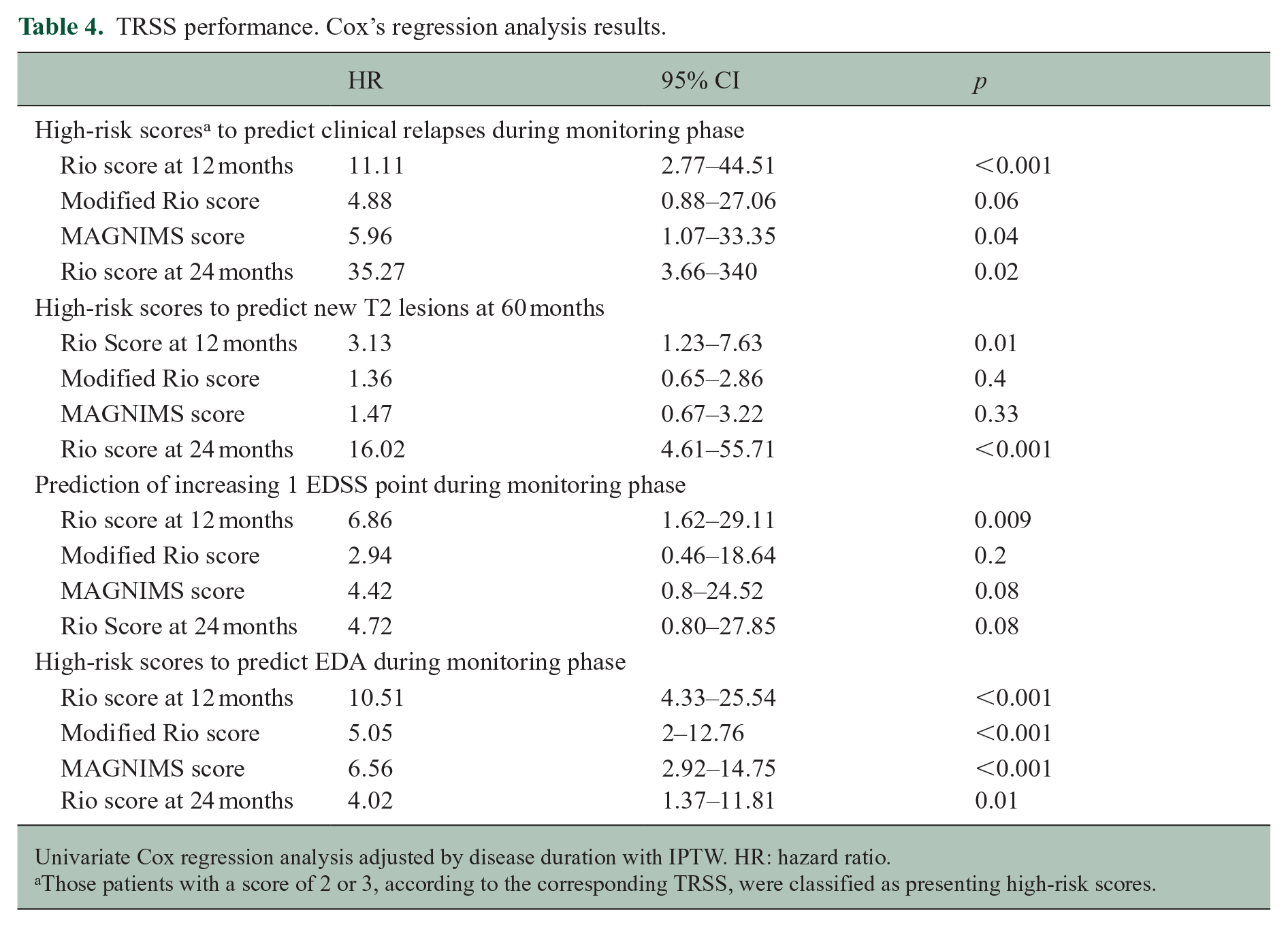
Univariate Cox regression analysis adjusted by disease duration with IPTW. HR: hazard ratio.
Those patients with a score of 2 or 3, according to the corresponding TRSS, were classified as presenting high-risk scores.
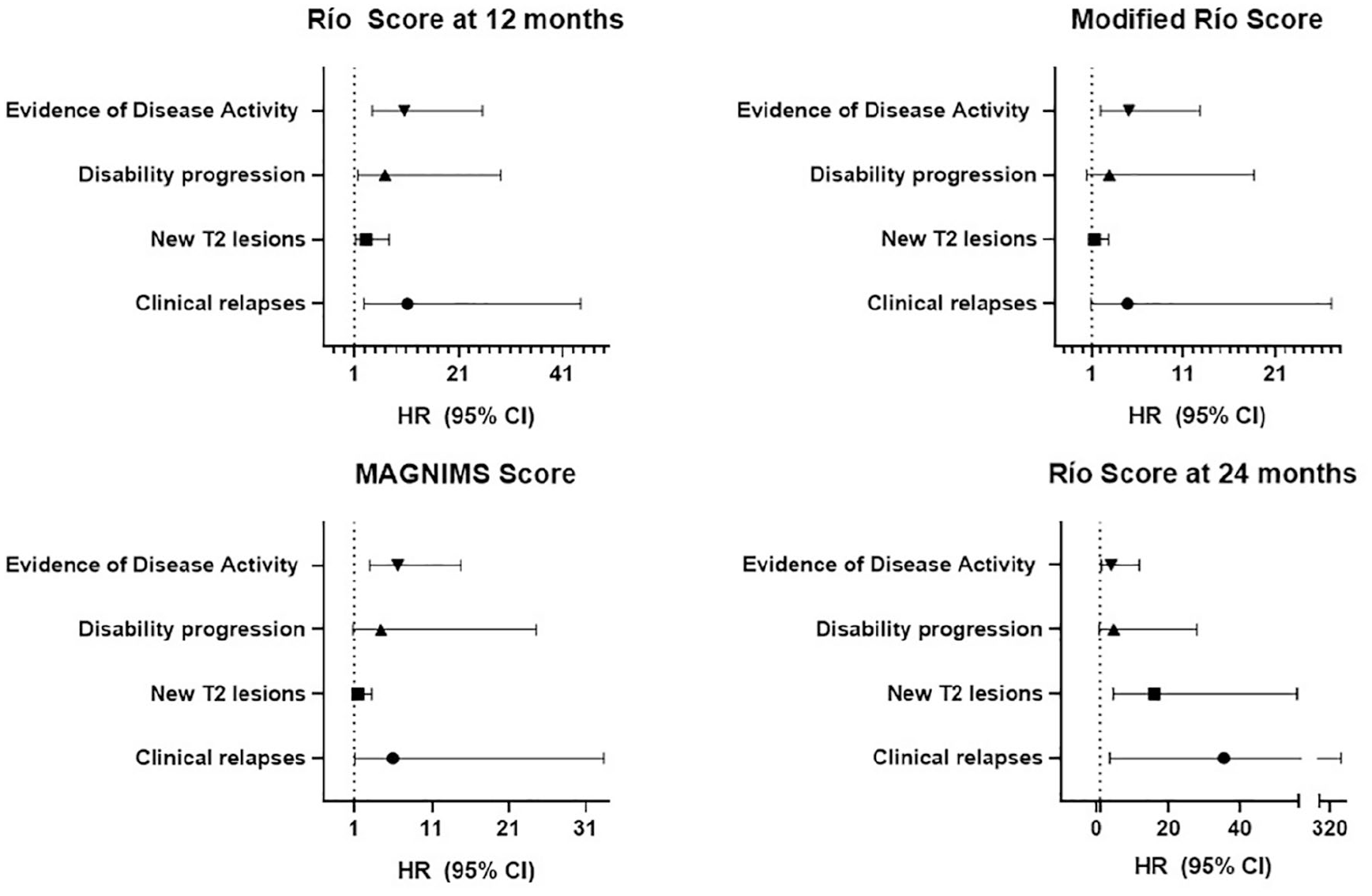
TRSS performance evaluation. Summarized illustrative results.
Discussion
Predicting disease course and treatment response is one of the most challenging aspects on MS management. In the past, different longitudinal cohorts showed that patients with older age at onset, male sex, black race and motor or cerebellar presentation had worse long-term disability outcomes.22–24 Early relapses, high lesion burden on MRI, and increasing EDSS in the first 2 years from disease onset additionally condition long-term disease outcomes, highlighting the importance of early therapeutic intervention in MS.25–27
Prompt initiation of treatment and its assessment of its effectiveness are equally important. The Rio Score and Modified Rio Score were developed mainly for patients treated with IFNβ. The MAGNIMS score was validated in patients with glatiramer acetate, fingolimod and natalizumab. We attempted to validate their use for patients under HET/vHET. To the best of our knowledge, this is the first study assessing the performance of TRSS in patients treated with all currently available HET/vHET. We show that TRSS are valuable for predicting disease activity and future disability.
The different key components of the Rio score, modified Rio score and MAGNIMS score can explain the differences we observed. The Rio score is more sensitive for radiologic activity. Also, it is the only score that considers the increase in the EDSS, which makes it more specific for predicting the progression of disability.
Our findings are clinically relevant because no biomarker can predict alone the therapeutic response. This study validates simple scores based on clinically available information for HET/vHET monitoring. Thus, the confirmed utility of TRSS in patients receiving these treatments allows the clinicians to identify the ideal candidates for treatment optimization, which could result in better disease control and prognosis.
Our study has several limitations. First, treatment-naïve patients and those who switched to HET/vHET from a platform drug were jointly assessed to better represent real-word situations, considering that in many countries, the escalation approach is still mandatory. Second, DMTs with different efficacy and safety profiles were combined for analysis. The possibility of evaluating monoclonal antibodies separately would significantly have decreased the sample size and would not precisely reflect daily clinical decision-making processes. Furthermore, the number of patients with EDA at 12 and 24 months after treatment initiation was limited, likely due to high treatment efficacy. Fourth, there was a very broad disease duration in the entire cohort. We addressed this issue by applying propensity score matching. Fifth, patients had not undergone a re-baseline MRI within 3–6 months after HET/vHET was initiated. In this line, although there is a possibility of misinterpretation when swapping MRI scanners (1.5T–3.0T and vice versa), the evaluation by two blinded radiologists with extensive experience in the field reduces these possibilities. Seventh, there is an epoch phenomenon: most recently diagnosed patients decreased the time to MS diagnosis and treatment onset. 27 Moreover, the currently available treatment options and the cumulative experience have allowed to use HET/vHET earlier in the recent years. Finally, it must be considered that this is a single-centre study, thus these results may be influenced by specific practices (e.g. timing of baseline MRI) or patients’ demographics, which could affect the applicability on the findings to a broader population.
As strengths, this is a detailed evaluation of a prospective, real-world and deeply phenotyped cohort of patients treated with HET/vHET, with prolonged follow-up. Patients were closely monitored and studied yearly with MRIs, which allowed us to validate the use of TRSS on patients treated with HET/vHET,
Although our findings provide novel evidence in disease monitoring and prognosis, these results need to be confirmed in extensive cohorts, likely through large multicentric collaborative efforts. It would also allow for further evaluation of how the scores that could not be assessed in this study behave in a 2-year analysis, based on how the scores are constructed and their corresponding higher cut-off points, particularly for new T2 lesions. Incorporation of biological biomarkers in the future may also increase sensitivity and specificity to predict treatment response. 28
Supplemental Material
sj-docx-1-msj-10.1177_13524585251316471 – Supplemental material for Performance of treatment response scoring systems among patients with multiple sclerosis treated with high-efficacy therapies
Supplemental material, sj-docx-1-msj-10.1177_13524585251316471 for Performance of treatment response scoring systems among patients with multiple sclerosis treated with high-efficacy therapies by Mariano Marrodan, Augusto Sao Avilés, Jordi Río, Álvaro Cobo-Calvo, Victoria Fernández, Agustin Pappolla, Joaquín Castilló, Ángela Vidal-Jordana, Georgina Arrambide, Carmen Tur, Breogán Rodríguez-Acevedo, Ana Zabalza, Neus Mongay-Ochoa, Andreu Vilaseca, Marta Rodriguez, Ingrid Galán, Manuel Comabella, Jaume Sastre-Garriga, Mar Tintoré, Cristina Auger, Àlex Rovira, Xavier Montalban and Luciana Midaglia in Multiple Sclerosis Journal
Footnotes
CRediT Statement
M.M., J.R., A.C.C., X.M. and L.M. contributed to conceptualization; M.M., J.R. and A.C.C. performed investigation; M.M. and L.M. involved in data acquisition and writing—original draft; M.M. and A.S.A. participated in formal analysis; X.M. and L.M. involved in writing—review and editing and supervision; L.M. participated in project administration; J.R., A.C.C., V.F., A.P., J.C., A.V.J., G.A., C.T., B.R.A., A.Z., N.M.O., A.V., M.R., I.G., M.C., J.S.G., M.T., C.A. and A.R. participated in reviewing and editing original manuscript.
Data Availability Statement
All data are available to interested investigators on reasonable request.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: M.M. has been awarded with a Du-Pré Grant during 2023 to develop this project; he received fees for educational presentations and conference attendance from Merck Serono Argentina, Biogen Idec Argentina, Novartis Argentina, Gador, AstraZeneca and Roche Argentina. A.S.A., V.F., J.C., M.R., I.G., C.A., A.R. and L.M. report no disclosures. J.R. has received speaking honoraria and personal compensation for participating on Advisory Boards from Biogen Idec, Genzyme, Janssen, Merck Serono, Novartis, Teva, Roche and Sanofi-Aventis. A.C.C. has received grant from Instituto de Salud Carlos III, Spain; JR19/00007. A.P. has received funding travel from Roche and speaking honoraria from Novartis; he performed an ECTRIMS Clinical Training Fellowship programme during 2021 and is currently performing an MSIF-ARSEP Fellowship programme. A.V.J. has engaged in consulting and participated as speaker in events organized by Roche, Novartis, Merck and Sanofi. G.A. has received compensation for consulting services, speaking honoraria or participation in advisory boards from Merck, Roche and Horizon Therapeutics; and travel support for scientific meetings from Novartis, Roche, ECTRIMS and EAN. C.T. is currently being funded by a Junior Leader La Caixa Fellowship (fellowship code is LCF/BQ/PI20/11760008), awarded by “la Caixa” Foundation (ID 100010434); she has also received the 2021 Merck’s Award for the Investigation in MS, awarded by Fundación Merck Salud (Spain) and a grant awarded by the Instituto de Salud Carlos III (ISCIII), Ministerio de Ciencia e Innovación de España (PI21/01860); in 2015, she received an ECTRIMS Post-doctoral Research Fellowship and has received funding from the UK MS Society; she is a member of the Editorial Board of Neurology and Multiple Sclerosis Journal; she has also received honoraria from Roche and Novartis and is a steering committee member of the O’HAND trial and of the Consensus group on Follow-on DMTs. B.R.A. has received speaking honoraria from Merck and honoraria for consulting services from Novartis. A.Z. has a predoctoral grant Rio Hortega, from the Instituto de Salud CarlosIII, Spain (CM22/00237), received travel expenses for scientific meetings from Biogen Idec, Merck Serono and Novartis; speaking honoraria from Eisai; and a study grant from Novartis. N.M.O. had a predoctoral grant Rio Hortega, from the Instituto de Salud Carlos III (CM21/00018); she also has received speaking honoraria and travel expenses from Merck and Roche. A.V. has received a Rio Hortega grant (CM22/00247) by Institute of Health Carlos III (ISCIII). M.C. has received compensation for consulting services and speaking honoraria from Bayer Schering Pharma, Merck Serono, Biogen Idec, Teva Pharmaceuticals, Sanofi-Aventis, Genzyme and Novartis. J.S.G. serves as a co-editor for Europe on the editorial board of Multiple Sclerosis Journal and as Editor-in-Chief in Revista de Neurología; receives research support from Fondo de Investigaciones Sanitarias (19/950); and has served as a consultant / speaker for Biogen, Celgene/Bristol Myers Squibb, Sanofi, Novartis and Merck. M.T. has received compensation for consulting services, speaking honoraria and research support from Almirall, Bayer Schering Pharma, Biogen Idec, Genzyme, Janssen, Merck Serono, Novartis, Roche, Sanofi-Aventis, Viela Bio and Teva Pharmaceuticals. Data Safety Monitoring Board for Parexel and UCB Biopharma, Relapse Adjudication Committee for IMCYSE SA. X.M. has received speaking honoraria and travel expenses for participation in scientific meetings, has been a steering committee member of clinical trials, or participated in advisory boards of clinical trials in the past years with Abbvie, Actelion, Alexion, Biogen, Bristol Myers Squibb/Celgene, EMD Serono, Genzyme, Hoffmann-La Roche, Immunic, Janssen Pharmaceuticals, MedDay, Merck, Mylan, NervGen, Novartis, Sandoz, Sanofi-Genzyme, Teva Pharmaceutical, TG Therapeutics, EXCEMED, MSIF and NMSS.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.