
Abstract
Background:
People living with multiple sclerosis (PwMS) are at risk of experiencing communication difficulties that can limit their vocational outcomes.
Objective:
To investigate clinical and cognitive variables that may contribute to communication restrictions in PwMS, and to evaluate how these factors affect vocational status.
Methods:
In this cross-sectional study, 502 PwMS underwent clinical and cognitive assessment tasks and were administered self-reported measures assessing fatigue and mood. The communication and language assessment questionnaire for persons with multiple sclerosis (CLAMS) was also administered.
Results:
Performance in information processing speed (p < 0.001), the presence of dysarthria (p < 0.001) and levels of self-reported fatigue (p < 0.001) were independent predictors of communication difficulties. Higher levels of communication difficulties were associated with a higher risk of unemployment and allowance (area under the receiver operating characteristic curve 0.649, p < 0.001 and 0.749, p < 0.001, respectively).
Conclusion:
Cognitive deficits, high levels of fatigue and the presence of dysarthria may independently contribute to communication difficulties in PwMS regardless of disease type or disability levels. These factors are associated with poorer vocational outcomes, highlighting the need for targeted interventions to support effective communication and improve employment prospects for this population.
Introduction
Multiple sclerosis (MS) is a chronic, immune-mediated disorder of the central nervous system, characterised by heterogeneity of clinical presentations. Cognitive and communicative symptoms have received increased attention in recent years due to their potential impact on the quality of life (QoL) of people living with MS (PwMS). 1
Communication is a broad umbrella term that refers to the exchange of ideas and information as facilitated by a number of capabilities, including speech, voice, expressive and receptive language and other cognitive functions. 2 Communication disorders in MS frequently manifest as movement-based speech impairments (i.e. dysarthria), 3 with growing evidence pointing to the occurrence of language-related symptoms as well. 4 Specifically, ‘speech’ can be defined as the planning, programming, control and execution of movements that produce the acoustic speech signal, 5 whereas ‘language’ involves expressive and receptive skills including phonology, morphology, semantics, syntax and pragmatics. 6
Cognitive impairment can cause problems with complex attention, executive functioning, information processing speed (IPS) and various aspects of memory, impacting approximately 40% to 55% of PwMS. 7 Cognitive impairment may correlate with communication impairment 8 and can have a negative impact on many aspects of daily life, such as the ability to run a household, engage fully in society and retain employment; all of which can diminish the overall QoL of PwMS. 7 Memory disturbances, such as forgetting names and appointments, slowed thinking and attention deficits may affect PwMS’ occupational performance and communication with colleagues, friends and partners. 8
Fatigue and depression are two prevalent MS clinical characteristics that also impact communication, activity and participation. Specifically, fatigue is a debilitating symptom affecting more than 80% of PwMS and refers to a subjective loss of physical capacity and/or mental energy. 9 The association between fatigue and communication in MS has been outlined in the literature.9,10 Fatigue may pose a challenge to the social interactions of PwMS, limiting their opportunities for communication. In addition, PwMS often experience deterioration of dysarthria and language-related cognitive functions with the onset of fatigue. 10 In addition, PwMS report exacerbations of fatigue, when trying to focus and interact with others. 8 Moreover, MS is a chronic neurological disorder with psychosocial and psychiatric implications. Depressive symptoms, in particular, are highly common in PwMS and have been found to negatively impact cognitive ability, language and communication. 11
The aim of this study is to investigate which demographic, clinical and cognitive variables are associated with functional self-reported communication difficulties in a large sample of PwMS. We additionally explore the potential associations between self-reported communication difficulties and employment status or allowance.
Materials and methods
Participants
A total of 502 PwMS were included in this study. Participants were recruited from two MS clinics, located in two tertiary university hospitals. Participants were eligible to participate in this study if they met the following criteria: (1) have a diagnosis of MS according to the McDonald revised 2017 criteria, (2) be ⩾ 18 and ⩽ 65 years of age, (3) be native speakers of the Greek language, (4) have a stable disease course, defined by the absence of clinical and radiological activity or disease progression over the last 6 months prior to their participation to this study and (5) have a Mini-Mental State Examination (MMSE) score > 24. Exclusion criteria included conditions that may interfere with participants’ performance in testing: (1) the presence of psychiatric disorders (e.g. untreated depression, psychotic states, alcohol or drug abuse) or psychotic symptoms, (2) concomitant neurologic disorders (such as epilepsy, stroke and traumatic brain injury), (3) history of neurodevelopmental communication difficulties (e.g. childhood stuttering), (4) larynx and/or other malignancies and (5) severe visual and/or hearing impairment.
Tests and measures
Neurologists, certified as Expanded Disability Status Scale (EDSS) raters examined all individuals without knowledge of any previous assessments. Participants’ cognitive function was evaluated by experienced neuropsychologists who were likewise blind to other parts of the investigation. Administration of all tasks and questionnaires was made in a quiet clinic room and in the same order to all participants.
Cognitive function was assessed with the Greek version of the Brief International Cognitive Assessment for MS (BICAMS), 12 which includes the Symbol Digit Modalities Test (SDMT) to assess IPS, the Greek Verbal Learning Test (GVLT) 13 –a cultural adaptation of the California Verbal Learning Test—to assess verbal memory and learning and the Brief Visuospatial Memory Test-Revised (BVMT-R) to assess visual/spatial memory. Raw scores of each participant’s performance in cognitive testing were used in the analysis. Communication and language difficulties were assessed using the Greek version of the communication and language assessment for people with multiple sclerosis (CLAMS), 14 which consists of 11 questions graded on a 4-point scale (0 = ‘never’ to 3 = ‘usually or always’), with a maximum score of 33. Self-reported fatigue was assessed using the Modified Fatigue Impact Scale (MFIS). 15 Mood was assessed using the Beck Depression Inventory–Fast Screen (BDI-FS). 16 Participants were classified as having dysarthria if they received a score of mild or greater dysarthria in the relevant component of the EDSS brainstem functional system score. The type of MS of each individual was determined on the basis of the disease course, extracted from each participant’s medical record and according to the current phenotypic classification. 17
Statistical analysis
Standard descriptive statistical analysis was employed for quantitative variables (mean, median, standard deviation (SD), minimum and maximum) and qualitative variables (frequency and percentage). To investigate the impact of the independent factors (age, sex, level of education, MS type, disease duration, EDSS score, fatigue, depression, dysarthria, SDMT, GVLT and BVMT-R) on the CLAMS score, univariable and multivariable linear regression analyses were applied. The dependent variable was the CLAMS score. For the multivariable linear regression, the stepwise method was selected, which combines both forward selection and backward elimination, with the probability values for entry and removal set to 0.05 and 0.10, respectively. The variable selection process began with the null model. Regarding ‘sex’, the female category was compared to the male category. Regarding ‘level of education’, the categories Postgraduate and Undergraduate/ College were treated as distinct categories within the regression analysis and were compared to the Basic/Secondary Education category. MS type was collapsed into two categories: relapsing-remitting MS (RRMS) and progressive MS (including secondary progressive MS and primary progressive MS subtypes). Regarding dysarthria, the ‘yes’ category was compared to the ‘no’ category. Next, receiver operating characteristic (ROC) analysis was employed to assess the ability of the CLAMS score to predict the working status of a participant, and separately whether the PwMS received allowance or not. The assessment was based on the value of the area under the curve (AUC) of the ROC curve in each case and the corresponding p-value. The level of significance was set at 0.05 in all cases of hypothesis testing. The statistical analyses were conducted using SPSS v27, and the R programming language, v4.3.3.
Ethics
This study was approved by the ethics committees of the Aristotle University of Thessaloniki (reference number 92/16-01-2024) and the University of Ioannina (reference number 15621/23-03-2022). All participants provided written consent prior to their participation in this study.
Results
Demographic and clinical characteristics
Participants’ demographic and clinical characteristics are presented in Table 1. All participants completed all tests and measures and there were no missing values. The mean CLAMS score was 18.51 ± 7.44. The mean performance in the BICAMS tests (SDMT, GVLT, BMVT-R) was 46.72 ± 13.90, 54.41 ± 11.31 and 23.87 ± 8.05, respectively. Participants’ mean performance in MFIS and BDI-FS were 29.53 ± 19.17 and 3.69 ± 3.82, respectively.
Participants’ demographic and clinical characteristics.
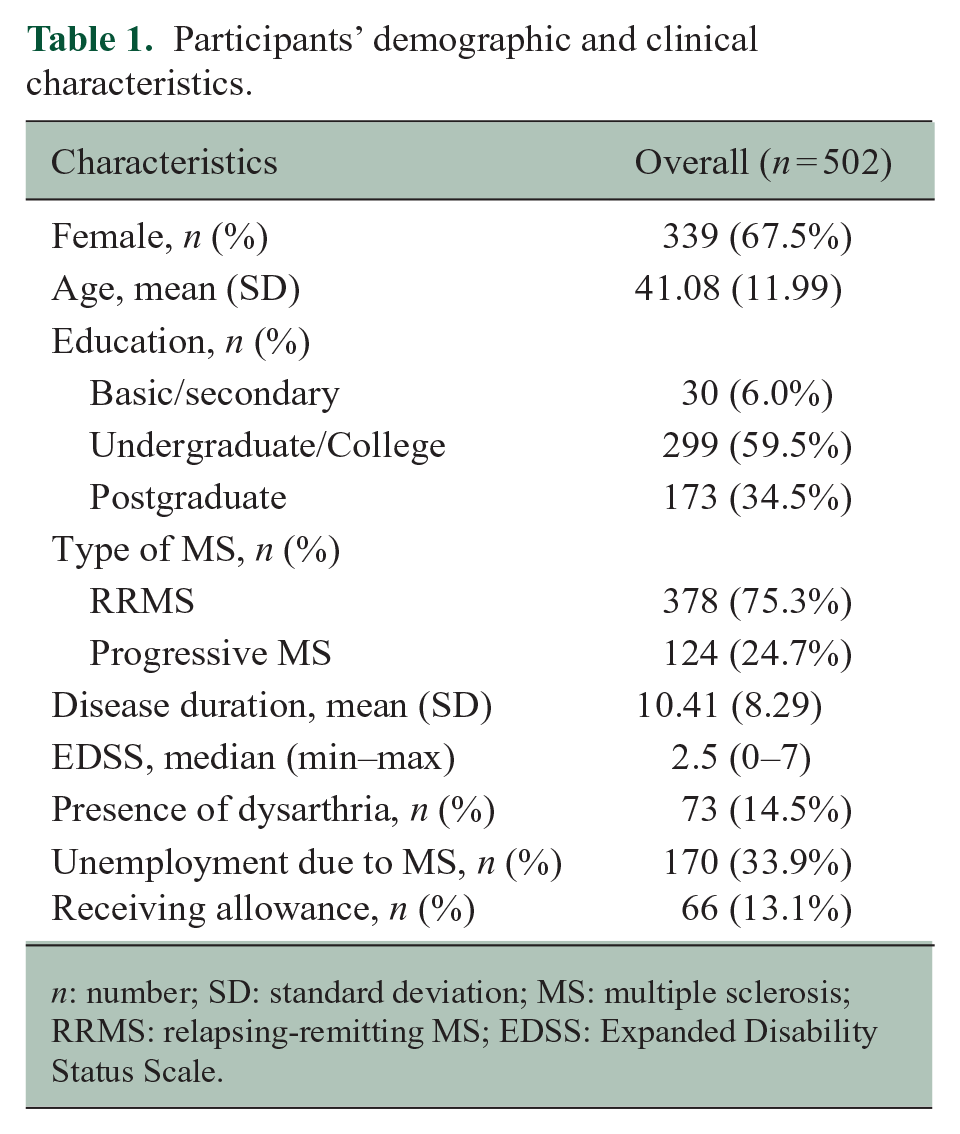
n: number; SD: standard deviation; MS: multiple sclerosis; RRMS: relapsing-remitting MS; EDSS: Expanded Disability Status Scale.
Univariable linear regression analysis
An initial univariable linear regression analysis revealed that age (0.147, p < 0.001), progressive course of the disease (4.383, p < 0.001), longer disease duration (0.163, p < 0.001), higher EDSS score (1.395, p < 0.001) and presence of dysarthria (6.910, p < 0.001) were all statistically significantly associated with self-reported communication difficulties. Similarly, the scores from questionnaires and cognitive tests (MFIS: 0.256, p < 0.001, BDI-FS: 0.788, p < 0.001, SDMT: −0.245, p < 0.001, GVLT: −0.174, p < 0.001 and BVMT-R: −0.334, p < 0.001) were significantly correlated with the CLAMS score . As compared to basic/secondary education, attending or having attended college was significantly associated with less communication difficulties (–5.055, p < 0.001), while for those with a postgraduate degree, this association was marginal (–2.756, p = 0.057). Sex (0.704, p = 0.322) was not associated with CLAMS score (see Table 2).
Univariable linear regression analysis of variables associated with the performance on the CLAMS questionnaire.
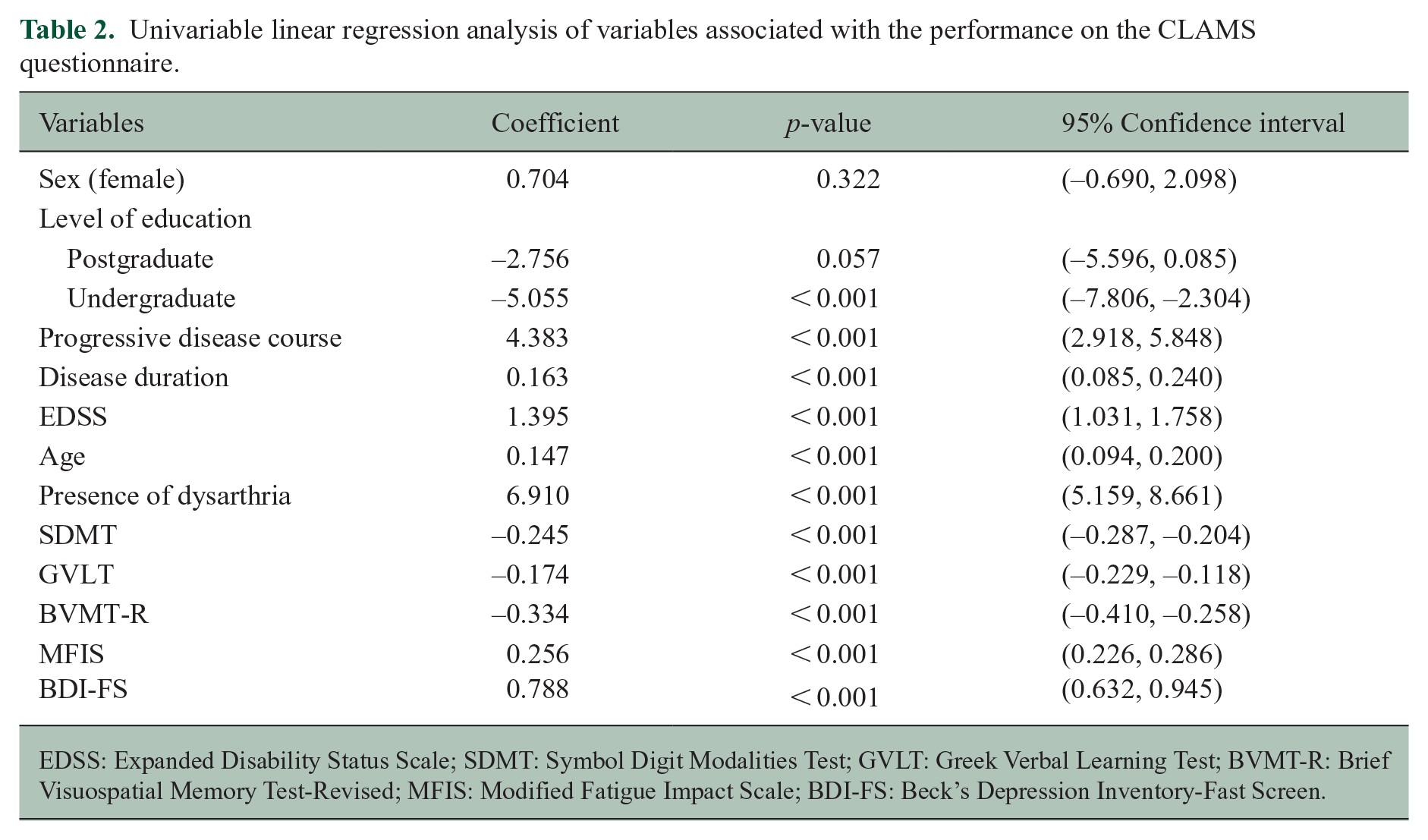
EDSS: Expanded Disability Status Scale; SDMT: Symbol Digit Modalities Test; GVLT: Greek Verbal Learning Test; BVMT-R: Brief Visuospatial Memory Test-Revised; MFIS: Modified Fatigue Impact Scale; BDI-FS: Beck’s Depression Inventory-Fast Screen.
Multivariable stepwise linear regression analysis
The multivariable stepwise linear regression analysis resulted in only three variables retaining their predictive capacity of communication difficulties in PwMS: SDMT score, dysarthria, and fatigue (see Table 3). Self-reported fatigue and dysarthria exhibited a statistically significant increasing impact on the CLAMS score (0.203, p < 0.001 and 3.307, p < 0.001, respectively), while SDMT performance had decreasing impact on the CLAMS score (−0.131, p < 0.001).
Multivariable stepwise linear regression analysis of variables associated with performance on the CLAMS questionnaire.
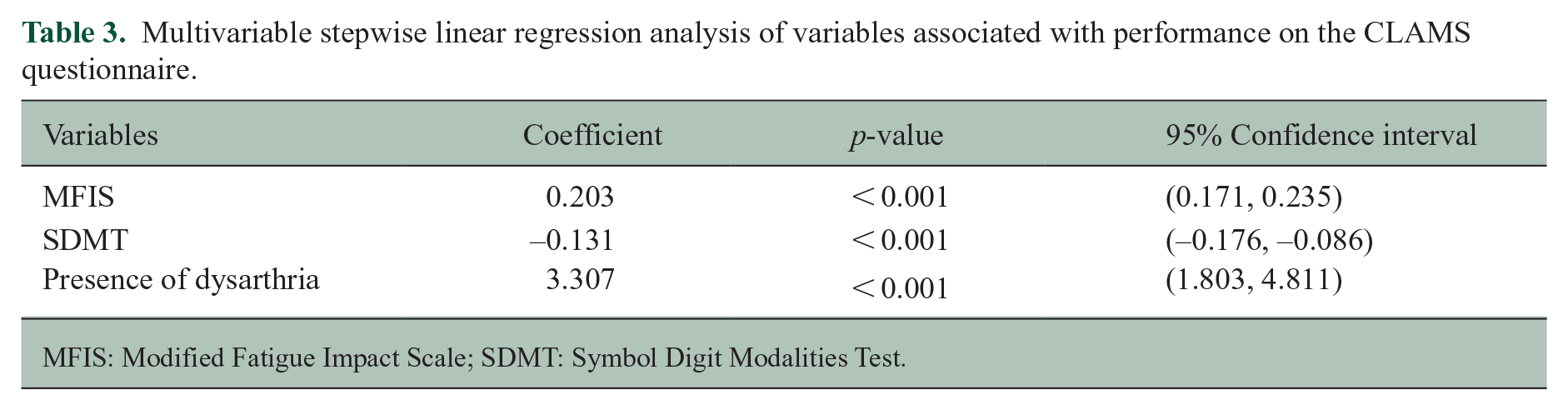
MFIS: Modified Fatigue Impact Scale; SDMT: Symbol Digit Modalities Test.
Communication difficulties and unemployment/allowance
The ROC curve analysis revealed that larger values on the CLAMS questionnaire indicated stronger evidence for a state of unemployment due to MS as the AUC of the ROC curve was 0.649 and statistically significantly higher than 0.5 (p < 0.001, 95% confidence interval (CI): 0.597–0.701; Figure 1(a)). In addition, the ROC curve analysis exhibited that larger values on the CLAMS questionnaire indicated stronger evidence for receiving allowance. The corresponding AUC of the ROC curve was found to be 0.749 (p < 0.001, 95% CI: 0.682–0.817; Figure 1(b)).
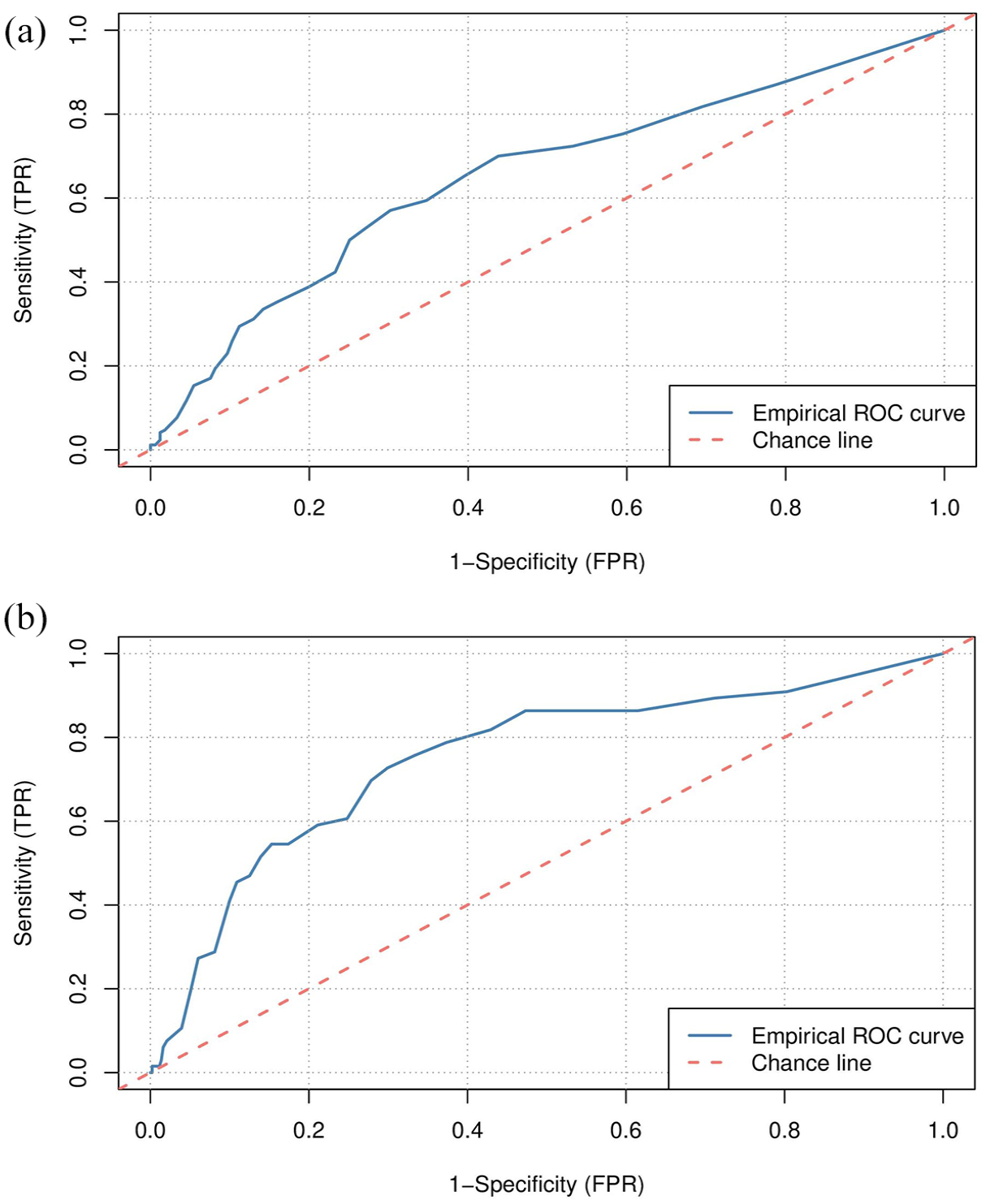
Receiver operating characteristic (ROC) curve analysis of the performance on the CLAMS questionnaire (a) on the working status and (b) on the unemployment allowance.
Discussion
There is increasing evidence that communication may be impaired in PwMS. 1 This study aimed to investigate which demographic, clinical and cognitive characteristics are associated with communication difficulties in PwMS, and their relationship with employment and allowance status. This study used both subjective (CLAMS, MFIS and BDI-FS) and objective neuropsychological instruments (BICAMS).
Most of the demographic (except for sex) and clinical variables were statistically significantly associated with the CLAMS score in the univariate analysis, and therefore entered the multivariate analysis, where they lost significance. Hence, communication difficulties may be observed in PwMS, regardless of such demographic or disease-related factors. This is consistent with prior research, which found that socio-demographic and clinical variables may not be useful in identifying PwMS at risk for communication difficulties. 18 In addition, the EDSS score did not correlate with self-perceived communicative function, despite previous research indicating the contrary. 19 The lack of emphasis on cognitive and communication skills in the EDSS might account for this outcome. 20
The comparison between the BICAMS and the CLAMS scores revealed that PwMS with lower SDMT scores, that is, greater deficits in IPS, were more likely to score higher on the CLAMS, indicating greater communication deficits. This finding aligns with the study conducted by Rodgers and colleagues, who investigated the cognitive predictors of communication/speech difficulties in 50 PwMS and found that IPS deficits, as measured by the SDMT and the Paced Auditory Serial Addition Test (PASAT), was the strongest predictor among numerous cognitive tests for speech problems. 21 Moreover, another research reported that decline in IPS was the most important factor for slow articulation rates in PwMS. 22 Slowed speech has been previously identified as a factor of poor communication in this population.8,10 Given that IPS is one of the most frequently affected cognitive domains in MS, even during early MS stages where clinical disability may be minimal, 23 this finding highlights the precocious and frequent emergence of communication difficulties in PwMS. On the contrary, various aspects of memory, as measured with the GVLT and the BVMT-R, were significant predictors of communication skills in the univariable regression analysis but not in the multivariable analysis.
Furthermore, the presence of dysarthria was linked to higher CLAMS scores. This finding is consistent with previous research suggesting that dysarthria might co-occur and impair other communication skills in PwMS. 24 Taking into account that CLAMS focuses more on the language/cognitive aspects of communication, a connection between speech and language is apparent.
The third significant variable in the multivariable analysis was self-reported fatigue. Participants who reported higher levels of fatigue in the MFIS questionnaire tended to score higher on the CLAMS questionnaire, suggesting that perhaps PwMS with fatigue experience greater communication difficulties. Results from other studies also suggest that communication difficulties, as well as cognitive, physical and psychosocial challenges that PwMS experience, can be caused by fatigue. 25 Furthermore, Yorkston et al. conducted qualitative interviews with seven PwMS, asking them about how everyday communication has changed as a consequence of MS. The combined effects of ‘speech’, ‘language’ and ‘cognitive’ changes, as well as ‘fatigue’, were all important variables. 26
According to the existing research, 54% of PwMS with low levels of physical disability (EDSS of 3 or less) are unemployed in Europe. 27 Having a job has been associated with language and cognitive abilities; unemployed PwMS perform worse on neuropsychological assessment tools than employed individuals. 28 Inversely, a study conducted using the Swedish MS registry found that cognitive abilities have an enormous impact on income, independent of physical disability. 29 Some cognitive tests, such as the SDMT or the PASAT, may predict unemployment in this disease group. 30 The current findings demonstrated, using ROC analysis, that the CLAMS score is also associated with vocational status; higher CLAMS score indicating the presence of significant communication difficulties was related both to unemployment and disability benefits income (allowance).
Previous studies have investigated variables associated with self-reported language and communication difficulties,18,30 but they did not use standardised neuropsychological assessment tools or neurological evaluation; instead, they used self-administered cognitive and symptom-related PROMs only. Other researchers focused on variables that could contribute to participation restrictions, but not on communication impairment. 19 This study supports existing literature and further adds that, in addition to IPS and fatigue, communication skills may have an impact on daily functioning and employment status.
Although PROMs, such as the CLAMS questionnaire, provide a useful means for evaluating variables that are difficult to observe objectively (e.g. fatigue, communication skills), there has been limited research on the relationship between PROMs and clinical assessment tasks (e.g. confrontational naming, verbal/written discourse production, verbal/reading comprehension, speech intelligibility). Furthermore, it is known from the existing research that PwMS might over- or under-estimate their cognitive and physical abilities 31 and PROMs may provide only the patients’ perspective; however, they remain a useful insight for clinical management.
Progressive types of MS generally result in more severe cognitive impairment than RRMS. 7 In addition, specific language functions, such as verbal fluency, are primarily affected in the later stages of the disease, especially in individuals with progressive MS types. 32 Nevertheless, the majority of our sample comprised of PwMS with a relapsing-remitting disease course; therefore, significant language and cognitive deficits were not expected. Hence, future studies should include individuals with greater disease severity to measure the impact of cognitive functioning on communication skills across the spectrum of disease severity.
It is also important to recognise the different definitions of terms such as ‘communication disorders’, ‘communicative functioning’, ‘communicative participation’ and ‘speech and language impairment’, as well as the different neuropsychological assessment tools that have been used across the research to measure cognitive and communication skills. Accordingly, this variability may contribute to a degree of heterogeneity and inconsistencies in study results, leading to the possibility that some PwMS identified as having cognitive or communication impairments in one study might not be classified as such in another. Therefore, developing and using psychometrically robust tools, such as the CLAMS, could be beneficial for evaluating communication difficulties in PwMS. Future research could focus on developing a clinical assessment specifically designed to evaluate all aspects of communication in PwMS. Such a new clinical tool could incorporate elements from established communication assessment tools, such as those used for post-stroke or traumatic brain injury, while also considering additional aspects that have the most impact on communication in PwMS. Validating and optimising this tool for PwMS would ensure that it effectively considers the aspects unique and most relevant to their communication challenges. In addition, it would be beneficial for the MS research community studying communication to establish standardised terminology for terms such as ‘speech’, ‘language’, ‘cognition’ and ‘communication’ to promote more consistent progress in this area of research.
This study presents an early model of communication function in MS, highlighting that communication difficulties are significantly associated with deficits in IPS, dysarthria and fatigue. There is a timely need to develop evidence-based interventions to support PwMS manage communication changes and reduce their impact 33 and our findings can inform future intervention approaches. Future research could focus on developing a treatment protocol that incorporates motor speech exercises, education on optimising fatigue management and cognitive skills training along with self-management strategies. This approach could draw inspiration from the ‘Living with Dysarthria’ treatment programme for individuals living with chronic speech problems. 34
Conclusion
This study presents an early model of communication function in PwMS, highlighting significant symptom-related variables (dysarthria and fatigue) and cognitive variables (IPS) that impact communication. The findings reveal that a decline in communication skills correlates positively with reduced career opportunities. This helps identify individuals who are at high risk of unemployment due to their MS. This research identifies critical symptom-related and cognitive variables that affect communication, defining clinically meaningful changes in communication skills. These insights provide valuable guidance for clinicians in advising PwMS about changes in their work capacity over time. Moreover, this study highlights the need for tailored clinical assessments and interventions for PwMS. Future research can draw inspiration from existing assessment tools and treatment protocols from other clinical populations to better address the unique challenges faced by PwMS in managing their communication changes and work capacity over time, ultimately to improve their QoL.
Footnotes
Consent to Participate
All participants had been informed about the nature of the study and provided written consent prior to their participation. They were also notified that they could withdraw from the study at any time without any impact on their medical care.
Data Availability
Data and material are available upon reasonable request to the corresponding author.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: C.B. has received travel support and lecture fees from Novartis, Merck, Genesis Pharma, Sanofi, Teva, Roche, Viatris, Bristol Mayers Squibb, Tikun Olam Europe, Pharmaserve – Lilly and Sandoz . M.-K.B. has received travel support and/or research grants and/or lecture fees and/or advisory services from the Hellenic Foundation for Research and Innovation (H.F.R.I.), the Ministry of Education’s Education and Lifelong Learning Program, the Hellenic Neurological Society, the Hellenic Academy of Neuroimmunology, Biogen, Novartis, Teva, Bayer, Genesis, Sanofi, Roche and Merck, N.G. has received travel support and/or research grants and/or lecture fees and/or advisory services from Novartis, Bayer, Merck, Genesis, Sanofi, Roche, Biogen, Teva and Viatris. T.M., N.D., S.E.-W., A.A., E.N., G.N. and L.M. report no disclosures.
Ethical Considerations
This study was approved by the ethics committees of the Aristotle University of Thessaloniki (reference number 92/16-01-2024) and the University of Ioannina (reference number 15621/23-03-2022).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.