
Abstract
Introduction:
Neurofilament light chain (NfL) and glial fibrillary acidic protein (GFAP) are associated with multiple sclerosis (MS) outcomes. We compare how high-efficacy early therapy (HEET) and lower-efficacy early therapy (LEET) affect serum NfL and GFAP at the initiation of disease-modifying therapy (DMT) and in the years afterwards.
Methods:
Adults diagnosed with MS within 5 years of symptom onset at our centre were eligible. Records from DMT-naïve patients with serum NfL and GFAP drawn in the year before treatment start and follow-up samples 6–36 months after treatment initiation were included in the ‘pre-initiation’ cohort. Those with baselines after DMT initiation and follow-up samples within 5 years were included in the ‘post-initiation’ cohort.
Results:
There were 155 pre-initiation patients (HEET: 85, LEET: 70) and 213 post-initiation (HEET: 55, LEET: 158). NfL levels were reduced following DMT initiation but did not differ significantly between HEET and LEET in either cohort. GFAP was not substantially impacted by either HEET or LEET.
Conclusion:
The difference in NfL reduction with HEET and LEET may be smaller than anticipated, perhaps reflecting that disease activity risk is considered in real-world DMT selection. There is minimal impact of HEET or LEET on GFAP, at least over several years.
Keywords
Introduction
Over the past two decades, there has been a proliferation of disease-modifying therapies (DMTs) for multiple sclerosis (MS). Clinicians face competing goals of achieving no evidence of disease activity (NEDA-3; no clinical relapses, new magnetic resonance imaging (MRI) lesions or disability progression) while minimizing the risks associated with immunosuppression. This has led to debate about whether to use lower-efficacy early treatment (LEET) and switch to more potent DMTs if NEDA-3 is not achieved (‘escalation therapy’) or use highly effective early treatment (HEET or ‘induction therapy’) and potentially de-escalate over time.
Multiple studies now demonstrate improved outcomes for HEET at a population level. A combined analysis of Swedish and Danish MS registries found reduced rates of 24-week confirmed disability worsening and of reaching expanded disability status scale (EDSS) scores of 3 or 4 in Sweden compared to Denmark (where a lower percentage of patients were started on HEET). 1 Similarly, a study from the United Kingdom showed less 5-year EDSS progression and a longer time to sustained disability worsening in those on HEET compared to LEET. 2 Despite population-level data, the decision about which DMT to use and for how long can be difficult in individual cases. Tools such as serum biomarkers provide additional quantitative measures of MS disease activity that may not be otherwise captured in the NEDA-3 framework.3,4
Among the most well-studied biomarker proteins in MS, neurofilament light chain (NfL) is a cytoskeleton protein released in the setting of axonal damage and is consequently elevated in the presence of new gadolinium-enhancing lesions. NfL also has prognostic value, correlating with future brain atrophy, clinical relapses and conversion from clinically isolated syndrome (CIS) to MS.5,6 Glial fibrillary acidic protein (GFAP), a marker of astrogliosis, is not directly affected by acute inflammatory lesions in MS but does predict disability worsening.7–9 Serum biomarkers can now be drawn for routine clinical use in the United States and may help to risk stratify patients and guide DMT choice.
GFAP levels are generally reported not to change with DMT use in MS, although data are mixed.10–14 In contrast, NfL levels are reduced with DMT use, and increases in NfL following DMT discontinuation can help predict the need to resume treatment.15,16 NfL in cerebrospinal fluid (which correlates with serum levels) is further reduced on higher-efficacy DMTs such as natalizumab and fingolimod compared to interferon beta-1a and glatiramer acetate.6,11,16–19 While patients on anti-CD20 therapy have lower NfL levels on average in randomized control trials and after escalating from platform therapy, the change in NfL levels across HEET and LEET paradigms in a real-world cohort at DMT initiation is less clear, as many oral therapies have not been included in these comparisons.19,20 Data on the impact of HEET and LEET on GFAP at DMT initiation and longitudinally are also limited. In this study, we compare how treatment with HEET and LEET strategies affects serum NfL and GFAP levels in real-world cohorts of MS patients at DMT initiation and in the years following treatment start.
Materials and methods
Research ethics
This research was approved by the Mass General Brigham Institutional Review Board. Patients provided written informed consent as part of the Comprehensive Longitudinal Investigation of Multiple Sclerosis at Brigham and Women’s Hospital (CLIMB) study.
Data source
Clinical and demographic information on patients enrolled in the CLIMB study who met inclusion criteria was queried from the Brigham MS Centre Research Database. Serum NfL and GFAP were measured according to previously published methodology. 7 Serum samples were stored in red-topped tubes and frozen at −80 degrees centigrade. Samples were then thawed and run on a single-molecule array platform using a Neurology-4-Plex A assay kit from Quanterix (Quanterix Corp., Billerica, MA, USA).
Study population
The inclusion criteria were as follows: (1) adult patients who were diagnosed with MS by McDonald 2010 or 2017 criteria within 5 years of symptom onset (or first abnormal MRI in the case of those who started as radiologically isolated syndrome [RIS]); (2) DMT initiation after 2005 (corresponding to Food and Drug Administration (FDA) approval of natalizumab); (3) at least two serum NfL and GFAP samples corresponding to the time points listed below; and (4) treatment with HEET or LEET for at least 1 year. We defined HEET to include S1P receptor modulators, B-cell therapy and natalizumab. Glatiramer acetate, interferons, teriflunomide and fumarates were classified as LEET. Treatment was selected according to patient preference and the clinical judgement of the treating MS specialist.
Patients were divided into two cohorts based on the timing of biomarker samples relative to DMT initiation. Cohort A (‘pre-initiation’) was composed of treatment-naïve patients who had baseline samples drawn in the year prior to starting DMT and follow-up samples in the 6 months to 3 years after treatment start. Cohort B (‘post-initiation’) had all samples drawn after DMT initiation and served as a longitudinal comparison of the on-treatment change. For these patients, baseline samples were chosen as close to DMT start as possible; follow-up samples were taken after at least 1 year of treatment and within 5 years of starting a DMT. Those who did not have baseline or follow-up samples within the above ranges were excluded. Patients were categorized as HEET or LEET based on the first DMT recorded in the database. Given the difficulty of assessing treatment adherence at scale, an intention-to-treat analysis was used.
Statistics
The characteristics of the HEET and LEET groups were compared using two-sample t-tests for continuous variables, a chi-square test for sex and Fisher’s exact test for corticosteroid use. These comparisons were performed separately in the two cohorts. Biomarker levels were compared using two-sample t-tests. Each comparison was completed separately in the two cohorts. For time-to-event analyses (time-to-sustained progression, time-to-relapse and time-to-MRI events), a Cox proportional hazards model was used to compare the HEET and LEET groups. A multivariable model was used to estimate the treatment group difference adjusting for age, sex and baseline EDSS, and pre-treatment biomarker levels were assessed as a predictor of each of the time-to-event outcomes. As a secondary analysis, the median follow-up NfL and GFAP levels and the change in levels over time were stratified by DMT class and assessed using the Kruskal–Wallis test. All statistical analysis was completed in R version 3.6.3 (www.r-project.org).
Results
Population
The pre-initiation cohort included 155 patients (85 on HEET, 70 on LEET; Figure 1). Both arms had relatively limited disability (Table 1). However, the HEET group was slightly younger and included more patients with progressive disease. Pre-treatment samples were drawn an average of 0.23 years before any DMT exposure. Post-treatment samples were drawn 2.10 years after DMT initiation on average (mean time between samples: 2.33 years).
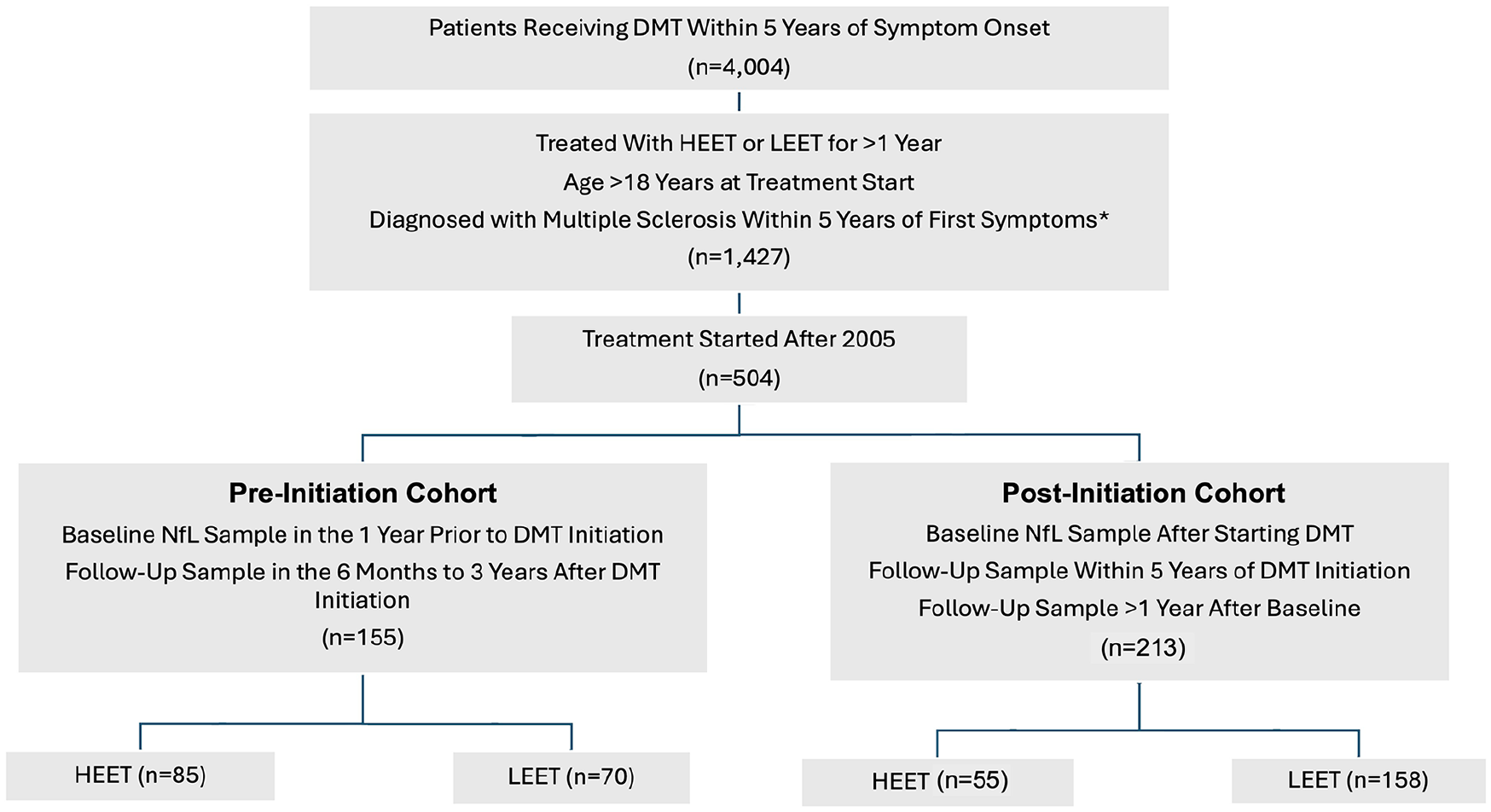
Consort diagram of patients screened and included.
Pre-initiation cohort characteristics.
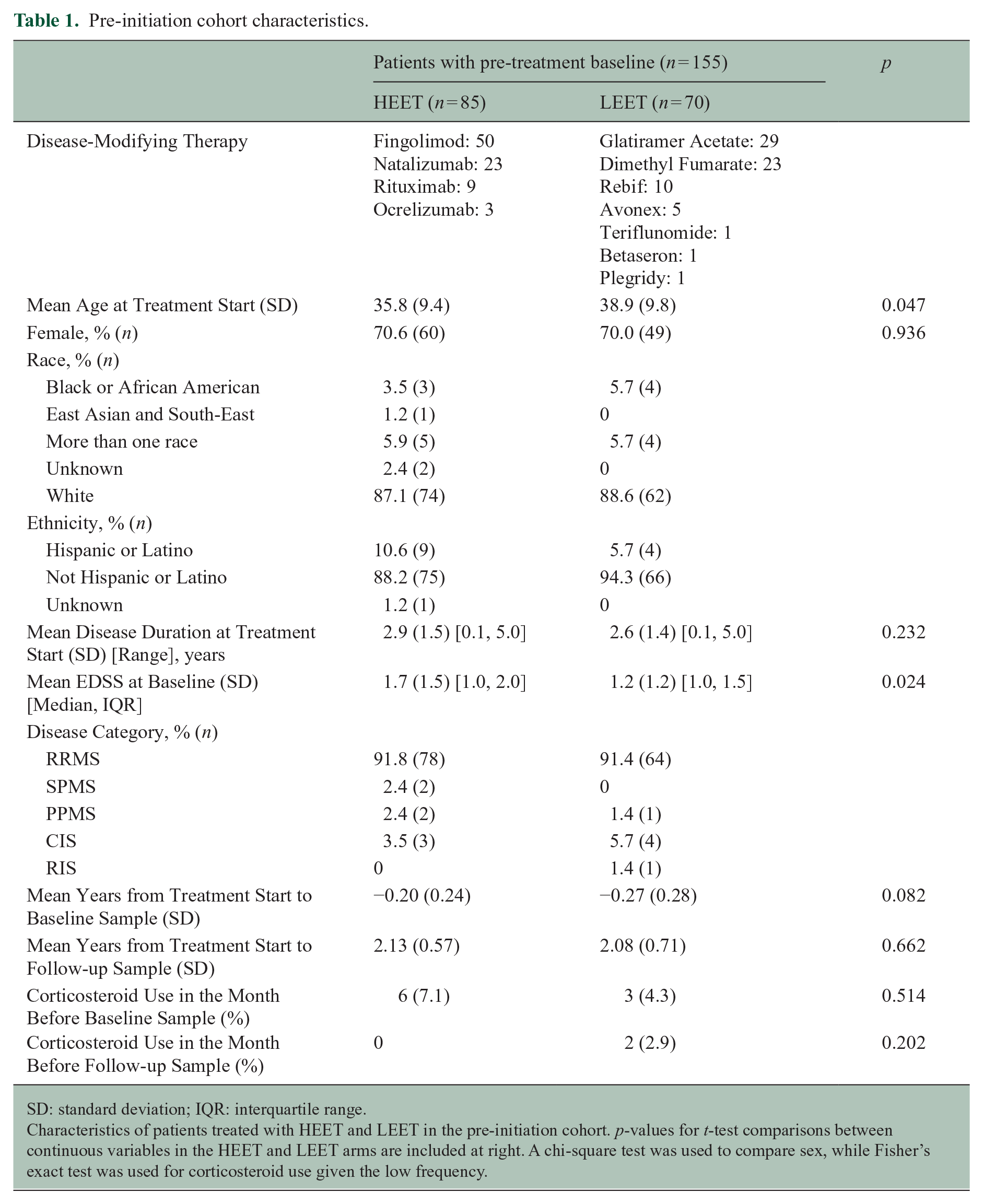
SD: standard deviation; IQR: interquartile range.
Characteristics of patients treated with HEET and LEET in the pre-initiation cohort. p-values for t-test comparisons between continuous variables in the HEET and LEET arms are included at right. A chi-square test was used to compare sex, while Fisher’s exact test was used for corticosteroid use given the low frequency.
Among the 213 patients included in the post-initiation cohort, 55 were on HEET, compared to 158 on LEET. Reflecting the observational nature of the data, the LEET arm was older with a lower EDSS and longer disease duration (Table 2). In the post-initiation patients, first biomarker samples were drawn an average of 1.13 years after starting treatment. On average, follow-up samples were drawn 3.79 years after DMT start (mean time between samples: 2.66 years). Few patients in either the pre- or post-initiation cohort received corticosteroids in the month before baseline and follow-up samples were drawn (Tables 1 and 2). The frequency of corticosteroid use was not significantly different between HEET and LEET patients.
Post-initiation cohort characteristics.
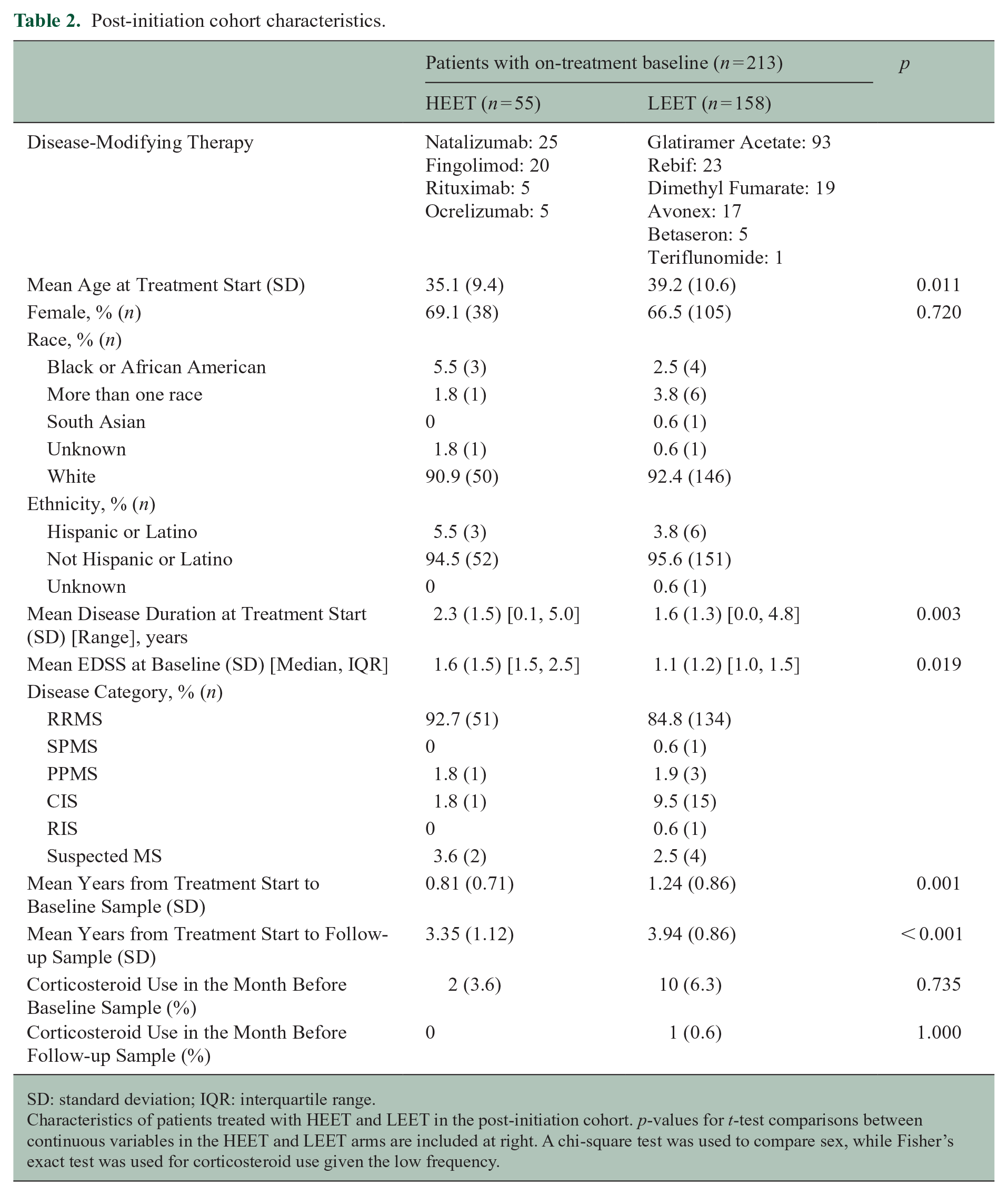
SD: standard deviation; IQR: interquartile range.
Characteristics of patients treated with HEET and LEET in the post-initiation cohort. p-values for t-test comparisons between continuous variables in the HEET and LEET arms are included at right. A chi-square test was used to compare sex, while Fisher’s exact test was used for corticosteroid use given the low frequency.
One patient on fingolimod was retrospectively excluded from the post-initiation HEET cohort as an outlier, as her NfL level increased by over 300 pg/mL (approximately 10 times more than the patient with the next greatest increase). On chart review, the patient had a cholecystectomy 3 months before her follow-up biomarker sample; she developed hepatitis post-operatively and temporarily discontinued fingolimod. At the time of her repeat NfL level, she had no new lesions on MRI, but she had experienced a significant functional decline since hospitalization, with EDSS increasing from 2.0 to 6.5.
NfL, but not GFAP, is reduced with treatment initiation for both HEET and LEET
Prior to DMT start, mean NfL in the pre-initiation cohort was elevated compared to established age-matched healthy controls (Table 3). 21 There was no significant difference in NfL between the HEET and LEET arms prior to starting therapy. Initiation of a DMT resulted in a marked decrease in NfL for both groups: 47.7% in HEET compared to 33.7% in LEET (Figure 2). Although patients on HEET had lower mean NfL levels at follow-up (7.74 vs. 10.20 pg/mL), the between-group difference was not statistically significant. Mean pre-treatment GFAP levels were similar between HEET and LEET patients (Table 4). Both groups saw a minimal reduction in GFAP (3.0% and 6.3%, respectively). There was no significant difference between the treatment arms.
Neurofilament light chain levels by cohort.
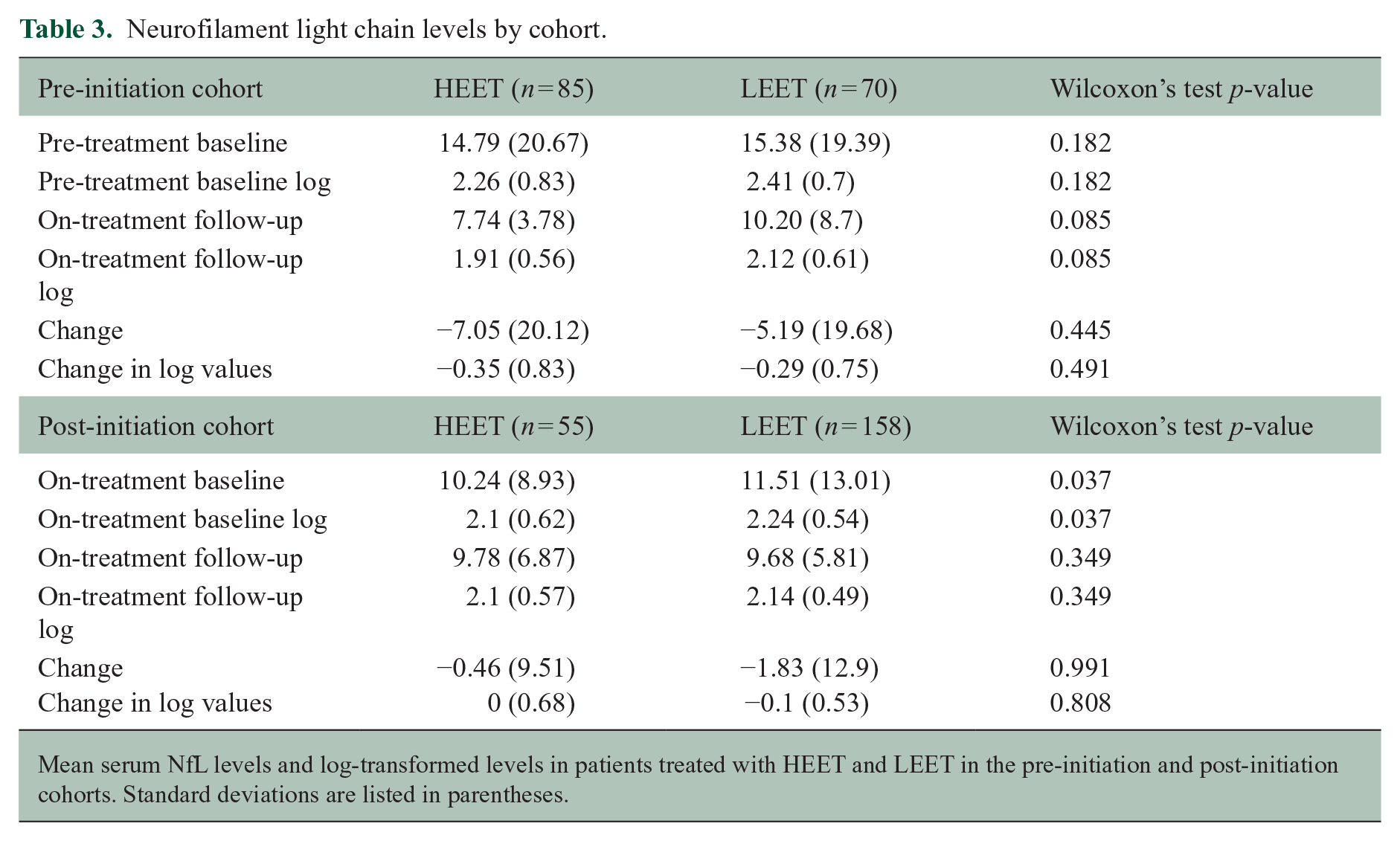
Mean serum NfL levels and log-transformed levels in patients treated with HEET and LEET in the pre-initiation and post-initiation cohorts. Standard deviations are listed in parentheses.
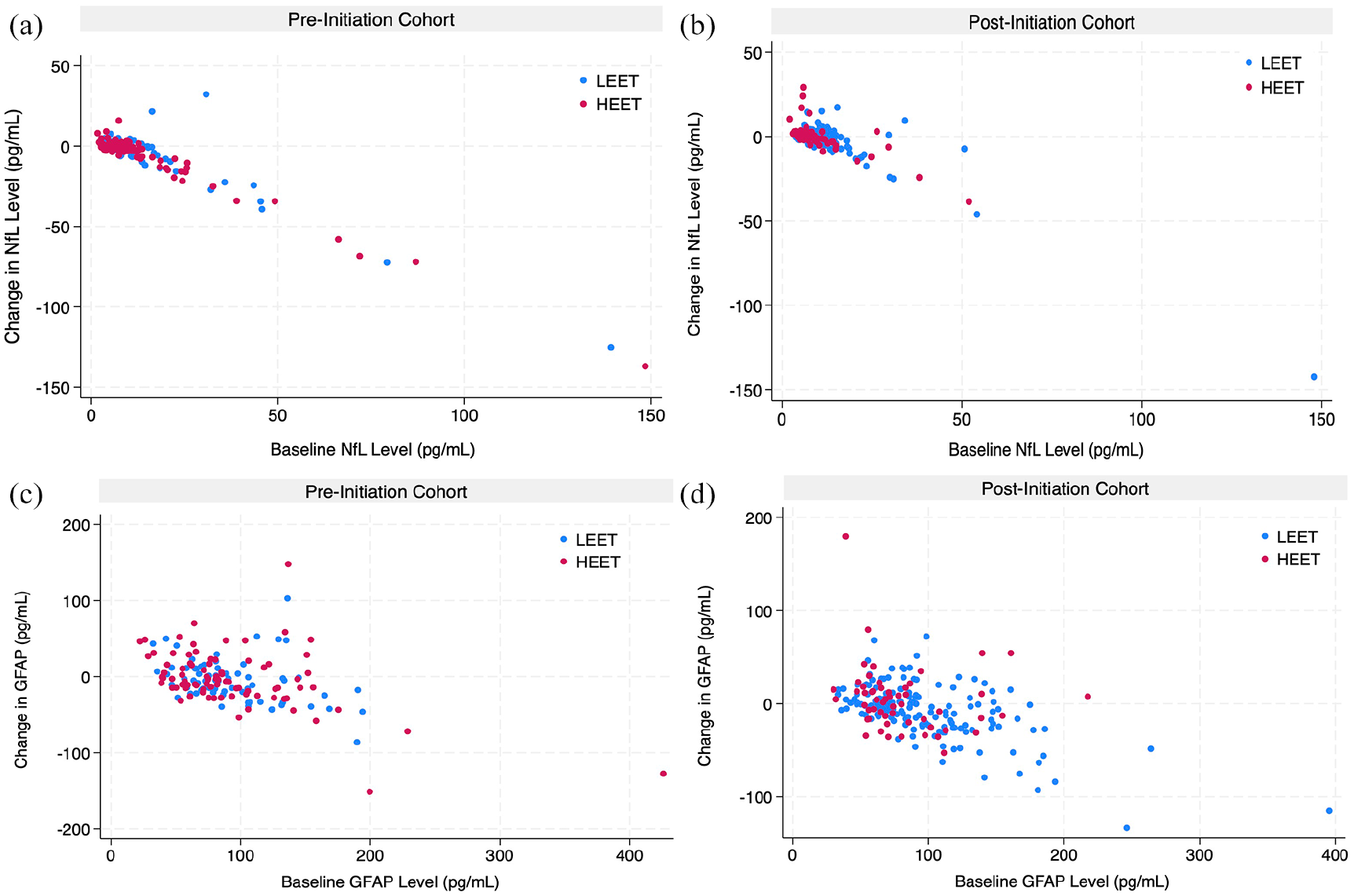
Change in biomarker levels in HEET and LEET patients. Scatter plots of the change in serum NfL levels over the study period graphed against baseline NfL levels in the pre-initiation cohort (a) and the post-initiation cohort (b). The change in serum GFAP levels plotted against baseline GFAP levels is also shown for the pre-initiation cohort (c) and the post-initiation cohort (d).
Glial fibrillary acidic protein levels by cohort.
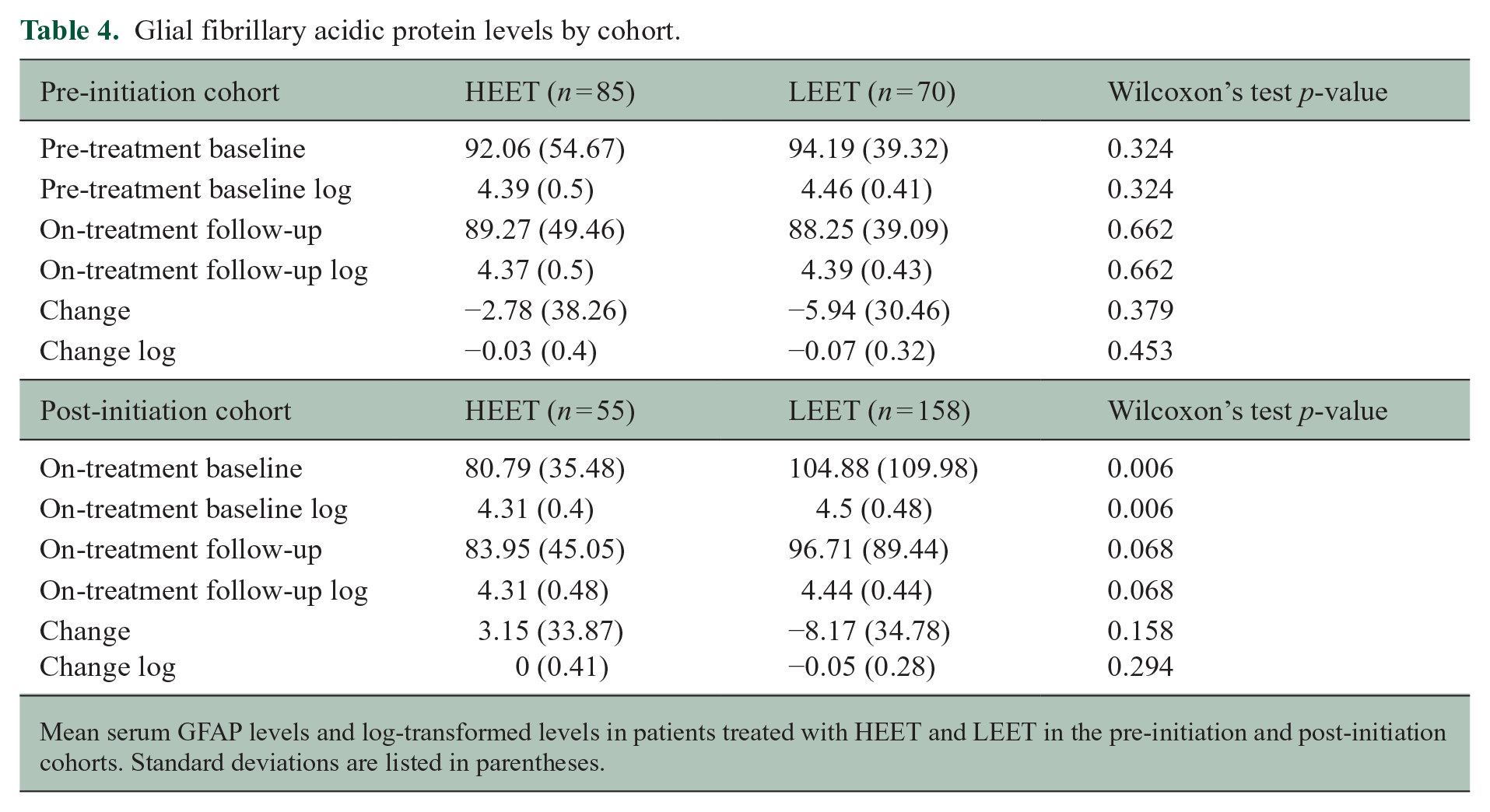
Mean serum GFAP levels and log-transformed levels in patients treated with HEET and LEET in the pre-initiation and post-initiation cohorts. Standard deviations are listed in parentheses.
Reduction in NfL longitudinally while on treatment is modest
In the post-initiation cohort, the baseline on-treatment NfL level was marginally higher in LEET compared to HEET patients (11.51 vs. 10.24 pg/mL). Over a mean of 2.54 years between samples from HEET patients, NfL decreased by an average of 4.5%. LEET patients experienced an average decrease of 15.9% over a mean of 2.70 years. This difference was not statistically significant, and follow-up NfL levels between the post-initiation HEET and LEET patients were almost identical.
Change in GFAP longitudinally while on treatment is mixed
In the post-initiation cohort, the first available GFAP level (mean 0.81 years after treatment start for HEET, 1.24 years after treatment start for LEET) was higher in LEET patients compared to HEET (104.88 vs. 80.79 pg/mL). In contrast to the pre-initiation cohort, the difference between HEET and LEET patients at baseline was significant (p = 0.006). GFAP increased slightly (3.9%) over the study period among the HEET patients, while there was a reduction in GFAP among LEET patients (7.8%); the change between groups was not statistically significant. GFAP remained numerically higher among LEET patients at longitudinal follow-up.
Pre-treatment NfL and GFAP levels are not associated with future relapses or progression in either HEET or LEET
Among both HEET and LEET patients, log-transformed pre-treatment serum NfL levels were not associated with future relapse, subsequent new T2 or enhancing lesions, or with sustained disability progression (Table 5). Similarly, serum GFAP prior to DMT initiation was not associated with any outcome in either arm. The interaction terms were not significant, suggesting that the predictive value of the biomarkers for future outcomes was not fundamentally different in patients treated with HEET or LEET.
Association of pre-treatment biomarker levels and clinical outcomes.
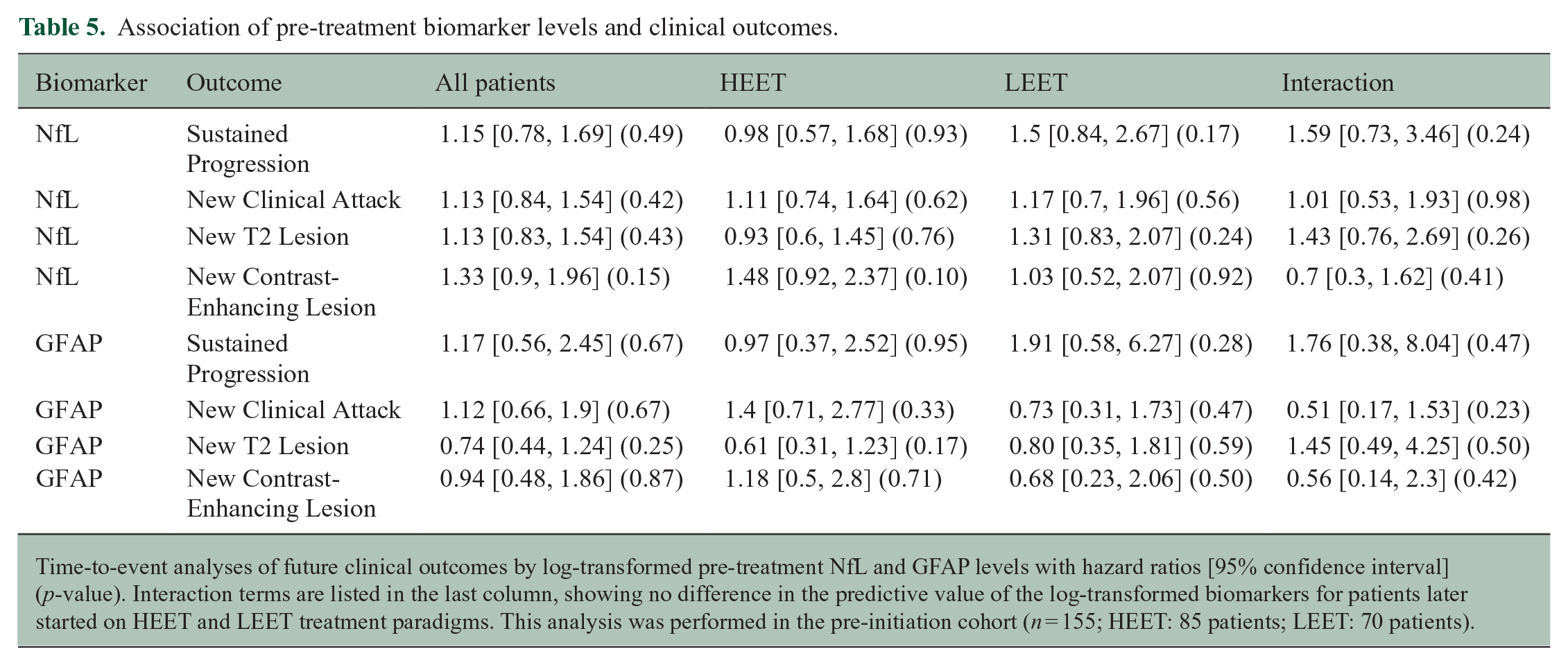
Time-to-event analyses of future clinical outcomes by log-transformed pre-treatment NfL and GFAP levels with hazard ratios [95% confidence interval] (p-value). Interaction terms are listed in the last column, showing no difference in the predictive value of the log-transformed biomarkers for patients later started on HEET and LEET treatment paradigms. This analysis was performed in the pre-initiation cohort (n = 155; HEET: 85 patients; LEET: 70 patients).
Change in NfL and GFAP levels did not differ by DMT class
We evaluated biomarker levels by individual DMT class to determine if significant heterogeneity exists within the HEET or LEET paradigms (Supplemental Materials: Table A). There was no significant difference in median NfL levels at follow-up in the post-initiation group, but follow-up GFAP levels did differ by DMT class (Kruskal–Wallis six-group comparison p-value: 0.413 and 0.023, respectively). In the pre-initiation cohort, median NfL and GFAP levels differed by DMT at follow-up (Kruskal–Wallis six-group comparison p-value: 0.047 and 0.046, respectively), although these results were borderline for an alpha level of 0.05. Nevertheless, there was no difference in the change in NfL or GFAP between baseline and follow-up samples for either cohort, potentially reflecting the non-randomized nature of DMT selection (Figures 3 and 4).

Change in NfL levels by treatment class. Box plots of the change in serum NfL level (pg/mL) between the first and second samples by DMT class in the pre-initiation cohort (a) and post-initiation cohort (b).
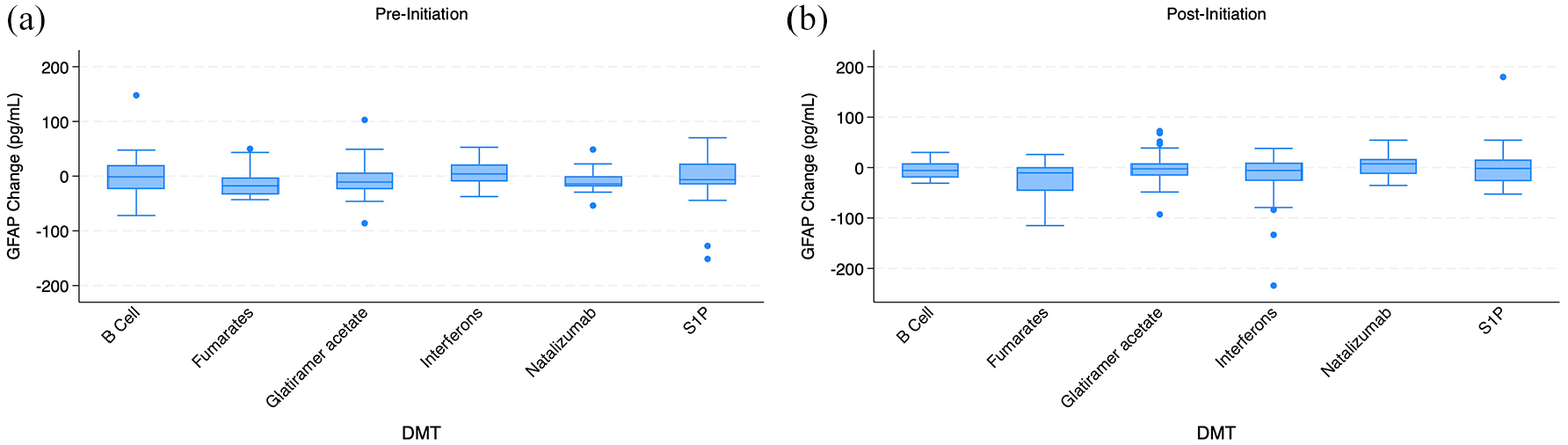
Change in GFAP levels by treatment class. Box plots of the change in serum GFAP level (pg/mL) between the first and second samples by DMT class in the pre-initiation cohort (a) and post-initiation cohort (b).
Conclusion
In this study, we describe changes in serum NfL and GFAP levels with DMT initiation and longitudinally while on treatment in real-world cohorts of early MS patients. We show that NfL is reduced with both HEET and LEET when starting a DMT, while GFAP is not substantially affected. There was a trend to greater reduction in NfL among HEET compared to LEET patients (mean change: −7.05 vs. −5.19 pg/mL), along with lower levels of NfL at follow-up (7.74 vs. 10.20 pg/mL), but the differences between the treatment paradigms were not statistically significant.
Previous studies have shown a greater reduction in NfL with natalizumab, fingolimod and B-cell therapy compared to platform therapies.17–20 While our results were directionally similar, they did not reach statistical significance, likely in part due to substantial individual variability. The specific DMTs used in our HEET and LEET cohorts may also have played a role. We did not see a significant difference in the change in NfL over time by specific DMT class, but the sample size for this subgroup analysis was small. It may be that differences become apparent with larger or randomized samples, and that NfL is reduced in proportion to DMT efficacy. The number of patients on fingolimod and dimethyl fumarate in our study may have attenuated some of the difference between high- and lower-efficacy therapies that was apparent in prior studies comparing infusion to platform therapies.19,20 In addition, many previous studies evaluated NfL in cerebrospinal fluid, where there may be a more pronounced response to treatment. 22
Unlike NfL, GFAP was not significantly impacted by DMT initiation with either HEET or LEET in our study. Both arms of the pre-initiation cohort had a minimal reduction in GFAP over the study period. Despite a minimal GFAP increase in post-initiation HEET patients and a small decrease in the post-initiation LEET patients, the change between groups was not statistically significant. Notably, baseline GFAP levels were lower in HEET and higher in LEET when compared to the pre-initiation cohort (despite similar demographics), and there was again substantial variability between patients. Overall, the relative changes in GFAP levels were small compared to what was seen with NfL. This is consistent with prior studies showing that GFAP is not clearly affected by DMT in MS, although new work has shown that there may be some change in GFAP z-scores with specific treatments like S1P receptor modulators.11,13,23 As GFAP is associated with progressive disease, MRI lesion burden, and other markers of disease severity, it seems likely that GFAP levels would be impacted by DMT when measured over many years.1,10,12,24,25 However, there does not appear to be any notable impact over at least several years of follow-up in our sample.
We found no association between pre-treatment biomarker levels and future clinical and radiological markers of disease activity. This is consistent with recent work showing that treatment with ocrelizumab abrogates the predictive value of pre-treatment NfL for future disease activity. 20 GFAP is known to be associated with sustained disease progression, but it is unclear whether DMT initiation also abrogates the predictiveness of pre-treatment GFAP levels or whether the duration of follow-up in our study was too short to see a difference in outcomes.7,9,26
Several limitations should be considered when interpreting these results. In particular, DMT choice was not randomized and reflects clinician and patient decision-making. It is likely that patients on LEET generally had less active disease or were otherwise judged to be low risk. We relied on the report of the treating neurologist to determine DMT use and were unable to directly assess treatment adherence, which is a potential limitation. We were also unable to ascertain certain measures of disease activity (e.g. contrast-enhancing lesions on MRI) throughout the study period. However, there was no difference in the low rates of recent corticosteroid use between HEET and LEET patients prior to baseline and follow-up samples. Although there were not marked differences in patient age by DMT class, we did not adjust NfL or GFAP levels for age or body mass index. The lack of normative data for GFAP measured by the assay used in this study precluded conversion to z-scores, which help standardize comparisons across age and sex. The time interval between baseline and follow-up samples did vary between patients in the same cohort. While the average difference in treatment duration at baseline and follow-up samples was small and is unlikely to affect our results given the dynamics of NfL and GFAP, the variability in subsets of patients may be meaningful. For example, 19.6% of post-initiation HEET patients had biomarker levels drawn within 3 months of treatment start, compared to 7.0% of LEET patients. Therefore, a larger percentage of HEET patients may not have reached a steady state at the baseline sample. While our study offers a relatively large sample size, the heterogeneity of the follow-up intervals may mitigate the impact of treatment, particularly for the post-initiation cohort. Of note, NfL and GFAP levels vary based on the assay kit (in our case, the Quanterix Neurology 4-PLEX A), which can limit direct comparisons of unadjusted biomarker levels across studies with different methodologies.
A strength of this study, beyond the large sample size, is the real-world comparison of different treatment paradigms in MS patients early in the disease course. Evaluating biomarkers such as NfL and GFAP is of particular relevance because levels may change in advance of clinical outcomes like EDSS, relapse and ability to walk independently.9,15,26 Biomarkers can be used to risk stratify patients and identify subtle disease activity and may therefore be helpful in guiding early treatment decisions given that most disability occurs from progression independent of relapse activity, which can take years to become clinically apparent.4,20,27 Our results suggest that the difference in NfL levels between non-randomized patients treated with HEET and LEET paradigms may be smaller than anticipated, perhaps reflecting the spectrum of DMT efficacy and that the risk of disease activity is a factor in DMT selection. However, this is not to say that small differences in NfL compounded over years are not clinically meaningful. Further research on the association of post-treatment biomarker levels with MS disease outcomes and the long-term effects of various DMTs on GFAP levels is needed. This work broadly supports and extends prior literature describing the minimal impact of DMT on GFAP, at least over the short-to-medium term. In contrast to GFAP, our results highlight similar, notable reductions in NfL levels with both HEET and LEET in a real-world cohort of DMT-naïve, early MS patients and further small reductions in mean levels among those who had recently started on treatment.
Supplemental Material
sj-docx-1-msj-10.1177_13524585251335521 – Supplemental material for Change in serum neurofilament light chain and glial fibrillary acidic protein levels with high-efficacy and low-efficacy early therapy in multiple sclerosis
Supplemental material, sj-docx-1-msj-10.1177_13524585251335521 for Change in serum neurofilament light chain and glial fibrillary acidic protein levels with high-efficacy and low-efficacy early therapy in multiple sclerosis by Evan Madill, Vanessa Moreira Ferreira, Brian Healy, Jonathan Zurawski, Mariann Polgar-Turcsanyi, Howard L Weiner and Tanuja Chitnis in Multiple Sclerosis Journal
Footnotes
Data Availability Statement
De-identified data described in this article will be made available upon reasonable request to the corresponding author (subject to IRB review)
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: TC has consulted and received research support (unrelated to this study) from Octave Bioscience, Inc., which makes a biomarker panel test for multiple sclerosis. The other authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was supported by a grant from Novartis (to T.C.).
Ethical Considerations and Consent to Participate
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Mass General Brigham Institutional Review Board (#2024P000226) on 22 March 2024, with the need for individual written informed consent waived.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.