
Abstract
Violence is a global health concern with profound physical, psychological and social consequences. People with multiple sclerosis (MS) may experience sustained risk due to the intersection of chronic illness, disability, gendered dynamics and structural inequality. MS-specific evidence remains limited and methodologically heterogeneous, precluding reliable conclusions regarding prevalence, outcomes or health system responses. Nonetheless, emerging findings, alongside broader disability literature, indicate that violence is relevant to MS care. This review situates MS within international evidence on disability, chronic illness and violence, synthesises what is known from MS focused literature and highlights key knowledge gaps. It translates the combined evidence to neurology by examining how services can recognise and respond to lived experience. Trauma-informed approaches, case-finding and sensitive inquiry, together with related global frameworks, are discussed as evidence-based models that could be adapted for MS care. People with MS who are victim-survivors remain underserved in research and health-system responses. Violence is pervasive across disability populations, and consistent signals in MS make the issue relevant to neurology. Building an evidence base is essential to establish prevalence, examine longitudinal outcomes and evaluate how recognition and response can be safely integrated and adapted for MS care.
Keywords
Introduction
Violence is a global public health issue with significant physical, psychological and social impacts. The World Health Organization (WHO) defines it as the intentional use of physical force or power, threatened or actual, against oneself, another person or against a group or community, that either results in or has a high likelihood of resulting in injury, death, psychological harm, maldevelopment or deprivation. 1 Throughout this review, we use the WHO definition of violence, noting that ‘abuse’ is used interchangeably across health, legal and policy contexts.1,2
Although violence occurs across all cultures, ages and socioeconomic groups, its distribution and impact are shaped by structural inequality and power imbalance.3,4 It is most often perpetrated by men against women, reflecting entrenched gender norms.3,4 Women with disability experience violence at roughly twice the rate of non-disabled women.4,5 Men and gender-diverse people with disability are also affected, although population-level data remain limited.6,7
There is growing recognition of violence within intimate and family relationships. Intimate partner violence (IPV) encompasses physical, sexual and psychological harm, controlling behaviours, reproductive coercion, technology-facilitated violence and financial violence. 4 It sits within the broader category of family and domestic violence (FDV), which includes violence and coercion within family, household or family-like relationships, including by paid or unpaid carers.8,9 Related forms include gender-based and sexual violence, interpersonal violence and disability-specific violence and neglect. 3 These categories often overlap throughout the life course and across settings, contributing to cumulative exposure and compounding harm.1,3
People living with disability are not inherently vulnerable or in need of protection. Labelling them as such reinforces power imbalances and obscures perpetrator responsibility. 10 Higher recorded rates of violence reflect deliberate targeting, enabled by entrenched discrimination, marginalisation, ableism, paternalism, systemic inequality and structural power imbalances.10,11 When caring and family roles coincide, perpetrators may exploit role shifts to manipulate power and restrict autonomy. 11 The ‘halo effect’ can idealise caregivers, making violence harder to recognise. 11 Carer stress and burnout may contribute to harm, but framing such situations as ‘two-sided’ risks inviting sympathy for perpetrators, minimising harm and shifting blame to the victim.11,12
Multiple sclerosis has a female predominance, onset during the reproductive years and progression to multidomain disability. This places people with MS in a landscape of prolonged exposure to contexts where the risk of violence is higher.5,10,13,14 Physical dependence, socioeconomic disadvantage, financial reliance, communication barriers, isolation and cognitive change can limit independence and make it harder to leave unsafe situations.5,6,15 Invisible symptoms such as fatigue, cognitive impairment, neuropathic pain and reduced endurance create a mismatch between outward appearance and the realities of disability. 16 This can reduce recognition of disability, reinforce expectations of normative functioning and deepen marginalisation. 16
Victim-survivors living with MS represent an underserved population in healthcare and research. Evidence on prevalence, health impacts and clinical responses to victim-survivorship remains limited. However, the longitudinal and multidisciplinary nature of MS care offers repeated opportunities to recognise and respond to violence. In this narrative review, we synthesise MS-specific findings, place them within international evidence on disability and chronic illness, identify knowledge gaps and outline evidence-informed directions for recognition and response in MS services.
Methods
This narrative review draws on a targeted search of peer-reviewed literature in PubMed and Google Scholar (August 2023 to July 2025), alongside grey literature from WHO and government sources. MS-specific studies on violence prevalence and clinical implications were identified using combinations of ‘multiple sclerosis’, ‘interpersonal violence’, ‘intimate partner violence’, ‘family violence’, ‘sexual violence’, ‘trauma-informed care’, ‘screening’, ‘healthcare response’, ‘disability’, ‘disability violence’ and ‘chronic illness’. Most MS studies identified were prevalence-focused and have already been synthesised in recent reviews.10,15,17
Given the limited scope of MS-specific evidence, the search was extended to interdisciplinary literature on chronic illness, disability care and general healthcare. Recent systematic reviews, meta-analyses and other methodologically rigorous studies were prioritised; alongside grey literature focused on evidence-based recognition and response frameworks. Only English-language publications were included. Synthesis and recommendations were developed in collaboration with people with MS who have lived experience of violence, alongside clinicians, researchers and policy specialists, to maximise applicability across neurology, in line with the review’s aim to identify evidence-informed directions for MS care and research.
Violence in MS: what do we know?
Although empirical research remains limited, two recent reviews outline the current evidence base. Freedman et al. 15 provided a reflective overview of how IPV may intersect with MS, emphasising the absence of clinical recognition and offering practical considerations for response. In contrast, the 2025 scoping review by Mallahzadeh et al. 17 systematically assessed seven studies (n = 1991) and reported consistently low methodological quality, with evidence graded between OCEBM levels 2c and 4.
Prevalence: how common is violence in MS?
Current evidence is insufficient to determine whether people with MS experience higher rates of violence than the general population. While several studies report frequent experiences of violence, estimates are self-reported, lack controls, have limited confounder adjustment and are mostly cross-sectional. 17 These features constrain interpretation and preclude inference about relative risk.
The only published analysis to directly compare prevalence between women with and without MS is a large Norwegian population-based study of pregnant women. 18 This study included 106 women with MS and 77,278 matched controls and adjusted for potential confounders. Women with MS had higher odds of adult rape (adjusted odds ratio (aOR) = 2.37, 95% confidence interval (CI) = 1.02–5.49), emotional violence (aOR = 1.75, 95% CI = 1.08–2.83) and revictimisation (aOR = 2.23, 95% CI = 1.22–4.10). 18 Although limited to pregnancy and with few MS cases reporting adult violence (n = 27), its population-based design and adjustment strengthen its value for hypothesis generation. Replication in larger and more diverse cohorts across the disease course and settings is warranted. Given frequent non-disclosure and ethical, clinical and methodological barriers, published estimates are likely conservative. 19
Patterns: who are the perpetrators and what forms are reported?
The scoping review 17 summarised findings from individual studies documenting experiences of violence among people with MS. Reported ranges included 11% to 34% for physical violence,12,18,20 44% to 53% for psychological or emotional violence,12,20 25% to 63% for financial or economic violence,12,20 8% to 20% for sexual violence,12,18,20 21% to 35% for emotional or verbal violence,18,21 17% for neglect 12 and 20% to 36% for combined physical and/or sexual violence. 21 One study found that 84% of disclosures involved repeated episodes. 21 These figures reflect study samples and measurement instruments and should not be interpreted as population prevalence, but they do highlight the frequent, multiform nature of violence reported in MS.
Perpetrators reported across the literature include intimate partners, family members, caregivers and employers. 17 Because most studies focused on a single perpetrator type or context, overlapping patterns are likely underestimated.
Reported associations: have risk factors for violence in MS been identified?
Key MS context (phenotype, duration, disability, relapse severity, treatment response) is rarely detailed in studies of violence in MS, limiting interpretation. 17 Within available data, lived experience of violence has been associated with higher care needs, cognitive impairment, lower income and education, alcohol use (by the person with MS or their caregiver) and being married/cohabiting.12,15,17,22 –24 Protective associations included older age and strong social networks.12,15,21 –24 One study found that those without a violence history had lower fatigue and fewer neuropsychological symptoms. 25 These observations are provisional signals rather than MS-specific risk factors; causal direction is uncertain, and current data do not support risk stratification.
What we don’t know
Evidence on how violence influences MS outcomes remains limited. Available datasets are small, heterogeneous and largely cross-sectional, with minimal stratification by gender, disability or sociocultural context, limiting interpretation of directionality and temporal sequence. 17
Gender and sociocultural variation: do gender and context change the picture?
The existing evidence base is concentrated in high-income settings (United States four studies, Sweden one, Norway one, Iran one), which limits generalisability. 17 Women comprised approximately 79% of participants, leaving gender-diverse people and men largely excluded and limiting analysis of gendered experiences. 17
Impact on MS: how might lived experience influence outcomes?
The relationship between violence and MS morbidity is not established. In a small Swedish cohort (n = 47, relapse-onset MS), a history of violence exposure was associated with elevated cerebrospinal fluid (CSF) interleukin (IL)-6 (ρ = 0.35, p < 0.05), with higher levels among those with comorbid depression (ρ = 0.39, p < 0.05). 25 The association did not persist after accounting for depression and was not seen among people receiving disease-modifying therapies (DMTs), 25 suggesting potential links between trauma, mood and neuroinflammatory processes. No studies have looked at the impact of trauma on relapse activity, disability progression or disease course.
Temporal and bidirectional dynamics: how do violence and MS interact over time?
Existing studies are mostly cross-sectional or short-term; therefore, temporal ordering cannot be established. 17 Violence may precede, coincide with or follow multiple sclerosis onset, and repeated victimisation is recognised. 21 We hypothesise a bidirectional compounding cycle, in which trauma, stress, comorbidity and disrupted care may worsen MS outcomes, while worsening outcomes increase exposure to coercion and control (Figure 1). This remains untested in longitudinal research.
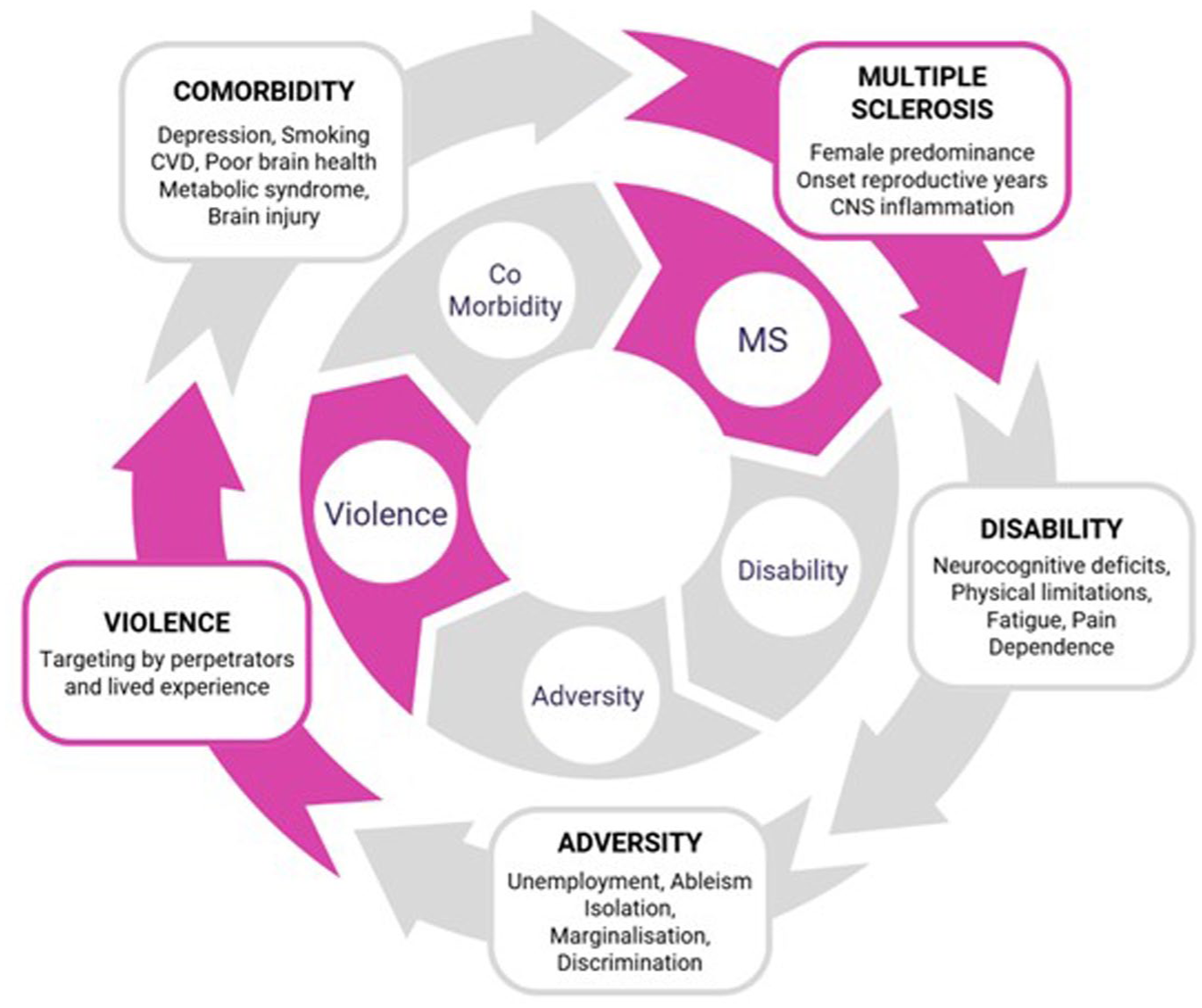
A hypothesised bidirectional, compounding cycle between multiple sclerosis and lived experience of violence.
Emerging conceptual pathways
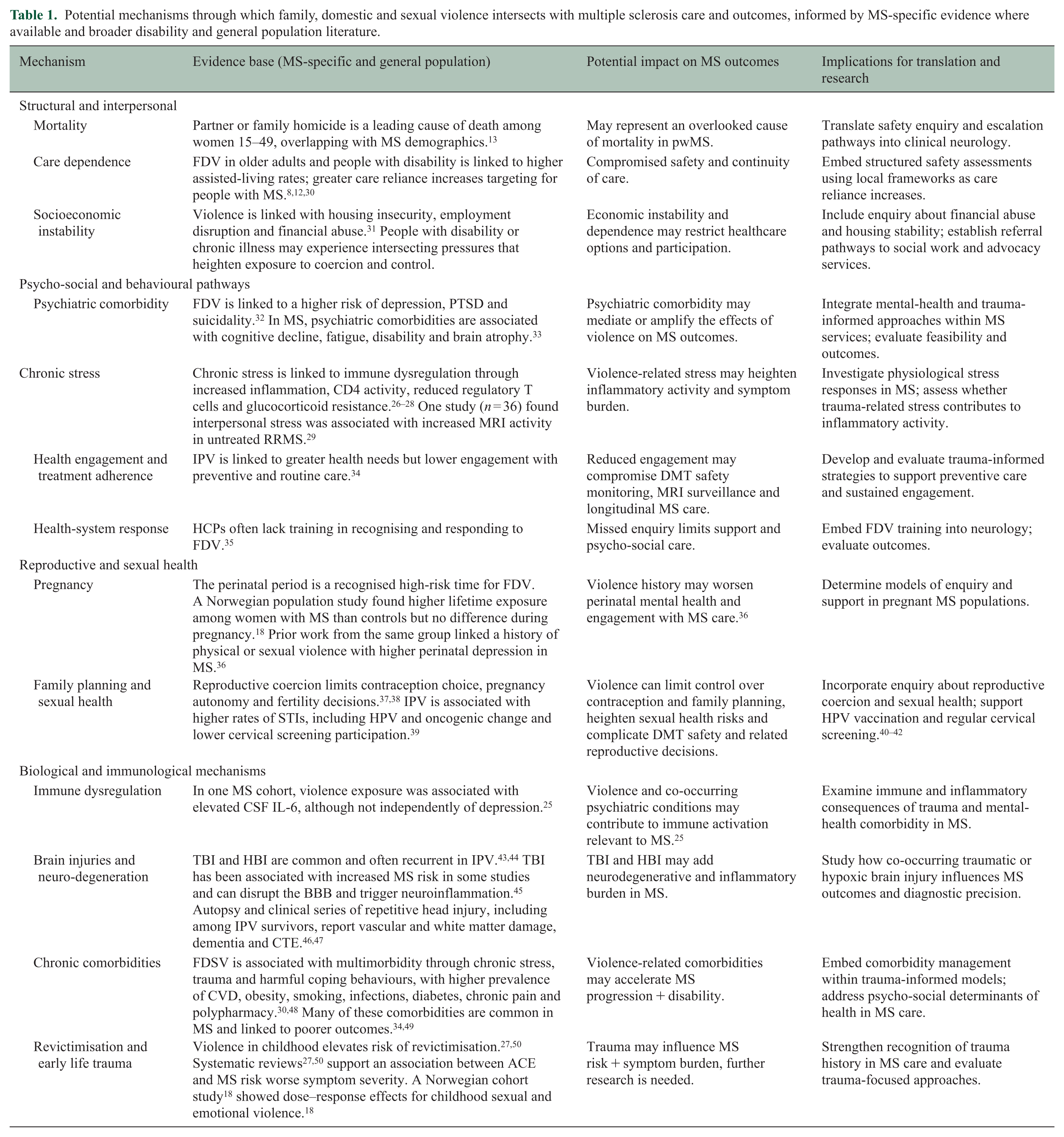
Findings from population and disability research, together with broader MS evidence, suggest potential mechanisms linking family, domestic and sexual violence (FDSV) and MS outcomes (Table 1). These include stress-responsive immune and neuroendocrine changes, psychiatric comorbidity, behavioural and cardiometabolic factors, injury and reduced participation in preventive or ongoing care. Although not yet examined within MS cohorts, these mechanisms warrant systematic investigation and are key considerations for the development of trauma-informed neurology.
Potential mechanisms through which family, domestic and sexual violence intersects with multiple sclerosis care and outcomes, informed by MS-specific evidence where available and broader disability and general population literature.
Screening, detection and documentation in practice: what should be built and tested?
Most studies have used disability-focused violence tools, standard IPV instruments or researcher-designed measures, but rarely in combination. 17 Given the multiple forms of violence and perpetrator roles across the life course in MS, single-tool approaches may miss the full scope of lived experience. The lack of robust, tested tools likely contributes to low identification and poor integration into care.
In a US study of 200 women with MS, 38% disclosed violence in research surveys, yet none had this recorded in their retrospective clinical records. 21 Whether this reflects non-identification, non-documentation or both is unclear, but it highlights the absence of standardised, evidence-informed processes in MS care. No studies have evaluated the impact of screening, toolkits or frameworks on clinician behaviour, feasibility, safety or health and MS outcomes. Evidence from other populations highlights both the limitations and ongoing debate about violence screening. 51 In MS care, where feasibility and outcomes have not been tested, a reasonable priority is the integration, evaluation and refinement of evidence-informed frameworks for safe recognition and response.
A call to evidence-based action
Recognition is the first step, but it is not straightforward
Recognition is essential to addressing violence in MS, yet it is complicated by the absence of MS-specific guidance and ongoing debate about screening in healthcare. Many people with lived experience report that being asked in clinical settings is acceptable when privacy and trust are ensured, but the approach and the evidence remain contested. 52
The 2025 US Preventive Services Task Force (USPSTF) 51 systematically reviewed screening for IPV and for caregiver violence or neglect in older adults and in adults who rely on others for care. These categories may apply to people with MS at different times across the disease course. For IPV, the Task Force reaffirmed a Grade B recommendation to screen all women of reproductive age, including those who are pregnant or postpartum, and to refer positive screens to multicomponent, ongoing supportive interventions. 51 Benefits are strongest in perinatal studies, where multi-session programmes reduced recurrence.51,53 –56 Outside perinatal care, screening increases identification, but trials have not consistently improved mental or physical health, quality of life or safety outcomes. 51 Trials have not shown serious harms from IPV screening or brief first-line support; evidence on screening harms in caregiver violence is limited.51,57,58 The Task Force therefore concluded that evidence is insufficient to assess the balance of benefits and harms in caregiver violence and neglect screening. 51
Given these uncertainties, many health systems emphasise targeted case-finding or sensitive inquiry outside perinatal care. This involves trauma-informed questioning when signs, risk indicators or contextual concerns are present, often repeated over time, recognising that disclosure may depend on both trust and being asked on more than one occasion.59 –61 This approach is embedded in frameworks such as NICE (United Kingdom), 62 VEGA (Canada), 59 MARAM (Victoria, Australia) 60 and the New Zealand Ministry of Health guidelines. 63 Common indicators include repeated injuries, chronic pain, sleep disturbance, depression, anxiety, missed appointments, medication interruption and escalating caregiver control.59,60,62 Many overlap with MS symptoms, creating a risk of misattribution without disclosure. Research is needed to determine whether MS-specific indicators add value beyond population-level indicators and how they can support safe case-finding.
Frameworks for response
Evidence-based response models such as WHO’s LIVES framework (Listening, Inquiring about needs, Validating, Enhancing safety, Support) are associated with better help seeking and engagement when implemented well. 64 Training staff in local evidence-based recognition and response frameworks and establishing warm referral pathways, involving active and supportive handover to specialist services, are pragmatic and feasible first steps.
Healthcare response and trauma-informed care
The WHO 2 recommends strengthening health-system responses through survivor-centred care, early identification, first-line support, gender equity in service provision and data collection to monitor and improve practice. Systematic reviews of violence prevention and response interventions for people with disability across primary, secondary and tertiary settings have identified very few high-quality studies, with meta-analysis precluded by heterogeneity.3,65 Most were short term, focused on intellectual disability and a single form of violence, rarely conducted in healthcare settings and did not incorporate patient-reported measures, health-related quality of life or objective health and safety indicators. 65 No studies have evaluated healthcare-based models in neurology.
Within this evidence gap, trauma-informed care is an established theoretical and organisational framework that has been associated with improved engagement and safety across diverse healthcare contexts.66,67 Developed by the U.S. Substance Abuse and Mental Health Services Administration (SAMHSA), the framework draws on extensive trauma research and outlines six core principles: (1) safety, (2) trustworthiness and transparency, (3) peer support, (4) collaboration and mutuality, (5) empowerment, voice and choice and (6) attention to cultural, historical and gender issues.67,68
Trauma-informed care has not been evaluated in MS neurology. Its translation does not represent a treatment shift but an acknowledgement that trauma can influence communication, trust and symptom experience, and that consultation structure, clinician gender and the availability of culturally safe and trauma-focused supports each shape how care is experienced (Figure 2).66 –68
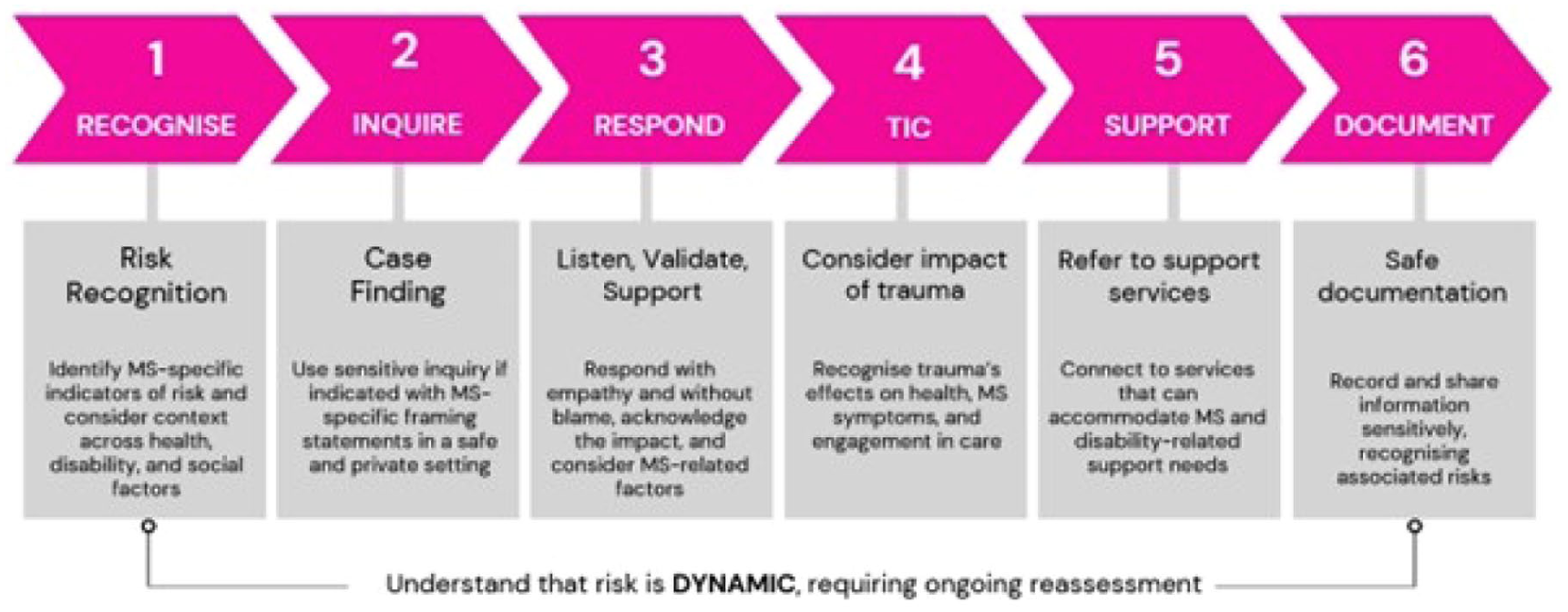
Sensitive inquiry in the context of MS healthcare.
Implementation barriers and emerging MS evidence
Systematic reviews and qualitative syntheses consistently identify barriers to implementing frameworks for recognising and responding to violence in healthcare.69,70 These include limited clinician awareness of referral pathways and available supports, uncertainty regarding professional responsibilities and prevailing beliefs that violence falls outside the scope of healthcare ‘not my job’.69,70 Structural constraints such as excessive workloads, time constraints, emotional demands and limited resources further impede clinical response.68 –70
Emerging evidence indicates that similar barriers are present within neurology. A recent qualitative evaluation of Australian MS clinicians reported that experiences of violence are frequently encountered in practice yet seldom addressed through structured pathways. 71 Participants described limited training, uncertainty around enquiry and reporting, absence of referral pathways and the emotional toll. 71 Complementary data from the United Kingdom, examining the lived experience of women with MS who are victim-survivors of violence, demonstrate that system-level barriers in healthcare can translate into patient-level obstacles to support. 72 Ambiguity regarding the clinician’s role and inconsistent follow-up generated uncertainty about appropriate avenues for assistance and constrained disclosure, whereas clear and sustained clinician engagement was perceived to facilitate both safety and access to care. 72
Addressing these intersecting challenges requires organisational structures that sustain clinician and patient safety through workforce development, clear governance of reporting and referral processes and resourced supports such as supervision, debriefing and wellbeing programmes. 61 The emotional demands of trauma-related work are well documented and are particularly relevant in neurology, where burnout is prevalent.32,73 Healthcare professionals also experience gendered and family violence at higher rates than the general population, meaning some are both providers and victim-survivors. 74 How system-level supports can be developed, implemented and evaluated within neurology remains untested and represents an important direction for future research.
Conclusion: closing the evidence gap
In an environment where health systems are increasingly reshaping their responses to violence, neurology has remained largely absent, despite evidence of high prevalence among people with disability and emerging signals in MS. 17 Victim-survivors with MS remain underserved, with no systematic data on prevalence, no evidence on how violence affects MS outcomes and no evaluation of whether existing frameworks are appropriate for neurological care. Trauma-informed principles may be practised informally, but they have not been studied or tested in neurology, and their influence on health, safety or MS outcomes has not been defined.
MS services, with longitudinal clinician–patient relationships and multidisciplinary models, provide a context in which these questions could be addressed. As the WHO 19 emphasises, safety should precede data. Future work needs to embed this principle while also generating evidence through the establishment of an epidemiological base. Investigation of longitudinal associations of violence with MS outcomes, and evaluation of the feasibility, acceptability and safety of adapting or developing frameworks for neurological care in this population are key unmet needs and critical steps towards informing prevention and response interventions. Equity demands that this work include men, gender-diverse people, culturally diverse groups and services beyond high-income contexts.
Addressing violence is ‘everyone’s job’.60,61 Progress will require participation across research, clinical practice, services and governance, recognising that the potential implications for health, safety and MS outcomes are too important to leave unexamined.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Data availability statement
Data sharing is not applicable to this article, as no data sets were generated or analysed during the current study.