
Abstract
Background:
Event-related potentials (ERPs) are valuable tools for the early detection and monitoring of cognitive impairment in people with Multiple Sclerosis (pwMS) and towards the evaluation of the effectiveness of treatment. The Symbol Digit Modalities Test (SDMT), a screening tool for cognitive dysfunction, is often impaired in pwMS.
Objective:
To explore the ERPs and reaction time (RT) correlates of SDMT as indicators of cognitive impairment in pwMS.
Methods:
We developed an EEG-compatible (EEG-SDMT) paradigm. Ninety-two pwMS and twenty-eight healthy controls (HC) underwent ERPs and RT measurement during EEG-SDMT.
Results:
SDMT-ERPs presented a centro-parietal (Pz electrode) positive peak (P5) with a significantly longer latency in pwMS (611.72 ± 122.30 ms) versus HC (517.29 ± 75.53 ms) (p < 0.01). RTs and raw scores in the standard SDMT were inversely correlated (r = −.722, p < .001).
Conclusion:
Our EEG-SDMT paradigm identified neurophysiological correlates of SDMT performance, which was significantly affected in pwMS. Although the P5 showed longer latencies in pwMS, this component did not differentiate between cognitively impaired and preserved individuals, likely because it is still too early to capture higher-order cognitive deficits. In contrast, RTs emerged as a more reliable and sensitive indicator of cognitive performance.
Introduction
Cognitive impairment is a very common deficit that affects approximately 30% to 70% of people with MS (pwMS), with the highest prevalence observed in progressive forms of the disease. 1 The most commonly affected cognitive domains include information processing speed, complex attention, memory and learning, executive functions, and visuospatial ability. 2 These deficits are highly relevant due to their substantial impact on daily activities, employment, and employability.3,4 Therefore, both early detection and prompt interventions for cognitive impairment are crucial. The Symbol Digit Modalities Test (SDMT) 5 is currently the most widely used screening tool for cognitive dysfunction in MS. The SDMT is classically defined as a measure of processing speed, although it measures also lexical access speed, memory, visual search, and attention. 6 It is highly sensitive to cognitive changes and it is considered an effective test for discriminating between people with MS with or without cognitive impairments. 7 Digital versions of the SDMT have been developed,8 –10 however, none of these tests have been developed to be completed during electroencephalographic (EEG) recordings.
Event-related potentials (ERPs) have been used to assess cognitive decline in MS and have been shown to be in line with data obtained from neuropsychological tests.11 –13 The P300 ERP component has been proposed as a neurophysiological marker of cognitive functioning in MS, 14 due to its ease of recording and reliability. P300 amplitude is related to attention and information processing, while latency is a measure of stimulus classification speed. 15 ERPs have proven to be a cost-effective, reliable, and easily administered tool for investigating cognitive deficits in individuals with MS.16,17 While neuropsychological tests, such as the Brief International Cognitive Assessment for Multiple Sclerosis (BICAMS), 18 are relatively quick to administer, their application can be limited in individuals from diverse cultural backgrounds or those with visuomotor impairments. In contrast, ERPs despite requiring additional time for electrode placement and data acquisition, offer practical advantages in providing an objective and direct measurement of brain activity that does not rely on verbal or motor responses. These advantages include their ability to capture subtle neurophysiological changes that may precede cognitive deficits detectable through standard neuropsychological testing. As a complementary approach, ERPs enable a more holistic evaluation of cognitive functioning in individuals with MS, offering unique insights that can enhance traditional assessments and support clinical decision-making. Considering the advantages of EEG, our primary motivation was to investigate the electrophysiological correlates of cognitive processing engaged by the SDMT in pwMS. We aimed to determine whether EEG-derived markers could provide objective evidence of the cognitive functions measured by the SDMT, thereby offering a neural substrate for its behavioural outcomes. We also sought to improve the sensitivity of cognitive assessment by combining behavioural and electrophysiological measures. With this aim, we developed an EEG-compatible version of the SDMT (EEG-SDMT), designed to minimize movement artefacts. Finally, we evaluated the clinical relevance of EEG-SDMT task by testing its ability to differentiate between cognitively preserved and impaired pwMS and by assessing correlations with performance on the standard paper-based SDMT.
Methods
Participants
Participants were recruited between June 2023 and May 2025 from the inpatient Neurorehabilitation Department at Casa di Cura Igea in Milan, Italy. Eligibility criteria for pwMS included: (1) aged 18-75 years, (2) diagnosis of MS according to the revised McDonald's criteria, 19 (3) no history of major neurological and/or psychiatric disorders, and (4) absence of severe visual or motor impairments that could compromise neuropsychological testing (EDSS ⩽ 7.5). Healthy controls were selected to match pwMS in demographic characteristics and to have no history of neurological or psychiatric disorders. All study procedures followed the principles outlined in the Declaration of Helsinki. Written informed consent was obtained from all participants before their participation in the study, in accordance with the protocols approved by the Institutional Ethics Committee (protocol number: 1162_2022).
Neuropsychological assessment
All participants underwent a neuropsychological evaluation. An experienced neuropsychologist administered the BICAMS, which includes: the oral version of the SDMT, the California Verbal Learning Test-II (CVLT-II), 20 measuring verbal learning and memory, and the Brief Visuospatial Memory Test-Revised (BVMT-R), 21 measuring visuospatial learning and memory. PwMS were classified as cognitively impaired if their performance on at least one of these tests fell 1.5 SD below the mean, based on published normative data for the Italian population. 22
EEG-SDMT task
The EEG-SDMT is depicted in Figure 1(a). A legend with 9 symbols and 9 numbers was constantly displayed at the top of a PC screen. A symbol-digit pair was presented in the centre of the screen for 5 s, or until a motor response, followed by a 2-s inter-stimulus interval. Stimuli were displayed in white on a fully black background to maximize contrast and readability. Symbol-digit pairs were presented in random order, in two different blocks (90 per block). Participants were instructed to judge if the symbol-digit pair presented was correct or incorrect, and to press the left or right arrow key accordingly. The left/right correspondence was randomly assigned to each participant, with on-screen red and green cues serving as response reminders. Instructions were provided by the experimenter and displayed on the screen before the beginning of a training, featuring a shortened version (10 symbol-digit pairs), designed to help participants familiarizing with the task. Before the choice task, participants performed a simple reaction time task (SRT), with the same layout as the EEG-SDMT (Figure 1(b)) to involve the same visuo-motor processes. In the SRT, pressing the left or right arrow key as quickly as possible was required whenever a symbol-digit pair appeared on the screen, regardless of the specific pair presented. Symbol-digit pairs were presented for 2.5 seconds or until a response was given, followed by a 2 ± 1 second inter-stimulus interval (two blocks, 10 stimuli per block). Key-press RTs and number of commission errors were measured. For each participant, cognitive response time (CogRT) was calculated by subtracting the mean of key-press RTs to the SRT from the mean of those obtained during the EEG-SDMT.
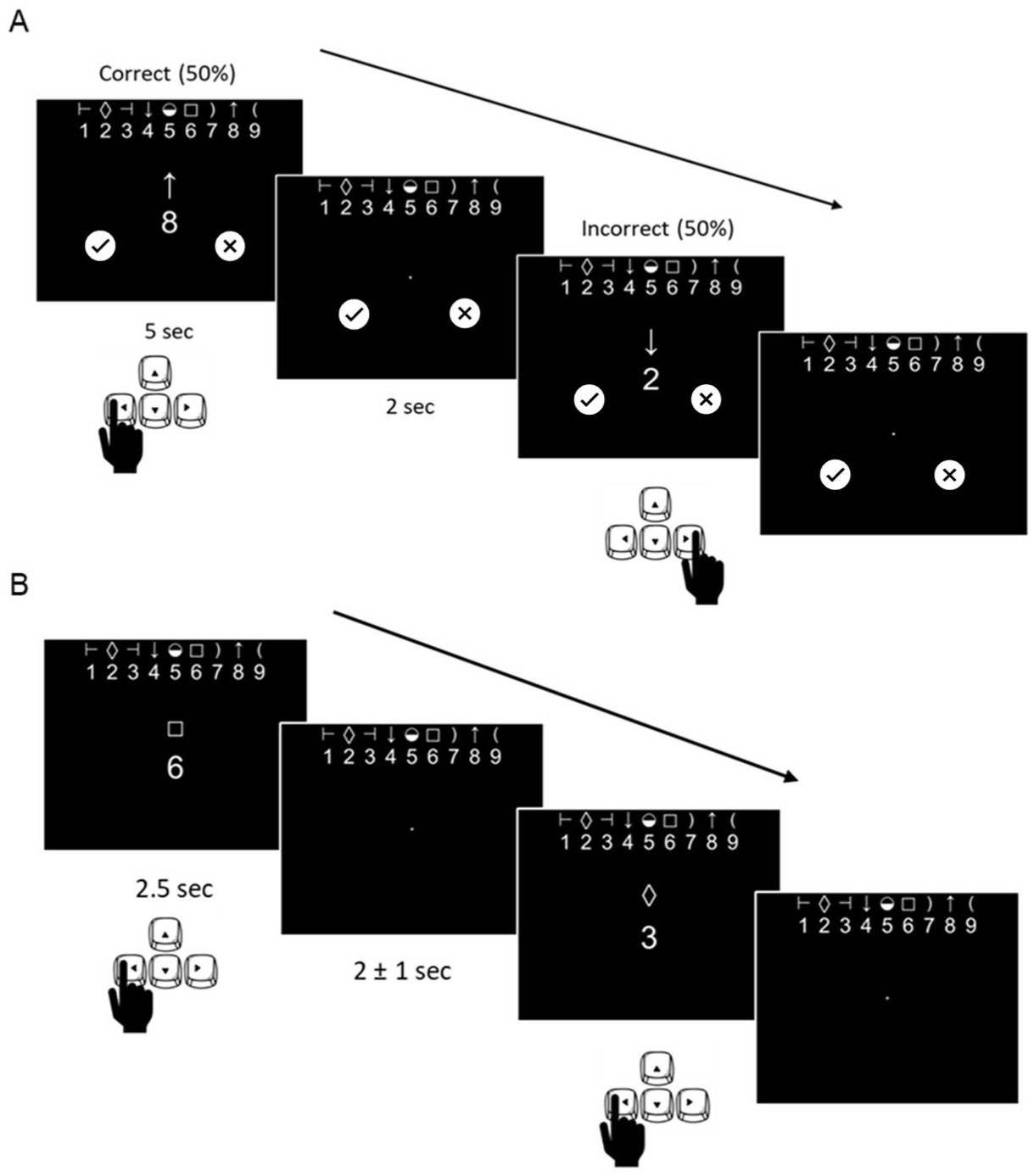
(a) An example of the EEG-SDMT in which a symbol-digit pair is presented at the centre of the screen for 5 sec or until a response is given, with a 2 sec inter-stimulus interval. The participant is asked to judge, by looking at the legend, if the symbol-digit pair is correct (50%) or incorrect (50%) by pressing the left or right arrow key respectively. (b) An example of the SRT task in which a symbol-digit pair is presented at the centre of the screen for 2.5 sec or until a response is given, with a 2 ± 1 sec inter-stimulus interval. The participant is asked to press, as quickly as possible, the left or right arrow key, every time a symbol-digit pair is presented.
Electrophysiology
EEG recordings were carried out with a 32-channel EEG system (actiCHamp Plus, Brain Products GmbH, Gilching, Germany), consisting of 29 scalp electrodes mounted on an elastic cap (ActiCap), organized according to the International 10-20 System. All electrodes were referenced to the linked earlobe channel and offline re-referenced to the opposite earlobe channel. Vertical and horizontal eye movements were recorded through two electrodes situated in the inferior and superior position of the eyes. A sampling rate of 500 Hz was used, and the impedances were kept below 5 kOhms. Raw EEG signal was preprocessed using BrainVision Analyzer software (Version 2.2.0, Brain Products GmbH, Gilching, Germany). EEG traces underwent band-pass filtering (0.1–40 Hz), visual artefact rejection, and eye movement correction. 23 The resulting EEG traces were segmented into 1 second epochs, time-locked to stimulus presentation (−200 to 800 ms, zero being the onset of the stimuli). After baseline correction (from −200 ms to stimulus onset), stimulus-locked averaging was performed for correct response trials (MATLAB Version R2022b). Electrode selection criteria for ERP measurement were guided by existing literature24,25 and the observed timing and ERPs topographic distribution. In particular, centro-parietal sites (e.g. Pz electrode) were considered for cognitive components (e.g. P300), as they best reflected the ERP peak of interest in our dataset, whereas early visual components (P1 and N1) were measured at O1, given the location of the primary visual cortex.
Statistical analyses
Independent samples t-tests were performed to evaluate demographic differences between HCs and pwMS, as well as between pwMS with and without cognitive impairment. We assessed the assumption of normality using the Shapiro–Wilk test. Behavioural data (i.e. key-press RTs, number of errors) from the EEG-SDMT and SRT tasks, as well as CogRT were analysed using the Wilcoxon test, with False Discovery Rate (FDR), performing pairwise comparisons between groups (HC, pwMS with cognitive impairment, pwMS without cognitive impairment). Demographics and behavioural data analyses were carried out in IBM SPSS Statistics (Version 26.0.0.1). ERP data were analysed in MATLAB (Version R2022b). We compared the differences in ERP latency and amplitude between HCs and pwMS using the Wilcoxon test, with False Discovery Rate (FDR) correction. The concurrent validity of the EEG-SDMT and the paper-based SDMT was assessed using Spearman’s rho correlation coefficient. All tests were two-sided, and we set the significance threshold as α = 0.05. To account for a potential confounding effect of age, we run a sensitivity analysis for behavioural data and ERP data, where age was entered as a covariate. We calculated estimated marginal means with standard error (SE) and reported FDR-adjusted p-values for pairwise comparisons, mirroring the procedure used for the main analysis.
Results
Out of 126 pwMS who met the inclusion criteria, 22 declined participation, and 8 were excluded due to logistical challenges (e.g. short hospitalization or unavailable staff for EEG recordings). Out of the 96 pwMS recruited, 2 voluntarily stopped the EEG recording session (one due to discomfort with EEG gel making contact with their hair, the other for urinary urgency) and 2 could not understand the complex EEG-SDMT task.
Demographics and neuropsychological assessment
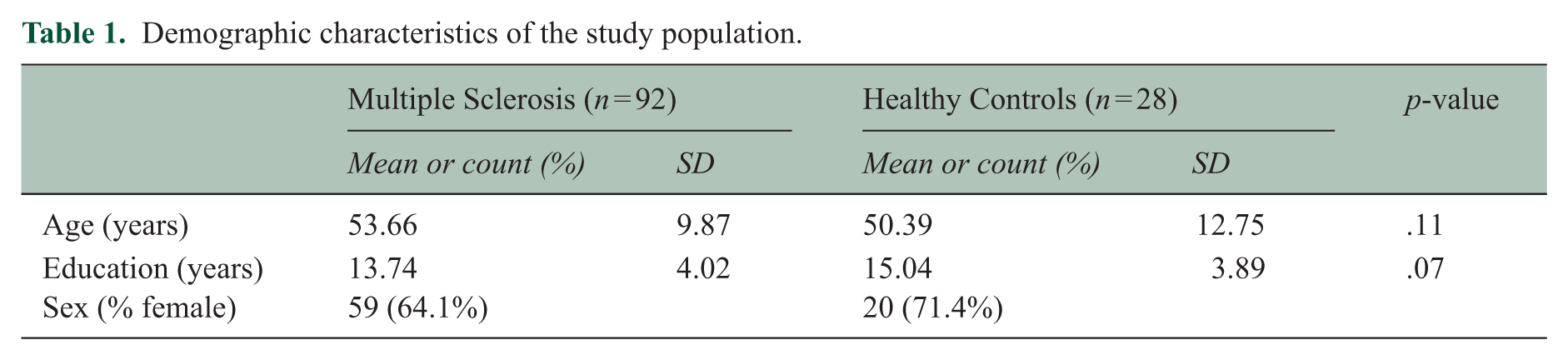
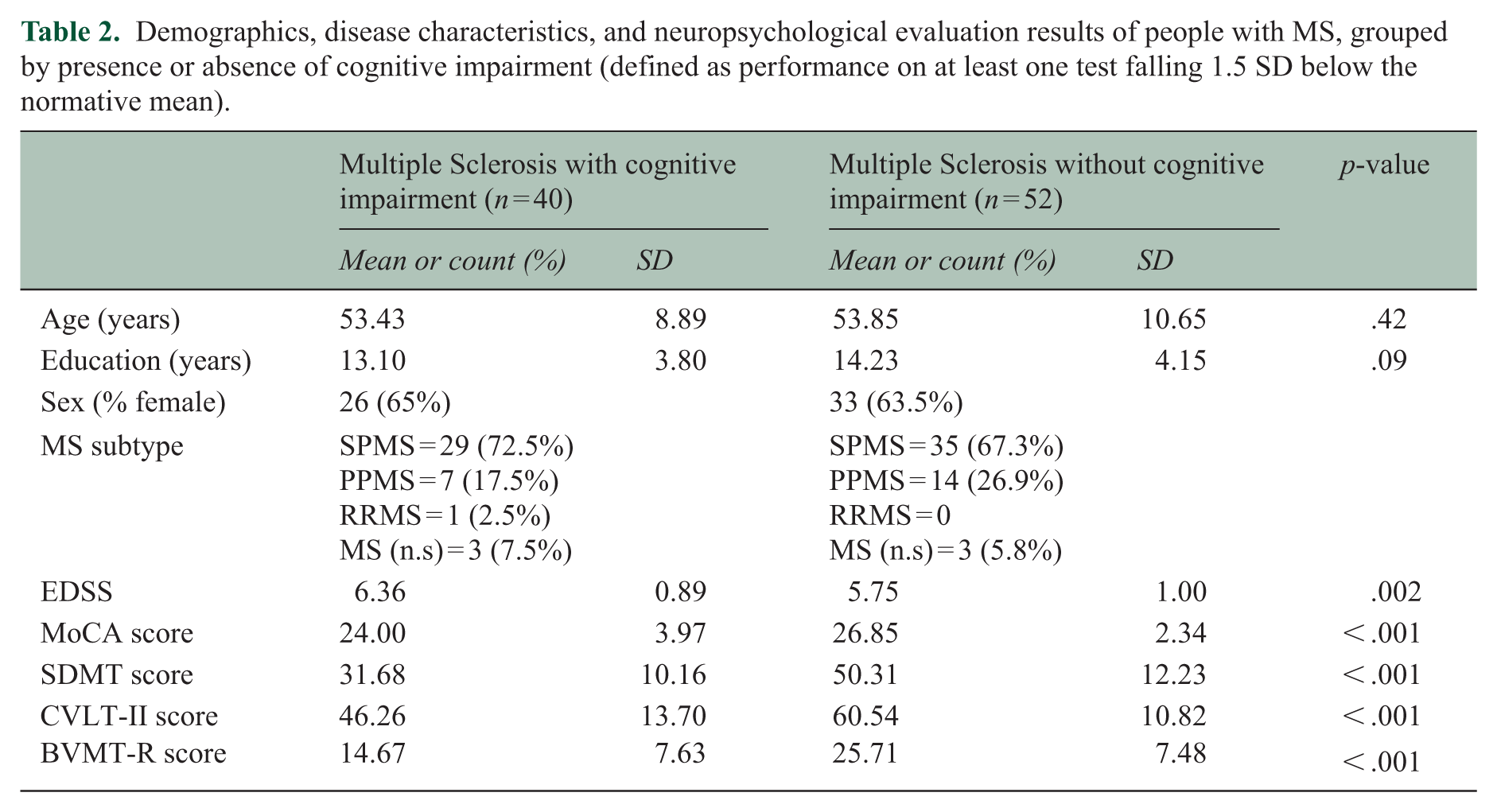
Group demographic variables for pwMS and HCs are presented in Table 1. There was no significant age difference between pwMS and HCs. HCs had more years of education, although this difference was not statistically significant (p = .07). When pwMS were divided into cognitively impaired and non-cognitively impaired groups (Table 2), there were no significant differences in age or years of education. EDSS scores were significantly higher in pwMS with cognitive impairment (p < .01). In addition, BICAMS scores were significantly lower in pwMS with cognitive impairment (all p < .001).
Demographic characteristics of the study population.
Demographics, disease characteristics, and neuropsychological evaluation results of people with MS, grouped by presence or absence of cognitive impairment (defined as performance on at least one test falling 1.5 SD below the normative mean).
Concurrent validity (EEG-SDMT vs paper-based SDMT performance)
Key-press RTs to EEG-SDMT showed a significant negative correlation with paper-based SDMT scores (ρ = −.76, p < .001) (Figure 2(a)). The number of errors committed during the completion of the EEG-SDMT also displayed a significant negative correlation with paper-based SDMT scores, albeit of lesser strength (ρ = −.39, p < .001) (Figure 2(b)).
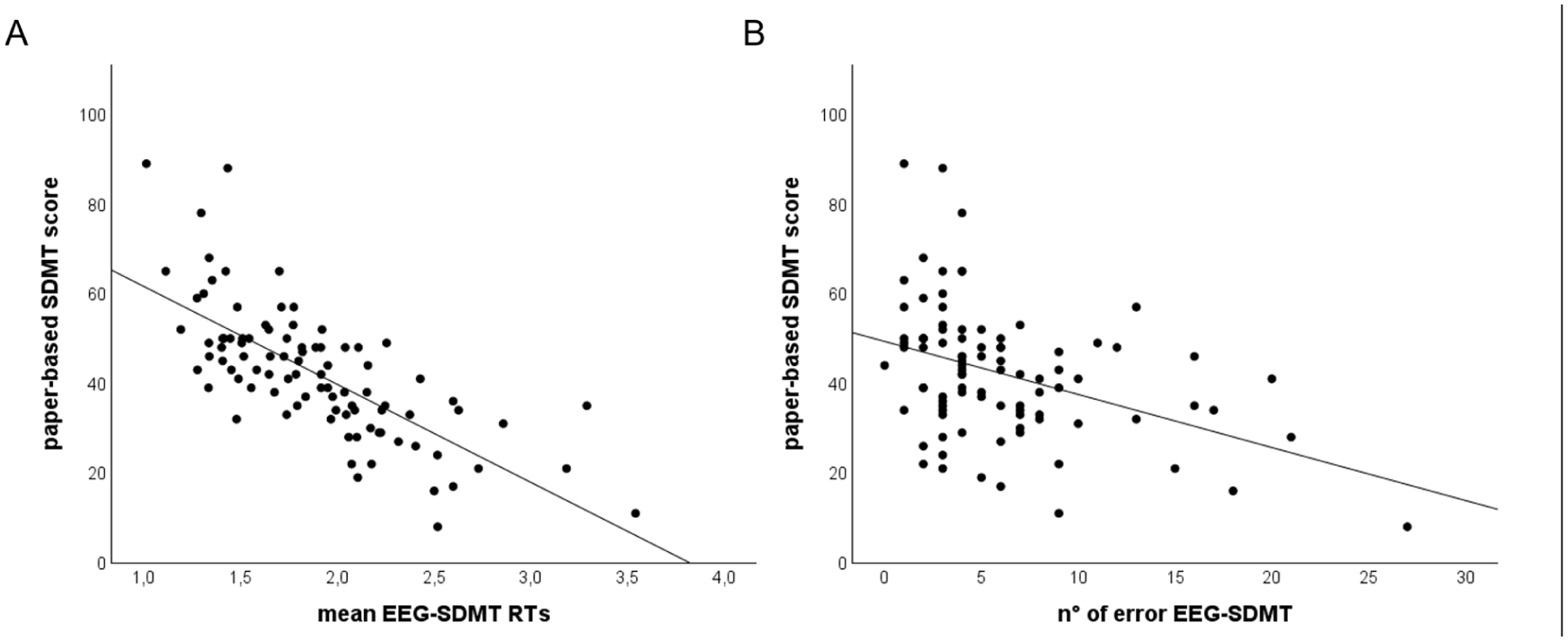
(a) Negative correlation between the key-press reaction times to EEG-SDMT (x axis) and paper based SDMT raw scores (y axis) in people with MS (n = 92). (b) Negative correlation between the number of errors in the EEG-SDMT (x axis) and paper based SDMT raw scores (y axis) in people with MS (n = 92).
Event-related potentials
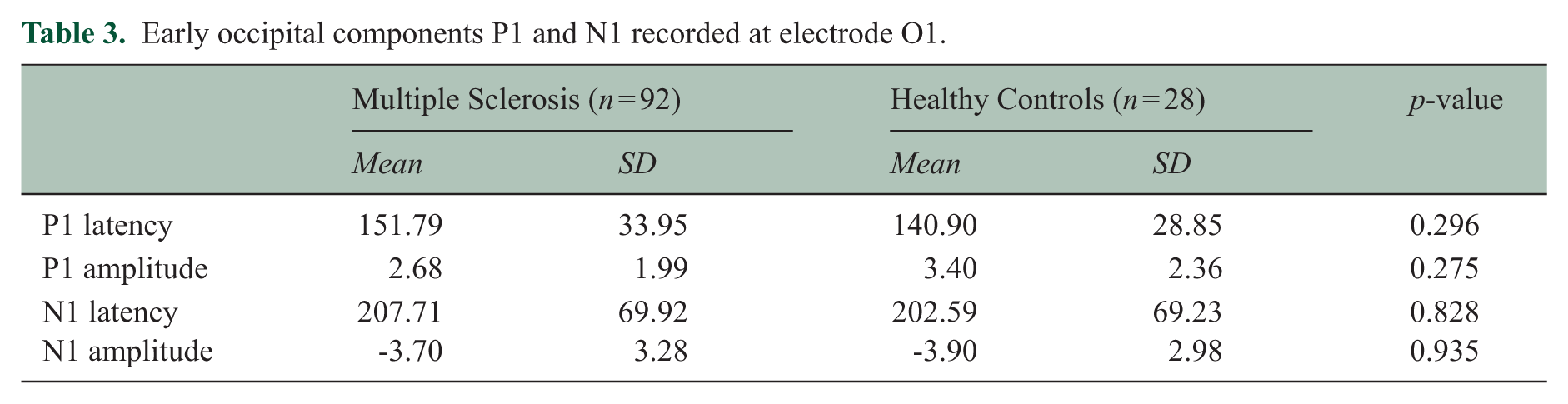
Grand average ERPs for PwMS and HCs are shown in Figure 3. After the stimulus onset, a positive peak – designated as the P5 component–with a higher amplitude in HC (13.12 ± 5.64 μV) in comparison to pwMS (10.84 ± 6.41 μV) was elicited over centro-parietal regions (Wilcoxon test, FDR corrected p = n.s). Latency was significantly longer in pwMS (611.72 ± 122.30 ms) in comparison to HCs (517.29 ± 75.53 ms) (Wilcoxon test, FDR corrected p < 0.01) as in Figure 3(a). No significant differences were found in P5 between pwMS with cognitive impairment (n = 40) and those without cognitive impairment (n = 52) (Wilcoxon test, FDR corrected p = .940). No significant difference between HC and pwMS were found for the early occipital components (Table 3). After subtracting the visual processing component P1 from the P5 component, a cognitive processing component was identified, exhibiting a significantly longer latency in pwMS (465.68 ± 121.07 ms) compared to HC (376.39 ± 64.42 ms) (Wilcoxon test, FDR corrected p < .001).
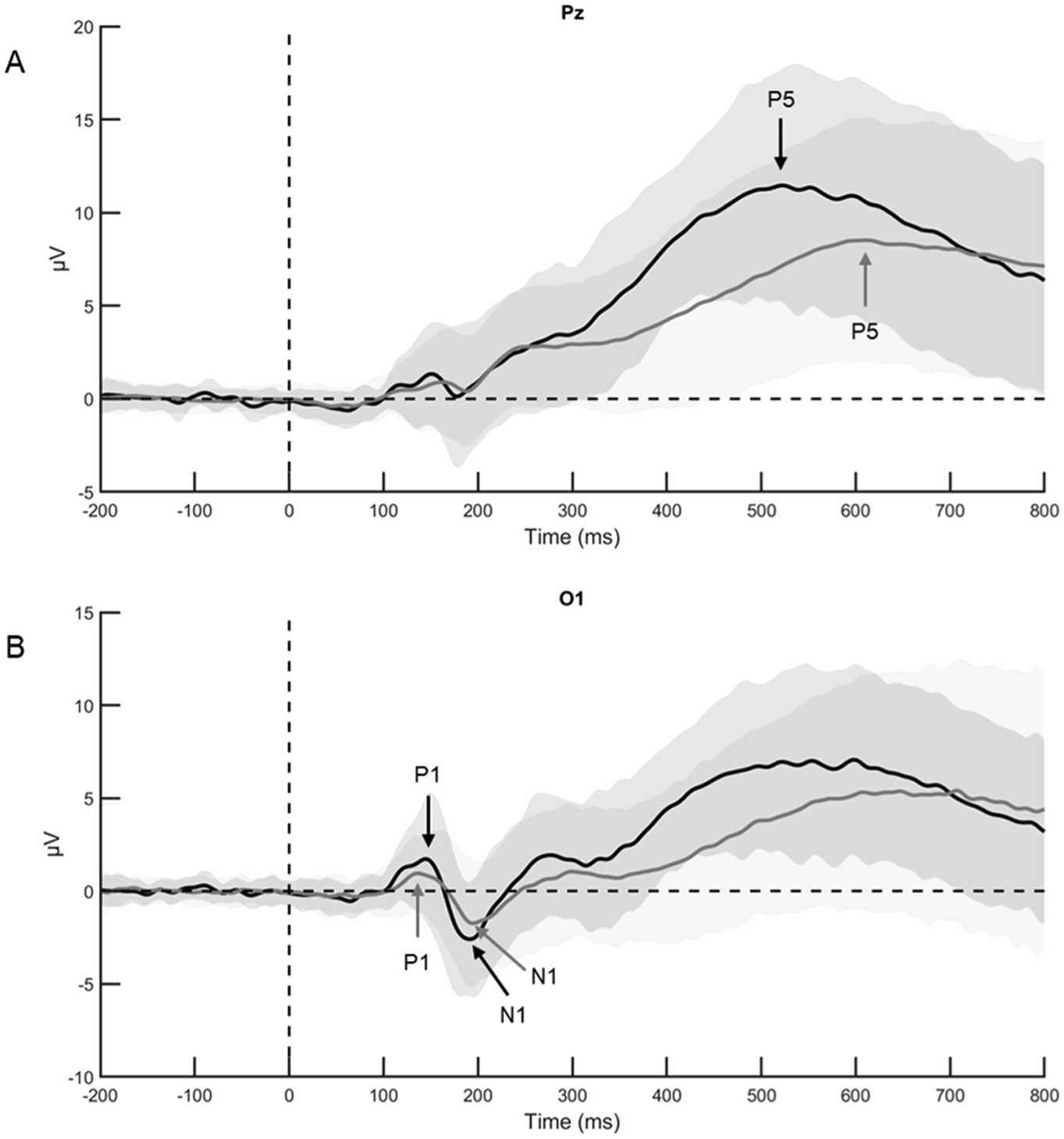
Grand average ERPs of healthy controls (in black) and people with MS (in grey). (a) The P5 component to EEG-SDMT recorded in response to stimulus onset at electrode Pz. The arrows indicate the average peak latency of each group. (b) The visual components P1 and N1 recorded at electrode O1.
Early occipital components P1 and N1 recorded at electrode O1.
Behavioural measures
EEG-SDMT
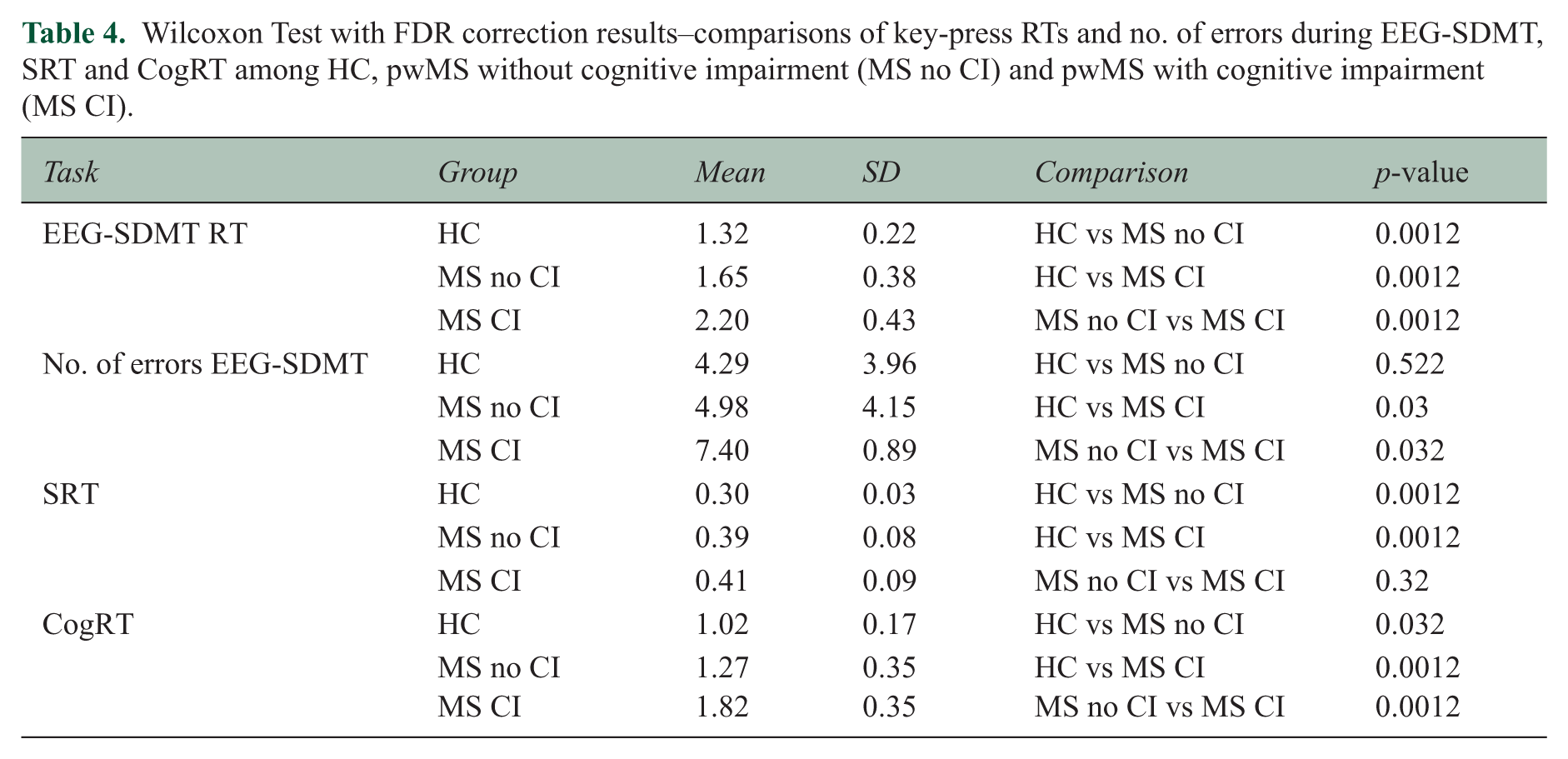
Pairwise comparisons found a significant difference in key-press RTs among the groups (HC, pwMS without cognitive impairment, pwMS with cognitive impairment). The number of errors also varied significantly between HC and pwMS with cognitive impairment, and between pwMS with and without cognitive impairment (Table 4).
Wilcoxon Test with FDR correction results–comparisons of key-press RTs and no. of errors during EEG-SDMT, SRT and CogRT among HC, pwMS without cognitive impairment (MS no CI) and pwMS with cognitive impairment (MS CI).
SRT
Among the 92 pwMS and 28 HC, only 62 pwMS and 12 HCs completed the simple RT task as this measure was implemented after the start of the study and was not included in the initial protocol. Significant differences in RTs were found between HC and pwMS without cognitive impairment, and HC and pwMS with cognitive impairment (Table 4).
CogRT
Pairwise comparisons showed significant differences across groups (Table 4). The CogRT demonstrated significant correlations with BICAMS scores. Specifically, CogRT was negatively correlated with paper-based SDMT scores (ρ = −.77, p < .001), CVLT-II scores (ρ = −.58, p < .001), and BVMT-R scores (ρ = −.61, p < .001) (Figure 4).
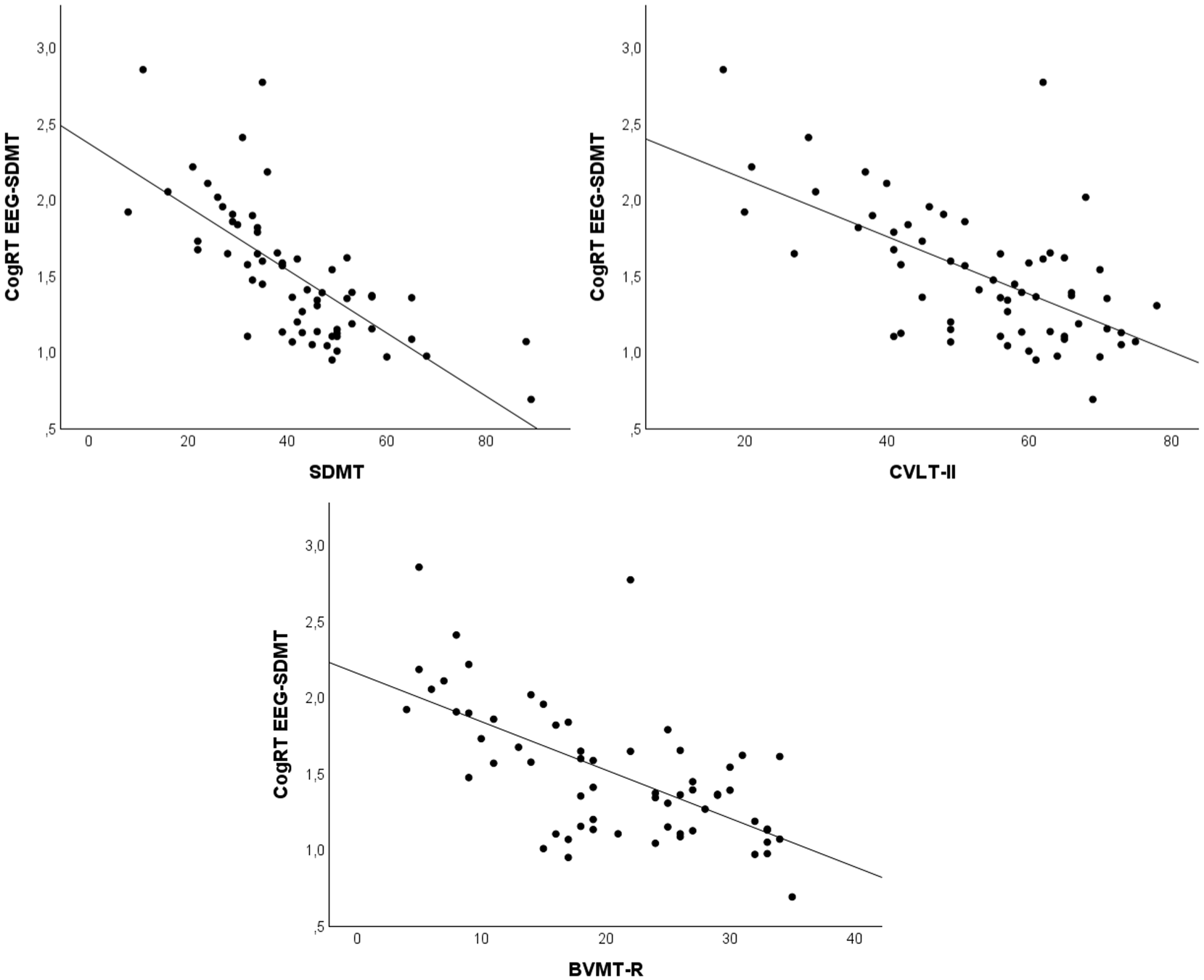
Negative correlation between the three sub-tests of the BICAMS (SDMT; CVLT-II; BVMT-R) (x axis) and the cognitive response time (y axis) in people with MS (n = 62).
Sensitivity analysis
The sensitivity analysis confirmed the original findings, with all results remaining unchanged after adjusting for age, as shown in the Supplementary Materials.
Discussion
We aimed at exploring the usefulness of an EEG-compatible SDMT for investigating its neurophysiological and behavioural correlates. Specifically, since the SDMT is widely used as a screening tool for cognitive dysfunction in MS, we aimed at identifying electrophysiological and behavioural markers able to index cognitive impairment. We developed an EEG-compatible version of the SDMT. To reduce potential artefacts, we minimized eye movements and replaced the oral response modality–known to introduce interference in EEG traces 26 –with a simple keypress response requiring minimal hand movement. While this adaptation differs slightly from the standardized paper-based SDMT, it engages the same cognitive functions.
This similarity is supported by the strong correlation observed between RTs in the EEG-SDMT and scores from the paper-based SDMT. A weaker association of errors with the clinical SDMT score could be expected, since the paper-based version is scored by the number of correct responses in 90 seconds. Errors may affect performance only indirectly, by reducing the total number of correct responses, whereas RTs more directly reflect the scoring principle of the test. These findings suggest that the EEG-SDMT may capture similar cognitive domains as the traditional version, while being tailored for neurophysiological research. Although alternative versions of the SDMT have been adapted for use on smartphones, tablets, and computers, these tools are primarily designed for practical usability in clinical or everyday contexts. To the best of our knowledge, the EEG-SDMT is the first version developed for EEG research, enabling the simultaneous collection of both neural and behavioural data. The P5 component identified in response to EEG-SDMT task can be interpreted as a P300 with prolonged latency when compared to the P300 typically elicited in traditional visual oddball or working memory paradigms.27,28 This difference is likely due to the number of items that must be processed before determining the correctness of the presented stimulus. Consistent with previous findings, greater task demands – reflected in the number of items to process – are associated with increased P300 latency. 29 We observed a longer peak latency in pwMS in comparison to controls over centro-parietal areas. As previous studies have consistently reported prolonged P300 latency in pwMS relative to controls in response to oddball paradigm,13,14 the P5 may similarly serve as a potential neurophysiological marker of a slowing in cognitive processing speed inherent to the pathological condition. Early afferent components did not differ between HC and pwMS, suggesting that the longer latency of the P5 component in pwMS is likely due to higher-order cognitive processes. This is supported by the hypothesis that information processes stages unfold sequentially in the brain. 30 Therefore, the similar latencies observed in the early sensory components in pwMS and HC support the notion that the group disparities stem from cognitive processing mechanisms. This hypothesis is further sustained by the longer latency of the cognitive processing component, calculated by subtracting P1 from P5 latency. However, despite its cognitive component, the P5 component still occurs relatively early in the temporal cascade of information processing and may be too premature and temporally constrained to robustly differentiate pwMS with and without cognitive impairment. ERP analysis, by definition, captures neural responses that are time-locked to external events and averages out trial-by-trial variability, thereby minimizing both intra- and inter- subject variability. While this provides insights into synchronized cognitive events, it may lack the sensitivity needed to detect more complex, variable patterns of cognitive impairment in MS. Thus, while the P5 may serve as a useful general marker of cognitive slowing, other EEG features may be more suitable for describing further stages of cognitive processing involved in the task. Moreover, complementary neuropsychological testing may be necessary to more accurately assess cognitive impairment and may be better suited for the continuous assessment of specific cognitive domains. As previously suggested (Piras et al.) 16 , ERPs may be especially valuable when physical disability hinders the administration of traditional cognitive assessments.
Cognitively impaired pwMS had significantly longer EEG-SDMT RTs and committed more errors compared with both pwMS without cognitive impairment and HCs. SRT did not significantly differ between pwMS with and without cognitive impairment.
Slower RTs and reduced response accuracy in pwMS have also been reported in other studies employing computerized visual-manual tasks. 31 Notably, Reicker et al. 32 demonstrated that pwMS exhibit significantly slower RTs compared to HCs in computerized information processing tasks. Moreover, increasing the difficulty of the test further amplified the RT differences between the two groups. Importantly, their analysis accounted for potential generalized motor slowing by normalizing task performance relative to a baseline SRT. They concluded that the prolonged RTs observed in pwMS are associated with reduced information processing speed, consistent with our findings. However, that study lacked a comparison between cognitively impaired and preserved pwMS. To our knowledge, only one study has shown RTs from a tablet-based test to be sensitive to cognitive dysfunction in pwMS. 33 The CogRT, obtained as a measure of cognition independent of the motor component, demonstrated its ability to discriminate between pwMS with and without cognitive impairment, with the cognitively impaired group showing significantly longer CogRT values. This finding is particularly important as it highlights the sensitivity of CogRT in capturing subtle variations in cognitive function that might be overlooked in traditional "pen-and-paper" tests, which cannot incorporate RTs as a parameter. Furthermore, the significant correlations observed between CogRT and all three tests of the BICAMS underline its utility in reflecting cognitive performance across multiple domains, such as processing speed, verbal learning, and visual memory. This relationship strengthens the case for integrating the calculation of CogRT into cognitive assessments, as it provides a quantitative and objective measure of processing efficiency, which traditional neuropsychological tools may not directly capture. This finding is aligned with a previous study that have identified a strong association between RTs (simple and complex) and cognitive functions as measured through the SDMT. 33 In addition, the independence of CogRT from the motor component allows for a more accurate evaluation of cognitive abilities, free from the confounding effects of motor impairments often observed in pwMS.
Taken together, our findings suggest that the slower performance observed in the cognitively impaired group was attributable to reduced cognitive efficiency rather than motor slowing, or visual dysfunction (as no differences were found in the visual ERP components). This interpretation is further reflected in their poor performance on the MoCA and BICAMS compared to cognitively preserved pwMS.
Limitations
Participants were recruited during hospitalization in a rehabilitation clinic, which is not fully representing the broader MS population, due to the overrepresentation of progressive forms and moderate disability within the MS cohort. However, the EEG procedures used are feasible in outpatient settings. Another limitation concerns the smaller number of HC (n = 28) compared to pwMS (n = 92), which may have reduced statistical power. In addition, the SRT task was not administered to all participants, partly limiting conclusions from this measure. Finally, ERP analyses did not differentiate pwMS with and without cognitive impairment, suggesting that alternative EEG analysis approaches may be explored.
Conclusion
Our EEG-SDMT paradigm allowed to obtain correlates of neurophysiological activity during SDMT performance, which was significantly affected in pwMS. The strong correlation between RTs in the EEG-SDMT and the scores in the paper-based SDMT demonstrate that this newly developed task is a reliable counterpart to the standard paper-based SDMT. Early afferent components did not differ between HC and pwMS, suggesting that the significantly longer latency of the P5 component in pwMS is likely due to higher-order cognitive processes. Finally, the CogRT is an effective index of cognitive functions as measured by the BICAMS.
Supplemental Material
sj-docx-1-msj-10.1177_13524585261423416 – Supplemental material for Event-related potentials and behavioural correlates of cognitive functions in MS: An EEG study during symbol digit modalities test
Supplemental material, sj-docx-1-msj-10.1177_13524585261423416 for Event-related potentials and behavioural correlates of cognitive functions in MS: An EEG study during symbol digit modalities test by Marta Tacchini, Giulia Gamberini, Michelangelo Dini, Chiara Rossi, Angela Boschetti, Letizia Turchi, Mariaemma Rodegher, Luca Chiveri, Jeroen Van Schependom, Guy Nagels, Giancarlo Comi and Letizia Leocani in Multiple Sclerosis Journal
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: G.C. received consulting and speaking fees from Biogen, Merck, Novartis, Roche, Sanofi Genzyme, Almirall, Teva, Actelion, Cellgene, BMS, and Janssen-Cliag (none related to the present study). L.L. received research support from Novartis, Almirall, Biogen, and Merck and consultancy or speaker fees from Novartis, Almirall, Biogen, Merck, Janssen-Cliag, Bristol-Myers Squibb, and Roche (none related to the present study). All other authors have no conflicts of interest to declare.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
Access to the datasets generated and/or analysed during the present study may be granted upon formal request to the corresponding author, conditional on approval by the institutional data protection authority.
Supplemental Material
Supplemental material for this article is available online.