
Abstract
Background:
Multiple sclerosis (MS) is a demyelinating disorder of the central nervous system that often affects women of reproductive age. The impact of MS on obstetric and neonatal outcomes remains unclear, particularly in women of advanced maternal age.
Objectives:
We aimed to evaluate obstetric and neonatal outcomes in women with MS using data extracted from the National Health Screening Examination (NHSE) and the National Health Screening Program for Infants and Children (NHSPIC) in Korea.
Methods:
Women with singleton live births between 2011 and 2020 who underwent the NHSE within 4 years before pregnancy were identified. Women with MS (n = 481) were matched 1:10 to women without MS (n = 4810) based on age and comorbidity indices. Outcomes were compared using multivariate logistic regression considering maternal age.
Results:
Women with MS had a higher risk of preterm birth (odds ratio [OR] = 2.50; 95% confidence interval [CI] = 1.38–4.52) and placenta previa (OR = 1.83; 95% CI = 1.05–3.20) compared with controls. The association between MS and preterm birth was particularly pronounced in women of advanced age. Other obstetric outcomes did not differ significantly according to MS status, and neonatal outcomes were similar between the two groups.
Conclusions:
Most obstetric and neonatal outcomes were comparable between women with and without MS. However, for pregnant women with MS, age ⩾ 35 years was associated with an increased risk of preterm birth, highlighting the importance of careful prenatal monitoring in this population. Further studies are warranted to elucidate the mechanisms underlying this risk.
Keywords
Introduction
Multiple sclerosis (MS) is a chronic immune-mediated demyelinating disease of the central nervous system, typically involving the spinal cord or optic nerves. 1 As many patients with MS are of reproductive age, the impact of MS on obstetric outcomes and neonatal health is an important, although underexplored, topic. Pregnancies in women with MS are often considered high-risk due to a higher incidence of obstetric complications such as preterm birth and cesarean delivery.2 –4
However, current evidence regarding obstetric or neonatal outcomes in women with MS remains inconsistent.5 –11 More critically, previous studies have not fully accounted for the recent global trend toward increasing maternal age.12 –16 Over the past decades, maternal age at childbirth has increased rapidly, with a substantial rise in the proportion of pregnant women aged 35 years or older.17,18 This upward trend in maternal age has been particularly pronounced in Asian countries such as South Korea, Japan, and Taiwan.19 –21 Furthermore, most existing studies have been conducted in Western populations, which limits the generalizability of their findings across diverse ethnic groups.22,23 Therefore, further investigation, particularly studies that stratify data by maternal age and account for ethnic diversity, is needed to elucidate better the effects of MS on obstetric and neonatal outcomes.
In this study, nationwide health data from Korea were used to evaluate obstetric complications, neonatal morbidities, and congenital anomalies in women with MS compared with propensity-matched controls. This study aimed to provide evidence of MS-related risks in an East Asian population. Importantly, an age-stratified analysis was conducted to examine whether the effect of MS on these outcomes differs between older and younger women.
Methods
Database
The National Health Insurance Service (NHIS) claims data, which cover over 97% of the Korean population, were used for the analysis. This dataset includes demographic information; diagnosis codes based on the International Classification of Diseases, 10th Revision (ICD-10); therapeutic procedures performed during inpatient and outpatient care; and prescription records. Alongside these claims data, data from the NHIS were extracted, including information from the National Health Screening Examination (NHSE) and National Health Screening Program for Infants and Children (NHSPIC) in Korea,24,25 which are well-established, routine health checkup programs in Korea with general participation rates of approximately 75%.26,27
The NHSE program, initiated in the 1980s, offers comprehensive biennial health checkups that cover blood pressure measurements, vision tests, laboratory studies, and health interviews for all citizens aged > 20 years.24,26 NHSE data have been available for analysis since 2002. The NHSPIC program, launched in 2007, includes history taking, physical examinations, visual acuity screenings, and questionnaires with anticipatory guidance. 25 Under the NHSPIC, all infants and children receive annual health checkups until the age of 8 years.
Both NHSE and NHSPIC represent the largest and most complete nationwide population-based datasets in Korea, providing reliable information even for rare diseases such as MS. In this study, these databases were linked by matching maternal and childbirth records, including associated health information.
Study population
The study cohort comprised women with singleton pregnancies resulting in live births between January 1, 2011, and December 31, 2020, who had participated in the NHSE within the 4 years prior to pregnancy. Women with incomplete information on obstetric and neonatal outcomes and those with multifetal gestation were excluded.
The study population was divided into two groups: women with MS and matched controls. Women with MS were identified when any of the following criteria were present: (1) two or more outpatient or hospitalization claims with the ICD-10 code G35.0 and within 4 years before pregnancy or (2) enrollment in the Rare Intractable Diseases (RID) program with the corresponding MS code. The NHIS RID registry requires all MS diagnoses to conform to the 2017 revised McDonald criteria for MS.
The control group included pregnant women without MS selected through propensity score matching based on age and the Charlson Comorbidity Index (CCI). Controls were matched to MS patients at a ratio of 10:1 using nearest-neighbor propensity score matching.
Outcome measures
The incidence of gestational hypertension (gHTN, ICD-10 code O13), gestational diabetes mellitus (gDM, ICD-10 code O24.4), preterm birth (ICD-10 code O60.1), cesarean section (ICD-10 code O82), placental abruption (ICD-10 codes O45.0–O45.9), placenta previa (ICD-10 codes O44.0–O44.1), and postpartum hemorrhage (ICD-10 codes O72.0–O72.2) in pregnant women with and without MS was investigated. Furthermore, the occurrence of peripartum complications, including deep vein thrombosis (ICD-10 codes O22.3, O87.1), sepsis (ICD-10 code O85), and respiratory distress (ICD-10 codes J80, J96.0) was also assessed. The peripartum period was defined as 30 days before and 30 days after delivery.
Neonatal outcomes included transient tachypnea (ICD-10 code P22.1), respiratory distress syndrome (ICD-10 code P22.0), necrotizing enterocolitis (ICD-10 code P77.0), intraventricular hemorrhage (ICD-10 codes P52.0–52.9), bronchopulmonary dysplasia (ICD-10 code P27.1), neonatal hypoglycemia (ICD-10 code P70.4), and congenital malformations. Congenital malformations were identified within the first 12 months of life and were classified by organ system using the following ICD-10 codes: Q00–Q07, nervous system; Q10–Q18, eye, ear, face, and neck; Q20–Q28, circulatory system; Q30–Q34, respiratory system; Q35–Q37, cleft lip and cleft palate; Q38–Q45, digestive system; Q50–Q56, genital organs; Q60–Q64, urinary system; Q65–Q79, musculoskeletal system; Q80–Q89, other malformations; and Q90–Q99, chromosomal abnormalities. Each outcome was defined by the presence of at least two outpatient or inpatient visits with the corresponding diagnostic codes in the MS and control groups.
Covariables
The following potential confounding variables that could influence obstetric and neonatal outcomes were considered: maternal age, the CCI score, parity, and pre-existing maternal comorbidities. Chronic hypertension (ICD-10 codes I10–I15) was recorded in the mother’s medical history within 4 years before pregnancy. Similarly, pre-existing diabetes mellitus was defined by any diagnosis of diabetes (ICD-10 codes E10–E14) in the 4 years before pregnancy. These definitions ensured that chronic hypertension and diabetes were distinguished from gHTN and gestational diabetes.
Statistical analysis
The chi-square test was used for categorical variables and two-sample t-test for continuous variables to compare between-group differences. Data are presented as mean ± SD or number with percentage. To reduce selection bias, propensity score matching was conducted based on maternal age and CCI using a 1:10 nearest-neighbor matching algorithm.
Multivariate logistic regression was performed to estimate odds ratios (ORs) and 95% confidence intervals (CIs) for obstetric neonatal outcomes associated with MS. As the study matched for age and overall comorbidity burden, primary analyses were conducted without further covariate adjustment. In addition, outcomes with fewer than five events were excluded from the regression analysis because reliable statistical estimates were not feasible with very small event counts. To protect participant confidentiality in accordance with national data protection guidelines, cell counts fewer than five individuals were suppressed and reported as “<5” in reported tables. Where necessary, additional complementary suppression was applied to prevent back-calculation of small cell counts. Subgroup analyses were conducted using age stratification (<35 or ⩾35 years) to evaluate effect modification by advanced maternal age (AMA). All statistical analyses were performed using IBM SPSS Statistics for Windows version 23.0 (IBM Corp., Armonk, NY, USA). Statistical significance was set at p < 0.05.
Standard protocol approvals, registrations, and patient consent
This study was approved by the Institutional Review Board of Korea University Guro Hospital (approval number: 2023GR0460). Informed consent was not required due to the use of de-identified public data from the NHSE and NHSPIC.
Data availability statement
Data sharing does not apply to this article.
Results
Characteristics of the study population
Among the 3,913,527 women who delivered infants from 2011 to 2020 and underwent NHSE within 4 years before pregnancy, 481 (0.01%) were diagnosed with MS before pregnancy. A total of 4810 pregnant women without MS were selected as controls (Figure 1). Baseline characteristics of the study population after propensity score matching for age and CCI are summarized in Table 1. The mean maternal age was 33.01 (SD = 3.96) years in both groups. Women with MS were more frequently primiparous (60.29% vs 50.35%, p < 0.001) and had pre-existing conditions, including DM (7.48% vs 2.37%, p < 0.001) and HTN (2.49% vs 0.98%, p = 0.003).
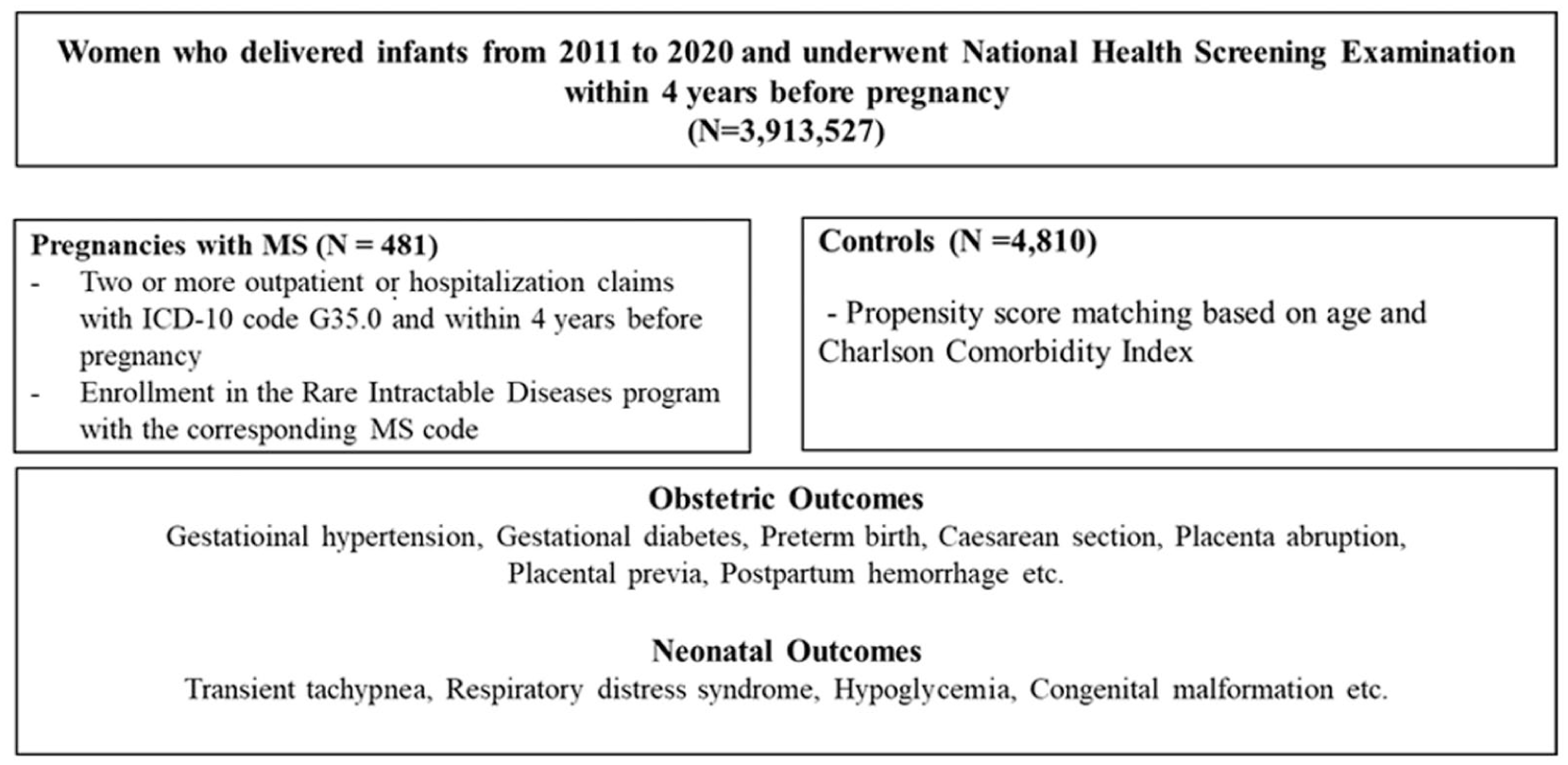
Flow chart of this study.
Comparisons of baseline characteristics and obstetric complications in propensity score-matched cohorts.
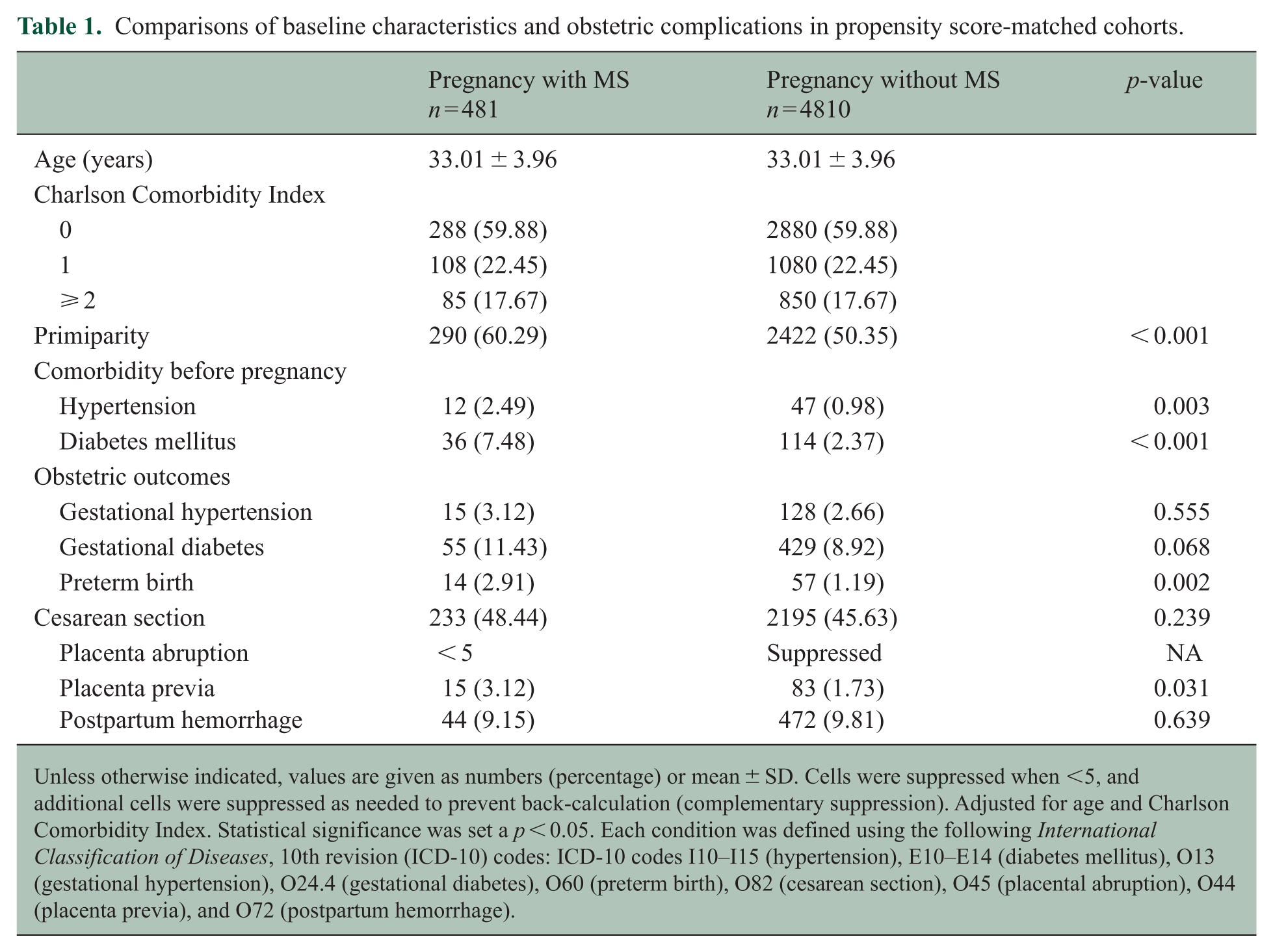
Unless otherwise indicated, values are given as numbers (percentage) or mean ± SD. Cells were suppressed when <5, and additional cells were suppressed as needed to prevent back-calculation (complementary suppression). Adjusted for age and Charlson Comorbidity Index. Statistical significance was set a p < 0.05. Each condition was defined using the following International Classification of Diseases, 10th revision (ICD-10) codes: ICD-10 codes I10–I15 (hypertension), E10–E14 (diabetes mellitus), O13 (gestational hypertension), O24.4 (gestational diabetes), O60 (preterm birth), O82 (cesarean section), O45 (placental abruption), O44 (placenta previa), and O72 (postpartum hemorrhage).
Similar to the steady decline in the annual number of pregnant women in South Korea from 835,359 in 2011 to 272,861 in 2020, the number of pregnant women with MS during the same period also decreased from 105 in 2011 to fewer than 5 in 2020 (Figure 2). Although the general downward trend in the total number of pregnancies likely reflects broader demographic changes, the number of MS cases among pregnant women has remained very low throughout the past decade, with minor year-to-year fluctuations.
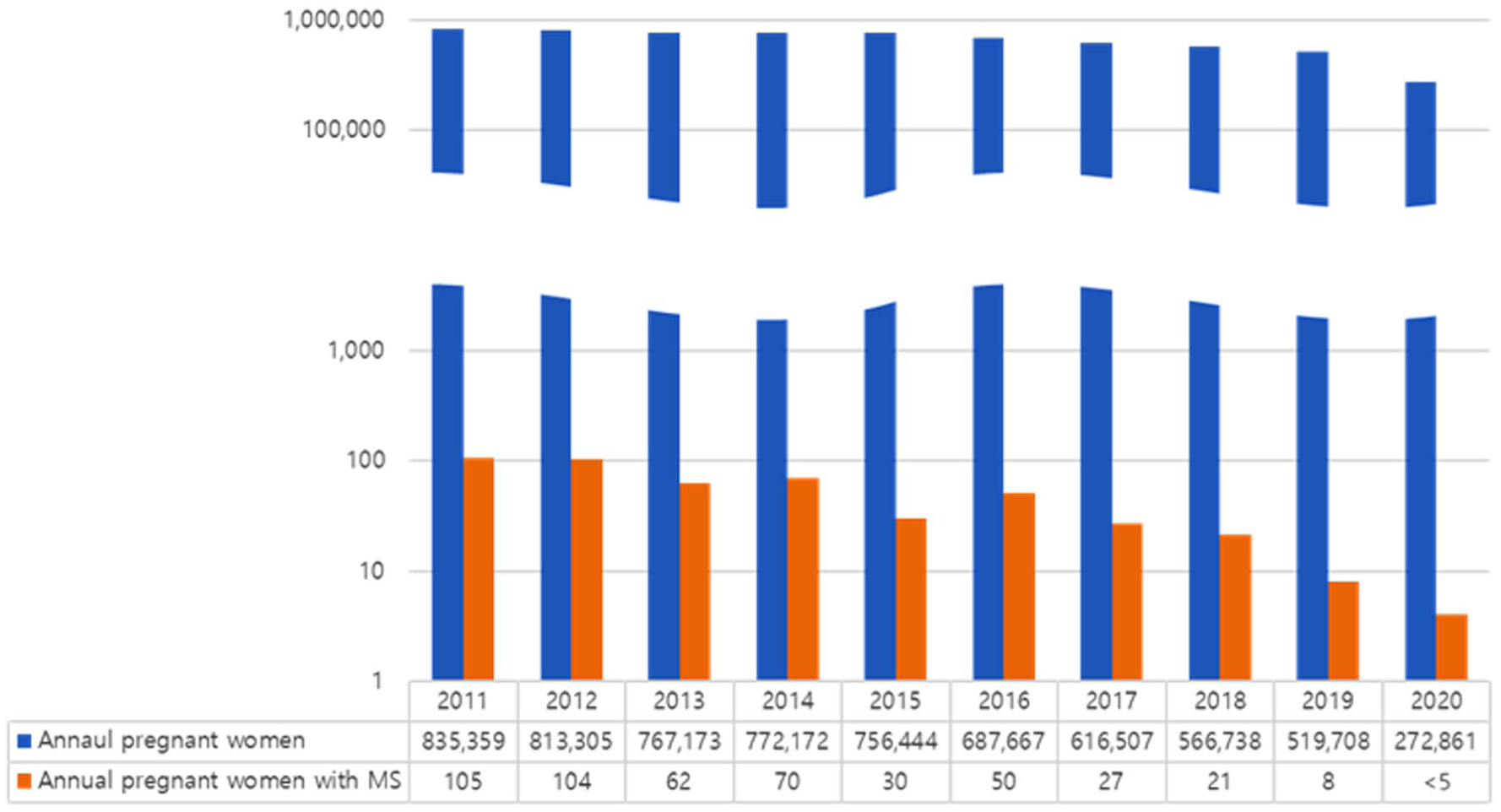
Childbirth trends in women with and without multiple sclerosis in Korea.
Pregnancy outcomes
Pregnant women with MS had a higher incidence of preterm birth (2.91% vs 1.19%, p = 0.002) and placenta previa (3.12% vs 1.73%, p = 0.031) than controls. However, no significant differences were observed between the groups in terms of other obstetric complications, including the cesarean section rate (p = 0.239), gHTN (p = 0.555), gDM (p = 0.068), and postpartum hemorrhage (p = 0.639). Other peripartum complications, such as sepsis or respiratory distress, were not reported, and deep vein thrombosis occurred very rarely in the entire cohort. In multivariable logistic regression analysis, the risk of preterm birth (OR = 2.50; 95% CI = 1.38–4.52) and placenta previa (OR = 1.83; 95% CI = 1.05–3.20) were significantly higher in pregnant women with MS (Table 2). No significant differences were found between the groups for other outcomes.
Age-dependent risk estimates of obstetric and neonatal outcomes in pregnant women with and without multiple sclerosis.
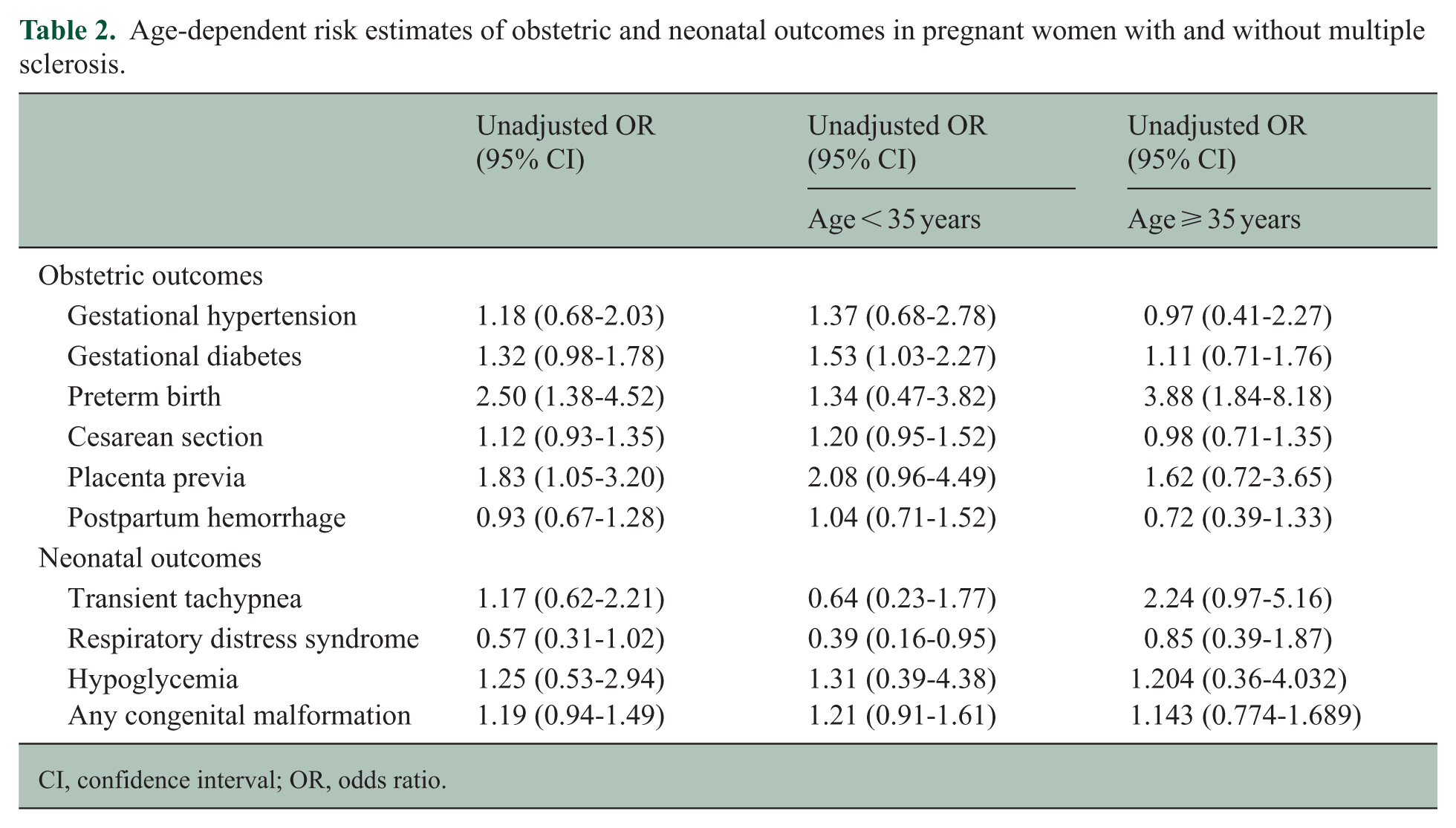
CI, confidence interval; OR, odds ratio.
Neonatal outcomes
The offspring of women with MS exhibited a higher incidence of certain organ-specific congenital malformations than the offspring of controls. In particular, congenital malformation of the musculoskeletal system (6.86% vs 4.39%, p = 0.014), respiratory system (1.25% vs 0.44%, p = 0.017), and head and neck anomalies (3.95% vs 2.16%, p = 0.013) were more frequent in children born to mothers with MS. In contrast, no significant differences were observed between the MS and control groups with regard to other neonatal complications, including transient tachypnea (p = 0.618), respiratory distress syndrome (p = 0.055), or neonatal hypoglycemia (p = 0.604) (Table 3). In the multivariate regression analysis, neonatal outcomes, including the overall occurrence of any congenital malformations, did not differ significantly between the two groups (21.41% vs 18.67%, p = 0.143).
Neonatal outcomes in pregnant women with multiple sclerosis.
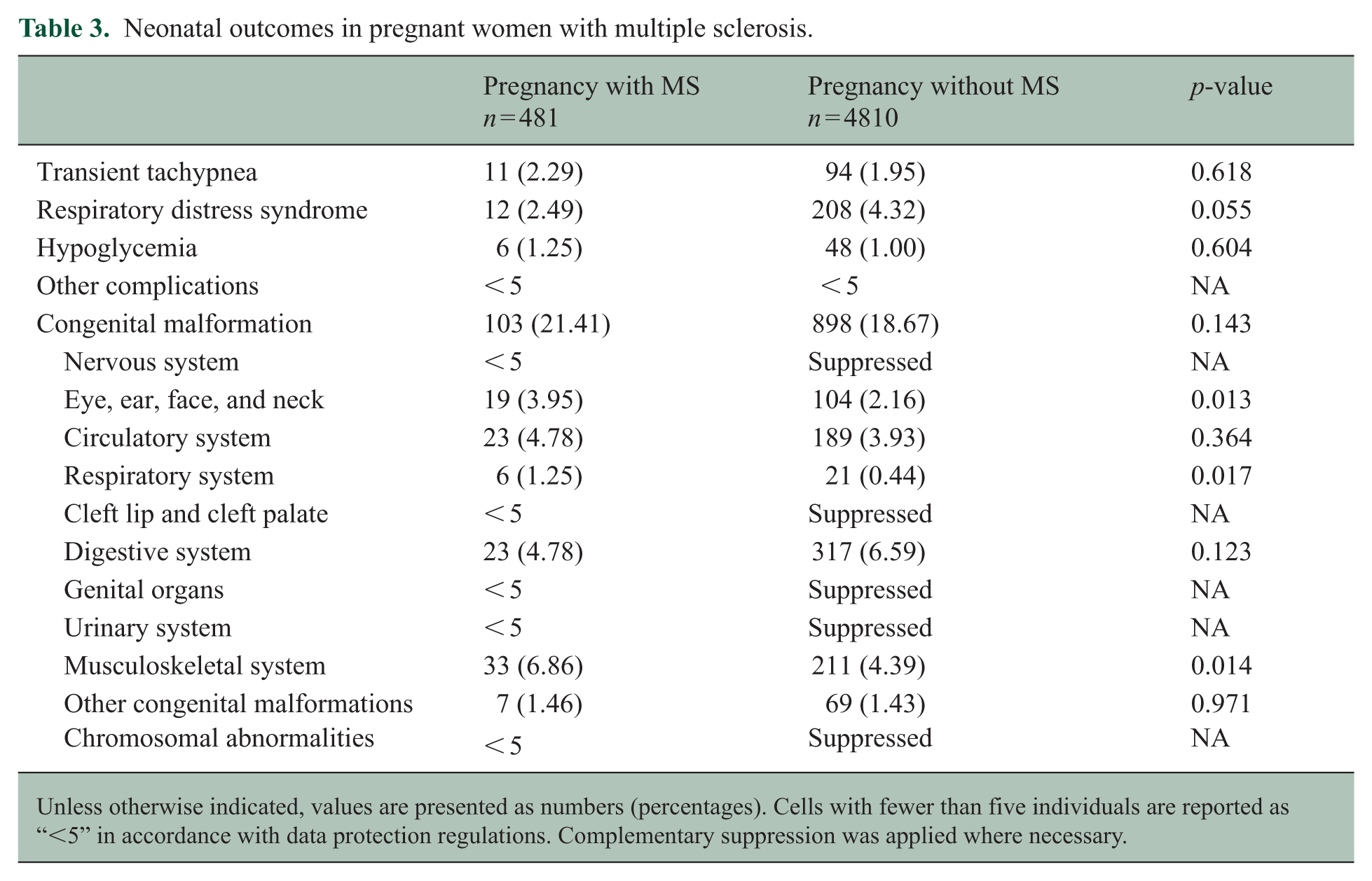
Unless otherwise indicated, values are presented as numbers (percentages). Cells with fewer than five individuals are reported as “<5” in accordance with data protection regulations. Complementary suppression was applied where necessary.
Age-stratified analysis
The population was stratified into two groups based on maternal age (<35 or ⩾35 years), and the risk of obstetric and neonatal outcomes was analyzed. In the younger group, no statistically significant differences were observed between women with and without MS. However, in the older group, the risk of preterm birth was significantly higher in women with MS (OR = 3.88; 95% CI = 1.84–8.18). However, other complications, including placenta previa and congenital malformations, did not differ between the groups.
Discussion
This study evaluated obstetric complications and neonatal outcomes in women with MS using data from the NHSE and NHSPIC within the NHIS claims database. The incidence of preterm birth (2.91% vs 1.19%, p = 0.002) and placenta previa (3.12% vs 1.73%, p = 0.031) was significantly higher among women with MS than among matched controls. In the multivariate regression analysis stratified by age, the risk of preterm birth was substantially higher in women with MS and AMA (⩾35 years; OR = 3.88, 95% CI = 1.84–8.18). However, no significant statistical differences in neonatal outcomes, including congenital malformations, were observed between pregnant women with MS or without MS.
This is notable for being one of the few investigations evaluating obstetric and neonatal outcomes in East Asian women with MS. Previous studies have primarily focused on Western populations, reflecting the higher prevalence of MS in North America and Europe.4 –7,10,11,28 Among East Asian countries, a nationwide population-based study from Taiwan is the only large-scale investigation to evaluate pregnancy outcomes in women with MS. A Taiwanese study reported an increased incidence of preterm birth (OR = 2.25) and small for gestational age (SGA) infants (OR = 1.89), consistent with our results regarding preterm birth. 22 In the multivariable regression analysis, MS was associated with an increased risk of preterm birth (adjusted OR = 2.46; 95% CI = 1.35–4.48). Although several studies from the United States and Canada have suggested a trend toward increased preterm births in women with MS, these findings have not consistently reached statistical significance.7,29
Recent data from the German MS and Pregnancy Registry suggest an increased risk of preterm birth or SGA, which is attributable to placental dysfunction induced by MS-associated chronic inflammation, involving higher levels of cytokines such as interleukin-6 or tumor necrosis factor alpha.7,30 –34 This matched cohort analysis helped to clarify this issue by demonstrating a significant association with preterm delivery in pregnancy in women with MS. Furthermore, the study determined that the impact of MS on preterm birth was age-dependent. An age-stratified analysis was performed to account for AMA in MS, a widely recognized risk factor for peripartum and obstetric complications.12 –16 The study showed that the risk of preterm birth was more pronounced in the older maternal age group among women with MS. This finding is more consistent with an additive effect, whereby the established obstetric risk associated with AMA was compounded by the presence of MS. Potentially, the increased risk may be partially explained by age-related impairment of remyelination, referred to as immunosenescence, in older pregnant women with MS.35,36
In addition, a higher incidence of placenta previa in women with MS was observed. Although the exact pathophysiology remains unclear, immunological dysregulation in MS may contribute to complications such as placenta previa. Previous studies have highlighted the importance of cytokine interactions in successful implantation and placental development,37,38 which suggests that MS-related immune dysfunction might be associated with abnormal placentation, although further research is needed to confirm this hypothesis.
Meanwhile, we did not include multi-gestational pregnancy, which is a strong independent risk factor for preterm birth and confounds obstetric risk. 39 By analyzing only singleton pregnancies, we aimed to isolate the MS-specific effects on pregnancy outcomes without the confounding influence of twin or higher-order pregnancies.
Medications used in MS, such as corticosteroids and disease-modifying therapies (DMTs), may be relevant factors in pregnancy and delivery outcomes. 28 Previous studies have suggested that steroid exposure during the first trimester is considered a risk factor.30,39,40 However, corticosteroid was not used as maintenance therapy in patients with MS but are applied as a rescue treatment for acute relapses in clinical practice. Since relapse was not frequently observed during the pregnancy period in patients with MS, corticosteroid exposure is unlikely to be a major cause of neonatal disability. In addition, recent findings from the German MS and Pregnancy Registry have indicated that treatment with DMTs was not associated with an increased risk of congenital anomalies.30,40,41 Because the treatment status could not be assessed in this cohort, this study could not examine the potential influence of corticosteroids or other DMTs, and the possibility that treatment contributed to the observed congenital anomalies cannot be excluded. Nonetheless, the risk of congenital anomalies was not statistically significant in multivariate analysis in this study.
Finally, the national birth rate in Korea has declined sharply over the past decade (Figure 2). By 2011, the country registered 835,359 deliveries nationwide; by 2022, this number decreased to 272,861. Although this trend is well known in the general population, it was even more pronounced among women with MS. In 2011, 105 deliveries were recorded among women with MS compared with fewer than five births in 2022. This sharp decline may be partially attributed to nationwide demographic changes and the impact of the coronavirus disease pandemic and suggests a disproportionately severe decrease in childbirth among women with MS. This trend contrasts with previous findings from a study conducted in the United States, although further research is required to explore the underlying causes. 29
This study had some limitations that should be acknowledged. As previously mentioned, information regarding medication use was not available for analysis in this study. Although most DMTs for MS have not been associated with adverse pregnancy outcomes or congenital anomalies, steroid use during the first trimester has been considered a risk factor for SGA, preterm birth, or congenital anomalies.30,42-44 Since corticosteroids are often required to manage acute relapses in patients with MS, our findings may reflect real-world clinical practice. Second, the degree of disability due to MS was not assessed because disability scores such as the Expanded Disability Status Scale were not included in the NHIS claims data. Further investigations are warranted to clarify the relationship between disability severity and pregnancy outcomes in women with MS. Finally, the use of the CCI may be a limitation given its original design for mortality prediction. Although it might underestimate the comorbidity burden in the younger population, it was selected for this study as a broadly validated scoring system widely utilized in large-scale health claims-based studies.
In summary, this study evaluated obstetric and neonatal outcomes in women with MS using nationwide claims data. The findings indicate that women with MS are at an increased risk of preterm birth and placenta previa compared with matched controls. Notably, the risk of preterm birth was significantly higher in patients with AMA. Although the overall incidence of complications was relatively low, comprehensive prenatal monitoring remains essential, particularly for pregnant women with MS and AMA. As healthcare providers become more informed about these potential risks, pregnancy in women with MS should be supported and encouraged through individualized multidisciplinary care. Further studies are warranted to explore the underlying mechanisms and treatment-related factors influencing these outcomes.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Korea Disease Control and Prevention Agency (no. 2023-ER0505-02) and a Korea University Guro Hospital Grant (K2512341).
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.