
Abstract
Background:
Natalizumab (NTZ) effectively suppresses clinical and radiologic disease activity in paediatric patients with multiple sclerosis (MS), however, it is unclear whether serum neurofilament light chain (sNfL), a biomarker of neuronal injury, normalizes.
Objective:
To evaluate sNfL response to NTZ in the paediatric setting.
Methods:
sNfL was measured (single-molecule array) in 66 paediatric patients on NTZ for highly active MS in a single-centre between 2007 and 2023. sNfL levels were converted to age-adjusted z-scores for longitudinal assessment.
Results:
sNfL declined significantly on NTZ, however, not all patients achieved normalized levels. Percentage of patients with sNfL < 90th percentile of healthy aged-matched individuals increased from 6.8% initially to 50%, 65% and 75% within 12, 24 and 36 treatment-months, respectively. Higher on-treatment levels were associated with higher baseline levels (B = 0.791, p < 0.001) and John Cunningham virus (JCV) seropositivity (B = 0.286, p < 0.001). sNfL > 97th percentile at 12 treatment-months indicated greater likelihood of disease activity in following year.
Conclusions:
NTZ treatment resulted in a significant reduction in sNfL levels, correlating with its clinical efficacy in paediatric MS. However, higher baseline sNfL concentrations were associated with a prolonged time to normalization. In addition, JCV seropositivity was linked to elevated NfL levels during treatment.
Keywords
Introduction
Paediatric patients with multiple sclerosis (MS) often have a more active inflammatory disease course, generally better attack recovery, overall slower disease progression, yet younger age at disability development, than observed in adult-onset MS.1–3 Lower-efficacy disease modifying therapies (DMTs) often prove insufficient at controlling high disease activity, thus treatment strategies have evolved towards increased use of more effective therapies. 4
Natalizumab (NTZ) is extremely effective at suppressing high disease activity.5,6 It is a humanized monoclonal antibody that targets the cell adhesion molecule alpha4 integrin expressed on leukocytes, disrupting leukocyte-endothelium adhesion and preventing transmigration of lymphocytes across the blood-brain barrier. 7 NTZ is administered as an off-label treatment to paediatric patients and is generally well tolerated. Limiting its use, however, is an increased risk of progressive multifocal leukoencephalopathy (PML) associated with prior John Cunningham virus (JCV) exposure, previous immunosuppressive therapy or prolonged NTZ treatment (>24 months). 8
Neurofilament light chain (NfL) is a structural protein released following neuroaxonal injury and detectable at very low levels in blood of healthy individuals. 9 Although not a pathology-specific biomarker for neurodegeneration, numerous studies have shown that levels are elevated in patients with relapsing-remitting MS and that these levels correlate well with CSF levels and also reflect clinical and subclinical disease activity, treatment response and future disease progression.10–14 Possible benefit for assessing PML risk in NTZ-treated adults has also recently been reported. 15
In this study, we evaluated sNfL in a cohort of paediatric patients treated with NTZ for highly active MS. We assessed whether sNfL normalizes during therapy, if factors influence trajectory, and if levels reflect or predict on-treatment disease activity.
Methods
Cohort
Retrospective study of sNfL in 66 patients treated with NTZ between 2007 and 2023 for highly active MS at the German Centre for Multiple Sclerosis in Childhood and Adolescence, Department of Paediatrics and Adolescent Medicine, University Medical Centre Göttingen, Germany. All patients had a first demyelinating event before age 18 years, an MS diagnosis fulfilling 2017 revised McDonald criteria and one or more serum samples collected during NTZ treatment (mean treatment duration 24 ± 12 months, range 6 to 96 months). 16 Patients were switched to NTZ due to ongoing clinical/subclinical disease on a low-efficacy DMT, or were induced after presenting with high initial lesion counts and evidence of recent active lesions, a severe recent relapse or incomplete recovery after a relapse. 4 Patients received 300 mg NTZ intravenously 4-weekly with the exception of 17 patients: six patients received a weight adapted dose of 5 mg/kg 4-weekly, six patients were initiated on extended dosing (300 mg 5–6 weekly) and five further patients were extended from 4-weekly to 5–6 weekly dosing within 6–18 months of treatment. Cases with positive anti-JCV antibody status at initiation were treated maximally 24 months with NTZ. 8 A positive myelin oligodendrocyte glycoprotein antibody titer were grounds for exclusion. Older cases that presented prior to MOG antibody-testing with a presentation consistent with MOG-associated disease were also excluded.
Clinical and MRI data were obtained from medical records. Clinical evaluations were performed at 6-monthly intervals after NTZ initiation by qualified paediatric neurologists. Cranial MRIs were performed 6-monthly and spinal MRI at least once a year using standardized protocol sequences including axial and sagittal T2-weighted scans, fluid-attenuated inversion recovery (FLAIR) sequences and post-contrast T1-weighted scans. MRIs were compared with previous in-house images for evidence of new/enlarging and/or gadolinium enhancing (Gd+) lesions.
Baseline data refers to data at NTZ initiation. Patients were defined as untreated at NTZ initiation if they had had no prior DMT exposure (n = 22), <3 months treatment with a lower-efficacy DMT (n = 6) or had discontinued a DMT > 3 months before NTZ initiation (n = 1). Treated patients (n = 37) had received > 3 months therapy with either interferon-beta 1a/1b, glatiramer acetate or fingolimod. Baseline T2 lesion counts were ⩽ 3 months and Gd+ lesion counts ⩽ 1 month prior to sampling. JCV serostatus was assessed at baseline and at follow-up visits for possible seroconversion. 17 Expanded disability status scale (EDSS) scores were > 1 month after an acute attack. 18 No evidence of disease activity (NEDA-3) during follow-up on NTZ was defined as no clinical relapse, no evidence of MRI activity (no new/enlarging and/or Gd+ lesions) and no confirmed disability progression since the previous assessment. 19 Alternatively, patients were classified with EDA (evidence of disease activity).
Serum NfL measurement
We analysed 261 serum samples including 59 baseline samples collected <3 months before NTZ initiation and 170 samples collected during first 2 years of treatment (Supplemental Figure 1). Sample availability in ascending order: two (n = 15), three (n = 12), four (n = 15), five (n = 16), ⩾ six samples (n = 8). Samples were collected according to standard operating procedures in serum separator tubes, transferred to the laboratory, centrifuged at 2000 g for 10 minutes, aliquoted then stored at either −20°C or −80°C until analysis on a single-molecule array (Simoa®) HD-X Analyzer. Analysis was done in duplicate in accordance with manufacturers’ instructions applying appropriate standards and internal controls, and blinded to clinical and MRI data. Inter-assay coefficient of variation (CV) was <10% and mean CV between duplicate sample measurements was 7.2%. Samples with a CV > 20% were remeasured or excluded. All measured concentrations were above the threshold for the functional lower limit of quantification (LLOQ) (1.6 pg/mL; dilution 1:4).
Standard protocol approvals, registrations, and patient consents
This study received approval from the local ethics committee. All patients and their legal guardians provided written informed consent for the collection and use of medical data and biological fluids for research purposes.
Statistical analysis
Descriptive statistics report counts and percentages, median and interquartile range (IQR) for skewed distributions, otherwise mean and standard deviation (±SD). For analysis, we converted raw sNfL values to an age-adjusted z-score using sNfL references provided on the online platform by Abdelhak et al. 20 (https://shiny.dkfbasel.ch/baselnflreference-for-kids). Reference values ref-lect sNfL findings of 2667 healthy children aged 0–18 years as analysed on a Quanterix Simoa HD-X Analyzer. Cut-off levels for reported baseline sNfL-terciles were lowest: 5.2–17.3 pg/mL, n = 19, intermediate: 17.4–58.2 pg/mL, n = 20, and highest: 60.0–501.9 pg/mL, n = 20. We used univariable and multivariable linear regression to assess predictors of baseline log10sNfL and linear generalized estimating equation (GEE) to assess predictors of longitudinal sNfL z-scores. For GEE analysis we used an exchangeable working correlation matrix, missing data was not imputed. Four models were analysed: (1) baseline characteristics (sex, age, BMI, JCV status); (2) baseline disease activity and treatment status (recent relapse, Gd+ lesions, EDSS, corticosteroid treatment, lower-efficacy DMT); (3) baseline sNfL z-score and (4) NTZ dosing interval controlling for sex, BMI, JCV status, baseline treatment status and Gd+ lesions. We analysed the whole cohort and a subset of patients (n = 36) with a more complete dataset (baseline sample plus ⩾ 3 samples during 24 months treatment). We used the Mann–Whitney U test for group level comparisons, and Kaplan–Meier survival curves, re-baselining at 6 months, to assess the cumulative probability of (1) remaining free of disease activity during treatment, and (2) of maintaining NEDA-3 status to 24 months stratified by (a) sNfL-percentile at 12 months (< P90, P90–97, or > P97) and (b) JCV status.
A two-sided p ⩽ 0.05 was considered statistically significant. Analyses were performed using IBM SPSS (version 30; SPSS Inc., Chicago, IL, USA) and graphs created with GraphPad Prism software version 10.2.2.
Results
Baseline characteristics
Baseline characteristics (n = 66, 56% females) are summarized in Table 1. Mean age at clinical onset was 13.3 ± 2.3 years and at NTZ initiation 14.8 ± 2.1 years. All had high baseline disease activity (70% had a recent relapse, 84% > 20 T2 lesions, 81% ⩾ 1 recent active lesion, 85% combined cranial and spinal lesions) and 43% had minimal to moderate disability at NTZ initiation (EDSS 2.0–2.5, n = 14; ⩾ 3.0, n = 14). Eleven patients were JCV positive at initiation and seven seroconverted during therapy (five within 12 months, two at 30 months). Altogether, 54.6% (35/64) had received corticosteroid therapy within 4 weeks of NTZ initiation (one pulse n = 26, two pulses n = 9) and 37 patients were switched from a lower-efficacy DMT at NTZ initiation.
Baseline characteristics of the cohort at NTZ initiation.
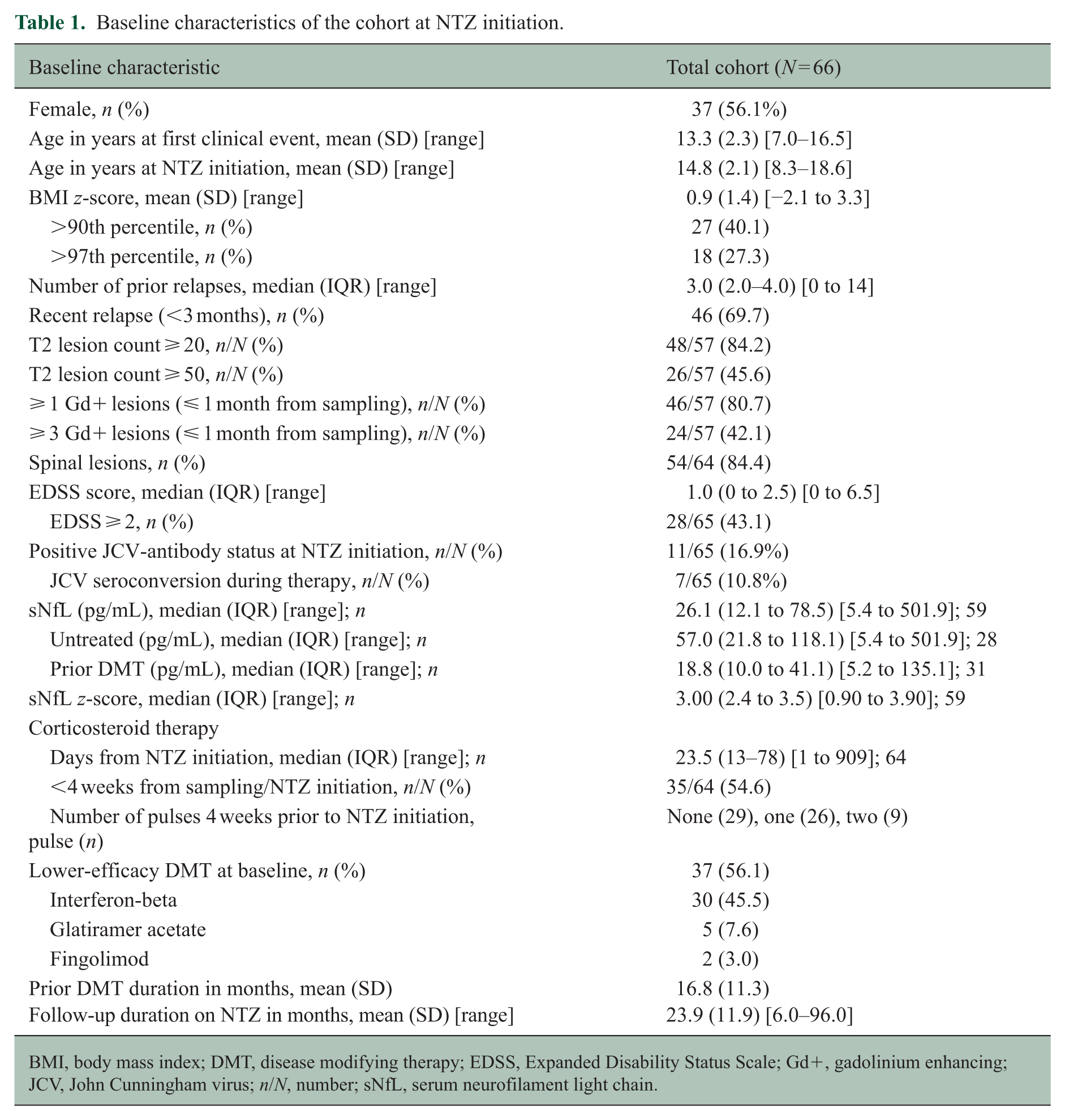
BMI, body mass index; DMT, disease modifying therapy; EDSS, Expanded Disability Status Scale; Gd+, gadolinium enhancing; JCV, John Cunningham virus; n/N, number; sNfL, serum neurofilament light chain.
Baseline serum NfL
Median sNfL at NTZ initiation was 26.1 pg/mL (IQR 12.1–78.5, range 5.4–501.9, n = 59), with 93% above P90 of healthy age-matched individuals (≈6.2 pg/mL) and 76% above P99 (≈12 pg/mL) (Table 1). 20 Untreated patients had higher baseline levels than those switched from a lower efficacy DMT (median 57.0 pg/mL [IQR 21.8–118.1] versus 18.8 pg/mL [IQR 10.0–41.1], respectively; p < 0.001). Higher numbers of recent Gd+ lesions were also associated with higher baseline log-10 sNfL levels (B = 0.038, 95% CI: 0.018–0.057; p < 0.001). Baseline log-10 sNfL was not associated with age, sex, BMI, JCV status, recent relapse, recent corticosteroid therapy or EDSS (Table 2).
Baseline predictors of log10-sNfL at NTZ initiation.
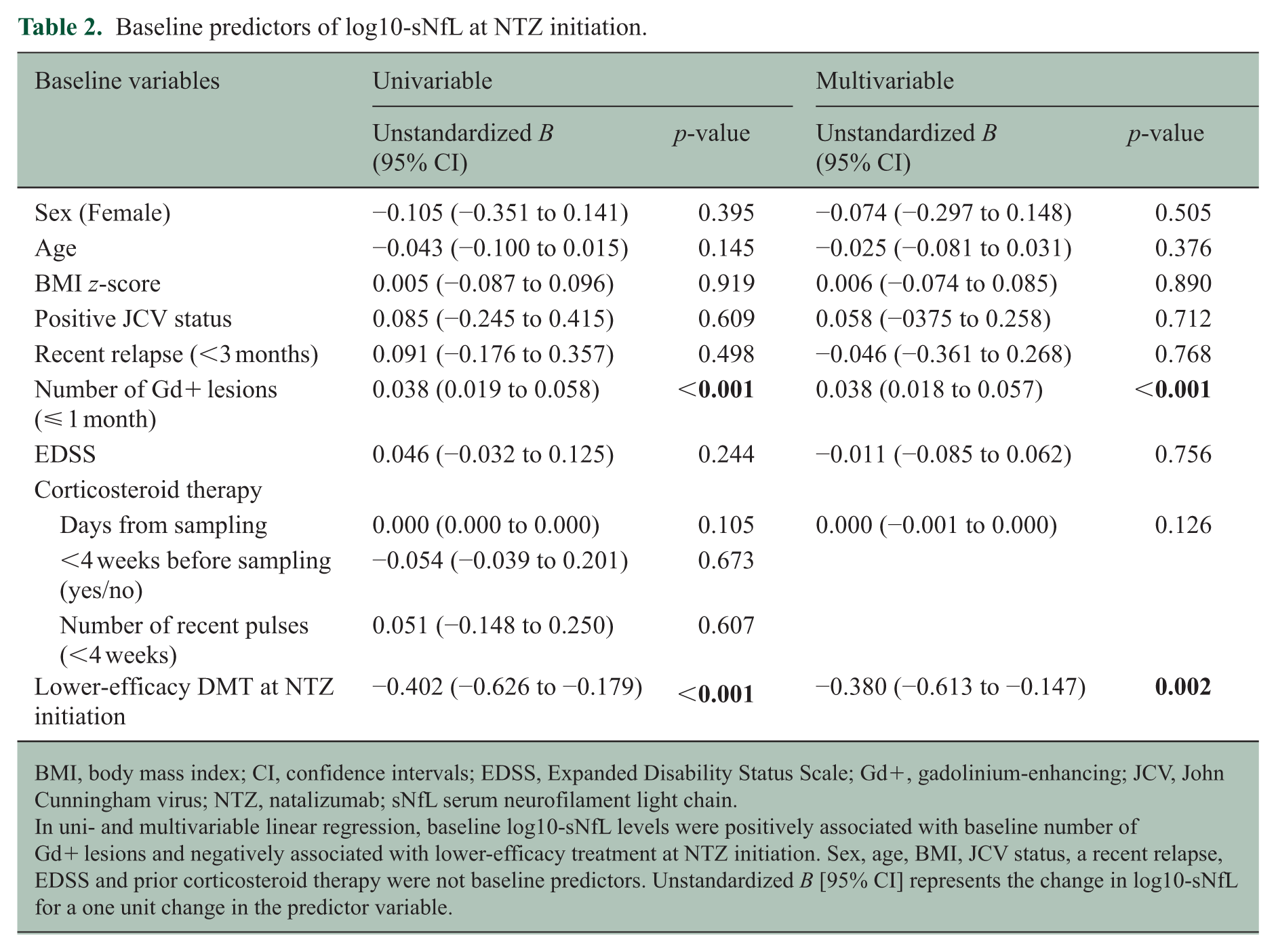
BMI, body mass index; CI, confidence intervals; EDSS, Expanded Disability Status Scale; Gd+, gadolinium-enhancing; JCV, John Cunningham virus; NTZ, natalizumab; sNfL serum neurofilament light chain.
In uni- and multivariable linear regression, baseline log10-sNfL levels were positively associated with baseline number of Gd+ lesions and negatively associated with lower-efficacy treatment at NTZ initiation. Sex, age, BMI, JCV status, a recent relapse, EDSS and prior corticosteroid therapy were not baseline predictors. Unstandardized B [95% CI] represents the change in log10-sNfL for a one unit change in the predictor variable.
Change in serum NfL on NTZ–baseline levels affect normalization
sNfL decreased substantially within the first year of NTZ treatment, with the largest decline within six months of initiation (Figure 1(a)–(c)). Slower decline was still observed over of the second and third year of therapy. Median sNfL decreased from 26.1 to 8.6, 6.2, 5.3 and 4.5 pg/mL after 6, 12, 24 and 30–36 months, respectively (Supplemental Table 1). Only 6.8% of cases were below P90 of healthy age-matched individuals at initiation, this increased to 50% (26/52), 65% (20/31) and 75% (15/20) after 12, 24 and 30–36 treatment-months, respectively (Figure 1(d)). Patients in the highest baseline sNfL-tercile were less likely to fall below P90 within 2 years of therapy compared to those in the lowest baseline-tercile (57% versus 86%, respectively) (Figure 1(d)). In five patients that received prolonged treatment (48 to 96 months), low sNfL levels were sustained throughout the extended period (range 1.7 to 7.2 pg/mL) (Figure 1(e) and (f)). Conversely, in a patient with sub-optimal NTZ therapy adherence over a three-month period, sNfL rose by 41% within the follow-up interval and a relapse occurred.
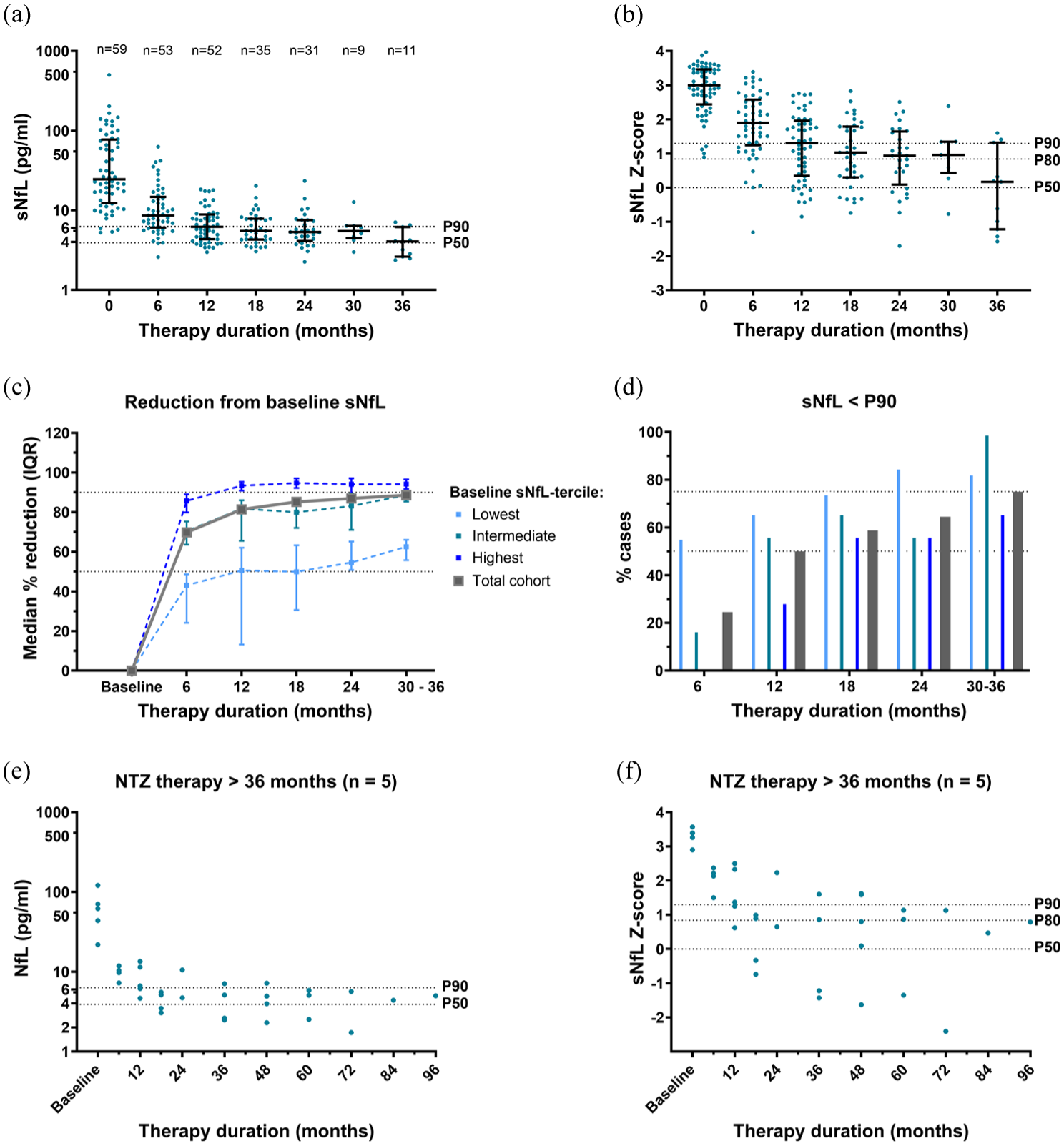
Longitudinal changes in sNfL levels during treatment with NTZ. Changes in sNfL level (a) and z-score (b) in the cohort during NTZ treatment; bars indicate median and IQR, and dotted lines P50, P80, and P90 of healthy age-matched children. (c) shows median percent reduction from baseline sNfL and (d) percent of cases with sNfL below P90 at each 6 month interval, for the whole cohort (grey) and stratified by baseline sNfL-tercile (lowest, intermediate, highest). (e) and (f) show sNfL levels and z-scores of five cases treated with NTZ > 36 months.
Associations with longitudinal sNfL–JCV positive patients at risk for ongoing disease activity
Analysing longitudinal sNfL z-scores of the cohort over two years of treatment we found that higher on-treatment scores were associated with higher baseline z-scores (B = 0.791, 95% confidence interval [95% CI] 0.577–1.004; p < 0.001) (Table 3). This finding was confirmed in subgroup analysis (Table 3). In line with this, on-treatment sNfL z-scores for the whole cohort were negatively associated with DMT treatment at initiation (B = −0.417, 95% CI: −0.811–−0.024; p = 0.038) and positively associated with number of baseline Gd+ lesions (B = 0.059, 95% CI: 0.036–0.083; p < 0.001) (Table 3). Only an influence of Gd+ lesions was confirmed in subset analysis. We also identified a temporal effect of JCV positivity (B = 0.286, 95% CI 0.136–0.435; p < 0.001) (Table 3). JCV positive patients had higher on-treatment levels than JCV negative patients, despite similar baseline values (Figure 2(a)). Included in the analysis were 11 patients that were JCV positive at initiation and 5 that seroconverted (four by 6-treatment-months and one by 12 months). Separate trajectories are shown in Figure 2(b). We found no longitudinal sNfL associations with age, sex, BMI, recent baseline relapse, baseline EDSS, recent corticosteroid therapy or NTZ dosing interval. We cannot exclude that a transient effect of corticosteroid treatment may have been masked by the very high-efficacy of NTZ.
Associations with longitudinal sNfL z-scores over 24 treatment-months with NTZ.
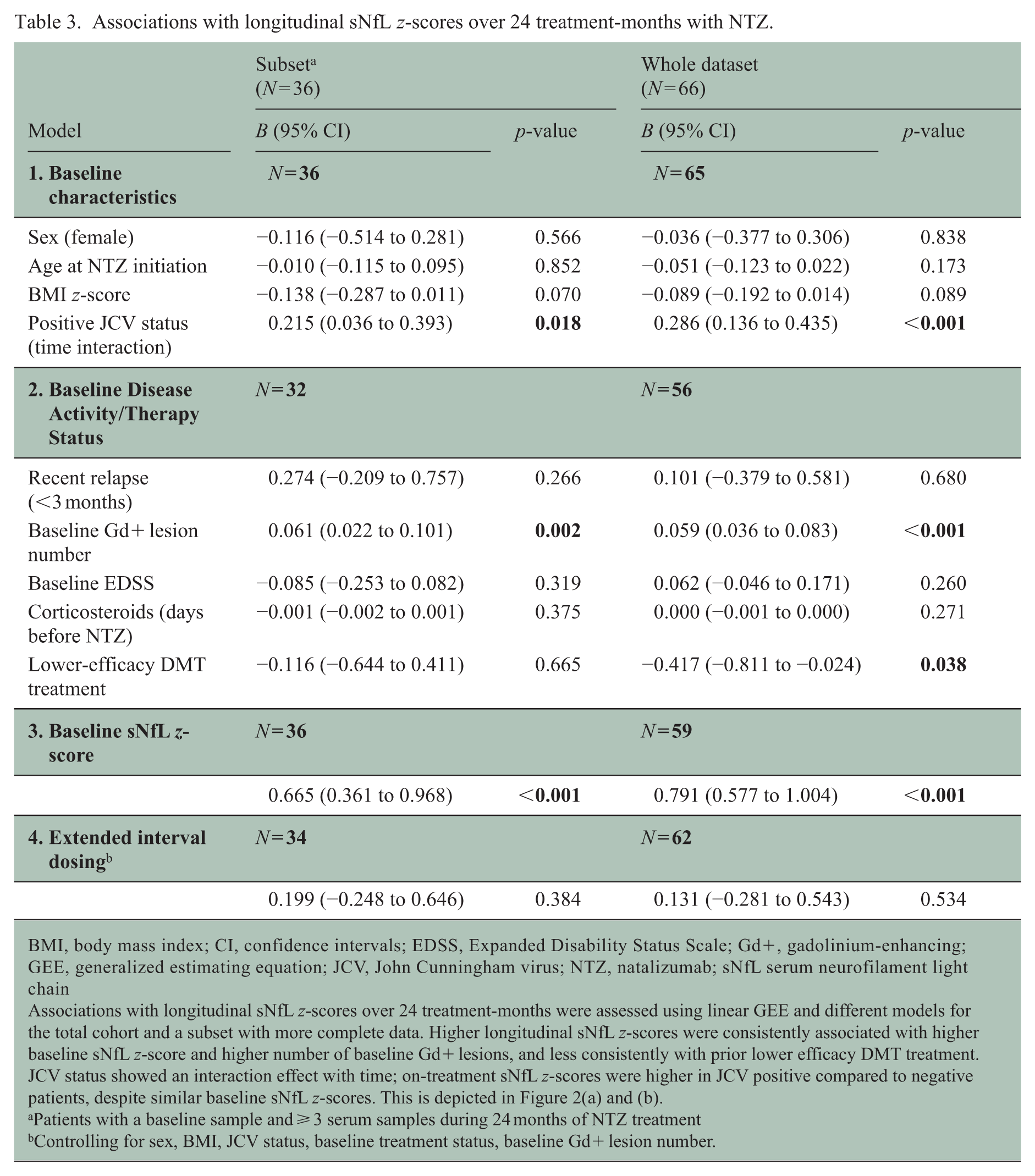
BMI, body mass index; CI, confidence intervals; EDSS, Expanded Disability Status Scale; Gd+, gadolinium-enhancing; GEE, generalized estimating equation; JCV, John Cunningham virus; NTZ, natalizumab; sNfL serum neurofilament light chain
Associations with longitudinal sNfL z-scores over 24 treatment-months were assessed using linear GEE and different models for the total cohort and a subset with more complete data. Higher longitudinal sNfL z-scores were consistently associated with higher baseline sNfL z-score and higher number of baseline Gd+ lesions, and less consistently with prior lower efficacy DMT treatment. JCV status showed an interaction effect with time; on-treatment sNfL z-scores were higher in JCV positive compared to negative patients, despite similar baseline sNfL z-scores. This is depicted in Figure 2(a) and (b).
Patients with a baseline sample and ⩾ 3 serum samples during 24 months of NTZ treatment
Controlling for sex, BMI, JCV status, baseline treatment status, baseline Gd+ lesion number.
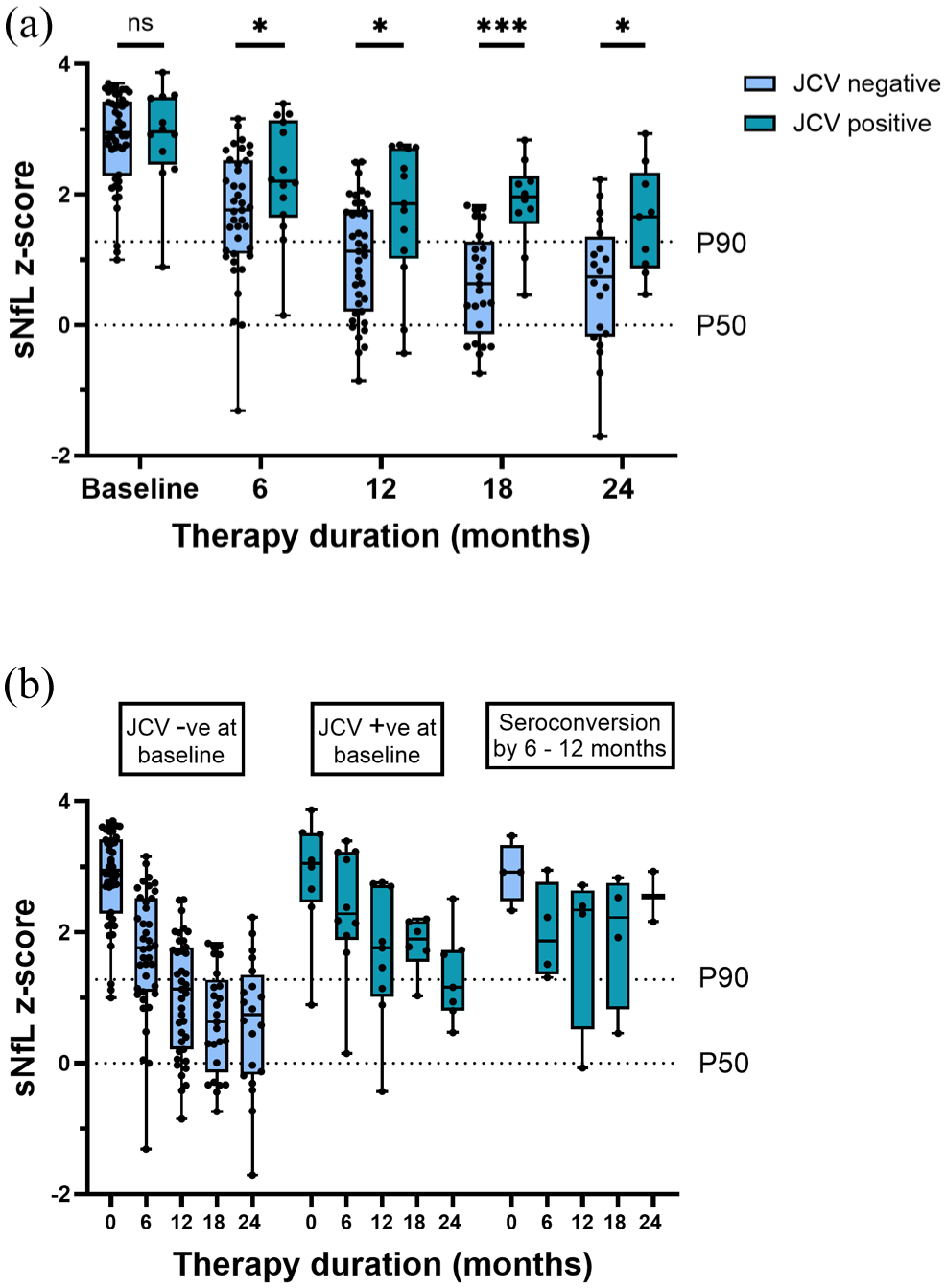
JCV status and sNfL z-scores during treatment with NTZ. (a) and (b) show longitudinal sNfL z-scores in JCV negative and positive patients over 24 treatment-months shown as boxplots with median, interquartile range and minimum/maximum values (whiskers).
Disease activity and sNfL during NTZ treatment
Disease activity occurred predominantly within 6 months of NTZ initiation (new lesions in 12 patients, clinical relapse in one) (Figure 3(a)). At 12 months, 88% (53/60) had NEDA-3, increasing to over 90% in year 2, and 100% in year 3 (n = 20). After re-baselining at 6 months, the estimated cumulative probability of having no evidence of disease activity up to 24 treatment-months was 83% (Figure 3(b)). We found no significant group level differences in sNfL between patients with NEDA-3 and EDA, although a tendency towards higher levels was seen in the latter group (Figure 4(a)). sNfL at 6 months did not predict future disease activity, however, patients with an sNfL > P97 at 12 months were less likely to maintain NEDA-3 status to 24 months (estimated survival probability 61% compared to 85% and 92% for P90–97 and <P90, respectively; Log Rank p = 0.032) (Figure 4(b)). NEDA-3 outcomes were not different between JCV positive and negative patients.
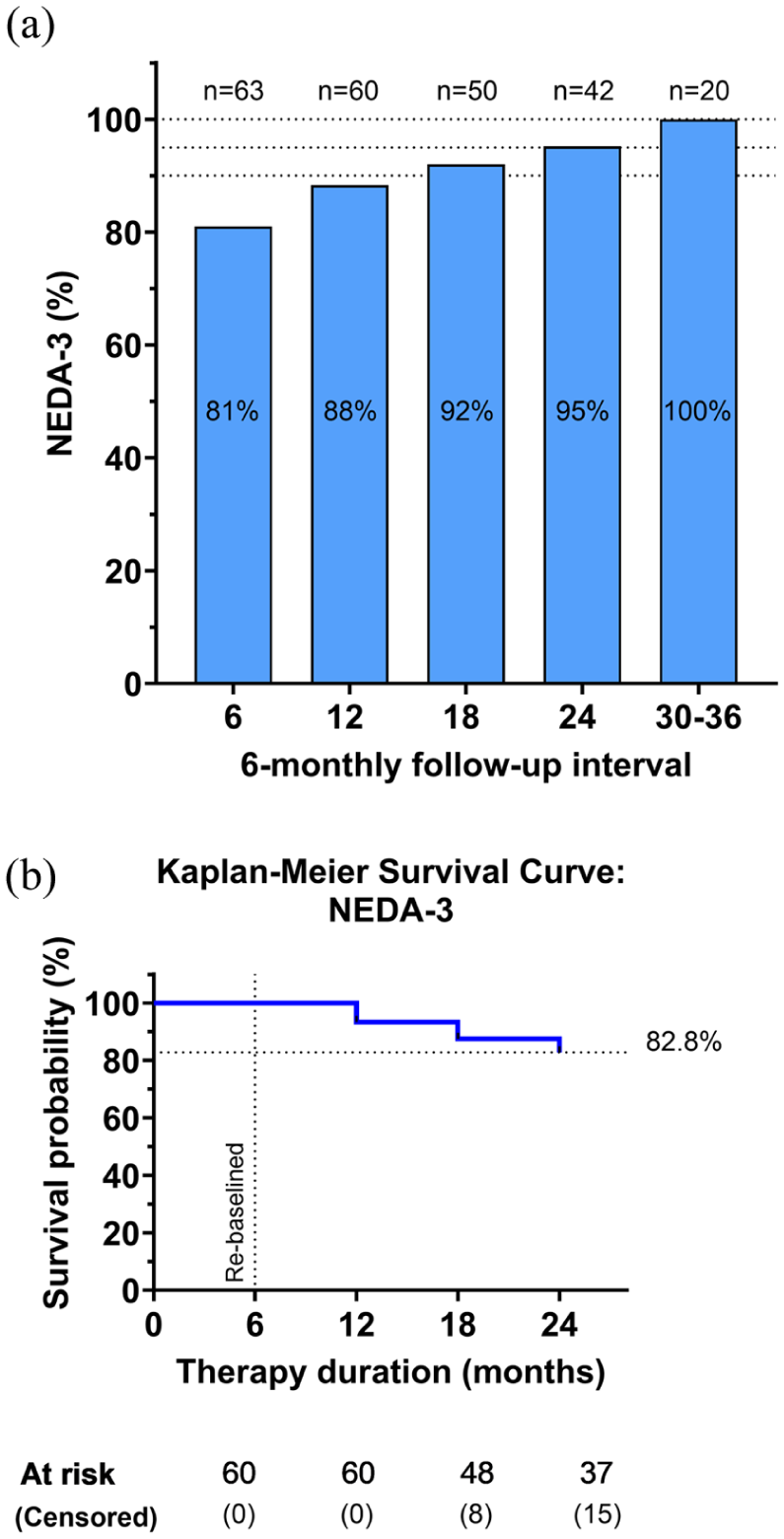
Disease activity during treatment with NTZ. (a) Percent of cases at each 6-montlhy follow-up interval with NEDA-3. (b) Kaplan–Meier survival curve showing the estimated cumulative probability of having no evidence of disease activity up to 24 treatment-months. after re-baselining at 6 months.
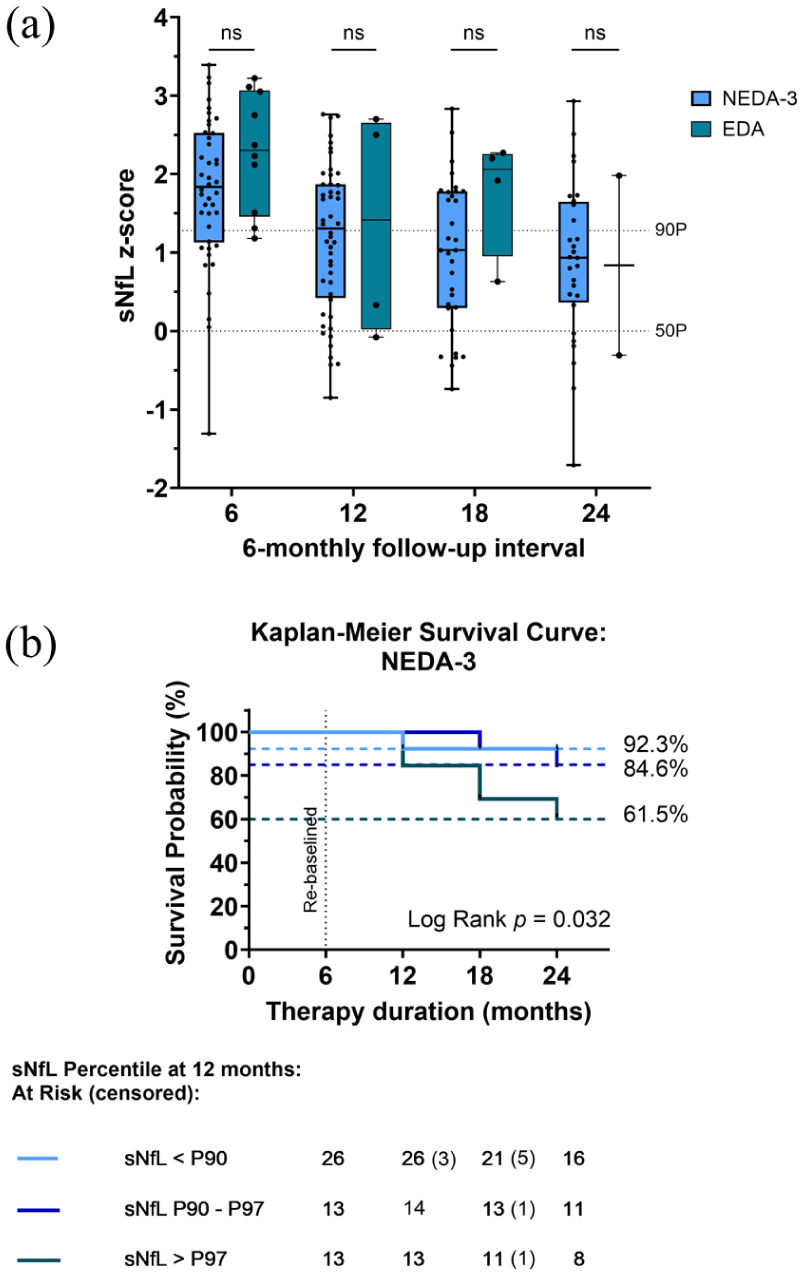
Disease activity and sNfL z-scores during treatment with NTZ. (a) sNfL z-scores for cases with or without disease activity at each 6-monthly follow-up interval; depicted as boxplots with median, interquartile range and minimum and maximum values (whiskers). (b) Kaplan–Meier survival curves with re-baselining at 6 months showing the cumulative probability of maintaining NEDA-3 status over 24 months of NTZ therapy based on sNfL-percentile at 12 months stratified as sNfL < P90, P90–97, and > P97.
EDSS development on NTZ
No patient experienced EDSS progression on NTZ and nearly half (46%) showed some improvement. After 24 months, 78% had an EDSS < 2.0 compared to 57% at initiation.
Discussion
sNfL is emerging as a useful treatment-response biomarker that could greatly benefit young patients with MS. We found a rapid and pronounced decline in sNfL levels in response to NTZ treatment that is maintained over time. Higher baseline sNfL concentrations, however, were associated with a slower normalization trajectory. Interestingly, JCV seropositive patients showed persistently higher on-treatment sNfL levels than seronegative patients.
Consistent with high initial inflammatory activity, we found substantially elevated sNfL levels before NTZ initiation, particularly among untreated patients and cases with high numbers of baseline Gd+ lesions. These findings align with previous paediatric studies.21–24 We found no association between baseline sNfL and a recent relapse or baseline EDSS suggesting that levels were possibly being driven predominantly by very high subclinical disease activity. The findings may also, in part, reflect limited statistical power, the restricted EDSS range, and the relatively crude nature of these clinical measures in capturing subclinical disease activity. While sNfL levels in healthy children are influenced by both age and, to a lesser extent, BMI, neither were predictors of baseline sNfL among our patients. 20 The effect was possibly masked by considerably elevated levels. After NTZ initiation, we observed a rapid, substantial and sustained decline in sNfL with the largest reduction occurring within 6 months. Notably, minimal decline in sNfL was still being observed after 2 to 3 years of therapy. Cases with prolonged therapy (> 36 months) showed consistently low sNfL levels throughout, indicating that NTZ maintains its effect over the long term.
Only limited paediatric MS studies have evaluated sNfL response to DMTs, and none have specifically evaluated NTZ.21–23 Nevertheless, findings indicate that sNfL levels fall in response to therapy with the degree of reduction reflecting DMT efficacy profiles.21–23 In adults with MS, monoclonal antibody therapies have been associated with the greatest on-treatment sNfL reductions, with some studies showing normalized sNfL levels in the majority of NTZ-treated patients within 12 months of initiation.14,25,26 sNfL levels did not normalize as quickly in our cohort. Baseline sNfL levels in our study, however, were higher than those reported in the adult studies, and as we found that higher baseline levels were associated with higher on-treatment levels, this may have contributed to the difference. 25 High baseline levels likely reflect more extensive neuronal damage, both focal and diffuse, and greater immune system activation, all of which may take longer to resolve or suppress during treatment.
An interesting finding in our study was that JCV positive patients had higher sNfL levels on NTZ than seronegative patients, irrespective of baseline level. We found no difference in on-treatment disease activity to explain the difference. JCV positive patients with impaired cellular immunity are at greater risk of developing PML. 8 In seropositive patients with no prior immunosuppressant exposure, the risk of PML is low in the first 2 years of natalizumab treatment. 8 However, anti-JCV antibody titers increase over time and as viral burden increases so does PML risk.27,28 At PML onset, blood NfL levels rise dramatically in the magnitude of 10- to 16-fold.15,29 We did not observe such a massive increase in sNfL nor detect any MRI changes to suggest PML development. This suggest that, even in the absence of PML or prolonged treatment, young patients with JCV positivity may have a vulnerability for persisting neuronal damage on NTZ. Matching our findings, higher sNfL levels in JCV positive compared to negative patients were also shown in a recent study of NTZ-treated adult MS patients without PML. 30 A positive association between sNfL level and JCV antibody titer was also detected in the study.
Consistent with prior paediatric MS studies, clinical and MRI disease activity occurred most commonly in the initial months after NTZ initiation, thereafter only seldomly.5,6,31 Although we found no significant group level differences in sNfL between patients with and without disease activity during treatment, there was a tendency towards higher values in the former group. In one patient with sub-optimal therapy adherence we detected a rapid rise in sNfL coinciding with a relapse, which is consistent with quick return of disease activity due to swift normalization of peripheral immune cells after NTZ discontinuation. 32 It also emphasizes that rising sNfL levels may herald forthcoming clinical and radiologic disease activity. In individuals with stable MS and no clinical or MRI evidence of disease activity, sNfL has also been shown prognostic of future disease activity. 14 Consistent with this, we found higher likelihood of disease activity in the second year of treatment in patients with an sNfL > P97 at 12 treatment-months. In a recent observational study of NTZ-treated adults, future MRI activity but not relapses were predicted by sNfL ratios at 12 months. 33 Greater reduction in sNfL early in the course of NTZ treatment has also been linked to lower subsequent disease activity. 34
Our study has several limitations including retrospective data collection, variable availability of serum samples and follow-up times, and anti-NTZ antibody status was also not assessed. Higher anti-NTZ antibody titers have been associated with lower NTZ concentrations and loss of clinical efficacy. 35
In conclusion, we show that NTZ rapidly reduces sNfL levels in young patients with high inflammatory activity, and sustains the effect over time. Rate of normalization was influenced by baseline levels. Interestingly, JCV positive patients were identified as a sub-group with increased vulnerability for persisting neuroaxonal damage on NTZ, even in the absence of prolonged NTZ treatment. This finding requires validation in future studies. sNfL did not reliably reflect actual on-treatment disease activity, but showed possible predictive potential for future activity. Findings support the growing body of research demonstrating utility of sNfL as a biomarker for monitoring treatment efficacy, identifying sub-optimal response and informing personalized therapy decisions.
Supplemental Material
sj-docx-1-msj-10.1177_13524585261450816 – Supplemental material for Serum neurofilament light chain in paediatric patients treated with natalizumab for highly active multiple sclerosis
Supplemental material, sj-docx-1-msj-10.1177_13524585261450816 for Serum neurofilament light chain in paediatric patients treated with natalizumab for highly active multiple sclerosis by Brenda Huppke, Marie-Christine Reinert, Wiebke Stark, Jutta Gärtner and Peter Huppke in Multiple Sclerosis Journal
Supplemental Material
sj-docx-2-msj-10.1177_13524585261450816 – Supplemental material for Serum neurofilament light chain in paediatric patients treated with natalizumab for highly active multiple sclerosis
Supplemental material, sj-docx-2-msj-10.1177_13524585261450816 for Serum neurofilament light chain in paediatric patients treated with natalizumab for highly active multiple sclerosis by Brenda Huppke, Marie-Christine Reinert, Wiebke Stark, Jutta Gärtner and Peter Huppke in Multiple Sclerosis Journal
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: B.H. reports no disclosures. M.-C.R. reports no disclosures. W.S. reports no disclosures. J.G. reports fees for lectures and consultancy fees from Novartis, and Roche. P.H. reports honoraria for talks from Biogen and Acadia.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data availability statement
Anonymized data will be made available by request from any qualified investigator. Please submit such requests to the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.