
Abstract
Background:
Motor rehabilitation effectiveness in progressive multiple sclerosis (PMS) remains uncertain. We assessed whether task-oriented (TO) rehabilitation, with or without non-immersive virtual reality, improves upper limb function in PMS and evaluated magnetic resonance imaging (MRI) changes related to motor performance.
Methods:
Eighty-one progressive multiple sclerosis patients on B-cell depleting therapy were randomized to task-oriented rehabilitation with virtual reality (TO-VR), TO rehabilitation, or passive mobilization (CG) for 8 weeks. Upper extremity performance was measured with the Nine-Hole Peg Test (9-HPT), Action Research Arm Test (ARAT), AbilHand Test (ABILHAND), and Manual Ability Measure-36 (MAM-36). Upper limb function, neurological status, and MRI were evaluated at baseline, after rehabilitation, and at 3 months.
Results:
Seventy-nine patients completed the study. No difference was observed in 9-HPT, but in the whole sample, ABILHAND improved post-treatment (p < 0.001), and ARAT improved on the left side (p = 0.014, false discovery rate adjusted p = 0.084). Additional gains appeared in several neurological tests. Brain volumes, morphometry, and diffusion indices were unchanged, while functional MRI showed increased connectivity post-treatment in TO-VR and TO groups, but not in CG. Connectivity changes were correlated, in particular, with clinical amelioration (ABILHAND) in both TO-VR (r = 0.54, p = 0.013) and TO groups (r = 0.50, p = 0.035).
Conclusion:
In PMS treated with high-efficacy therapy, TO rehabilitation, particularly when combined with VR, can improve motor function, inducing functional gains and plasticity in cerebral networks.
Keywords
Introduction
Physiotherapeutic interventions are fundamental for managing symptoms and improving the quality of life in people with multiple sclerosis (PwMS).1,2 While most rehabilitation efforts focus on balance, gait, and lower limb strength, upper limb dysfunction (ULD) is a highly prevalent but often underrecognized issue, affecting more than 70% of PwMS. 3 Despite its clinical relevance, ULD has been relatively underexplored in MS rehabilitation research. 2 Few studies have addressed upper limb recovery in PwMS, suggesting that task-oriented (TO) rehabilitation might be able to induce structural and functional brain changes associated with motor improvement.4–6 TO rehabilitation involves practicing meaningful, goal-directed activities that closely simulate everyday tasks, fostering motor learning through repetition and active engagement. When integrated with virtual reality (VR), this approach may enhance outcomes by increasing motivation, delivering real-time multisensory feedback, and enabling intensive, progressively challenging training tailored to individual capabilities. 7 However, the benefits of physiotherapy in advanced progressive MS remain inconsistent.8,9 Possible explanations include older age, comorbidities, greater structural damage, and diminished neuroplasticity, which may all reduce recovery potential. 10 Moreover, a key factor contributing to these variable outcomes may be the presence of ongoing, uncontrolled inflammation, which can interfere with mechanisms of neuroplasticity and reduce the brain’s capacity to respond to rehabilitation. 11 Many prior studies have enrolled heterogeneous cohorts with varying disease activity and treatment regimens, complicating the interpretation of rehabilitation efficacy. 12
Advanced neuroimaging techniques have been used to assess the effects of rehabilitation, having highlighted the potential for rehabilitation-induced brain plasticity in MS. 13 Resting-state functional magnetic resonance imaging (rs-fMRI), which maps spontaneous fluctuations within intrinsic brain networks, diffusion magnetic resonance imaging (MRI), which evaluates white matter microstructure, and volumetric analysis of brain volumes have revealed functional and structural changes following motor training.12,14
To clarify the true rehabilitative potential of ULD in progressive MS, we conducted a randomized controlled trial using advanced MRI, focusing on PwMS treated with B-cell-depleting therapies, comparing intensive TO upper limb rehabilitation with non-immersive VR, intensive TO therapy without VR, and passive upper limb mobilization.
This study addresses progressive multiple sclerosis by focusing on patients receiving effective disease-modifying therapy, examining upper limb function, an aspect often overlooked in clinical assessment, and comparing different rehabilitation approaches, with particular attention to their potential impact on functional reorganization in a central nervous system (CNS) affected by long-standing disease. The authors had a previous positive experience with TO rehabilitation in multiple sclerosis, 5 and the working hypothesis was that the addition of a VR treatment could be followed by greater clinical or MRI changes.
Material and methods
Study design and population
This was a multicenter, double-blind, and randomized controlled study, supervised by a Contract Research Organization (CRO) that oversaw randomization, monitored recruitment progress, and ensured strict adherence to the approved protocol across different centers. The study was approved by the Ethics Committee of Istituti Clinici Scientifici Maugeri IRCCS of Pavia (approval no. 2510CE), supported by the Italian Ministry of Health and registered in ClinicalTrials.gov (ID NCT06894940). Written informed consent was obtained by the principal investigator of each clinical center from all participants before enrollment. Personal information of enrolled participants was pseudonymized and securely stored, with access restricted to authorized study personnel to ensure confidentiality throughout the trial. Main inclusion criteria were as follows: (a) age 25–65 years; (b) right-handedness; (c) diagnosis of active primary progressive or secondary progressive MS, treated with B cells depleting agents for at least 6 months (ocrelizumab, rituximab or ofatumumab); (d) Expanded Disability Status Scale (EDSS) 3–7; and (e) Mini-Mental State Examination (MMSE) ⩾ 24. Exclusion criteria included (a) history of a cardiovascular disorder or any other disease that can hamper active participation in the study and (b) contraindication to perform MRI examinations.
Given that subtle ULD and related changes in CNS organization may be present even in patients with near-maximal scores on standardized upper limb assessment scales, no minimum baseline level of upper limb impairment was required for inclusion.
Rehabilitation protocols
Patients were randomized into three groups using the Blockrand algorithm implemented in R. A restricted randomization method with a fixed block size of six was employed to ensure balanced allocation across groups. No stratification factors were used.
The overall duration of the intervention period (8 weeks), session frequency (three times per week), and session length (90 minutes) were identical across groups. Importantly, the time specifically devoted to upper limb rehabilitation (50 minutes per session) was also matched between groups; only the type of upper limb intervention differed.
Task-Oriented + Virtual Reality (TO-VR): Participants received intensive upper limb TO physiotherapy. The first 15 minutes consisted of a preparatory phase aimed at optimizing joint mobility, reducing pain, and spasticity. The next 20 minutes were devoted to TO therapy using object manipulation tailored to motor skills, and then, 30 minutes of targeted upper limb motor activity utilizing the Nirvana System (BTS Bioengineering, Garbagnate Milanese, Italy), a non-immersive VR system, with a wall-projection mode, with exercises of increasing complexity every 2 weeks (in Supplemental Appendix 1). This phase addressed recovery, preservation, and improvement in upper limb strength, motor control, inter-joint coordination, and manual dexterity. Exercises were selected from a dedicated library and adapted to individual needs and residual motor skills, following specific therapeutic criteria ( Supplemental Appendix 2). Then, finally, the last 25 minutes were focused on general rehabilitation addressing active motility, balance, and gait and reduction in spasticity.
Task-oriented (TO): Participants followed the same protocol as TO-VR, except that the 30 minutes of VR training were replaced with active upper limb movements aimed at improving coordination and strength.
Passive mobilization (CG): Patients underwent a passive mobilization protocol of the upper limbs. The first 15 minutes and the last 25 minutes mirrored the other groups’ general rehabilitation, while the remaining 50 minutes were dedicated to passive mobilization and stretching of the upper limbs.
A no-treatment control group was not included, as withholding rehabilitation was considered ethically inappropriate, and the study was designed to compare active rehabilitation approaches.
Clinical and behavioral assessments and statistical analysis
All patients underwent clinical and behavioral evaluations with brain MRI at baseline (T0), immediately after the rehabilitation program (T1), and 3 months later (T2). Outcome assessors and the statistician performing the data analysis were blinded to group allocation.
At the beginning of the study, the coordinating center (Pavia) organized a training course to ensure homogeneity in the collection of clinical and MRI data, and a CRO conducted monitoring visits every 6 months to assess the quality of the data.
Upper limb performance was assessed using (a) Nine-Hole Peg Test (9-HPT); 15 (b) Action Research Arm Test (ARAT); 16 (c) 23-item AbilHand Test (ABILHAND) scale; 17 and (d) Manual Ability Measure-36 (MAM-36). 18
General neurological evaluation included the following measures: (a) EDSS; 19 (b) Functional Independence Measure (FIM); 20 (c) Timed 25-foot walk test (T25FW); 21 (d) 12-Items Multiple Sclerosis Walking Scale (MSWS-12); 22 (e) Trunk Control Test (TCT); 23 and (f) Modified Fatigue Impact Scale (MFIS). 24 Cognitive, psychological, and ecological measures were evaluated through the Brief International Cognitive Assessment for MS (BICAMS), 25 the Hospital Anxiety and Depression Scale (HADS), 26 and the SF-36 score. 27
The sample size was calculated for our primary outcome (9-HPT) to compare the change from baseline to the end of treatment in the time to complete the 9-HPT in Group TO-VR compared with Group TO and Group CG. Specifically, assumptions on effect size were based on a published paper, where we observed a mean reduction of 2.1 seconds (SD = 2.2) in patients treated with an active occupational therapy protocol. 5 Our sample size calculation was based on this result, assuming an additional improvement of 2.1 seconds (for a total reduction of 4.2 seconds) in patients treated with an intensive rehabilitation program plus a high technology protocol with VR. We fixed the power to 80% and the significance level to 5%. We also accounted for an expected dropout rate of 5%.
Analyses were conducted on available data. Regarding the motor and cognitive tests, the proportion of missing values was minimal, and we assumed that these few missing values were missing at random. Clinical results were reported as N (%), mean (SD), or median (IQR) depending on the nature of the variables. The primary endpoint was the change in the 9-HPT across groups. Repeated measures models were performed to study changes over time (T1 vs. T0 and T2 vs. T0). Time was included as a categorical variable with levels T0, T1, and T2, allowing us to estimate changes at each time point without assuming a linear trajectory. All measurements (T0, T1, and T2) were thus included simultaneously in the same model, allowing changes relative to baseline (T0) to be properly estimated. An unstructured covariance matrix was specified to account for within-subject correlations, and appropriate transformations were applied to the dependent variables based on their distributions.
To identify possible differences among groups, interactions with time were assessed. A two-sided α less than 0.05 was considered statistically significant. We have also explored the impact of correction for multiple comparisons using the false discovery rate (FDR) statistical method.
All statistical analyses were performed using Stata version 18.0 (Stata Corporation, College Station, TX, USA).
MRI acquisition protocol
At baseline (T0), immediately after treatment (T1), and 3 months after therapy (T2), all subjects underwent a brain MRI scan with a 3 T scanner. The MRI protocol included 3D sagittal FLAIR (TR = 5000 ms, TE = 393 ms, resolution 0.4 × 0.4 × 1 mm3), 3D sagittal T1 (TR = 2300 ms, TE = 2.96 ms, TI = 919 ms, resolution 1 × 1 × 1 mm3), T2* echo-planar imaging (TR = 720 ms, TE = 33 ms flip angle = 52°, resolution 2.3 × 2.3 × 2.3 mm3, time points = 600) for resting-state fMRI, two-dimensional echo-planar imaging single-shot for diffusion-weighted imaging (TR = 4300 ms, TE = 90 ms, flip angle = 90°, resolution 2 × 2 × 2 mm3, single-shell with 8 unweighted volumes and 80 volumes with b = 1000 m/s2). DWI sequences were acquired with anterior-posterior (AP) phase encoding; another sequence with inverted phase encoding (PA), with the same acquisition parameters and three unweighted volumes, was acquired to correct EPI distortion artifacts.
MRI processing and statistical analysis
Detailed information about MRI pre-processing is reported in Supplemental Material Appendix 3. Rehabilitation-related changes in brain volumes over time were assessed with the longitudinal pipeline of the Computational Anatomy Toolbox for SPM (CAT12) and whole-brain voxel-based morphometry. We assessed gray matter volume changes within groups over time (paired t-test; T1 > T0 and T2 > T1) and compared changes across groups (analysis of variance (ANOVA) with age and sex as covariates).
Diffusion metrics, including fractional anisotropy (FA), radial diffusivity (RD), and mean diffusivity (MD), were calculated. We analyzed white matter tracts of interest, including the bilateral cortico-spinal tract (CST), optic radiation (OR), and the middle cerebellar peduncle (MCP). To investigate cortical microstructure, MD values were also extracted from sensory-motor and visual cortical regions, including the primary motor cortex (M1), somatosensory cortex (S1), dorsal premotor area (PMd), ventral premotor area (PMv), supplementary motor area (SMA), pre-SMA, and visual-related areas, including visual cortex V1, V2, V3, and V4.
Resting-state functional MRI was used to analyze seed-based connectivity (SBC) maps within an extended set of classical resting-state networks, including motor, sensorimotor, and visual ones. We assessed the following: (1) functional connectivity (FC) changes over time within each group and differences of FC changes over time between groups (ANOVA with age and sex as covariates). Finally, we performed a correlation analysis to investigate whether FC changes over time were associated with improvements in clinical variable outcomes.
Results
A total of 81 outpatients were included in the study. In total, 27 were randomized to TO-VR, 27 to TO, and 27 to CG. In total, 79/81 patients completed the rehabilitation protocols, which were well tolerated.
Demographic and clinical characteristics of the study populations at baseline are reported in Table 1. No patients had relapses during the study period, and no new-enlarging T2/FLAIR lesions were documented on brain MRI.
Baseline characteristics of the study populations.
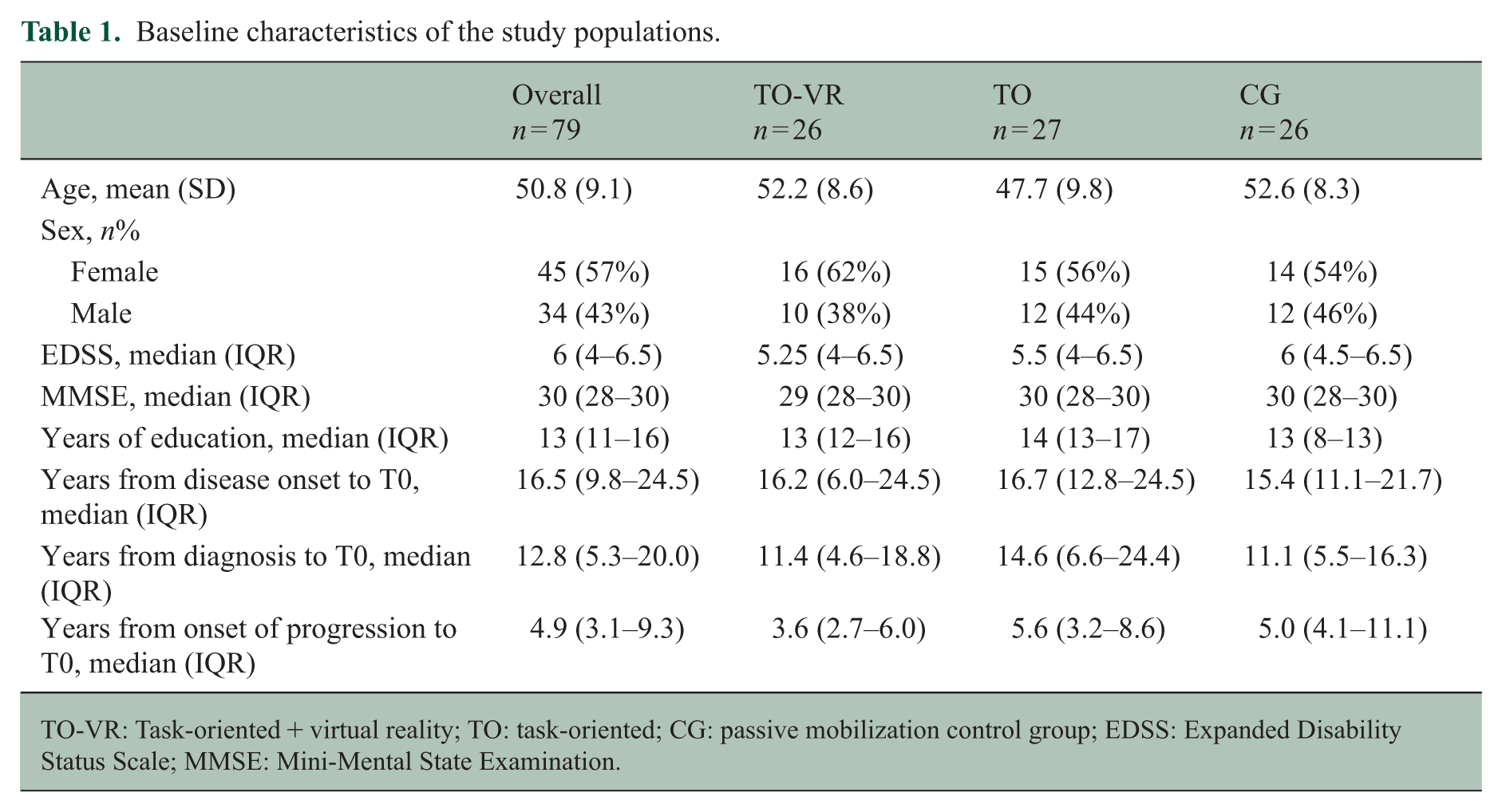
TO-VR: Task-oriented + virtual reality; TO: task-oriented; CG: passive mobilization control group; EDSS: Expanded Disability Status Scale; MMSE: Mini-Mental State Examination.
Upper limb assessment
There were no differences in 9-HPT scores between T1 versus T0 and T2 versus T0 in the right and left hand, and the interaction analysis did not demonstrate any variation between the three rehabilitation protocols (Tables 2A, 2B, and 3). Overall, an increase in ABILHAND scores was observed in the whole sample between T1 versus T0 (p = 0.001), without differences between the three protocols. The increase was not maintained at T2. Similarly, an increase in ARAT scores was noted in the left hand in T1 versus T0 (p = 0.014), with a tendency toward a worsening in CG in T2 versus T1. When we corrected for multiple comparisons, a statistically significant impact of time was confirmed for ABILHAND (p < 0.05), while the FDR-corrected p value for ARAT-left was 0.084.
Upper limb measures.
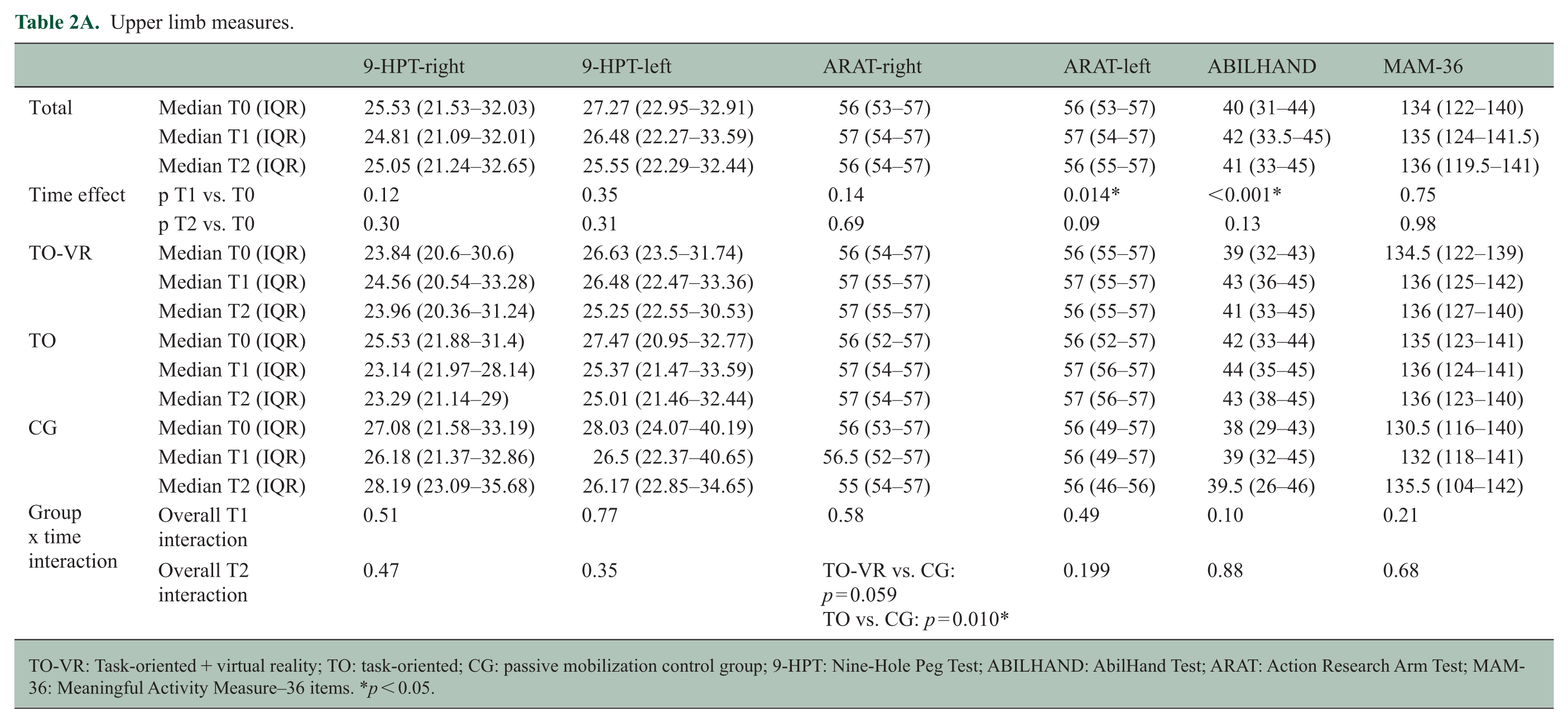
TO-VR: Task-oriented + virtual reality; TO: task-oriented; CG: passive mobilization control group; 9-HPT: Nine-Hole Peg Test; ABILHAND: AbilHand Test; ARAT: Action Research Arm Test; MAM-36: Meaningful Activity Measure–36 items. *p < 0.05.
Upper limb measures—mean (standard deviation, SD) changes over time (T1–T0 and T2–T0) and corresponding |Cohen’s d| for between-group comparisons.
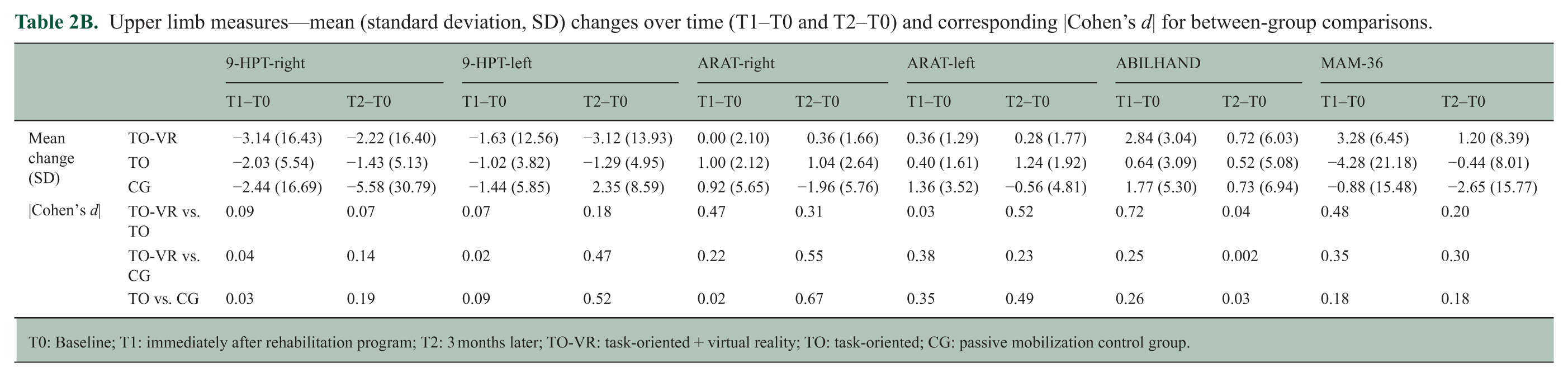
T0: Baseline; T1: immediately after rehabilitation program; T2: 3 months later; TO-VR: task-oriented + virtual reality; TO: task-oriented; CG: passive mobilization control group.
Mean Differences of Upper Limb Evaluation in the whole sample and within group.
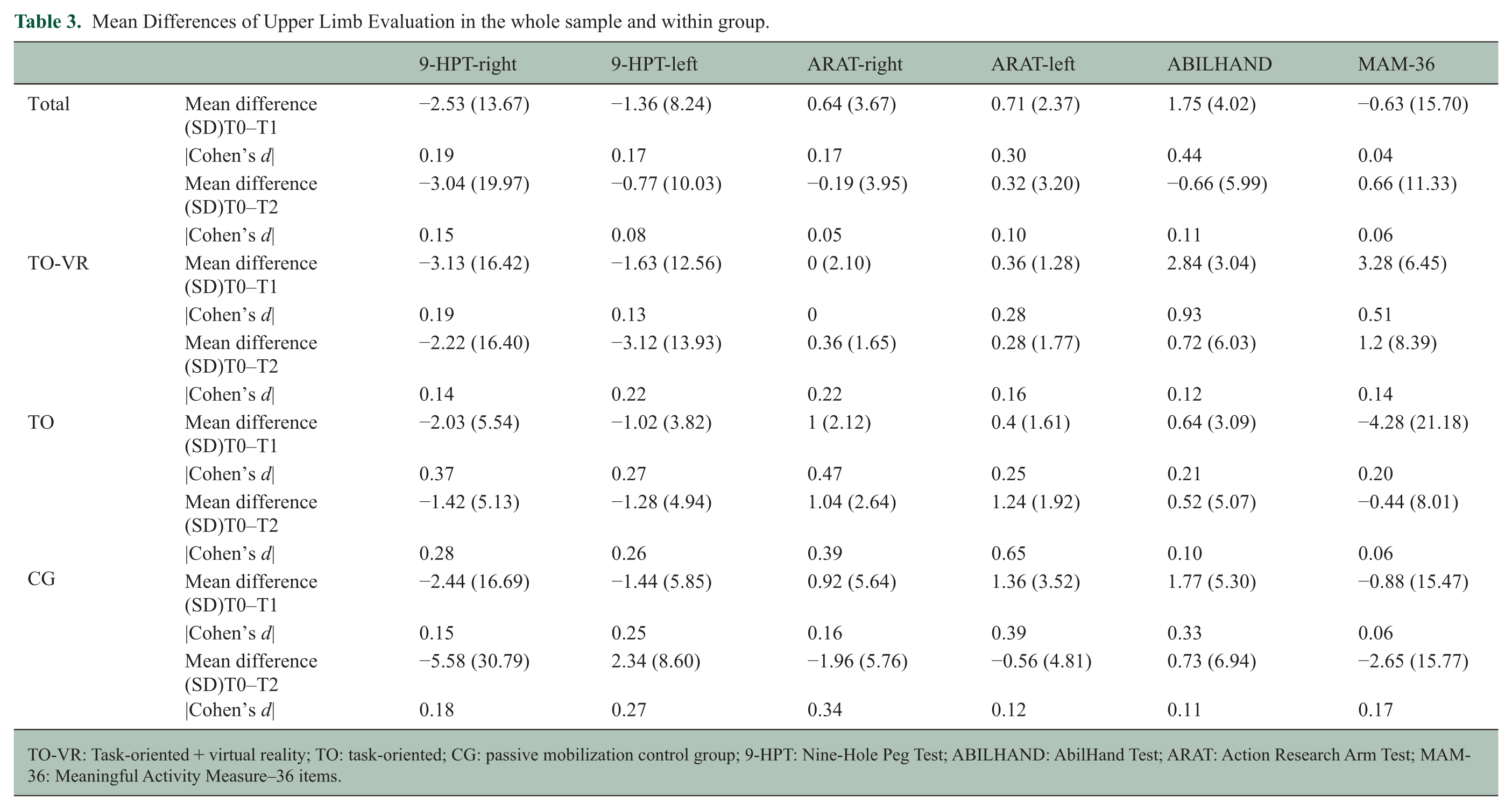
TO-VR: Task-oriented + virtual reality; TO: task-oriented; CG: passive mobilization control group; 9-HPT: Nine-Hole Peg Test; ABILHAND: AbilHand Test; ARAT: Action Research Arm Test; MAM-36: Meaningful Activity Measure–36 items.
For the right hand, regarding the ARAT scores, a protocol-specific effect emerged at T2, a significant improvement was observed in the TO group compared with the passive treatment (p = 0.010), and a trend toward significance was also found when comparing the VR intervention with the passive treatment (p = 0.059). In the overall evaluation using the MAM-36 and in the interaction analysis, no statistically detectable differences were found.
General neurological evaluation
Several measures, including T25FWT, HADS, FIM, and SF-36, showed improvements at T1 compared with T0, but not at T2. No effects emerged in the interaction analyses. For the MSWS-12, differences were observed at both T1 versus T0 (p < 0.001) and T2 versus T0 (p < 0.001), with no variations in the interaction test. The TCT did not show changes at any time point. The MFIS revealed differences between T1 and T0 (p < 0.001) and between T2 and T0 (p = 0.002), with no significant interaction effects. The BICAMS, comprising the Symbol Digit Modalities Test (SDMT), the California Verbal Learning Test-II (CVLT-II), and the Brief Visuospatial Memory Test–Revised (BVMT-R), showed improvements at T1 and T2 compared with T0. Interaction analyses indicated differences between-groups TO and CG at T1 (p = 0.007) and T2 (p = 0.022), mainly driven by the California Verbal Learning Test-II (CVLT-II). Detailed results of general neurological functioning evaluation at T0, T1, and T2, including interaction analyses, are reported in Supplemental Appendix 4.
Advanced MRI analyses
Of the 79 patients who completed the study, structural MRI was available for 71, diffusion analysis for 64, and functional MRI for 54 patients, due to scheduling difficulties or technical issues.
The number of patients with available scans for structural, diffusion-weighted, and functional MRI is also reported in Supplemental Appendix 3.
Cortical structural plasticity
No changes in total Gray Matter (GM), White Matter (WM), and cortical volumes were noted during follow-up in any of the three rehabilitation groups (Figure 1). Similarly, voxel-based morphometry did not yield any variation in cortical morphometry. Furthermore, MD within sensorimotor and visual cortical areas, reflecting cortical microstructural integrity, did not change over follow-up in any of the three treatment groups.
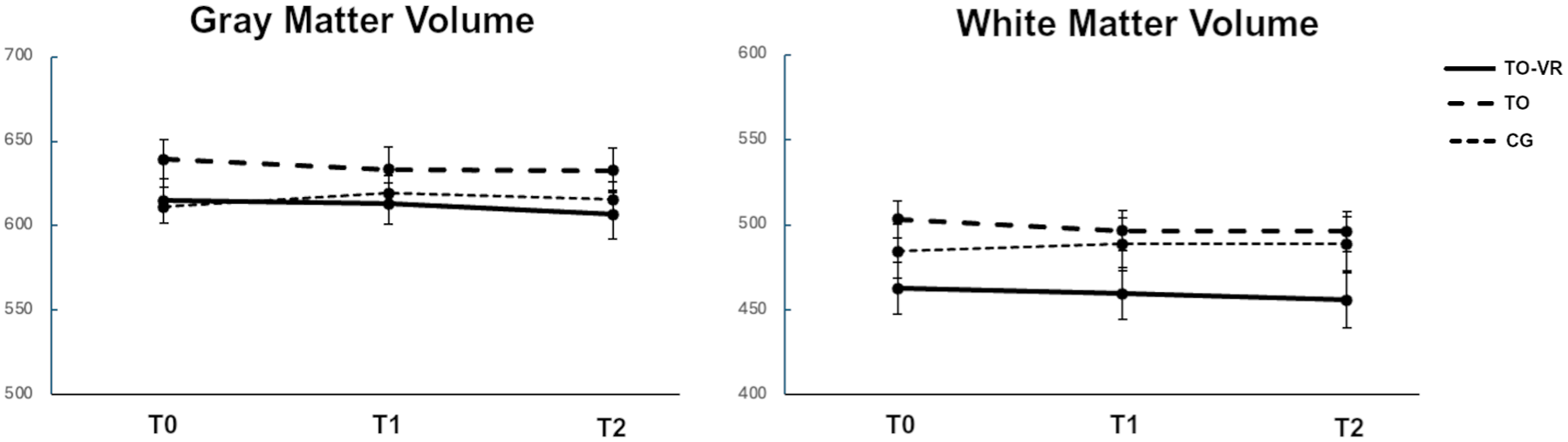
Gray matter and white matter volumes (mL) for each group at each timepoint (T0–T1–T2).
White matter plasticity
Diffusion MRI analysis did not reveal differences in FA, MD, and RD in the bilateral CST and OR and in the MCP. In addition, no differences were found when analyzing whole-brain white matter through tract-based spatial statistics analysis.
Functional plasticity
Several changes in seed base connectivity were noted between T1 and T0 in both TO-VR and TO groups, while no changes emerged in the CG (Figure 2). In the TO-VR group, increased FC was detected in cortical areas, including the cerebellum, the sensorimotor areas, the temporal lobe, and the visual cortex. Peak coordinates are reported in Supplemental Appendix 5. In the TO group, increased FC was observed within the cerebellar and somatosensory network, along with a decrease in FC between the cerebellum and the precentral and postcentral gyri.
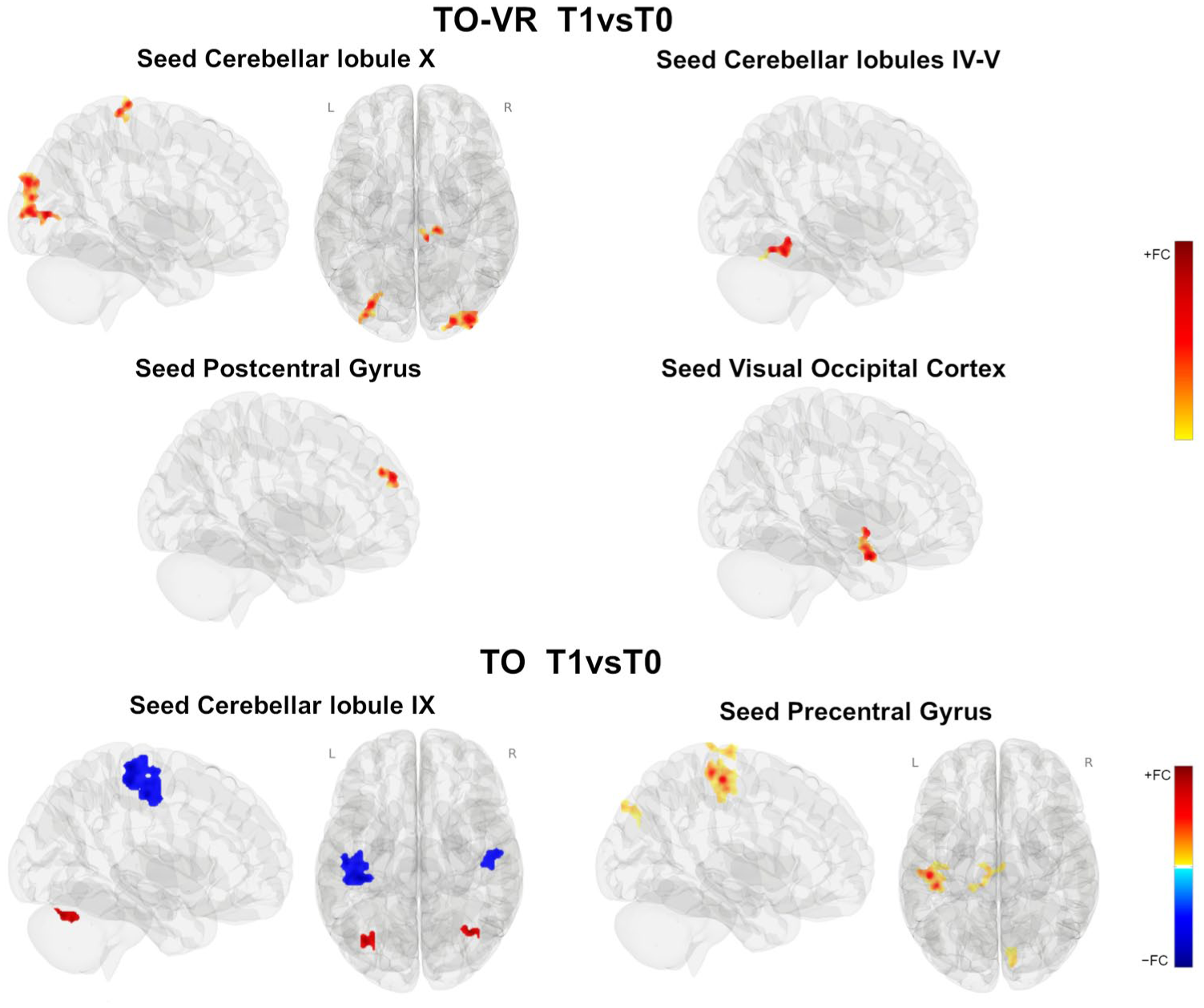
Results of seed-based connectivity analysis (between-conditions contrast T1 > T0 within each group) surviving advanced FWE correction. Color bars indicate positive and negative functional connectivity (FC).
Considering the FC changes between T2 and T0, only the TO-VR group maintained an increase in FC of cerebellar lobule X with a small cluster of voxels covering the lateral occipital cortex (figure not shown).
Considering the interaction analysis time × treatment group (Figure 3), an FC increase (T1 > T0) between the precentral gyrus and the right angular gyrus, lateral occipital cortex, and middle temporal gyrus was observed in TO-VR compared with CG. An increase in FC was also found in TO versus CG in the precentral and postcentral gyri. No differences were detected between TO-VR and TO. All between-groups differences were not maintained at T2.
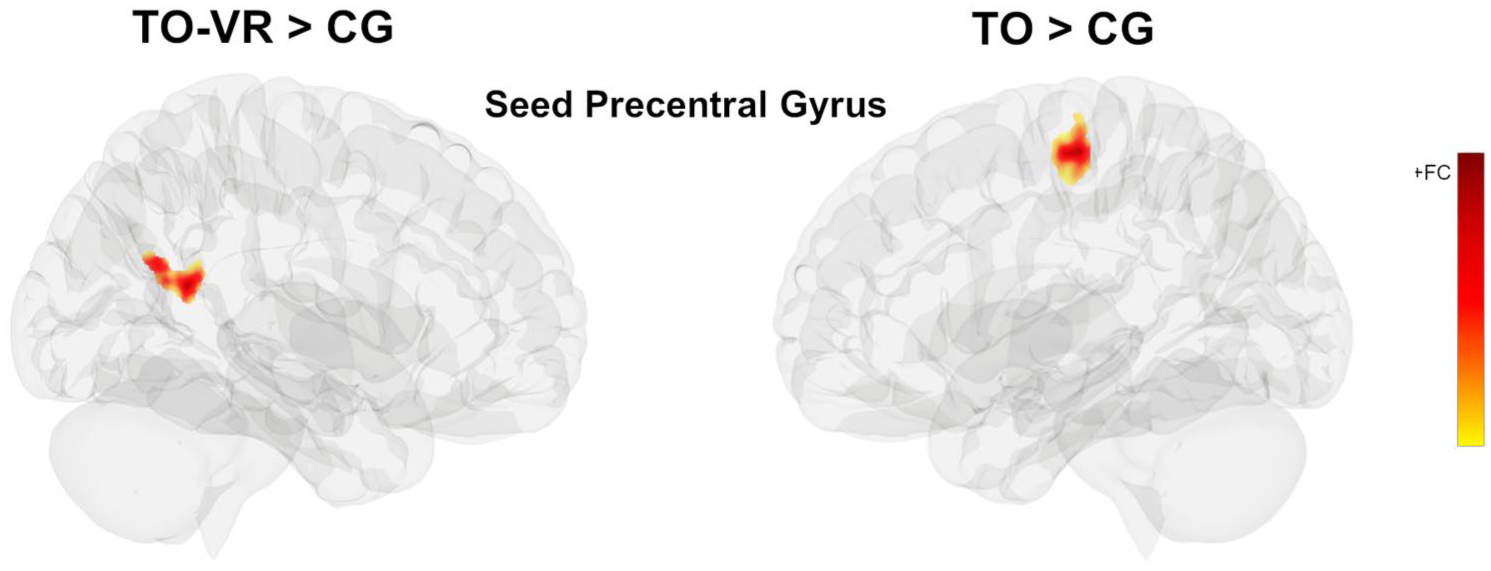
Results of SBC analysis between groups with between-conditions contrast T1 > T0 surviving FWE correction.
Correlation analyses
For group TO-VR, results revealed a significant correlation between FC increase in the occipital cortex with frontal pole and improvement in the ABILHAND score (r = 0.54, p = 0.013). For group TO, results revealed a significant correlation between FC increase in the precentral gyrus with precuneus and the improvement in the ABILHAND score (r = 0.50, p = 0.035).
Discussion
In this randomized study, comparing TO training versus passive mobilization in patients with progressive MS under inflammatory control with high-efficacy treatments (HETs), we found that, despite the absence of significant improvements in the 9-HPT, TO interventions, particularly in association with non-immersive VR, were able to induce clinically significant functional plasticity.
A few studies have reported that TO-VR is effective in improving upper limb motor function in MS patients,28,29 while others have found no additional clinical benefit compared with conventional rehabilitation therapies. 30 The difficulty in comparing results across studies depends on several methodological and clinical factors, including the type of VR used (immersive vs. non-immersive), the technology adopted, outcome measures, intervention intensity and duration, and patient characteristics. Overall, evidence suggests that VR is more effective than no intervention for upper limb rehabilitation; however, its superiority over conventional rehabilitation therapy remains uncertain.29,31,32 In this study, we did not observe statistically significant differences in the 9-HPT, the primary outcome measure of the study. Although the 9-HPT is widely used in clinical trials to assess upper limb impairment, 33 it primarily evaluates finger movements and manual dexterity, and its relevance to daily functional abilities remains uncertain, 34 with some rehabilitation trials in MS reporting improvements in the 9-HPT, 35 while others reporting no significant changes. 4
Our study included a real-world population with progressive multiple sclerosis (mean EDSS around 6), without specifically selecting patients with clinically evident upper limb impairment. The substantial stability of the 9-HPT may, therefore, be attributable also to a ceiling effect of the test, given the relatively mild impairment of our patients. However, other upper limb functional measures other than 9-HPT showed clinical improvements after treatment. Of particular interest is the ARAT, which is widely used to assess upper extremity performance and includes four subscales (grasp, grip, pinch, and gross movement), thus allowing evaluation of both proximal and distal arm and forearm movements and ABILHAND, which is a patient-reported outcome that measures the patient’s perceived difficulty in performing everyday manual activities. 36 Our ABILHAND and ARAT results showed that all three rehabilitation approaches significantly improved upper limb motor performance, even if, after correcting for multiple comparisons, the statistically significant effect of time was confirmed for ABILHAND (p < 0.05) and was reduced for ARAT (p = 0.084). The negativity of the primary endpoint, together with the improvement observed in the other tests, indicates an overall positive result of limited extent (Table 3), indicating a measurable clinical effect with modest yet consistent clinical relevance. Notably, improvements achieved through TO training and VR were substantially sustained at 3 months, while those from passive mobilization tended to decline over time.
Interestingly, the passive mobilization control group showed unexpectedly positive outcomes. Similar findings have been reported in previous studies on upper limb rehabilitation. 5 Passive movements can reduce spasticity 37 and provide continuous stimulation of proprioceptive and cutaneous receptors with subsequent activation not only of the primary somatosensory cortex but also of the primary motor cortex M1. 38 In addition, extensive passive mobilization may exert a thixotropic effect, reducing overall muscle stiffness. 39 Our general rehabilitation program also included trunk exercises, and it is well established that improved trunk control can positively influence upper limb function. 40 Therefore, passive mobilization, when combined with a comprehensive rehabilitation regimen, remains a relevant and valuable therapeutic approach in this population of patients.
Here, we found that TO interventions—and particularly TO-VR—can induce clinically relevant plasticity within the CNS. In particular, TO-VR, which appears to stimulate the visuospatial system to coordinate movement in space, showed an increase in FC in key areas of the sensorimotor and visual systems, namely the cerebellum, postcentral gyrus, visual cortex, and frontal and temporal lobes. Interestingly, in the TO group, no changes were detected in the visual area or frontal lobe; instead, FC changes were observed in the sensorimotor and cerebellar networks, as expected. Conversely, no FC changes were detected in the CG. Altogether, these results show that active rehabilitation induces FC changes that are specific to the networks directly engaged by the rehabilitation protocol.
Two main concerns arise when interpreting FC changes detected by fMRI in the context of MS rehabilitation: first, whether these changes are clinically relevant and associated with improvements; second, how long they persist over time. Here, we found that ABILHAND scores were positively associated with FC increases in key motor areas, suggesting that patients who strengthen functional connections between specific cortical regions are those who achieve the greatest clinical improvement. Although most FC changes were not maintained in the MRI scan performed 3 months after rehabilitation, TO-VR showed a persistent increase in FC between the cerebellum and the occipital cortex. These findings are consistent with previous studies reporting that functional changes after rehabilitation often fade, but they also suggest that more intensive, VR-based rehabilitation protocols might provide a more durable effect than traditional approaches. Importantly, a decline in FC is not always paralleled by a decline in clinical improvement, as also observed in our study. It is possible that other mechanisms, such as peripheral adaptations and compensatory strategies, may support recovery even in the absence of persistent FC changes. Nevertheless, continuous rehabilitation might still be required to maintain both functional reorganization within the cortex and clinical improvement.
Of note, we did not observe any changes in structural MRI, either in macroscopic volumetric measures of gray and white matter or in microstructural parameters within the cortex, particularly MD, which has been proposed as a proxy for cortical integrity. Similarly, no changes were found in white matter tracts, either when analyzing motor and visual tracts specifically or when performing voxel-wise analyses of the whole white matter.
Our findings are in line with previous studies, which reported minimal or absent structural brain changes elicited by motor rehabilitation but detectable functional changes.5,41 This result may reflect the relatively short duration of the intervention and the long disease duration of the enrolled patients, conditions that may limit the extent of detectable structural reorganization. FC measures may capture more subtle and dynamic neuroplastic adaptations occurring in response to rehabilitation, whereas structural and diffusion-based measures may require longer time intervals or more intensive interventions to detect measurable changes. A potential limitation of this study is the absence of a healthy control group, which would have allowed comparison with normative neuroimaging patterns. However, the aim of this study was to investigate longitudinal changes associated with rehabilitation interventions in patients with MS rather than to compare patients with healthy individuals.
Our cohort included homogeneous patients treated with B-cell-depleting therapies, and no new lesions developed during the rehabilitation protocol. Even in the absence of overt inflammation, structural plasticity of both gray and white matter seems very limited, if not absent. This indicates that full control of inflammation is necessary but not sufficient for repair, and that other factors play a fundamental role in determining the extent of repair.
In conclusion, we studied patients with advanced progressive MS and high disability, treated with HETs, a population traditionally considered to have poor potential for brain plasticity. We demonstrated that TO rehabilitation protocols, especially when associated with VR, are feasible, induce a modest but measurable clinical improvement, and are associated with durable and clinically meaningful changes in brain FC.
Supplemental Material
sj-docx-1-msj-10.1177_13524585261450820 – Supplemental material for Task-oriented virtual reality and brain functional plasticity in progressive multiple sclerosis: A randomized controlled trial on upper limb rehabilitation
Supplemental material, sj-docx-1-msj-10.1177_13524585261450820 for Task-oriented virtual reality and brain functional plasticity in progressive multiple sclerosis: A randomized controlled trial on upper limb rehabilitation by Mehrnaz Hamedani, Giada Lombardi, Giacomo Boffa, Caterina Pistarini, Federico Maria Cossa, Elisabetta Capello, Simona Malucchi, Arianna Anselmino, Elena Maria Fiabane, Alessia Di Sapio, Ilaria Poirè, Chiara Sciolla, Cinzia Calautti, Fabio Incollu, Francesca Spada, Antonio Bertolotto, Isabella Springhetti, Antonio Nardone, Riccardo Sollazzo, Giulia Fazio, Ginevra Galetti, Maria Pia Sormani, Andrea Boghi, Marta Ponzano, Matilde Inglese, Maria Cellerino and Gianluigi Mancardi in Multiple Sclerosis Journal
Footnotes
Acknowledgements
The authors would like to thank the Italian Ministry of Health (Ministero Della Salute) for supporting this project through the Ricerca Finalizzata program.
Author Contributions
M.H.: Conceptualization, Protocol writing, Methodology, Data curation, Investigation, Writing—Original Draft, Visualization, and Writing—Review and Editing. G.L.: Methodology, Data curation, Investigation, Writing—Original Draft, Visualization, and Writing—Review and Editing. G.B.: Methodology, Data curation, Investigation, Writing—Original Draft, Visualization, and Writing—Review and Editing. C.P.: Conceptualization, Investigation, and Writing—Review and Editing. F.C.: Conceptualization, Investigation, and Writing—Review and Editing. E.C.: Conceptualization, Methodology, and Writing—Review and Editing. S.M.: Investigation, Data curation, and Writing—Review and Editing. A.A.: Investigation, Data curation, and Writing—Original Draft Preparation. E.F.: Data curation, and Writing—Review and Editing. A.D.: Data curation, Investigation, and Writing—Review and Editing. I.P.: Investigation, and Writing—Review and Editing. C.S.: Methodology, Investigation, and Writing—Review and Editing. C.C.: Investigation, and Writing—Review and Editing. I.S.: Conceptualization, Investigation, and Writing—Original Draft Preparation. F.I.: Data curation, and Writing—Review and Editing. F.S.: Data curation, and Writing–Review & Editing. R.S.: Data curation, and Writing—Review and Editing. A.B.: Methodology, Investigation, and Writing—Review and Editing. A.N.: Conceptualization, resources, Investigation, and Writing—Review and Editing. G.F.: Investigation, and Writing—Review and Editing. G.G.: Data curation, and Writing—Review and Editing. M.P.S.: Conceptualization, Methodology, Formal analysis, and Writing—Review and Editing. A.B.: Methodology, data curation, and Writing—Original Draft Preparation. M.P.: Formal analysis, and Writing—Original Draft Preparation. M.C.: Investigation, Methodology, and Writing—Original Draft Preparation. M.I.: Conceptualization, Methodology, and Writing—Review and Editing. G.M.: Conceptualization, Protocol writing, Methodology, Investigation, resources, Writing—Original Draft, Visualization, Supervision, and Writing—Review and Editing.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financed by Ministero Della Salute, Ricerca Finalizzata 2019, RF 2019 12370447. Open access is supported by the Ricerca Corrente funding scheme of the Ministry of Health, Italy.
ORCID iDs
Data Availability Statement
The data supporting the results of this study are available upon request by a qualified investigator.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.