
Abstract
Background:
Individuals with pediatric-onset multiple sclerosis (POMS) experience higher levels of depressive symptoms compared with those with monophasic acquired demyelinating syndromes (mono-ADSs). Associations among racial identity, marginalization, and depression have not been investigated in these populations.
Objectives:
To determine the relationship among racial identity, neighborhood marginalization, and depression in POMS compared with mono-ADS.
Methods:
Secondary analysis of the Center for Epidemiologic Studies Depression Scale (CES-DC) and racial identity data linked to Canadian Marginalization Index scores for individuals with POMS and mono-ADS recruited from The Hospital for Sick Children. Descriptive and inferential analyses were conducted.
Results:
In POMS (n = 100, female = 65), being racialized was associated with elevated depressive symptoms in POMS (relative risk (RR) = 1.50, 95% confidence interval (CI) = 1.04, 2.15) but not in mono-ADS (RR = 0.83, 95% CI = 0.55, 1.26). Black individuals (n = 11) with POMS had higher odds of living in a neighborhood with the highest quintile of marginalization for material resources (OR = 12.7, 95% CI = 1.96, 82.1) compared with White individuals. Higher depression scores are associated with lower household and dwellings scores (rs = −0.27, 95% CI = −0.52, −0.017) in racialized POMS.
Conclusion:
Racialized identity is associated with elevated depressive symptoms in POMS but not mono-ADS. Racial identity and neighborhood marginalization may influence depression in POMS. Longitudinal studies are needed to verify the direction of these relationships.
Keywords
Introduction
Among individuals with multiple sclerosis (MS), 2%–10% of cases have pediatric-onset (POMS).1,2 Individuals with POMS experience high levels of disease activity and depressive symptoms. 3 Identifying contributing factors to depression can help inform future interventions.
Researchers have consistently identified racial identity as an important determinant of mental health outcomes among children and adolescents, with racialized adolescents facing an elevated risk for chronic mental illnesses in adulthood 4 and perceived racial discrimination associated with depression, anxiety, and decreased self-esteem. 5 Moreover, these mental health outcomes are often shaped by the social, economic, and environmental conditions in which individuals are born, grow, live, work, and age—social determinants of health (SDoH). 6 In healthy children and youth, higher levels of depression are associated with both neighborhood deprivation—limited access to social support and material resources—and inadequate housing and housing instability.7,8 These neighborhood factors and their influence on mental health vary by racial identity. 9
SDoH may have even greater effects on outcomes and experiences in individuals with POMS as a doubly affected vulnerable population (i.e. carrying a diagnosis of a chronic illness and being children) who often do not have agency to make decisions for themselves.10–12 Importantly, fatigue and depressive symptoms worsen through time in POMS but not in children with monophasic demyelinating disorders. 13 This difference may stem partly from experiences related to chronic illnesses: higher levels of anxiety, fatigue, pain, mobility, and environmental restrictions than healthy children.10–12 In addition, the relationships between racial identity, SDoH, and mental health may be intensified in MS populations. Among adults with MS, those living in the neighborhoods with greater deprivation and lower socioeconomic status (SES) were more likely to be Black or Latino American; and those from neighborhoods with greater deprivation had higher severity of depression, fatigue, and anxiety, 14 greater risk for disability progression, 15 and greater burden of comorbidities. 16 Experiences in POMS may differ from adult-onset MS, given the onset of illness in childhood (doubly affected, as described above) and higher levels of disease activity. 17 Therefore, being a racialized child with a chronic illness living in a marginalized neighborhood may have compounding effects leading to poorer mental health outcomes. Thus, understanding these relationships in POMS is needed to tailor strategies to improve mental health in this population.
We therefore aimed to evaluate the relationship among racial identity, neighborhood marginalization, and depression in individuals with POMS compared with those with a self-limited illness with no chronic disability, a monophasic acquired demyelinating syndrome (mono-ADS). Our specific objectives were to (1) compare the associations between racial identity and depression in individuals with POMS and individuals with mono-ADS and (2) compare the associations between neighborhood marginalization, racial identity, and depression in individuals with POMS and individuals with mono-ADS. We hypothesized that being racialized would be associated with elevated depressive symptoms, and being racialized and living in more marginalized neighborhoods would be associated with elevated depressive symptoms in individuals with POMS.
Methods
Participants and procedures
A secondary analysis of data collected as a part of the Neuroinflammatory Disorders Clinic Registry at the Hospital for Sick Children (2012–2024), located in Toronto, Ontario, Canada, was conducted (REB#1000005356). Inclusion criteria for POMS participants were as follows: (1) confirmed diagnosis of MS as determined by the 2017 revised McDonald criteria 18 before the age of 18 years, (2) English as the individual’s first language or at least 2 years of schooling in English, and (3) between 8 and 25 years. The comparator group was individuals with monophasic neuroinflammatory conditions 19 —children who experienced a single episode of neuroinflammation with the same age and language criteria as outlined above. Confirmation of monophasic status included re-evaluation of status a minimum of 1.5 years after data lock (July 2024) and a minimum of 2 years after presentation. Conditions found in the monophasic group can be found in Supplemental Table 1. Participants completed a clinic questionnaire, which included demographic questions and a standardized self-report measure of depression (Supplemental Table 2). Individual variables of each participant were linked to the neighborhood marginalization using postal codes. Participants were not excluded based on clinical outcomes.
Individual outcome
Depressive symptoms
Depressive symptoms were assessed using the Center for Epidemiological Studies Depression Scale-Children’s Rating Scale (CES-DC). This 20-item scale is a valid and reliable measure for children between the ages of 8–18 years. 20 The total score ranges from 0 to 60. The CES-DC has been found to appropriately represent depression as a continuous dimension, with higher scores indicating increasing severity of self-reported depressive symptoms. 21 Although the initial validation of the measure found that scores >15 indicate clinically significant depressive symptoms, the cutoff point indicating elevated depressive symptoms has been found to differ depending on the population. For our sample, the distribution of the CES-DC scores clearly identified two peaks above and below the score of 10. Therefore, based on this distinction, we used the cutoff score of 10 to indicate a higher severity of self-reported depressive symptoms for our analysis. Participant CES-DC scores were measured when they were below 18 years old.
Clinical covariates
Disability was assessed using the Expanded Disability Status Scale (EDSS), a validated, physician-scored measure of disability based on a neurologic examination widely used in MS clinical care and research. 22 The EDSS score ranges from 0 to 10, with higher scores indicating greater disability. The number of relapses was determined by the number of times a participant experienced the appearance of a new symptom or worsening of an old symptom that lasted longer than 24 hours, could not be attributed to fever or intercurrent illness, and was preceded by stability or improvement in the preceding 30 days.
Individual exposure
Racial identity
Racial identity was identified through the self-reported clinic questionnaire and/or through medical chart review. It was then grouped as per the Canadian Institute for Health Information race categories, which include the following: Black, East Asian, Indigenous, Latin American, Middle Eastern, South Asian, Southeast Asian, and White. 23 The categories were used individually as well as a collective “racialized” group that included all participants who did not identify as “White,” due to the smaller group sizes of individual categories.
Environmental exposure
Neighborhood marginalization
Neighborhood marginalization was measured using the Canadian Marginalization Index (CAN-Marg) 2016 with four dimensions of marginalization: (1) household and dwellings, referring to dwelling or housing security; (2) material resources, referring to individual and community access/attainment of basic material needs; (3) age and labor force, referring to seniors, children, and adults who do not have employment income; and (4) immigration and visible minority, referring to recent immigrants and/or people belonging to a visible minority group. 24 This index was developed based on a theoretical framework and is stable across time and place. 24 Higher scores on each dimension indicate greater marginalization. Specific indicators of each dimension can be found in Supplemental Table 3.
Data analysis
Descriptive analyses were performed using JASP (JASP Version 0.18.3). As depression, marginalization, and covariates were not normally distributed as per the Shapiro–Wilk test, Mann–Whitney U tests were performed to estimate the differences. Accordingly, rank-biserial correlations were used to estimate effect size. Spearman’s rho was used to calculate correlations between depression and marginalization. Depression and covariates were analyzed as continuous variables. Depression was also analyzed as a dichotomous variable (CES-DC >10 and CES-DC ⩽10). Marginalization was analyzed as continuous (scores as factor scores from principal component factor analysis) and dichotomous variables (CAN-Marg score = 5 and score <5). 24 Racial identity was dichotomized as White and racialized, the latter group encompassing all non-White racial identity groups. As presentation of elevations of depressive symptoms (i.e. CES-DC >10) is common in our population, Poisson regression with robust standard errors was performed using R (R Version 4.4.2) to test the association between racial identity and elevated depressive symptoms (i.e. CES-DC >10). The log-binomial model was not used because it would not converge. To compare the association in POMS and mono-ADS, an interaction term (i.e. racial identity × diagnosis) was included in the model, which was adjusted for sex, age (continuous), and disability (categorical). Logistic regression was performed to test the association between racial identity and living in the most marginalized neighborhood (CAN-Marg score = 5). To compare the association in POMS and mono-ADS, interaction terms for racial identity and diagnosis (i.e. racial identity × diagnosis) and depression and diagnosis (i.e. racial identity × depression) were included in the model, which was also adjusted for sex and age (continuous). For the regression models, White participants, females, and a diagnosis of mono-ADS were the reference groups. For the Poisson regression with robust standard errors, we report the relative risk, and for the logistic regression, we report the odds ratio for the associations. Pearson chi-square goodness-of-fit tests were also performed for the Poisson models. C-statistics were reported for the logistic models.
Results
Participants included 100 (female = 65.0%, racialized = 57.0%) individuals with POMS and 139 (female = 48.9%, racialized = 59.7%) individuals with mono-ADS (Table 1). Participants with POMS had minimal to no disability with a median EDSS of 1.5 (interquartile range (IQR) = 1; Q1 = 1, Q3 = 2). Participants with mono-ADS had no functional disability with a median EDSS of 1.0 (IQR = 1.5; Q1 = 0, Q3 = 1.5).
Demographic information and outcomes of participants.
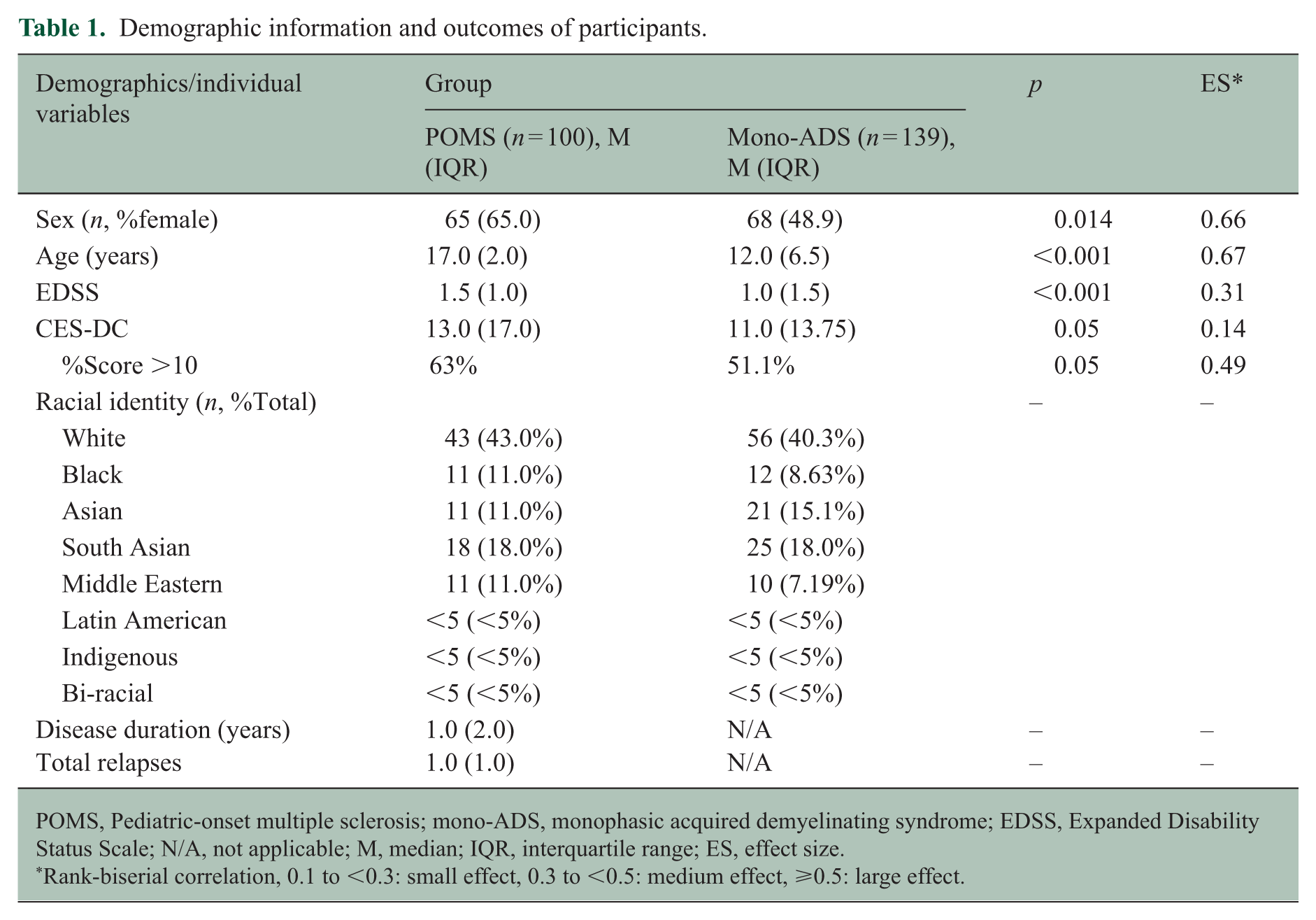
POMS, Pediatric-onset multiple sclerosis; mono-ADS, monophasic acquired demyelinating syndrome; EDSS, Expanded Disability Status Scale; N/A, not applicable; M, median; IQR, interquartile range; ES, effect size.
Rank-biserial correlation, 0.1 to <0.3: small effect, 0.3 to <0.5: medium effect, ⩾0.5: large effect.
Depressive symptoms and neighborhood marginalization in POMS and Mono-ADS
Individuals with POMS had higher depression scores (ES = 0.14, p = 0.05) and EDSS (rank-biserial correlation = 0.31, p < 0.001) compared with those with mono-ADS (Table 1). In the POMS cohort, 63.0% of the participants scored more than 10 on the CES-DC, while 51.1% of individuals with mono-ADS scored more than 10. The CAN-Marg scores did not differ between the two cohorts. In the POMS cohort, there were no differences in measured clinical characteristics between individuals with POMS who scored more than 10 and those who scored 10 or lower (Table 2).
Differences in clinical characteristics between individuals with POMS who scored more than 10 and those who scored 10 or lower.
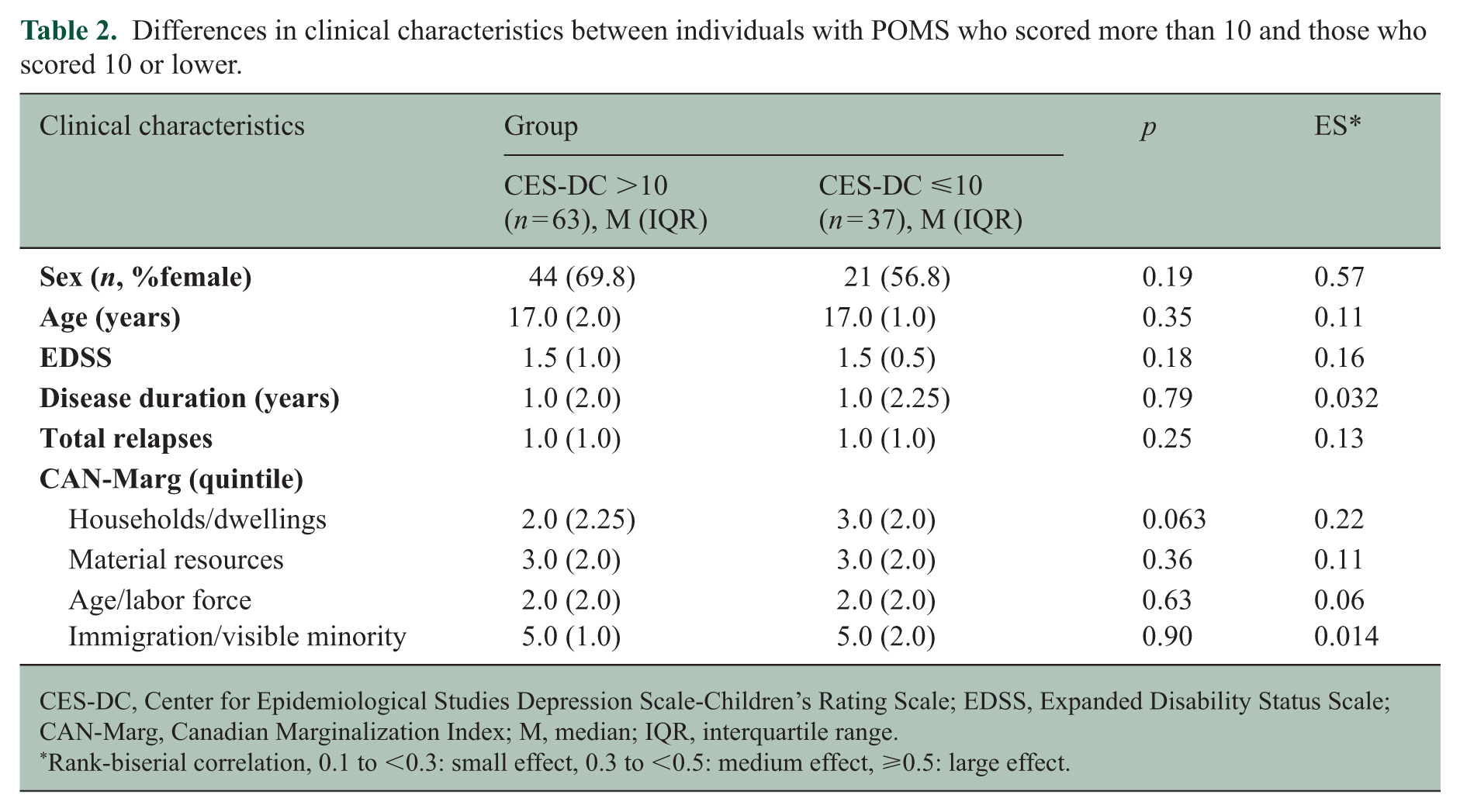
CES-DC, Center for Epidemiological Studies Depression Scale-Children’s Rating Scale; EDSS, Expanded Disability Status Scale; CAN-Marg, Canadian Marginalization Index; M, median; IQR, interquartile range.
Rank-biserial correlation, 0.1 to <0.3: small effect, 0.3 to <0.5: medium effect, ⩾0.5: large effect.
Associations of depressive symptoms and racial identity
The POMS cohort included 43 White and 57 racialized participants, and the mono-ADS cohort included 56 White and 83 racialized participants (Table 1). Controlling for age, sex, and disability, the interaction between racial identity and diagnosis was significant (relative risk (RR) = 1.83, 95% confidence interval (CI) = 1.07, 3.13); Pearson chi-square = 90.0, p = 1.00) in the association between racial identity and depression. Being racialized was significantly associated with the elevation of depressive symptoms (CES-DC >10) in individuals with POMS (RR = 1.50, 95% CI = 1.04, 2.15) but not in mono-ADS (RR = 0.83, 95% CI = 0.55, 1.26). In addition, being Black (RR = 1.71, 95% CI = 1.11, 2.65), Asian (RR = 1.72, 95% CI = 1.15–2.58), or South Asian (RR = 1.57, 95% CI = 1.02, 2.47) was significantly associated with elevated depressive symptoms (CES-DC >10) in individuals with POMS but not in mono-ADS (Black: RR = 0.69, 95% CI = 0.30, 1.63; Asian: RR = 1.07, 95% CI = 0.62, 1.85; South Asian: RR = 0.52, 95% CI = 0.23, 1.16). Individual associations between racial identity and elevations of depressive symptoms (CES-DC >10) can be found in Table 3.
Associations between racial identity and elevated depressive symptoms in POMS and mono-ADS.
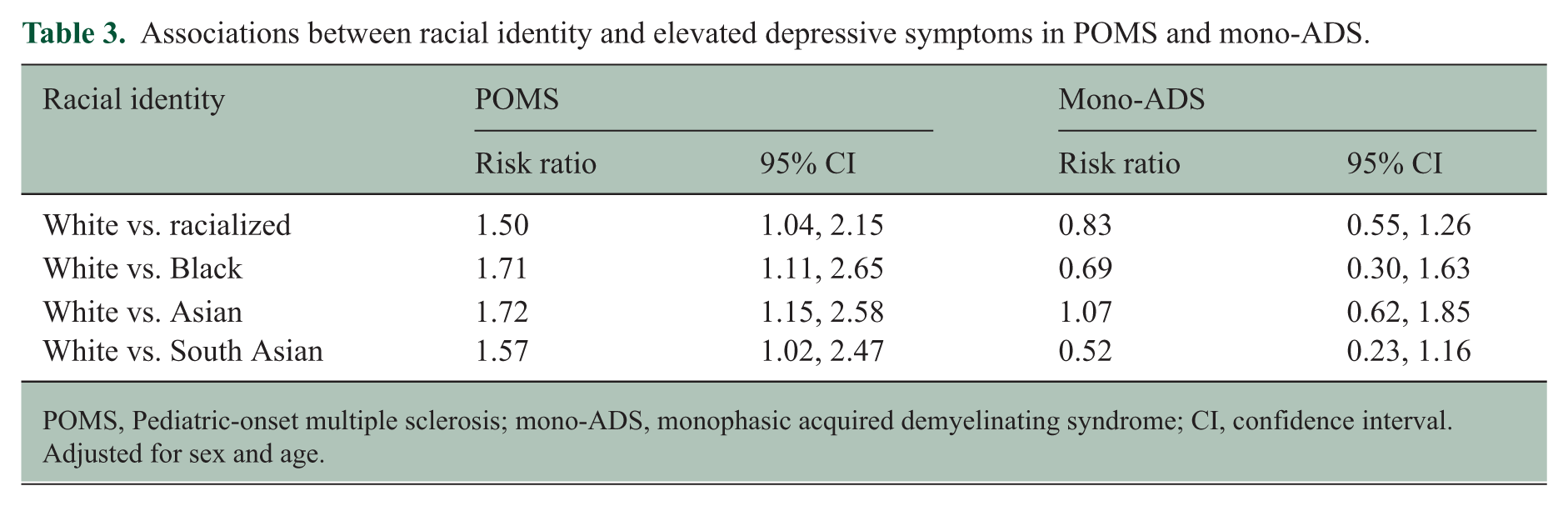
POMS, Pediatric-onset multiple sclerosis; mono-ADS, monophasic acquired demyelinating syndrome; CI, confidence interval. Adjusted for sex and age.
Neighborhood marginalization, racial identity, and depression
The CAN-Marg scores for material resources (ES = 0.22, p = 0.035) and immigration and visible minority (ES = 0.45, p < 0.001) were higher (worse) for racialized individuals with POMS than for White individuals, while age and labor force scores were lower (better) in racialized individuals than in White individuals (ES = 0.34, p = 0.003). Black individuals with POMS had the highest (worst) marginalization score for material resources (median = 4.5, IQR = 2.0) and households and dwellings (median = 3.5, IQR = 2.75) (Table 5).
In the POMS cohort, higher depression scores were associated with better (lower) household and dwelling scores (rs = −0.27, 95% CI = −0.52, −0.017) in racialized individuals. No other associations were found between neighborhood marginalization dimension scores in either White or racialized POMS. No associations were found in the mono-ADS cohort (Table 4) (Supplemental Table 4). When adjusted for sex and age, there were no significant associations in any groups.
Correlations between depression and neighborhood marginalization in POMS and mono-ADS.
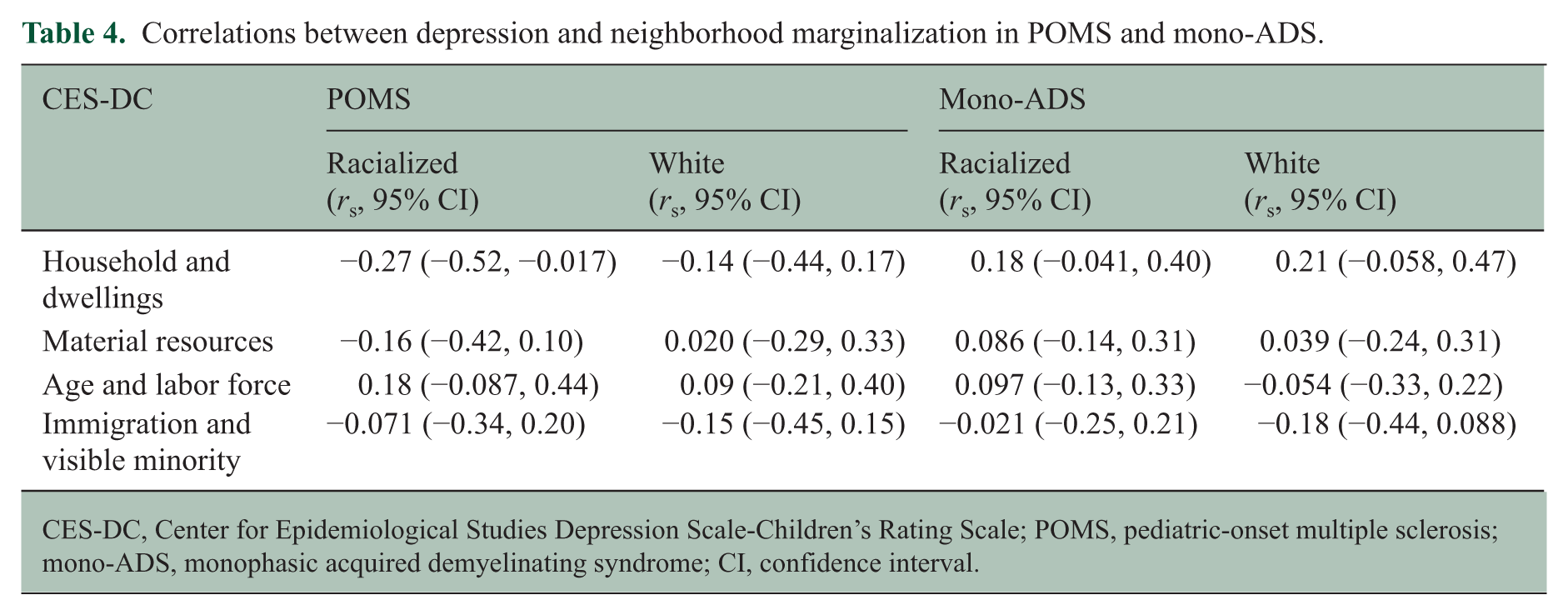
CES-DC, Center for Epidemiological Studies Depression Scale-Children’s Rating Scale; POMS, pediatric-onset multiple sclerosis; mono-ADS, monophasic acquired demyelinating syndrome; CI, confidence interval.
Marginalization scores of individuals with POMS can be found in Table 5. In POMS, Black individuals had higher odds of living in a neighborhood with the highest quintile of marginalization for material resources (OR = 12.7, 95% CI = 1.96, 82.1; C-stat = 0.81) and immigration and visible minority (OR = 5.70, 95% CI = 2.30, 14.1; C-stat = 0.68) compared with White individuals (Table 6). South Asian individuals with POMS (OR = 18.4, 95% CI = 3.49, 96.6; C-stat = 0.74) and Middle Eastern individuals with POMS (OR = 20.4, 95% CI = 2.30, 181; C-stat = 0.75) also had higher odds of living in a neighborhood with the highest quintile of marginalization for Immigration and Visible Minority score compared with White individuals. Controlling for age and sex, there were no differences between POMS and mono-ADS in the associations of racial identity, presenting elevated depressive symptoms, and living in a neighborhood with the highest quintile for all four domains of neighborhood marginalization.
Marginalization index scores of individuals with POMS.
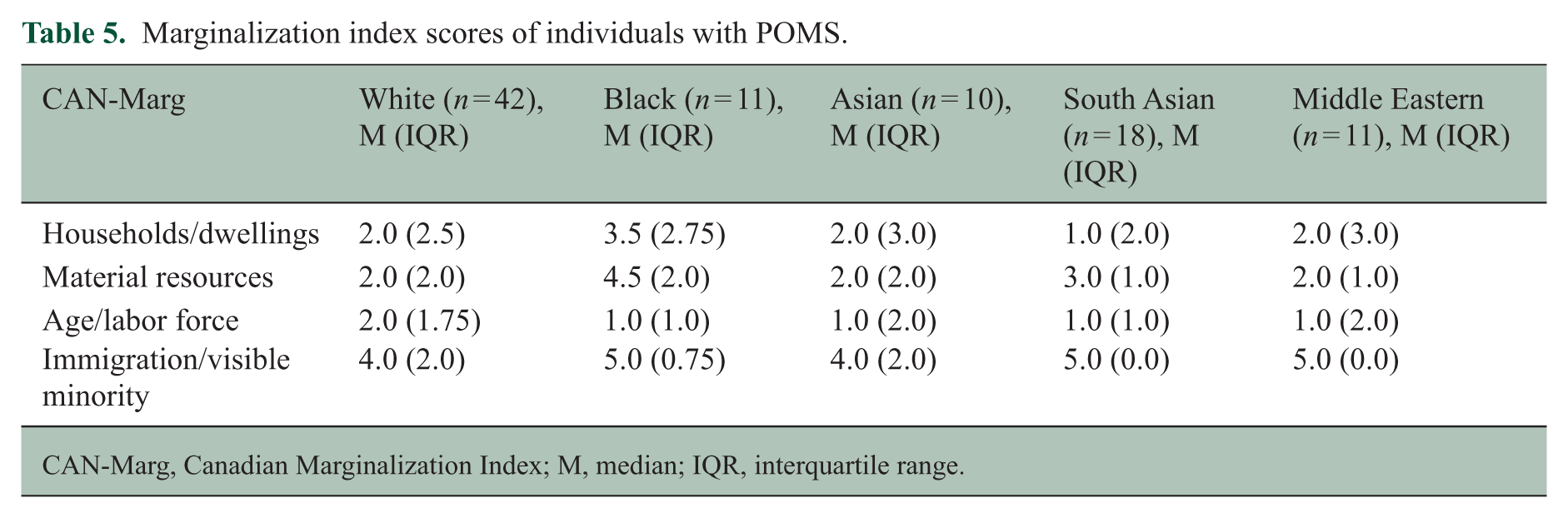
CAN-Marg, Canadian Marginalization Index; M, median; IQR, interquartile range.
Odds ratios of living in the highest quintile of neighborhood marginalization compared with living in the remaining four quintiles, in POMS.
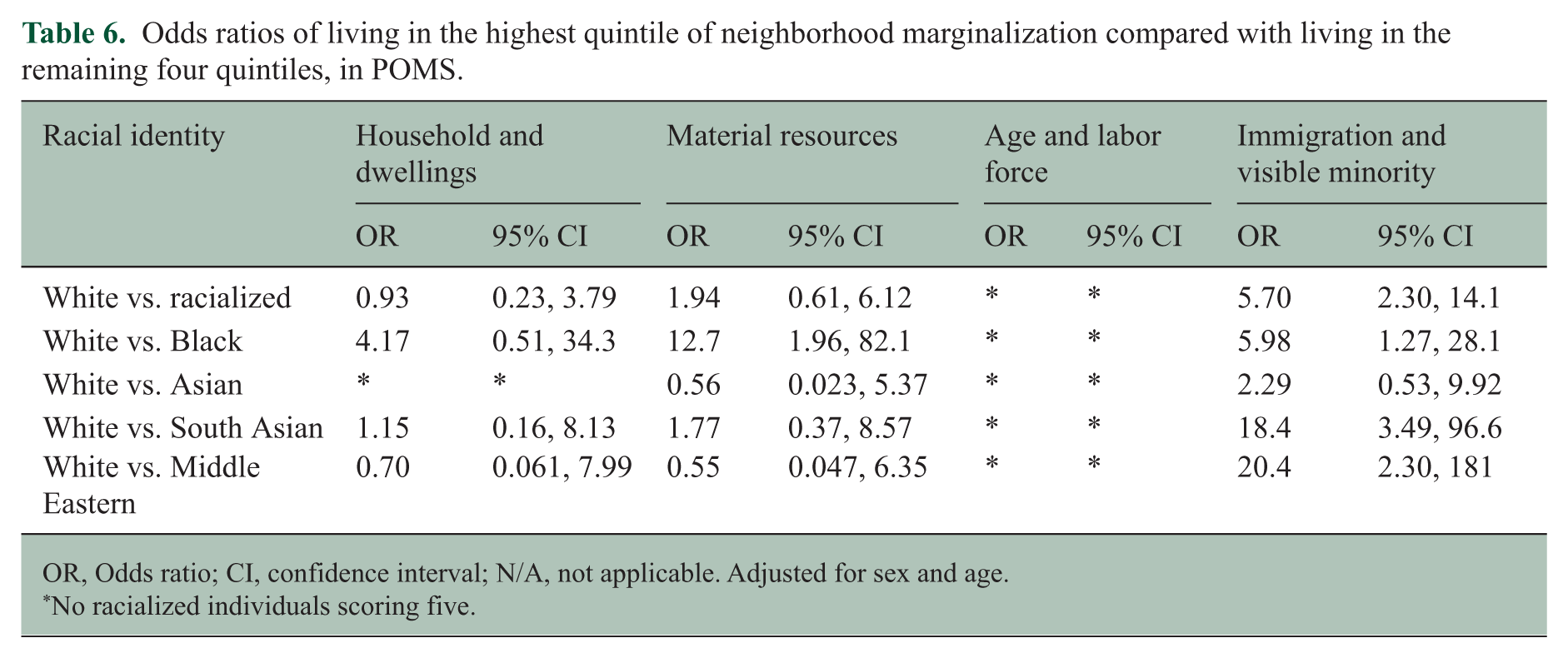
OR, Odds ratio; CI, confidence interval; N/A, not applicable. Adjusted for sex and age.
No racialized individuals scoring five.
Discussion
In this study, we investigated associations between depressive symptoms, racial identity, and neighborhood marginalization among individuals with POMS compared with those with mono-ADS. We found high rates of elevated depressive symptoms across both groups of children participating in our study (64% of POMS, 51% of mono-ADS), with more than half of all participants demonstrating elevated depressive symptoms. This finding aligns with recent literature pointing to high rates of depressive symptoms among youth, with pooled analyses identifying around one-third of otherwise healthy youth as harboring elevated depressive symptoms. 25 Of importance, despite high rates in both groups of elevated depressive symptoms, individuals with POMS had higher depression scores than individuals with mono-ADS, consistent with the literature. 13
Despite similarities in racial distribution between the mono-ADS and POMS groups, we found higher rates of elevated depressive symptoms in racialized individuals with POMS compared with White individuals, but not in those with mono-ADS. This supports our hypothesis that the presence of MS, a chronic illness, combined with being racialized, may exert “compounding effects” on outcomes.26,27 This is supported by findings from a population-based Canadian study: higher frequency of perceived discrimination based on race was associated with higher odds of having a chronic condition and poor self-rated health. 28 Our findings are also consistent with the literature in adults with MS in the United States: Black and Hispanic individuals with MS had higher depressive symptoms than White individuals. 29
We emphasize the higher marginalization scores observed overall in racialized individuals with POMS and, in particular, the observation that Black individuals with POMS had the highest neighborhood marginalization scores and were more likely to live in neighborhoods with less access and lower attainment of basic material needs (i.e. lower income, higher unemployment, lower housing quality, and lower educational attainment) 24 compared with White individuals with POMS. These findings reflect known demographic trends in Canada. A 2017 publication and federal report identified Black youth as three times more likely to report food insecurity than White youth. As well, one-fifth of Black individuals reported living in housing below standards compared to 7.7% of White Canadians.30,31 The report underscores the possibility that institutional disadvantages experienced by Black Canadians, such as access to health, education, employment, and housing, act as key drivers of inequitable health outcomes for this population 30
Although the association disappeared when adjusted for sex and age, interestingly, a paradoxical relationship was found between house and dwelling marginalization scores and depression scores. Average household size is one of the indicators of the household and dwelling dimension, such that the larger the household size, the higher the dimension score. 24 Our previous work has demonstrated that the number of people in an individual’s social network is associated with lower anxiety and higher levels of physical activity in youth with POMS.32,33 The household size accounted for in this dimension may be another measure of social network size, which could be a factor driving this finding. We do not have the granular information regarding social networks or household size from participants in this study to confirm this. Future studies are needed to understand the complex relationships between social networks, mental health outcomes, and marginalization in POMS.
Our study has limitations. First, the CAN-Marg is a composite environmental score linked to postal code; we did not have granular information on individual-level SES that could influence the relationship between marginalization and depression in POMS. Second, the CES-DC cutoff point of >10 was determined based on the distribution of scores for our sample, and we recognize that this differs from the initial validated cutoff score of 15. 20 Future studies are needed to determine a validated cutoff point for our specific population. Third, the study’s cross-sectional nature limits the ability to identify the direction of the associations and whether longitudinal changes in neighborhood marginalization will lead to changes in depression scores. Fourth, the wide confidence intervals for our significant findings may be due to the relatively small sample size of our study. It is also important to note that the smaller sample size required the consolidation of individual racial identity groups. Future longitudinal studies with a larger sample size are needed to better understand the direction of the relationship as well as the relationships within specific racial identities. In addition, a larger proportion of MS patients who did not complete the clinic questionnaire (and thus were not included in the study) were racialized compared with those who did. Future prospective studies need to employ intentional recruitment strategies that are culturally appropriate and address potential barriers for equitable representation. Fifth, the CAN-Marg scores were measured in 2016, the latest scores available during data collection. While our study extended to 2024, neighborhood characteristics generally change over decades, and, therefore, 2016 scores likely provide a relatively accurate approximation of marginalization. 34 Finally, although we included participants with mono-ADS without substantial long-term neurological impairment as the control group, we recognize that those with a single inflammatory episode may also experience disease-related challenges and may differ from a truly “healthy” control group.
Conclusion
Our study provides foundational evidence for associations between racial identity, neighborhood marginalization, and depression in individuals with POMS. It highlights differences in these relationships between POMS and those of a single, acute episode of neuroinflammation. Future longitudinal studies with larger sample sizes are needed in this population to better understand the influence of chronic illness, racial identity, and individual and neighborhood-level marginalization on depression and other mental health conditions. This will help identify modifiable individual and neighborhood factors and inform the development of interventions and policies that ameliorate the mental health of individuals with POMS.
Supplemental Material
sj-docx-2-msj-10.1177_13524585261453239 – Supplemental material for Racial identity, marginalization, and depression in pediatric-onset multiple sclerosis
Supplemental material, sj-docx-2-msj-10.1177_13524585261453239 for Racial identity, marginalization, and depression in pediatric-onset multiple sclerosis by Paul Yejong Yoo, Auva Zarandi, Samantha Stephens, Teresa To, Ruth Ann Marrie, Marcia Finlayson, Robert Motl and E Ann Yeh in Multiple Sclerosis Journal
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: E. Ann Yeh has received research funding from NMSS, CMSC, CIHR, NIH, OIRM, SCN, CBMH Chase an Idea, SickKids Foundation, Rare Diseases Foundation, MS Scientific Foundation, McLaughlin Centre, Leong Center, Peterson Foundation, and Gary Hurvitz Centre for Brain and Mental Health; Investigator-initiated research funding from Biogen. Scientific advisory: Hoffman-LaRoche, Alexion, and Pfizer. DSMB: Pipeline Therapeutics. Speaker honoraria: Biogen, JHU, Saudi Epilepsy Society, NYU, and MS-ATL; ACRS, PRIME, and CNPS. Co-Editor in Chief, MSARD. Governing Council: CANTRAIN. Steering Committee: Rare-Kids CAN. She holds the Hurvitz Chair in Neurology at The Hospital for Sick Children, Toronto, Canada. R.A. Marrie receives research funding from CIHR, MS Canada, Crohn’s and Colitis Canada, National Multiple Sclerosis Society, CMSC, the Arthritis Society, Public Health Agency of Canada, Pfizer Foundation, and the US Department of Defense, is a co-investigator on studies receiving funding from Biogen Idec and Roche Canada, and holds the Multiple Sclerosis Clinical Research Chair (Dalhousie University). The other authors have no conflicts of interest relevant to this article to disclose.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Edwin S.H. Leong Centre for Healthy Children at the University of Toronto and The Hospital for Sick Children. EA Yeh was supported in part by the Hurvitz Chair in Neurology, SickKids Foundation, The Hospital for Sick Children. The funding agencies had no role in the design of the study; collection, analysis, and interpretation of data; or in writing the manuscript. No products or services were provided.
Author contributions
Paul Yejong Yoo conceptualized and designed the study, secured funding for the study, coordinated and supervised data acquisition, analyzed the data, drafted the initial manuscript, and revised the manuscript.
Auva Zarandi acquired, cleaned, and analyzed the data, contributed to the initial draft of the manuscript, and critically reviewed and revised the manuscript.
Samantha Stephens conceptualized and designed the study, planned and designed the data analysis, and critically reviewed and revised the manuscript.
Teresa To, Ruth Ann Marrie, Marcia Finlayson, and Robert Motl contributed to the design of the study, planned and designed the data analysis, and critically reviewed and revised the manuscript.
E Ann Yeh conceptualized and designed the study, secured funding for the study, coordinated and supervised data acquisition, contributed to the initial draft of the manuscript, provided oversight and leadership responsibility for study conduct, and critically reviewed and revised the manuscript.
All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Ethical considerations
Ethics approval was obtained through the Hospital for Sick Children Research Ethics Board.
Consent to participate
Participants provided informed verbal and written consent, including child consent if the child was deemed to have the capacity by a healthcare professional or parent assent.
Consent for publication
Not applicable.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.