
Abstract
Background:
Multiple sclerosis (MS) is increasingly recognized as having a prodromal phase, characterized by non-specific symptoms preceding demyelinating events, yet prospective, longitudinal assessments of relevant signs before the first MS symptom are lacking.
Objectives:
To investigate whether a wide range of signs and symptoms occurred more frequently in individuals who later developed MS than in the underlying cohort.
Methods:
We followed 113,876 women from the Nurses’ Health Study II with prospectively collected data on lifestyle, health indicators, and diet. We examined the trajectory of these factors relative to the date of first symptom in 336 incident MS cases compared with the underlying cohort.
Results:
Several medical conditions, including migraine, depression, urinary leakage, and restless legs syndrome, were more prevalent in individuals who subsequently developed clinical MS. For example, the prevalence of migraine surpassed the underlying cohort 9–10 years before onset and reached 22.8% versus 19.3% at the time of first symptom. Furthermore, a decline in physical activity, physical function, and vitality occurred years before the first MS symptoms. Dietary changes were less pronounced.
Conclusion:
Several health indicators deteriorated years before typical MS symptoms emerged, suggesting that MS is preceded by a prodromal phase characterized by both specific and non-specific symptoms.
Introduction
Multiple sclerosis (MS) is increasingly recognized as having a prodromal phase, a period characterized by non-specific symptoms and biological changes that can precede the first clinically identified demyelinating events. This phase reflects an underlying disease process, as evidenced by subclinical pathology and subtle health changes that occur years before a formal MS diagnosis. 1 Biomarker studies further support this hypothesis, showing that neuroaxonal damage, indicated by elevated serum neurofilament light chain (NfL) levels, occurs during this prodromal period, sometimes as early as 5–10 years before clinical onset. 2 Understanding this early phase is crucial to identifying opportunities for earlier diagnosis and intervention.2,3
In previous research, the diagnosis of MS was preceded by an increased frequency of various signs and symptoms. These include elevated healthcare utilization extending up to two decades before the first demyelinating event,4,5 increased sickness absence, 6 psychiatric conditions like depression and anxiety,7,8 fatigue, sleep disturbances, pain, 9 and headaches, particularly migraine. 10 Gastrointestinal and urinary disturbances have also been reported more often in individuals years before their MS diagnosis.8,11 However, previous studies face some limitations inherent to their design. Most studies have relied on medical records or administrative data, which potentially miss milder symptoms that did not prompt a healthcare visit. Crucially, there has been a lack of studies involving prospective, longitudinal assessment of relevant signs and symptoms, collected identically in individuals who later developed MS and those who did not, long before disease onset.
To address these gaps, we conducted a prospective study within the Nurses’ Health Study II (NHS II) cohort. We aimed to investigate whether a wide range of signs and symptoms, assessed repeatedly via biennial questionnaires over decades, occurred more frequently in individuals who later developed MS during the years preceding clinical onset. By leveraging prospectively collected data up to two decades from the first MS symptom, we evaluated the trajectories of potential early features of the MS prodrome.
Methods
Study population
The NHS II is an ongoing prospective cohort study initiated in 1989, which recruited 116,429 female registered nurses across the United States (age range: 25–42 years). 12 Participants were followed biennially using questionnaires that collected information on health-related behaviors and outcomes. Over the full study period (1989–2019), the cumulative person-time-based response rate was 85.7%. MS cases were ascertained from 1989 to 2009. For the current analyses, participants were excluded if they had only baseline but lacked follow-up data, had unverified MS diagnoses, or had the first MS symptom before baseline. After applying these exclusions, 113,994 participants remained. Of these, 118 participants with MS onset before baseline or unknown onset date were further excluded, yielding 113,876 participants for analysis (Supplemental Figure S1). Excluded participants were similar to those included in age, body mass index (BMI), and smoking at baseline, but had higher proportions of missing data on geographic and lifestyle variables.
Assessment of potential prodromal factors
We selected the features of interest a priori based on existing literature and data availability.1,7,8,10 Health-related quality of life (HRQoL) was assessed using the Short Form 36 Health Survey Questionnaire (SF-36) 13 in 1993, 1997, and 2001. We specifically utilized three SF-36 sub-scales selected for their relevance to the MS prodrome, including the physical functioning scale (PF-10, encompassing 10 self-rated activity limitations such as walking, climbing stairs, and lifting), bodily pain (derived from questions assessing pain intensity and interference with daily activities), and vitality-tiredness (based on questions evaluating energy levels and fatigue). According to standard scoring procedures, SF-36 subscale raw scores were derived by summing Likert-type-scale item responses and linearly transforming them to range from 0 (worst state) to 100 (best state), as in previous studies in the NHSII cohort.14,15 Other lifestyle factors, including physical and mental health conditions, were assessed through biennial questionnaires. These conditions included physician-diagnosed migraine, depression (defined by self-reported clinical diagnosis, use of antidepressant medication, or a score of 52 or lower on the five-item Mental Health Index, a subscale of the SF-36),16,17 restless legs syndrome (defined using the International Restless Legs Study Group Criteria),18,19 and urinary leakage (defined as leakage occurring at least once per month). These conditions were also reported by the nurses in the biennial follow-up questionnaires, with the exact study waves presented in Supplemental Table S1.
Physical activity was quantified using reported weekly time spent in various activities, such as walking, running, swimming, and cycling, collected up to nine times between 1989 and 2017. Each activity was assigned a metabolic equivalent task (MET) value, and MET-hour/week was calculated for each participant by multiplying the MET score by the reported hours of activity per week. Total physical activity was determined by summing MET hours across all activities.20,21 Dietary intake was assessed using a validated food frequency questionnaire (FFQ) administered every 4 years from 1991 to 2015.22 –26 This assessment yielded 248 nutrients (including total caloric intake and 247 total-energy-adjusted nutrients), 32 food groups, and 8 dietary pattern scores. To ensure complete data sets for analysis, missing values for HRQoL, physical activity, and dietary variables (all continuous) were imputed using data from the previous wave or by averaging data between waves, as appropriate. Missing values arising from non-response at a given questionnaire wave were imputed using information from the most recent prior wave. For variables collected only at selected questionnaire cycles by design (e.g. FFQ administered every 4 years), values were estimated by averaging adjacent waves to reflect gradual temporal change.
Ascertainment of multiple sclerosis
The ascertainment procedure of MS in the NHS II has been detailed in a previous study. 27 Incident MS cases were identified by self-report on the biennial questionnaires. A questionnaire was sent to the treating neurologists of participants who reported an MS diagnosis to inquire about the certainty of the diagnosis (definite, probable, not MS) and the clinical history of the participant (including the date of the first symptom attributed to MS). Since 2003, one experienced neurologist has reviewed the medical history of participants who provided consent. To reduce misclassification, patients defined as definite or probable cases were included in the study, while those with unverified MS were excluded. For MS cases, the time to/from the first symptom was calculated as the difference between the return date of each questionnaire wave and the first clinical symptom.
Statistical Analysis
Participant characteristics were described using age-standardized means (standard deviation, SD) for continuous variables and percentages for categorical variables, stratified by incident MS status.
To characterize temporal trajectories of physical activity, migraine, HRQoL indicators, and other a priori defined conditions (depression, restless legs syndrome, and urinary leakage) relative to the time to/from first MS symptom and to identify when divergence emerged between future MS cases and the underlying cohort, each symptom and lifestyle indicator was modeled separately. To account for age and secular trends, continuous variables were standardized to z-scores by age and study wave, using the entire study population as the reference. For binary variables, the difference between the case’s value and the overall population prevalence rate was calculated to represent the excess probability of the condition in cases. Standardized values were visualized using loess curves (span α = 0.75), with loess-fitted means calculated to identify when indicator levels in cases diverged from the general population. Sensitivity analyses used years to clinical diagnosis as the time scale.
Longitudinal k-means clustering was applied to dietary variables to identify informative trends relative to the first MS symptom. Mean standardized values were calculated for 2-year intervals, and clusters were identified using the elbow method and visualized with loess curves. Given the high dimensionality of the feature set (especially the dietary variables) relative to the number of MS cases, elastic net regression with fivefold cross-validation was used to reduce overfitting through penalization and variable selection. Elastic net regression was used to predict future MS cases and distinguish prevalent cases using the information of the candidate indicators collected across different time frames (2-year intervals). Health conditions were modeled as binary variables, quality-of-life measures as continuous variables, and dietary variables as continuous variables. Two regression models were developed: one using the a priori selected variables, namely physical activity, migraine, depression, and HRQoL indicators, while the other included the dietary variables. Twelve case–control data sets were constructed at 2-year intervals relative to the first MS symptom, with up to 30 age- and wave-matched controls per case to maximize use of available data and improve the stability of estimates in this rare-outcome setting. Area under the curve (AUC) was used to assess model performance, and fivefold cross-validation was used to prevent overfitting. In sensitivity analyses, the composite depression measure was redefined by self-reported clinical diagnosis and the Mental Health Index, without further including the use of antidepressant medication.
All analyses were performed using SAS 9.4 and R 4.3.0. Loess curves and elastic net regression were implemented using ggplot2 and tidymodels packages, respectively. All tests were two-tailed, with an α level set at 0.05.
Results
Baseline characteristics of the study population
A total of 113,876 female participants were included, with a mean age of 34.4 years (SD: 4.7, Table 1). Among them, 336 developed MS, with the first MS symptom occurring between 1989 and 2009 (mean age at the first MS symptom: 42.3 years, SD: 6.4). Participants who developed MS were more likely to reside in northern or mid-latitude regions at age 15 years and to have a higher BMI. They also reported less supplemental vitamin D use.
Baseline characteristics of the study participants in Nurses’ Health Study II.
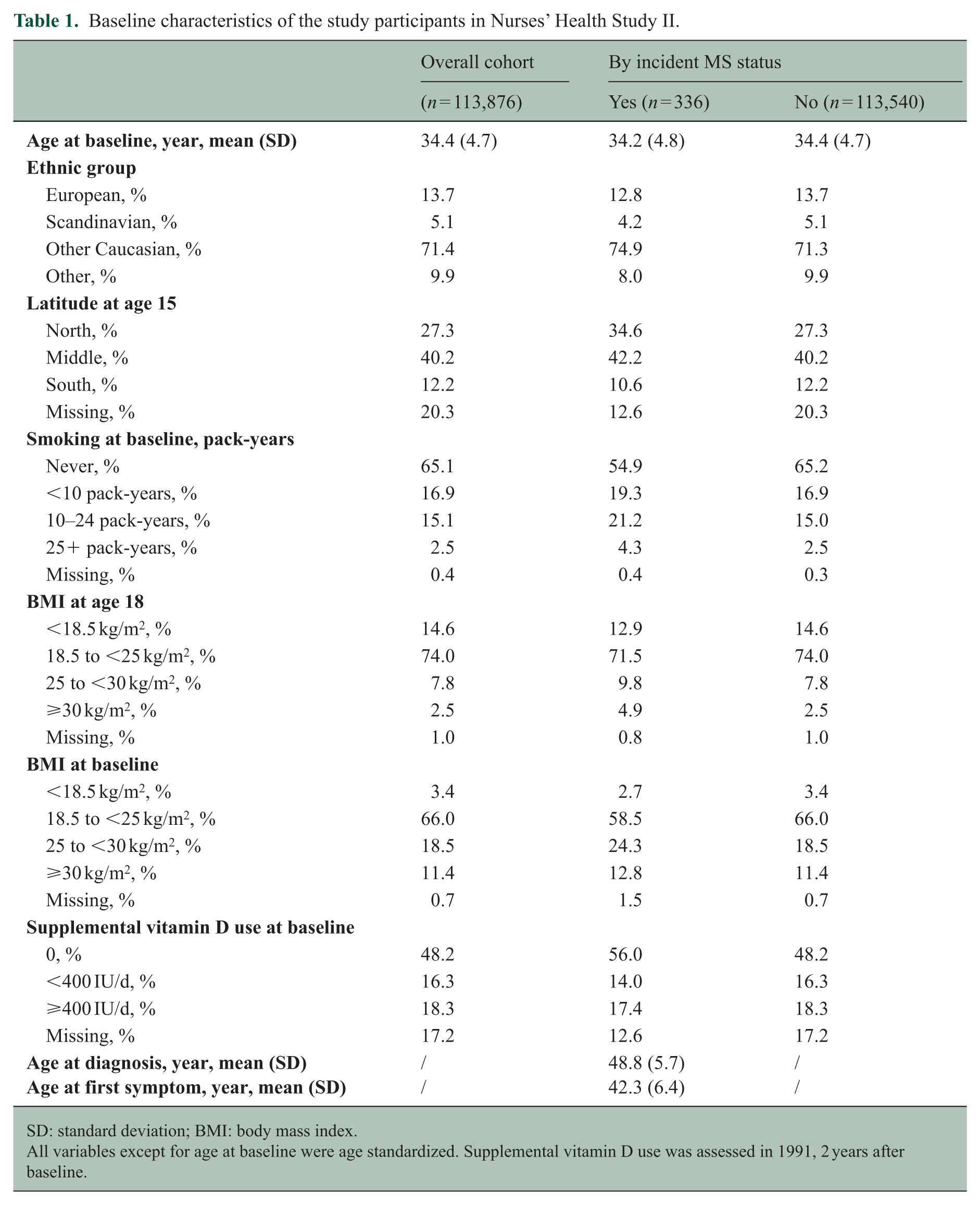
SD: standard deviation; BMI: body mass index.
All variables except for age at baseline were age standardized. Supplemental vitamin D use was assessed in 1991, 2 years after baseline.
Trajectories of the a priori defined indicators
Among the 336 participants who developed MS, trajectories of physical activity and migraine relative to years to first MS symptom are presented in Figure 1. Participants who developed MS had reduced physical activity compared with the overall underlying cohort approximately 15 years before the first identified neurological symptoms attributable to MS (MS symptoms from here on) and continued to decline around and after the time of the first symptom. Conversely, the relative prevalence of migraine increased with time to clinical MS onset. The prevalence of migraine was higher in individuals who developed MS approximately 10 years before their first MS symptoms, continued to increase in the year preceding MS onset, and remained higher in the 12 years of follow-up after onset. At the time of the first MS symptoms, the migraine prevalence was 22.8% in MS cases and 19.3% in the overall underlying cohort (Supplemental Table S2).
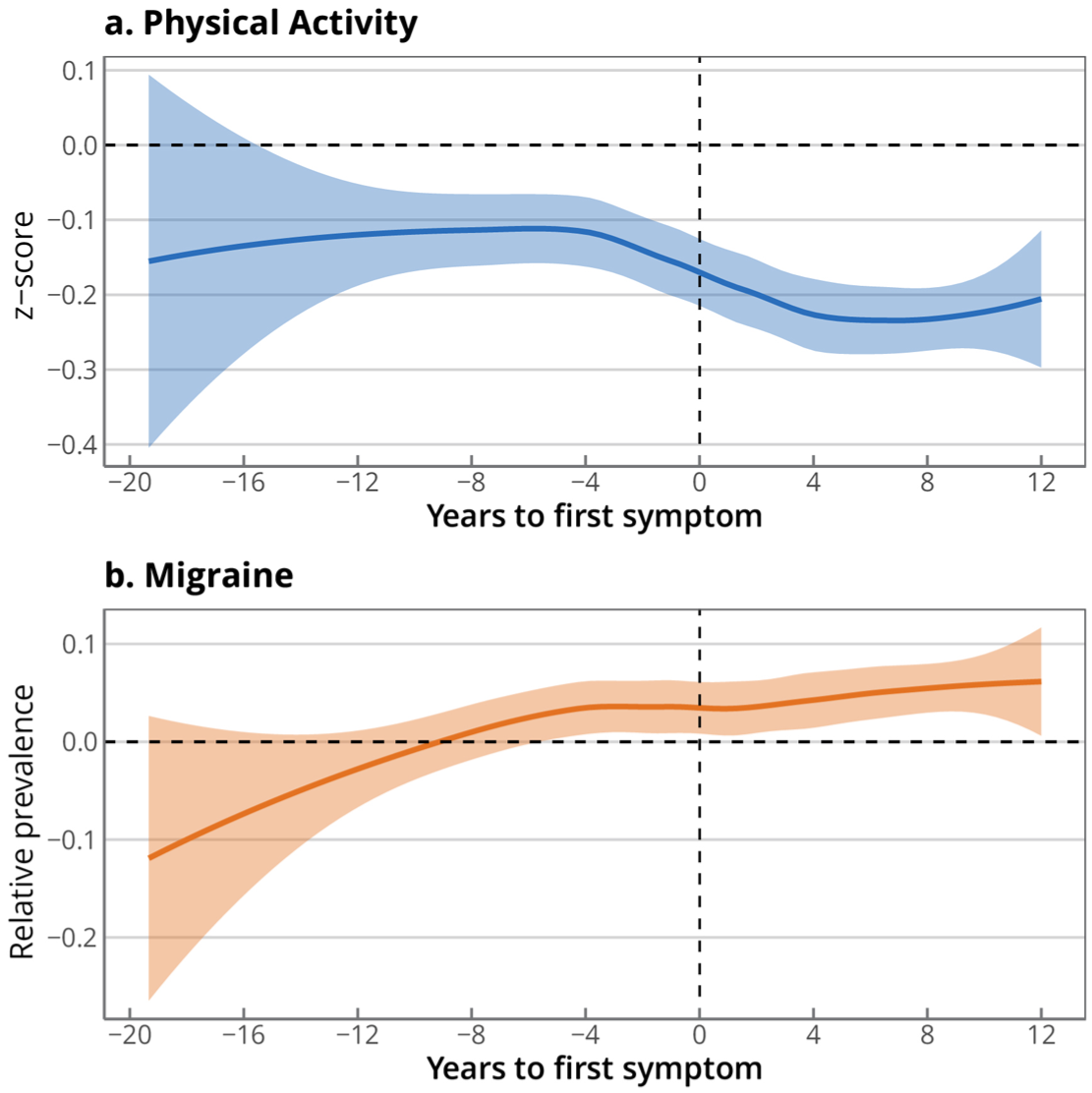
Trajectories of physical activity and migraine by year to first symptom among multiple sclerosis cases.
Figure 2(a) illustrates that participants who developed MS experienced a sharp decline in three HRQoL indicators around the time of the first symptom. Physical function and vitality/tiredness scores started to decline approximately 1-2 years before the first MS symptoms, while bodily pain scores started to decrease (indicating more pain) only around the time of the first MS symptoms. The scores continued to decline in the years following the first symptom, with the decline most pronounced in physical function scores. The trajectories of the relative prevalence of other mental and physical conditions are shown in Figure 2(b). For urinary leakage and restless legs syndrome, the prevalence relative to the overall underlying cohort started increasing approximately 10 years before the first MS symptoms. Conversely, the rate of depression was similar in MS cases and the overall underlying cohort until the time of the first symptoms, but markedly increased thereafter.
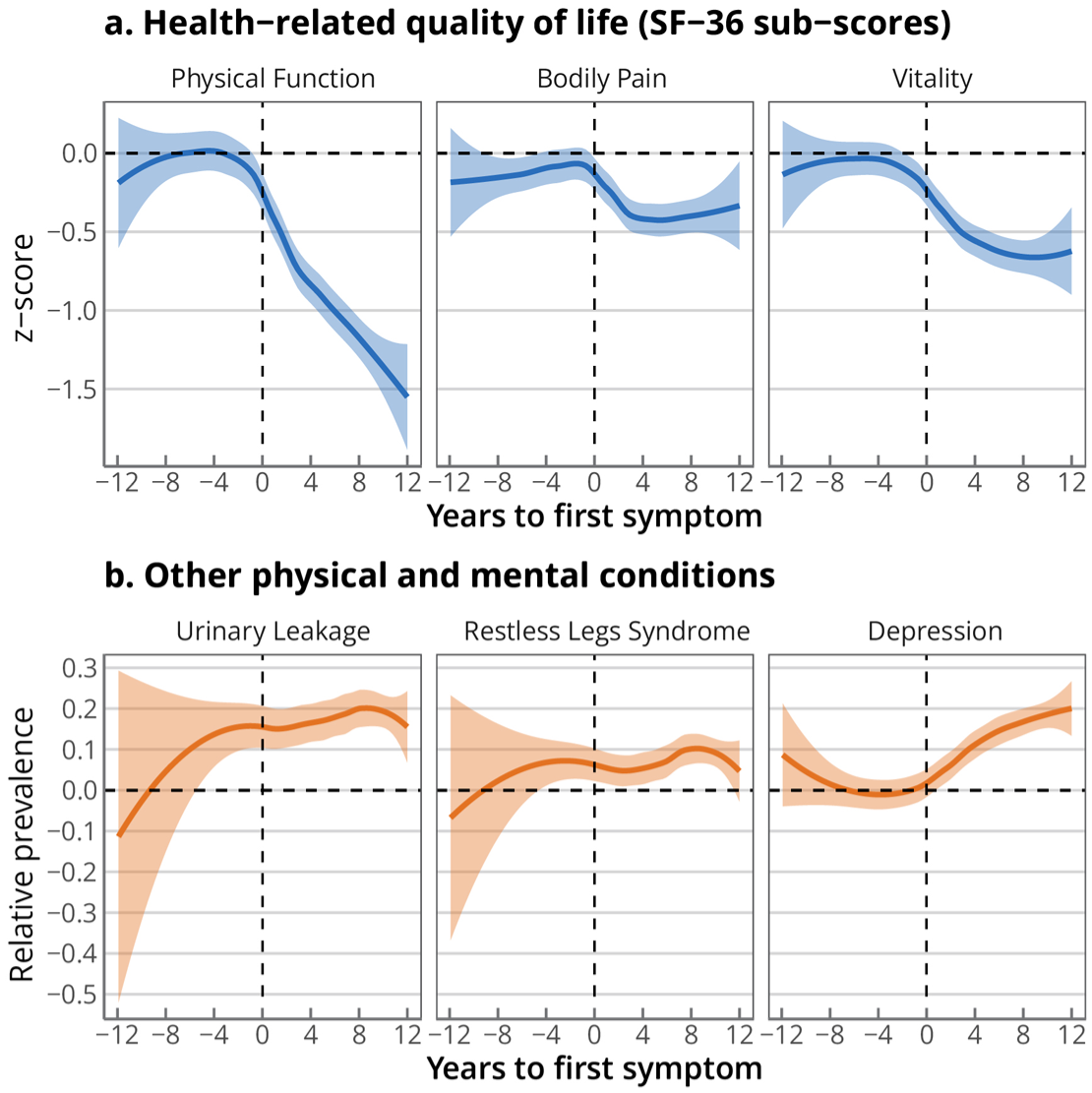
Trajectories of health-related quality-of-life indicators and other physical and mental conditions among multiple sclerosis cases.
When using the year of the first clinical diagnosis of MS as the time scale, the trajectories for most indicators diverged earlier in cases and the overall underlying cohort. For example, the physical functioning score was lower in MS cases than the population mean 3–4 years before clinical diagnosis, as shown in Supplemental Figure S2. When antidepressant use was excluded from the composite depression definition, the trajectory of depression relative to matched controls remained qualitatively similar in direction, with the relative prevalence increasing after symptom onset, although attenuated in magnitude (Supplemental Figure S3).
Trajectories of the dietary variables
With longitudinal k-means clustering applied to 268 dietary variables, we identified three patterns, including 153 that remained stable, 58 that increased, and 57 that declined over time (Supplemental Figures S4 and S5). We visualized the trajectories of three macronutrients and three selected variables that increased over time (Figure 3). The energy-adjusted intake level of total fat among MS cases did not differ from the overall population across the years before and after the first symptom, whereas that for protein declined. Carbohydrates increased from years before the first symptom, as did added sugars, and the deviance retained after the first symptom. Moreover, we observed that the intake levels of vitamin B12 and vitamin D both increased with time. Interestingly, the vitamin D intake level of the cases was lower than that of the overall population around a decade before onset, consistent with its role as an etiologically protective factor.
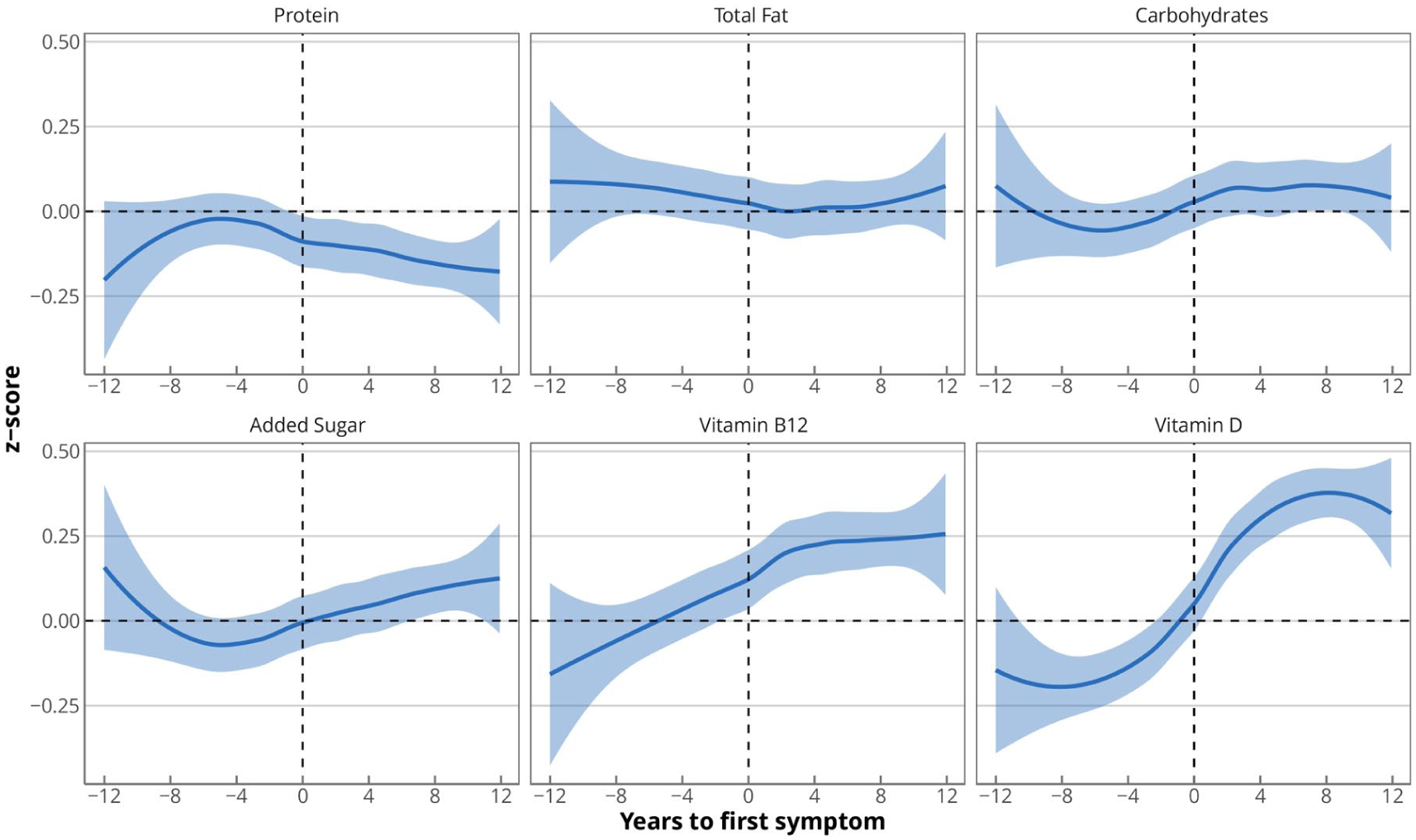
Trajectories of selected nutrient intake levels among multiple sclerosis cases.
Time-specific prediction models for multiple sclerosis
The AUC for the elastic net models combining the physical activity, migraine, depression, and HRQoL indicators or dietary variables across different time frames is presented in Figure 4 and Supplemental Table S3. The model combining physical activity, migraine, depression, and HRQoL indicators did not predict MS before the first symptom (AUC ranging from 0.479 to 0.567) but showed stronger discrimination after the first symptom (AUC: 0.619 in 0–2 years and 0.782 in 10–12 years after the first symptom). In contrast, the model utilizing the diet-related variables had limited predictive or discriminative ability across all time slots, with a maximal AUC of 0.616 (0.600–0.632) in 10–12 years after diagnosis.
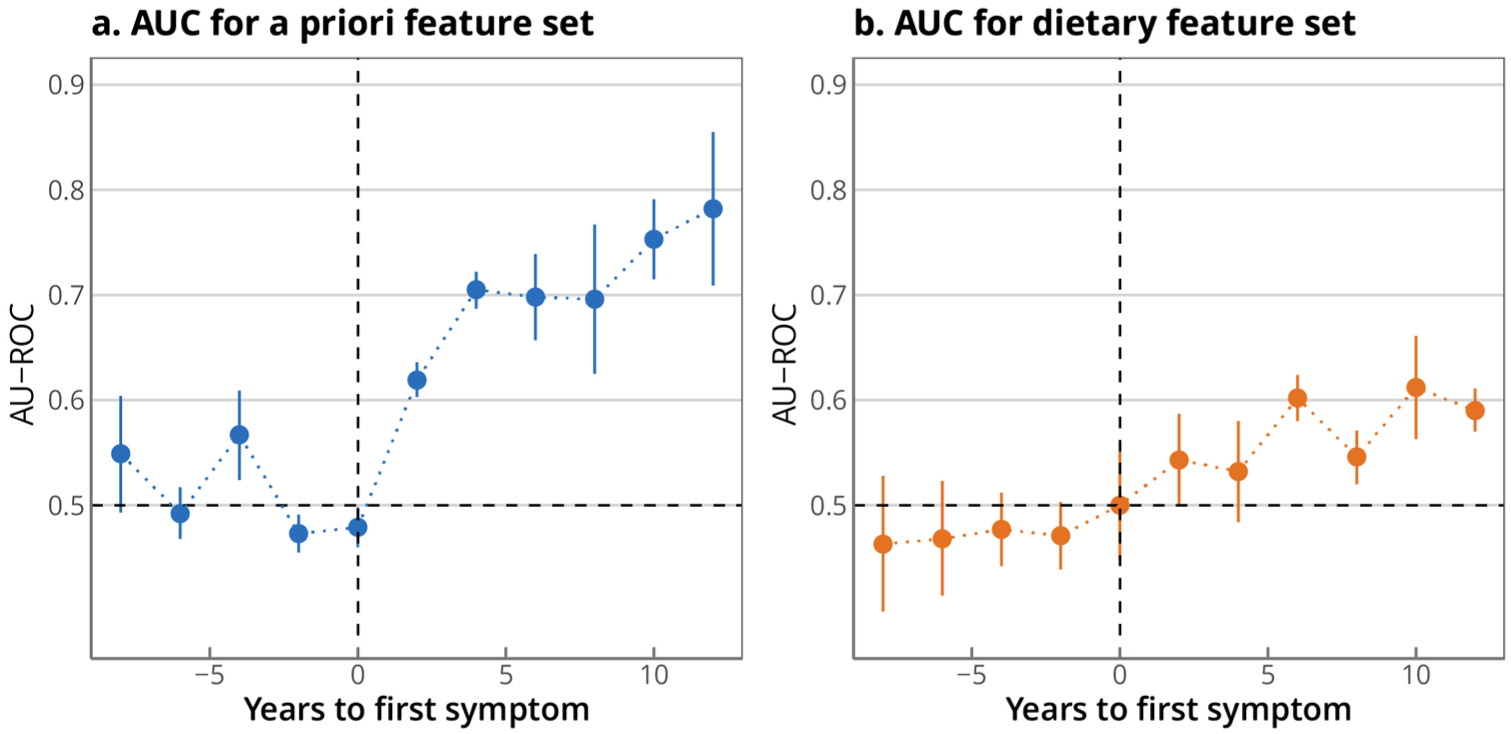
Area under the receiver-operating curve (AU-ROC) of the elastic net model for predicting or discriminating multiple sclerosis cases with the a priori defined variables and dietary variables.
Discussion
In this study, we found that a spectrum of symptoms and lifestyle changes emerge in the years preceding the clinically recognized MS onset. Specifically, several medical conditions, including migraine and restless legs syndrome, were more prevalent in individuals who subsequently were diagnosed with MS compared with those who did not. Furthermore, we observed a decline in physical function and vitality, a general measure of energy and fatigue, years before the onset of MS symptoms. Our findings suggest that MS may be preceded by non-specific symptoms that are not readily identifiable as manifestations of the disease at the time they occur. This underscores the inherent difficulty of recognizing MS during its prodromal phase, rather than indicating a missed opportunity for diagnosis.
Our findings are consistent with results from several previous studies. For example, we observed that participants who later developed MS had a higher risk of migraine up to 10 years before the first clinical symptoms, which is consistent with recent findings from a large Norwegian cohort study that reported a higher prevalence of migraine, but not other diagnosed headaches, up to 10 years before MS onset. 10 Furthermore, we observed a higher prevalence of bodily pain and depression, and lower vitality, in individuals who later developed MS, consistent with previous findings from healthcare database studies assessing early signs and symptoms.7 –9
Our study extends previous research due to the availability of extensively validated, repeatedly collected assessments of lifestyle factors, including physical activity and diet. We observed consistently lower physical activity levels in individuals who later developed MS, potentially indicating a protective effect of physical activity against MS risk, as previously reported.28,29 However, the decline in physical activity levels and physical function we observed in the years preceding clinical MS onset suggests these are also early manifestations in the prodromal phase. In our comprehensive assessment of dietary factors, which could change as individuals develop vague and nonspecific symptoms leading to dietary changes, we did not find marked changes until the years immediately preceding MS, but observed more marked changes after onset. This is illustrated by the fact that the machine learning models trained on all available dietary factors could not predict MS better than chance until after MS onset. Dietary features and selected lifestyle and symptom indicators demonstrated poor discriminative performance (AUC < 0.5), indicating limited predictive value when considered in isolation before symptom onset. However, the increased vitamin B12 consumption in the years before clinical MS onset may reflect self-treatment of nonspecific symptoms or increased medical visits due to non-specific paresthesia leading to B12 prescription.
The prodromal phase in MS has increasingly been recognized in recent years. Initial studies demonstrated lower cognitive performance up to 20 years before first progressive MS symptoms, 30 and subsequent work reported higher healthcare utilization up to two decades before a first demyelinating event,4,5,31 along with increased sickness absence 6 and elevated NfL levels, 2 suggesting ongoing neuroaxonal injury during the prodromal phase. 32 The duration of this phase remains uncertain. However, if Epstein–Barr virus (EBV) infection is proven to be causative, it could represent the earliest identifiable event in the prodromal phase, and a median of 7.5 years from primary EBV infection to the onset of clinical MS symptoms has been reported. 33 Other studies suggest this duration may extend over 10 years, likely reflecting variations in age at onset and quality of care across study populations.3,8 Although it remains unclear whether the MS prodromal phase represents undiagnosed demyelinating episodes or a distinct clinical entity,34,35 it may still offer an opportunity for earlier detection and potentially improved long-term outcomes through early treatment initiation.36,37
Although our prediction models did not show prominent performance in identifying future MS cases before symptom onset, the recognition of a prodromal phase still carries important clinical and public health implications. Identifying patterns of subtle symptoms and lifestyle changes years before classical MS onset suggests a potential window for earlier recognition and intervention. Clinically, increased awareness among healthcare professionals about clusters of symptoms such as persistent migraine, fatigue, depression, or declining physical function may facilitate timely neurological evaluation and monitoring in individuals at risk. From a public health perspective, these findings underscore the value of improving screening systems and longitudinal health data capable of detecting subtle health changes preceding neurodegenerative diseases. Understanding and characterizing the prodromal phase could ultimately inform strategies for risk stratification, targeted screening, and early initiation of treatment, thereby improving long-term outcomes and reducing disease burden at the population level.
Our study has several strengths, including the use of prospectively collected data from a large, well-characterized cohort, enabling the comparison of women with and without MS within the same study population. The long follow-up period and repeated measurements of lifestyle factors and health indicators allow for the assessment of prodromal signs with higher sensitivity than in previous investigations. Our study also has some limitations. Although the longitudinal design enabled assessment of pre-symptomatic predictors, the number of incident MS cases was modest compared with large administrative or registry-based studies, which may have limited statistical power and constrained the predictive performance of the models. Women in our cohort were recruited in 1989 between the ages of 25 and 42 years. Because the majority of participants were already in their mid-30s at enrollment, fewer person-years of observation were accumulated at younger ages, limiting the capture of younger-onset cases and shifting the observed age-at-onset distribution upward. This is reflected in the mean age at first symptom of 42.3 years and the mean age of diagnosis of 49 years, which is beyond the expected age at MS diagnosis in the general population, typically in the late 20s to early 30s. The approximately 6.5-year interval between first symptom and diagnosis likely reflects the diagnostic process of the era in which these cases were ascertained, predating the widespread availability of MRI and the adoption of the McDonald criteria. Therefore, the generalizability of our findings to contemporary diagnostic settings warrants further investigation. Furthermore, due to its focus on women and the predominantly white cohort with relatively high educational attainment, findings may not generalize to men or other demographic groups. Also, the precision in estimating the trajectories of some lifestyle factors and health domains may be limited by incomplete repeated measures. For health conditions, as MS patients in this cohort had an average interval of 6.5 years from symptom onset to diagnosis, they may have greater likelihood of diagnosis of other conditions given the frequent encounters with neurologists, and some conditions might overlap with the diagnostic process for MS. Similarly, dietary data are self-reported, which could introduce measurement error, although the prospective design mitigates reporting bias compared with retrospective data. Specifically, NfL levels, which are a biomarker of neuroaxonal injury, were not available for this analysis. Future studies incorporating biomarker data may provide additional biological insight into the MS prodrome. Finally, we cannot exclude the possibility of residual confounding induced by unknown factors that may similarly change over time.
In conclusion, several medical conditions, including migraine, depression, and restless legs syndrome, appear more frequently in individuals who later develop MS, alongside declining physical function and vitality years before traditional MS symptoms emerge. These symptoms, however, are non-specific and insufficient to predict the future onset of MS.
Supplemental Material
sj-docx-1-msj-10.1177_13524585261454827 – Supplemental material for Comorbidities and lifestyle changes as predictors of the multiple sclerosis prodrome: A prospective cohort study
Supplemental material, sj-docx-1-msj-10.1177_13524585261454827 for Comorbidities and lifestyle changes as predictors of the multiple sclerosis prodrome: A prospective cohort study by Hui Chen, Marianna Cortese, Mario H Flores-Torres, Xiao Chen, Vinicius A Schoeps, Tanuja Chitnis, Changzheng Yuan, Alberto Ascherio and Kjetil Bjornevik in Multiple Sclerosis Journal
Footnotes
Acknowledgements
The authors would like to thank the participants and staff of the Nurses’ Health Study II for their valuable contributions and several state cancer registries for their help: AL, AZ, AR, CA, CO, CT, DE, FL, GA, ID, IL, IN, IA, KY, LA, ME, MD, MA, MI, NE, NH, NJ, NY, NC, ND, OH, OK, OR, PA, RI, SC, TN, TX, VA, WA, WY. The authors assume full responsibility for the analyses and interpretation of these data.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a grant from the National Multiple Sclerosis Society awarded to KB (RFA-2301-40691). The cohorts were supported by grants UM1 CA186107, U01 CA176726, and UM1 CA167552 from the National Institutes of Health (NIH). HC was supported by the Zhejiang University Doctoral Academic Rising Star Training Program. The funding sources did not participate in the design or conduct of the study; collection, management, analysis, or interpretation of the data; or preparation, review, or approval of the manuscript. This manuscript is the result of funding in whole or in part by the NIH. It is subject to the NIH Public Access Policy. Through acceptance of this federal funding, NIH has been given the right to make this manuscript publicly available in PubMed Central upon the Official Date of Publication, as defined by NIH.
Data availability statement
Because of participant confidentiality and privacy concerns, requests to access NHSII data must be submitted in writing. According to standard controlled access procedures, applications to use resources will be reviewed by the External Collaborations Committee to verify that the proposed use maintains the protection of the privacy of participants and the confidentiality of the data. Investigators wishing to use NHSII data are asked to submit a brief description of the proposed project (go to ![]() (contact email:
(contact email:
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.