
Abstract
To assess whether oxidative stress drives biomarkers implicated in disability progression independent of relapses, we randomized 2:1 fifteen adults with progressive MS (Expanded Disability Status Scale (EDSS): 2.0–6.5) to receive high-dose oral N-acetyl cysteine (NAC, 1250 mg TID), a major source of endogenous antioxidants, or placebo for 4 weeks (NCT02804594). Using the Olink proximity extension assay, we measured 20 serum biomarkers at baseline and 4 weeks on treatment. NAC resulted in decreased glial fibrillary acidic protein (median change: −10.1 pg/mL vs. 39.5 pg/mL, p = 0.008) alongside stable neurofilament light chain levels (median change: 0.25 pg/mL vs. 0.61 pg/mL, p = 0.777). Our exploratory biomarker findings suggest NAC may be a promising agent to delay MS progression.
Keywords
Introduction
Multiple sclerosis (MS) is a chronic autoimmune demyelinating condition that is characterized by neuroinflammation and neurodegeneration. 1 Current disease-modifying therapies have a modest effect on the prevention of disability progression independent of relapse activity (PIRA), suggesting that, although residual inflammatory processes exist in non-active progressive forms of MS (PMS), mechanisms such as neuronal damage associated with chronic demyelination, metabolic failure, and oxidative stress are potentially more critical determinants.1,2
Oxidative injury is mediated by endogenous accumulation of reactive oxidative species (ROS) released by innate central nervous system (CNS) immune cells, iron deposition in the CNS parenchyma, and/or reduction of antioxidant synthesis leading to neurodegeneration and demyelination. 2 Glutathione (GSH), a major intrinsic antioxidant, has been shown by brain magnetic resonance imaging (MRI) spectroscopy to be decreased in the gray matter of MS patients compared to healthy controls. 3 N-acetyl cysteine (NAC) directly scavenges ROS and may restore neuronal GSH by providing the rate-limiting substrate for its intracellular synthesis. 3 As NAC crosses the blood–brain barrier at high oral doses, it is being tested as a promising add-on therapy in PMS patients.4,5
In this study, we investigated the effect of high-dose oral NAC on 20 serum biomarkers in PMS patients in a pilot phase 2 randomized, placebo-controlled, double-blinded, clinical trial (NCT02804594).
Methods
Individuals with PMS aged 18–75 years, with at least 1 year since progressive symptom onset, a Modified Fatigue Impact Scale (MFIS) of more than 38, and an Expanded Disability Status Scale (EDSS) 2.0–6.5, were randomized 2:1 to NAC 1250 mg TID or placebo for 4 weeks. Further details on the trial protocol are provided in Krysko et al. 4
Serum biomarkers were assessed utilizing a multi-protein assay panel, based on Olink proximity extension assay methodology.6,7 This platform enabled measurement of an a priori defined set of biomarkers, including neurofilament light chain (NfL), glial fibrillary acidic protein (GFAP), and myelin oligodendrocyte glycoprotein (MOG), providing mechanistic insights into pathways of potentially averted tissue damage, as well as interleukin-12 subunit beta (IL-12B), a surrogate marker of NAC effect. Additional proteins were available for post hoc evaluation. Changes in levels from baseline to week 4 between NAC and placebo arms were compared with the Wilcoxon rank-sum tests, as pre-specified for efficacy outcomes using a modified intention-to-treat analysis. The last observation carry-forward was performed to handle one missing follow-up sample in the NAC arm.
A sensitivity analysis to further adjust efficacy outcomes for age was conducted using permutation-based analysis of covariance (ANCOVA). Since this was an exploratory investigation, analyses were not adjusted for multiple comparisons. All statistical analyses were conducted in R version 4.3 (R Foundation, Austria) using two-sided tests.
Results
Fifteen individuals were randomized to receive either NAC (n = 10) or placebo (n = 5), with one subject assigned to the placebo arm not providing blood samples and not included in this study, resulting in a final placebo sample of four subjects. Baseline characteristics between the treatment arms were well balanced except for age. In the NAC arm, 80% of participants were female, with a median age of 51.0 years (interquartile range (IQR) = 44.50–56.75), whereas in the placebo arm, 75% of participants were female, with a higher median age of 63.5 years (IQR = 52.50–71.30).
Changes in GFAP levels, a marker of astrocytic damage, were significantly different between treatment groups, with levels decreasing in NAC while increasing in the placebo-treated participants (median change: −10.1 pg/mL vs. 39.5 pg/mL, respectively; p = 0.008) (Figure 1 and Supplemental Figure S1). NfL, a marker of neuro-axonal damage, remained stable over time with no evidence of level changes between the two arms (median change: 0.25 pg/mL vs. 0.61 pg/mL, respectively; p = 0.777). MOG, a marker of myelin injury, tended to decrease when comparing the difference in changes between NAC and placebo arms, especially after age adjustment (median change: 0.15 pg/mL vs. 4.8 pg/mL, respectively; unadjusted p = 0.106, adjusted p = 0.057). Additional differences in change between NAC and placebo were observed in IL-12B (median change: −6.5 pg/mL vs. 17.2 pg/mL, respectively; p = 0.054) and sCD6 levels (median change: 14.3 pg/mL vs. −19.9 pg/mL; p = 0.054) approached but did not meet the significance threshold. Results for the full panel of proteins are provided in Supplemental Figure S2 and were robust to age adjustment (data not shown).
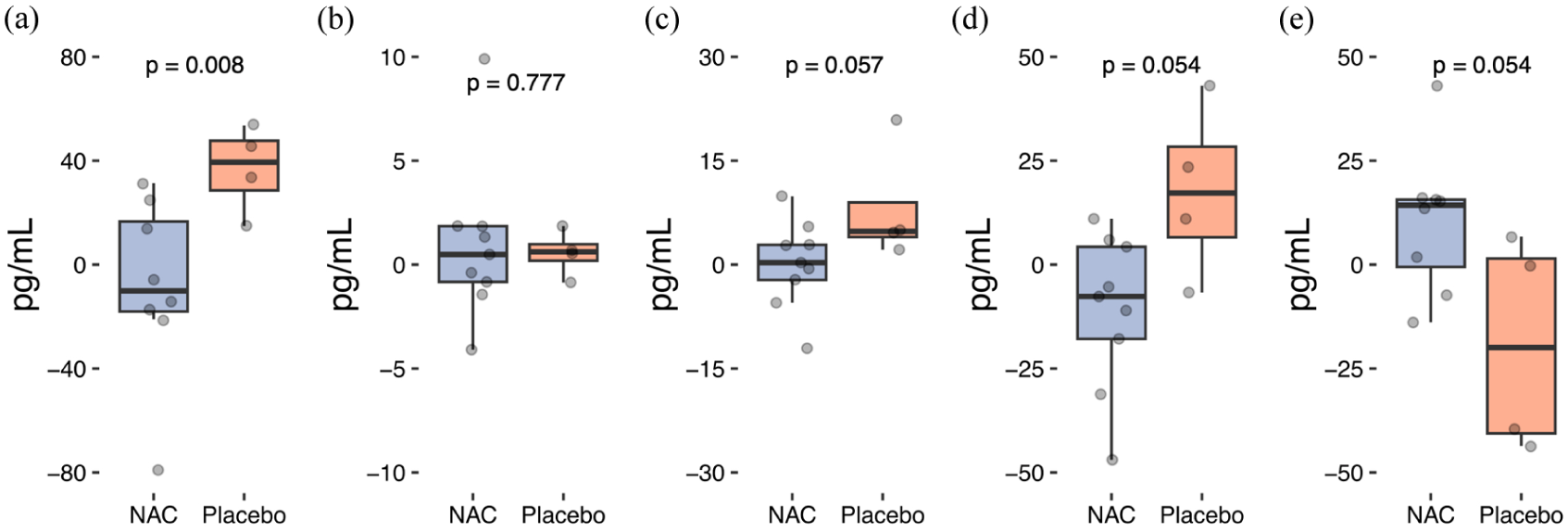
Changes in serum biomarker levels over 4 weeks between NAC and placebo treatment arms: (a) GFAP, (b) NfL, (c) MOG, (d) IL-12B, and (e) sCD6.
Discussion
In this study, a 4-week course of high-dose oral NAC in patients with PMS led to a decrease in markers of ongoing astrocytic and myelin damage, suggesting a biologically plausible impact on mechanisms implicated in PIRA. This trial was too short in duration to evaluate the impact of NAC on clinical PIRA, but previous observations have shown that GFAP levels, a marker of astrocytic damage, are 50% higher in patients experiencing PIRA than in matched stable MS patients. 8 Furthermore, NfL levels, a marker of neuro-axonal damage, were no longer predictive of PIRA after adjustment for GFAP, 8 indicating NfL may be less suited for identifying progression risk than for relapse activity. Therefore, the observed reductions in GFAP levels alongside stable NfL levels are consistent with a potential delay in biological processes linked to disability progression.
This biomarker profile is consistent with proposed mechanisms of disease progression and NAC treatment effect. Post-mortem studies suggest that axons remain relatively preserved while macrophages phagocytose reactive astrocytes and oligodendrocytes at the margins of expanding brain lesions. 9 Myelin debris becomes susceptible to peroxidation by ROS as they accumulate in a CNS environment of impaired microglial clearance, characteristic of PMS, contributing to experimental autoimmune encephalomyelitis severity.1,10 Directly counteracting this process, NAC has been shown to reverse lipid peroxidation and ameliorate disease severity in mice. 10 Our findings of relative reductions in MOG and GFAP levels in NAC recipients support the hypothesis that this pathway may contribute to the progression of disability in humans.
Furthermore, inhibition of IL-12B assembly has been previously shown in mice exposed to NAC, 11 which, in keeping with decreased IL-12B levels in NAC-treated subjects, may indicate a direct effect on activated myeloid cells in PMS. Finally, even though sCD6 results from proteolytic cleavage from its membrane-bound form following T-cell activation, its functional role and relationship to NAC treatment remain uncertain. 12
In summary, this exploratory study suggests NAC may be a promising agent to delay MS progression. However, given the relatively small sample size and short follow-up period, our findings should be considered hypothesis-generating and require confirmation. The ongoing NACPMS trial (NCT05122559) will further elucidate the potential of NAC as a neuroprotective agent in PMS.
Supplemental Material
sj-docx-1-msj-10.1177_13524585261454840 – Supplemental material for High-dose N-acetyl cysteine reduces GFAP levels: Exploratory results from a pilot double-blind, placebo-controlled randomized trial
Supplemental material, sj-docx-1-msj-10.1177_13524585261454840 for High-dose N-acetyl cysteine reduces GFAP levels: Exploratory results from a pilot double-blind, placebo-controlled randomized trial by Vinicius A Schoeps, Raviola Murataj, Akash Virupakshaiah, Carson E Moseley, Kristen M Krysko, Bardia Nourbakhsh, Ferhan Qureshi, Roland Henry and Emmanuelle Waubant in Multiple Sclerosis Journal
Footnotes
Author contributions
E.W. conceived the study design and obtained funding. V.A.S. and R.M. drafted the first version of the manuscript. V.A.S. contributed to the study design and conducted the data analysis. K.M.K. and B.N. participated in the conception and design of the study. F.Q. supervised the biomarker profiling and pre-processing of the data. All authors contributed to the data interpretation and manuscript editing and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: V.A.S. and R.M. have no conflicts of interest to report. A.V. is supported by Fellowship Grants from Biogen, EMD Serono, and Novartis (2022–2024) and is a recipient of the National Multiple Sclerosis Society (NMSS) Sylvia Lawry Fellowship Award (Grant#FP-2307-41848, 2024–2025) and Young Investigator Award from the Race to Erase MS. C.E.M. has received funding from a Neuroscience Research Training Scholarship from the American Academy of Neurology, a Clinician Scientist Development Award Grant FAN-2107-38301 from the National Multiple Sclerosis Society, a Clinician-Scientist Development Award from the Weill Neurohub, and the C.D. Spangler Foundation. He is listed on a patent application related to autoimmune aquaporinopathy. K.M.K. has received grants from MS Canada; a contract for a study site from Roche; speaking/consulting fees from Biogen, EMD Serono, Novartis, and Roche; advisory board member for Biogen, EMD Serono, Novartis, and Roche; scientific advisory committee member for Bristol-Myers Squibb; and adjudication committee member for Moderna. B.N. has been funded by the National Multiple Sclerosis Society, the National Institutes of Health, the US Department of Defense, PCORI, Genentech, and Axsome Therapeutics. He has received consulting honoraria from TG Therapeutics and Alkermes. F.Q. is an employee of Octave Bioscience. R.H. discloses consulting fees from Roche/Genentech, Novartis, Sanofi/Genzyme, QIA, and research support from Roche/Genentech and Atara. E.W. has participated in multicenter clinical trials funded by Genentech, Alexion, and Biogen. She has current support from the NIH, DoD, and Race to Erase MS.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Race to Erase MS (A127771, PI: Waubant) and the National Multiple Sclerosis Society (RG-1611-26299, PI: Oksenberg). The authors also acknowledge the in-kind testing of serum biomarkers by Octave Bioscience, United States.
Data availability statement
The data supporting this study’s findings are available from the study team upon request to the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.