
Abstract
Background:
Black individuals with multiple sclerosis (MS) experience greater disability than White individuals with MS, but the extent to which this disparity is driven by genetic versus environmental factors remains unclear. Social Determinants of Health (SDoH) are significant contributors to varied health outcomes due to their influence on healthcare access and disease management.
Objective:
To evaluate whether socioeconomic disadvantage, measured using the Area Deprivation Index (ADI), attenuates the observed association between race and MS-related disability.
Methods:
In this retrospective study of 1135 patients at a single MS center, we assessed whether accounting for SDoH using the ADI, a composite of neighborhood-level poverty, housing, education, and employment, would attenuate the association between Black race and MS-related disability.
Results:
After adjusting for confounders such as age and vascular risk factors, we found that while Black patients initially had an 86% higher odds of disability, this difference was attenuated to 72% after adjusting for socioeconomic disadvantage using ADI.
Conclusion:
Adjusting for neighborhood-level socioeconomic disadvantage reduces, but does not eliminate, racial disparities in MS-related disability. Persistent differences highlight the need to further examine structural inequities, healthcare access, and additional social determinants contributing to MS outcomes.
Keywords
Introduction
Multiple sclerosis (MS) is a chronic inflammatory disease of the central nervous system, characterized by a heterogeneous disease course and variable clinical outcomes. Increasing evidence suggests that these outcomes are not evenly distributed across racial and ethnic groups. Black individuals with MS experience a higher risk of early disability and a more aggressive disease trajectory compared to White individuals, which may indicate an unequal burden of disease potentially attributable to both biological and social determinants.
Data from 2017 revealed that African Americans with MS scored significantly higher on the Patient-Derived Multiple Sclerosis Severity Score (P-MSS: 4.5 ± 3.0) compared to non-Hispanic Whites (3.4 ± 2.6), even after adjustment for age, indicating greater neurologic impairment. 1 However, these disparities may not be fully explained by biological differences due to race. Marrie et al. 2 found that while Black patients with MS presented with greater disability at diagnosis, subsequent disease progression did not significantly differ from that of White patients when access to care was comparable, suggesting that delayed diagnosis, often a consequence of socioeconomic disadvantage, may play a central role. Supporting this, Harding et al. 3 demonstrated in a large multinational study that lower neighborhood-level socioeconomic status (SES)—a measurement typically reflecting income, education, and occupation—was significantly associated with more rapid disability progression, earlier transition to secondary progressive MS, and lower functional outcomes over time.
This relationship between SES and MS outcomes has also been observed at the structural level. In a study using high-resolution optical coherence tomography, Vasileiou et al. 4 found that individuals from socioeconomically disadvantaged backgrounds experienced faster rates of retinal neurodegeneration, independent of treatment status or comorbidities. These findings suggest that social determinants such as income, education, and neighborhood context may affect disease progression through mechanisms beyond access to disease-modifying therapy alone.
Importantly, these trends persist even in settings with universal healthcare access. He et al., 5 using Swedish national registry data, showed that lower premorbid SES—reflected by education level, income, and marital status—was associated with worse MS outcomes despite the absence of financial barriers to care. These results highlight the potential role of early-life social context and health literacy in shaping long-term neurologic outcomes.
Amezcua and McCauley further underscore the importance of considering both genetic ancestry and structural inequities. Their review emphasized that Black and Hispanic patients may present with additional genetic risk factors—including those that correlate to earlier disease onset and faster accumulation of disability—while also experiencing barriers to diagnosis, clinical trial representation, and treatment access.6–8 More recent reviews expand this perspective, emphasizing that structural racism and systemic barriers to healthcare, including under-resourced neighborhoods, limited access to early care, and chronic stress, may have biological consequences linked to increased MS risk and disability.9,10
Taken together, the existing literature suggests that racial disparities in MS-related disability are shaped not solely by congenital biological factors but by the complex interplay of biological factors and social determinants of health (SDoH), defined as the conditions in the environments in which people are born, live, work, play, worship, and age that influence health outcomes. 11 However, few studies have directly examined how neighborhood-level socioeconomic disadvantage modifies racial disparities in MS-related disability. In this study, we examine the relationship between race, SDoH—as measured by the Area Deprivation Index (ADI)—and neurologic disability among patients with MS in a single-center cohort.
Methods
We conducted a retrospective observational chart review utilizing data from the Ochsner MS center, a Louisiana-based tertiary care facility that serves as a major referral hub for the region. With over 30% of its MS patient population identifying as Black or African American, Ochsner is uniquely positioned to conduct research that addresses racial disparities in MS outcomes. Race was self-reported as American Indian or Alaska Native, Asian, Black or African American, Native Hawaiian or other Pacific Islander, White, or Other. Ethnicity was self-reported as either Hispanic or Latino or Non-Hispanic or Non-Latino. We hypothesized that Non-Hispanic Black patients with MS would have higher levels of disability compared to Non-Hispanic White patients when controlling for age and gender, but that adjusting for socioeconomic disadvantage using the ADI would significantly decrease the observed differences in neurologic disability by race. We categorized individual patients with MS seen at a single timepoint in the Ochsner MS Center between 1 February 2019 and 1 February 2021 by disability status using the validated MS Disease Steps Scale. 12 Covariates collected include age of diagnosis, smoking status, vascular risk factors, including hypertension, hyperlipidemia, diabetes, and Medicaid status. Inclusion criteria are detailed in Figure 1.
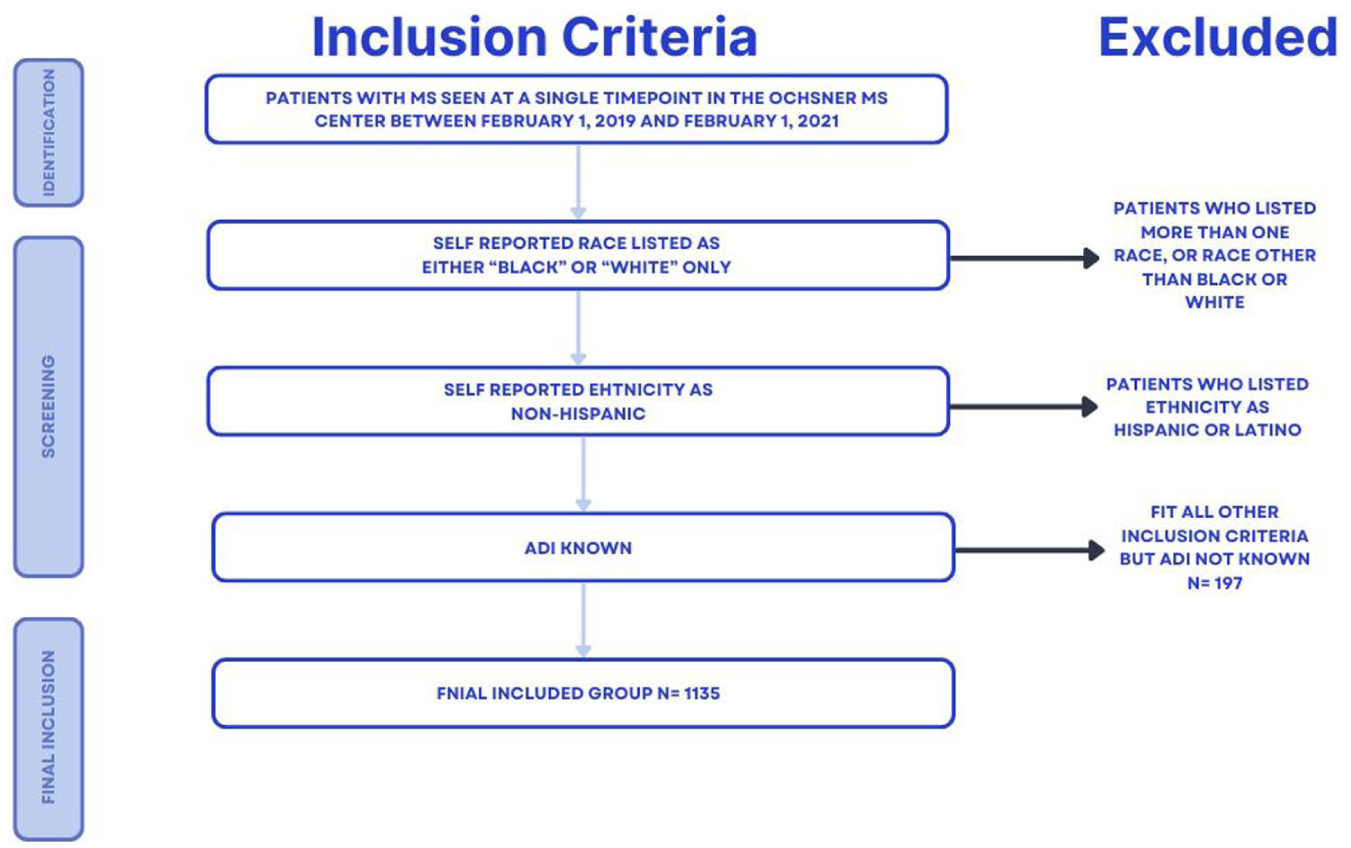
Inclusion and exclusion criteria.
The effect of SDoH was investigated via the ADI. ADI is a composite measure of socioeconomic disadvantage calculated using multiple items from the US Census Bureau American Community Survey (ACS). The items jointly represent the domains of poverty, housing, employment, and education. Rankings based on ADI at the census block group level are made available for download on the University of Wisconsin School of Medicine and Public Health’s Neighborhood Atlas website. These rankings are expressed as national percentiles (1–100) and state deciles (1–10), where a higher value indicates greater deprivation. For example, a block group with a national percentile of 80 is more disadvantaged than 80% of block groups across the country. Residential addresses from our patient cohort were geocoded to identify their corresponding census block groups, which were then matched to ADI values from the Neighborhood Atlas.
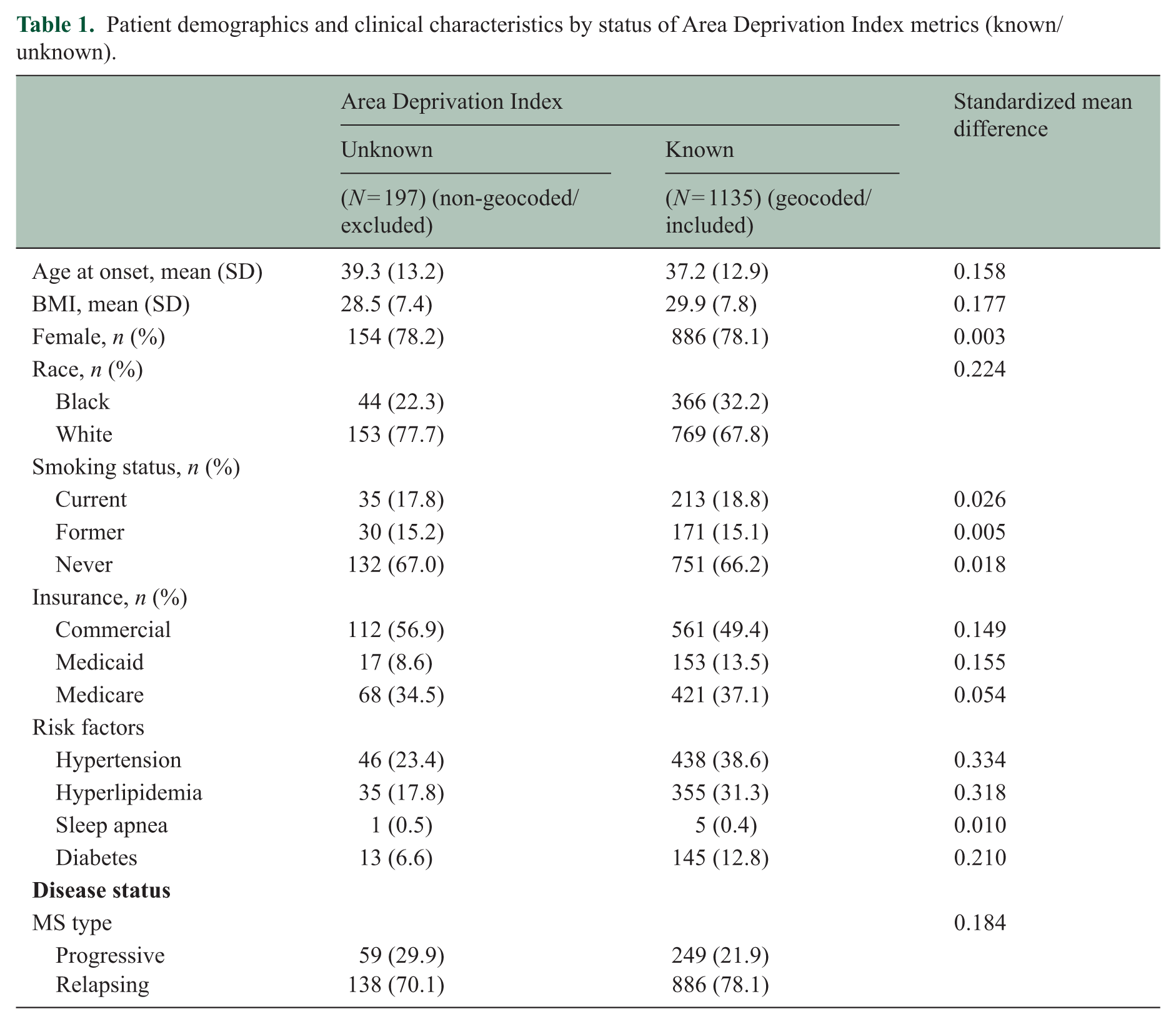
We collected geocoded address data and obtained ADI metrics from the 2017–2021 ACS for 84% (n = 1135) of patients in our sample. Demographics and clinical characteristics of the sample are summarized in Table 1 for patients with (n = 1135) and without (n = 197) geocoded addresses to assess group balance and the potential for introduction of bias into the analysis. The most substantial imbalance is observed in rates of risk factors. There is a smaller percentage of non-geocoded patients with at least one documented risk factor (31% vs 49.7% among geocoded patients). It is unclear whether this discrepancy represents a true difference between groups or is the result of other factors such as sample size, quality of documentation in electronic medical records, or degree of health services utilization.
Patient demographics and clinical characteristics by status of Area Deprivation Index metrics (known/unknown).
The rest of the analysis was done using only the geocoded patient sample, with the caveat that these patients may differ clinically from the rest. All measures are shown by race (Black/White). ADI metrics (national percentile ranking and state decile ranking) are presented as medians and interquartile ranges. For the remaining variables, continuous measures are summarized via means and standard deviations and categorical measures via frequencies and percentages. p values are from Wilcoxon rank-sum tests (ADI), two-sample t-tests (continuous measures), and chi-square or Fisher’s exact tests (categorical measures).
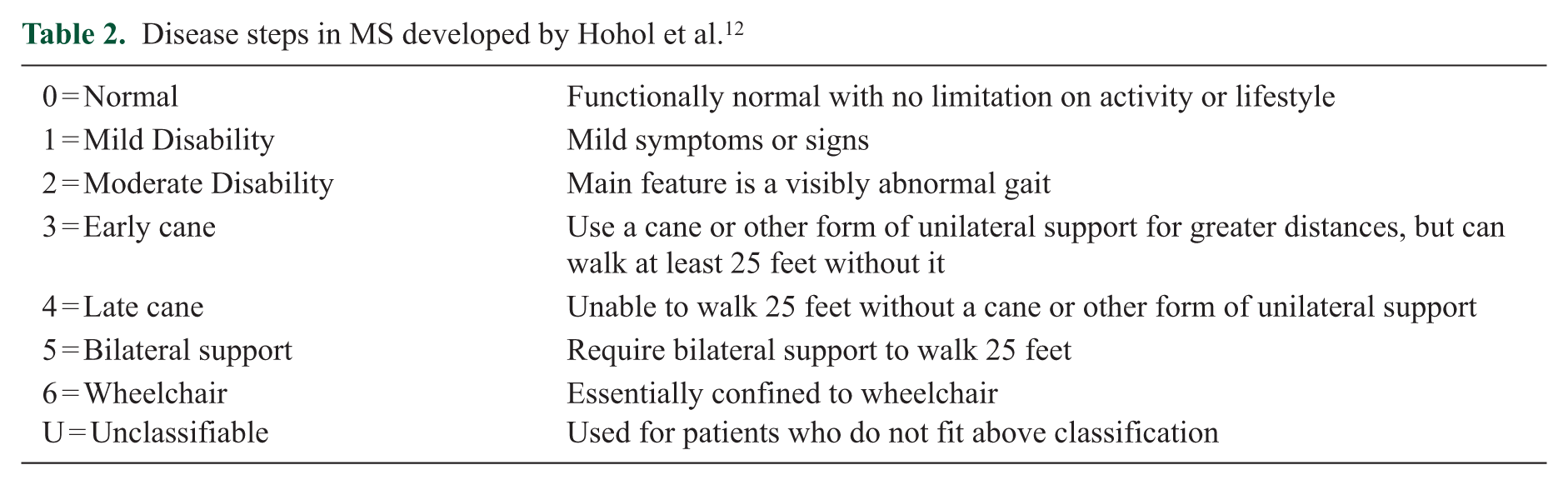
Disability was assessed using the Disease Steps Scale, as shown in Table 2. This scale offers a simple and reproducible method for categorizing functional impairment, has demonstrated high inter-rater reliability, and correlates well with other measures of disability, making it particularly useful for retrospective observational studies. 12
Disease steps in MS developed by Hohol et al.12
To assess racial equality in disease progression, the MS Disease Steps Score data was modeled via ordinal logistic regression. Multiple regression models were explored. The first included a single fixed effect for race to examine the crude association with disease progression. The second added explanatory variables for current age, disease duration, body mass index (BMI), smoking status, hypertension, hyperlipidemia, and diabetes to assess potential confounding of the race effect. The third added a binary indicator of Medicaid coverage to account for the potential impact of insurance status on health outcomes. This last model, Model 1 + Medicaid, captures the effect of race (Black, White) while controlling for age, disease duration, BMI, smoking status (current, former, never), hypertension, hyperlipidemia, diabetes, and Medicaid status.
Then, a region-level covariate for ADI national percentile ranking was added to Model 1 to capture neighborhood-level SDoH. This model (Model 1 + Medicaid + ADI) is used to investigate whether socioeconomic disadvantage contributes to the association between race and disability after accounting for all covariates from Model 1. Odds ratios (ORs) for disability scores in Black versus White patients are presented with 95% confidence intervals in Table 3 for each version of the model. All analyses were performed at significance level 0.05 and carried out using SAS version 9.4 for Windows.
Patient demographics and clinical characteristics by race.
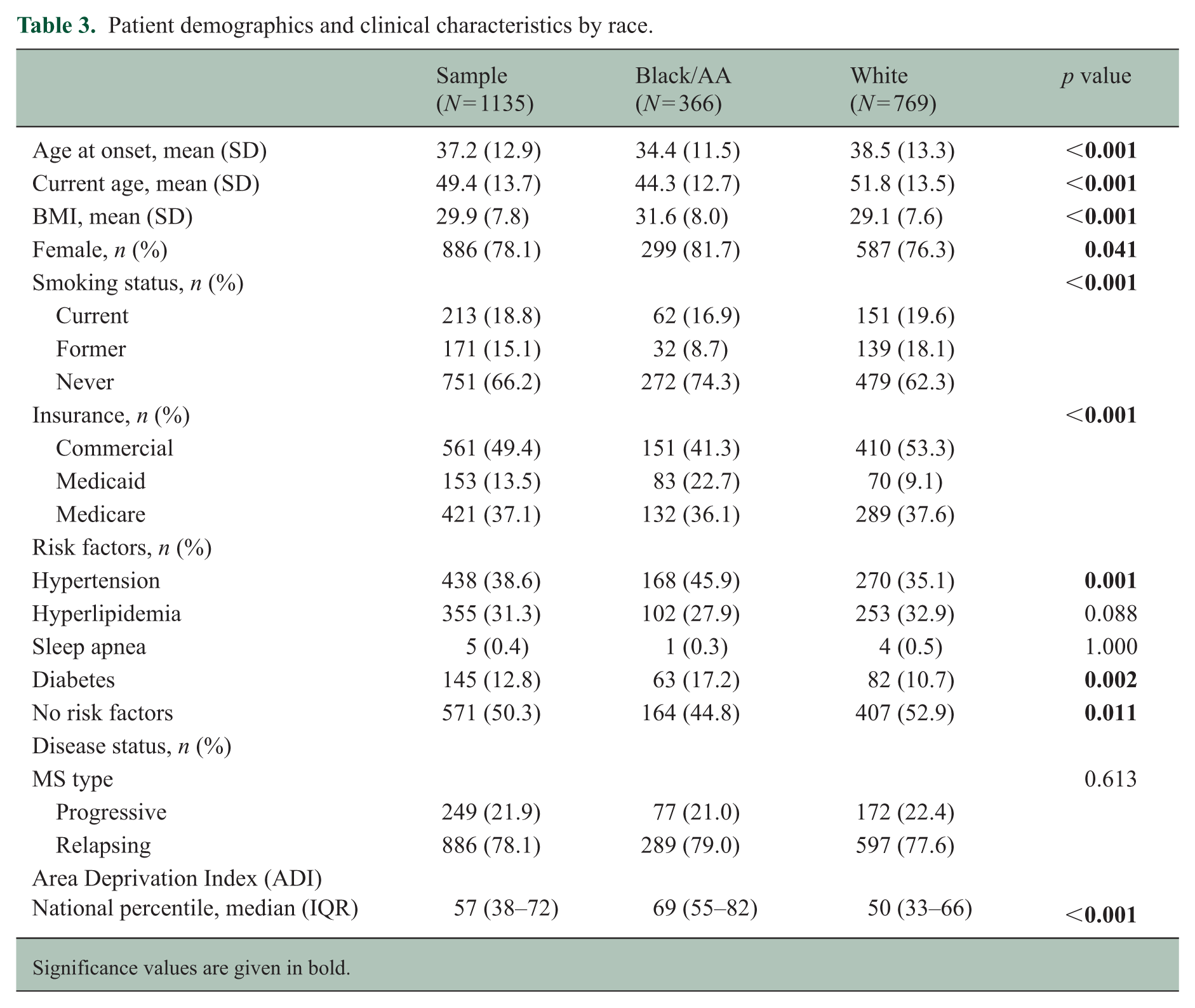
Significance values are given in bold.
Results
Table 1 presents demographic and clinical characteristics for patients with and without known ADI data. Among the geocoded cohort (n = 1135), 32.2% were Black and 67.8% White. The average age at onset was 37.2 years, an average BMI of 29.9. 78.1% of the population was female, 21.9% male. Notably, the geocoded group had higher rates of vascular risk factors (hypertension, hyperlipidemia, diabetes), which were controlled for in the final models. Table 1 shows patient demographics and clinical characteristics by status of Area Deprivation Index metrics (included/excluded).
In the model including Medicaid status and vascular risk factors (Model 1 + Medicaid), Black patients with MS had 86% higher odds of having more advanced disability than White patients (OR: 1.86, 95% confidence interval [CI]: 1.46–2.38). However, when socioeconomic disadvantage was incorporated into the model using ADI, the observed racial disparity in disability was attenuated such that Black patients had 72% higher odds of greater disability (OR: 1.72, 95% CI: 1.34–2.22), a 7.6% decrease in odds.
Table 4 displays the ORs for disability by race across the adjusted model, as well as the unadjusted model.
Odds ratios for more advanced disease progression in Black patients versus White patients.
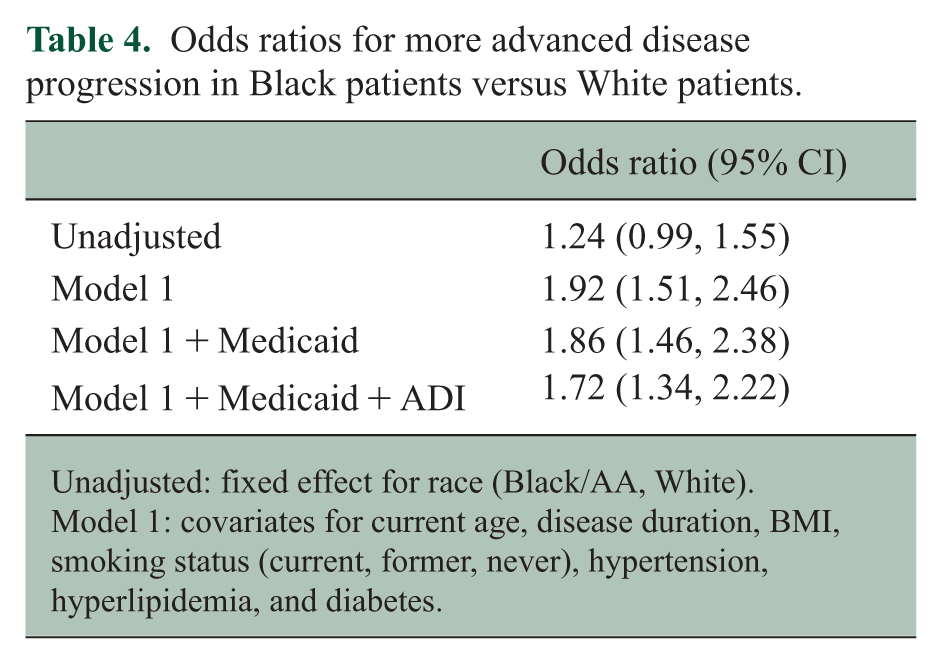
Unadjusted: fixed effect for race (Black/AA, White).
Model 1: covariates for current age, disease duration, BMI, smoking status (current, former, never), hypertension, hyperlipidemia, and diabetes.
Discussion
This study demonstrates that socioeconomic disadvantage attenuates the observed disparity in MS-related disability between Black and White patients. After accounting for SDoH using ADI, the magnitude of the difference between Black and White patients changed the difference in odds of disability from 86% to 72%. These findings support the hypothesis that differences in socioeconomic context—rather than race alone—may play a substantial role in disability outcomes among patients with MS. These findings are summarized in Figure 2. Furthermore, this study demonstrates that while adjusting for socioeconomic disadvantage attenuates the disparity in MS-related disability between Black and White patients, it does not eliminate it. After accounting for ADI, Black patients continued to show higher odds of greater disability, suggesting that additional, unmeasured factors may contribute to this disparity.
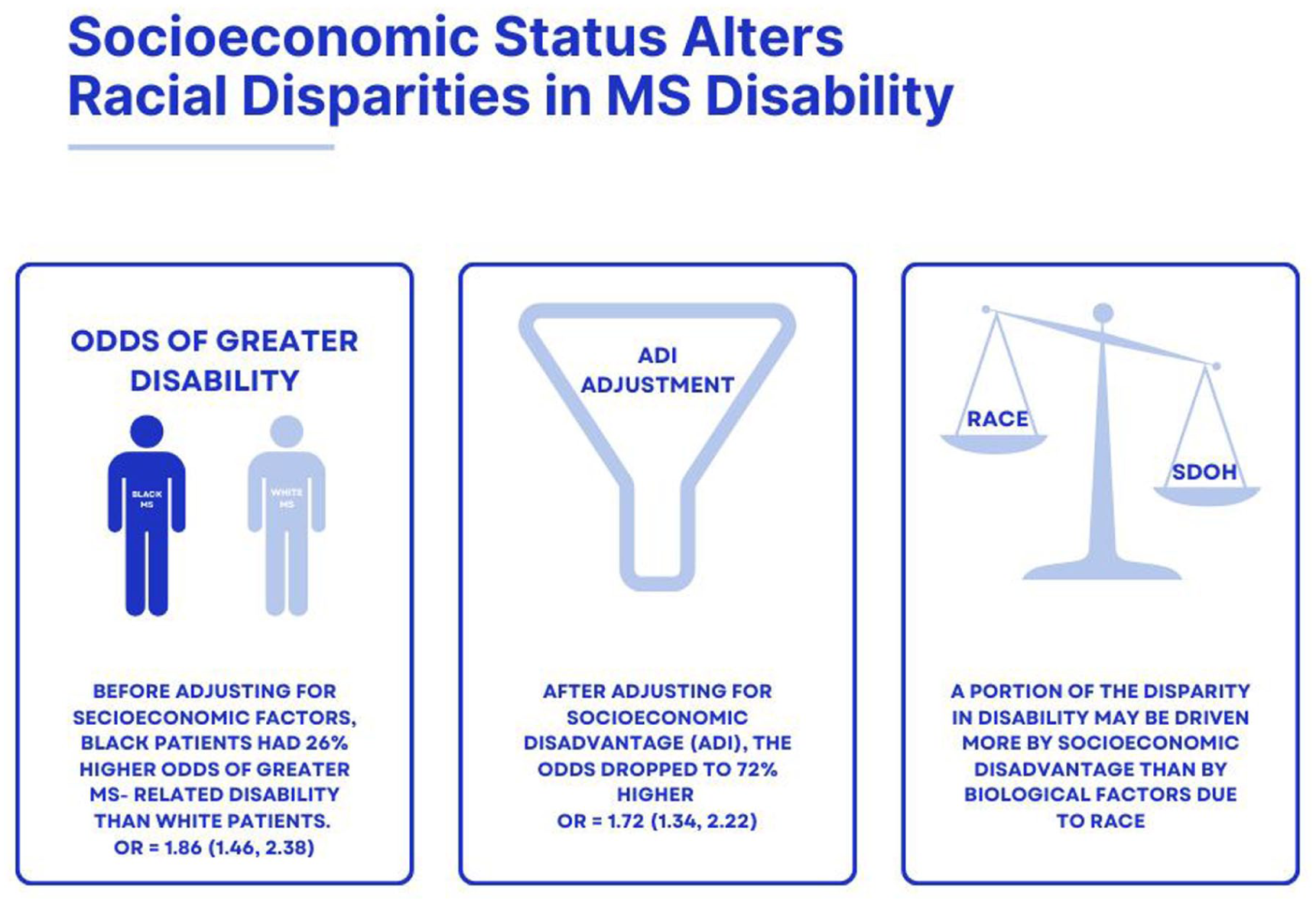
Summary of findings.
While our study did not directly measure structural inequities, the Area Deprivation Index serves as a proxy for neighborhood-level socioeconomic disadvantage, which is itself a product of long-standing structural and environmental inequities. These include disparities in education, employment opportunities, housing quality, and access to healthcare resources. Thus, our findings suggest that the conditions under which people live and receive care—shaped by decades of policy and systemic barriers—may contribute significantly to observed disparities in MS disability. This study contributes to a growing body of literature suggesting that socioeconomic disadvantage is a critical, modifiable determinant of MS outcomes, with implications for both clinical practice and health policy.
This study has several important limitations. First, its retrospective design limits our ability to establish causal relationships and is inherently more vulnerable to information and selection biases than prospective designs. In addition, this study classified race based on self-reported data, which, while practical, may introduce inaccuracies and oversimplify the complexity of racial identity.
Second, SDoH was measured at the neighborhood level (via ADI) and may not capture individual-level variables such as personal income, education, or employment. To better capture the impact of racial inequity, future work should also consider measures such as the Index of Concentration at the Extremes (ICE) and the Everyday Discrimination Scale (EDS), which reflect structural and interpersonal racism more directly than ADI alone.13,14 These tools may clarify how systemic disadvantage contributes to disparate MS outcomes beyond SES. Third, this study was conducted at a single center in Louisiana, and results may not generalize to MS populations in other geographic regions or healthcare systems. Finally, while we controlled for vascular comorbidities, this study did not assess time to diagnosis, access to MS specialists, adherence to disease-modifying therapy (DMT), or health literacy, all of which are potential confounders in the relationship between SDoH and disability. This work should be interpreted within the context of these limitations.
Conclusion
This study contributes to growing evidence that racial disparities in MS-related disability may be partially attributable to socioeconomic disadvantage rather than intrinsic biological differences. These findings underscore the urgent need to address systemic inequities related to SDoH such as access to care, early diagnosis, and long-term disease management, especially in marginalized communities. Future prospective studies incorporating both individual- and neighborhood-level SDoH data, as well as longitudinal clinical outcomes, are warranted to further elucidate the mechanisms by which social context shapes disease progression in MS.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical considerations
The study received ethical approval from Ochsner Clinic Foundation IRB (no. 2021.015) on 29 January 2021. This is an IRB-approved retrospective study; patient consent was not required.
Consent to participate
Not applicable.
Consent for Publication
Not applicable.
Data availability statement
The data supporting this study are available from the corresponding author upon reasonable request and in a deidentified format.