
Abstract
Background:
In multiple sclerosis (MS), real-world evidence supports early intensive treatment (EIT) with high-efficacy therapies (HET) over escalation (ESC), although comparative data on long-term safety across sequences remain limited.
Objective:
To compare the incidence of infections and neoplasms in patients treated with different treatment sequences.
Methods:
Data were extracted from the Italian MS and Related Disorders Register. DMTs were classified as moderate-efficacy treatment (MET), continuous HET (C-HET) or pulsed HET (P-HET). Six therapeutic sequences were reconstructed: MET-only, C-HET-only, P-HET-only, MET→C-HET, MET→P-HET and P-HET→MET. Incidence rates (IRs; per 1000 person-years) and incidence rate ratios (IRRs) were estimated using multivariable Poisson regression, adjusting for age, sex, Expanded Disability Status Scale (EDSS), disease duration, MS phenotype and prior relapse activity.
Results:
A total of 37,375 patients were included in the analysis, with a median duration of treatment exposure of 8.8 years. Infection risk was significantly higher with C-HET-only (IR, 24.82; IRR, 3.12), P-HET-only (IR, 13.43; IRR, 1.69), MET→C-HET (IR, 10.46; IRR, 1.32) and MET→P-HET (IR, 12.30; IRR, 1.55) versus MET-only (IR, 7.94), while P-HET→MET showed no significant difference from MET-only (IR, 7.67; IRR, 0.97). Regarding neoplasm incidence, P-HET-only showed the lowest rates (IR, 0.18; IRR, 0.24), whereas it was significantly higher in C-HET-only (IR, 1.33; IRR, 1.79) and MET→C-HET (IR, 1.01; IRR, 1.36) versus MET-only (IR, 0.74).
Conclusions:
This is the first real-world study to compare the safety of different sequences in a national registry. ESC strategies did not confer a long-term safety advantage over EIT. Among HET regimens, C-HET was associated with the greatest risk of both serious infections and neoplasms, whereas P-HET showed the lowest neoplasm incidence.
Keywords
Background
Over the past two decades, the therapeutic landscape of multiple sclerosis (MS) has evolved substantially, reshaping treatment goals and clinical decision-making. The introduction of an expanding armamentarium of disease-modifying therapies (DMTs) has dramatically altered the natural course of the disease.1,2
According to the European Medicines Agency (EMA) Guideline on clinical investigation of medicinal products for the treatment of multiple sclerosis (Revision 2, 2015), 3 DMTs are categorized by their efficacy in reducing relapse rate and magnetic resonance imaging (MRI) activity, as well as their safety profile. This framework – harmonized with the European Committee for Treatment and Research in Multiple Sclerosis and European Academy of Neurology (ECTRIMS/EAN) Guideline on the pharmacological treatment of people with multiple sclerosis (2024) – supports a functional classification of DMTs into moderate-efficacy treatments (METs), including interferon-β (IFNβ), glatiramer acetate (GA), teriflunomide (TRF) and dimethyl fumarate (DMF), and high-efficacy treatments (HETs), such as natalizumab (NTZ), alemtuzumab (ALEM), anti-CD20 monoclonal antibodies, cladribine (CLAD) and sphingosine 1-phosphate (S1P) receptor modulators. Among HETs, a further distinction is made between continuous (C-HET) and pulsed (P-HET) therapies, depending on the pattern of administration and immunologic effect. The MET/HET framework remains valid and widely adopted within European and national regulatory systems. 3 In Italy, the AIFA Determination No. 67/2024 4 (published in the Gazzetta Ufficiale on 5 April 2024) officially integrated this efficacy-based classification into national prescribing criteria, particularly within therapeutic plans for treatment-naïve patients with active disease and those eligible for switch strategies. Depending on the clinical context, this action explicitly endorses both the escalation (ESC) strategy – initiating with MET and switching to HET depending on disease activity – and the early intensive treatment (EIT) approach, in alignment with EMA and ECTRIMS/EAN guidance.3,5
Within this context, the debate between EIT and ESC approaches remains central to MS pharmacological management.6,7 The EIT strategy advocates prompt initiation of HETs soon after diagnosis to induce durable disease stability and prevent irreversible neurodegeneration, whereas ESC favours a stepwise approach, beginning with safer METs and escalating to HET only in the presence of clinical or radiological breakthrough. 8
Although real-world evidence (RWE) and registry-based studies have demonstrated the superior disease control achieved with EIT, for example, reduction in relapse rates, MRI activity and disability accumulation, the comparative safety profiles of EIT strategies remain incompletely understood. Concerns persist about the long-term immunological consequences of sustained immune modulation, particularly regarding the risk of serious infection and malignancy. Randomized controlled trials (RCTs) are not ideally designed to capture long-term or cumulative risks, given their limited duration, restricted inclusion criteria and absence of treatment sequencing. 7 Therefore, large-scale RWE studies and registry-based analyses represent the most appropriate methodological framework to explore major safety outcomes across different clinical scenarios.9,10
Although recent registry studies, including those from MSBase and the Swedish MS Registry, have advanced our understanding of DMT efficacy and long-term outcomes, systematic evaluations of serious adverse events (SAEs) across therapeutic sequences – especially distinguishing between C-HET and P-HET – remain limited. This distinction is clinically meaningful because C-HETs, such as anti-CD20 monoclonal antibodies, exert sustained immunosuppression effects through continuous immune-cell depletion, whereas P-HET affords transient immune reconstitution with potential for immune restoration between cycles. Whether these distinct immunobiological mechanisms translate into different real-world safety profiles remains unclear. 11 To address this knowledge gap, we employed data from the Italian Multiple Sclerosis and Related Disorders Register (I-MS&RD) – one of the largest and most comprehensive national MS databases – to assess the incidence and relative risk of serious infections and neoplasms across DMT classes and therapeutic sequences. By delineating the safety trajectories of C-HET and P-HET regimens and comparing EIT and ESC strategies, this study aims to generate robust, population-based evidence to inform therapeutic sequencing and long-term therapeutic risk–benefit appraisal in MS.
Methods
Study design and data source
This is a retrospective observational cohort study based on prospectively collected clinical data from the I-MS&RD. Data extraction was performed on 30 April 2025. The I-MS&RD is a nationwide, web-based registry established by the Italian MS Foundation (FISM) and the Italian MS Society (AISM) used to systematically collect demographic, clinical and therapeutic data from more than 200 MS centres across Italy. Data quality is continuously ensured through automated validation algorithms and periodic audits by a central coordinating team. 12
The I-MS&RD was approved by the Ethics Committee of the Azienda Ospedaliero-Universitaria Policlinico of Bari (Study ID: REGISTRO SM001, approved on 8 July 2016) and by the local ethics committees of all participating centres. The study was conducted in accordance with the Declaration of Helsinki. All patients provided written informed consent authorizing the use of their anonymized data for research purposes.
Eligible participants were adults aged 18 years or above with a relapsing MS phenotype – relapsing-remitting (RRMS) or active secondary-progressive MS (SPMS) – diagnosed according to the 2017 McDonald criteria. Study inclusion required at least one DMT and a minimum of one baseline and two follow-up visits after treatment initiation. Patients with incomplete records (missing core dataset) or a primary progressive disease course were excluded (Figure 1).
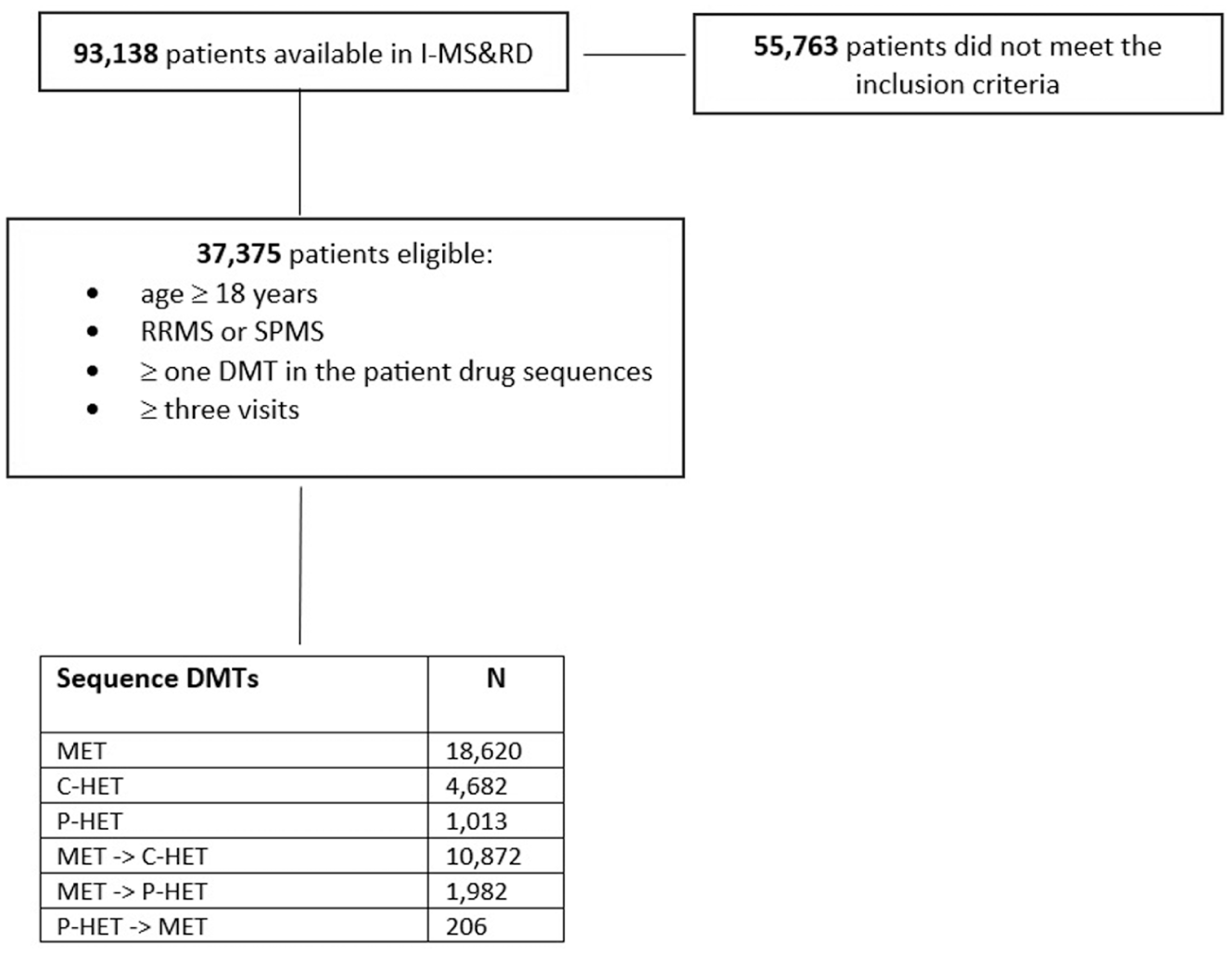
Flowchart of the patient selection procedure.
Baseline was defined as the date of the first DMT prescription. Demographic and clinical characteristics (age, sex, disease duration, Expanded Disability Status Scale (EDSS) score, relapse history and MRI activity) were assessed at this point and stratified by therapeutic sequence.
DMTs were categorized according to the EMA guideline: 3
MET: IFNβ (all formulations), GA, TRF, DMF;
C-HET: FNG (fingolimod), SP (siponimod), NTZ, OCRE (ocrelizumab), RTX (rituximab);
P-HET: CLAD, ALEM, Mitoxantrone (MX).
Based on these categories, six therapeutic sequences were reconstructed (Supplementary Figure 1): three representing single-category exposure throughout follow-up (MET-only, C-HET-only, P-HET-only) and three capturing treatment transitions (MET→C-HET, MET→P-HET and P-HET→MET). Other treatment sequences were excluded due to the limited number of patients. The distribution of individual DMTs within each therapeutic sequence is shown in Table 1.
Distribution of DMTs between therapeutic sequences (% given in brackets).
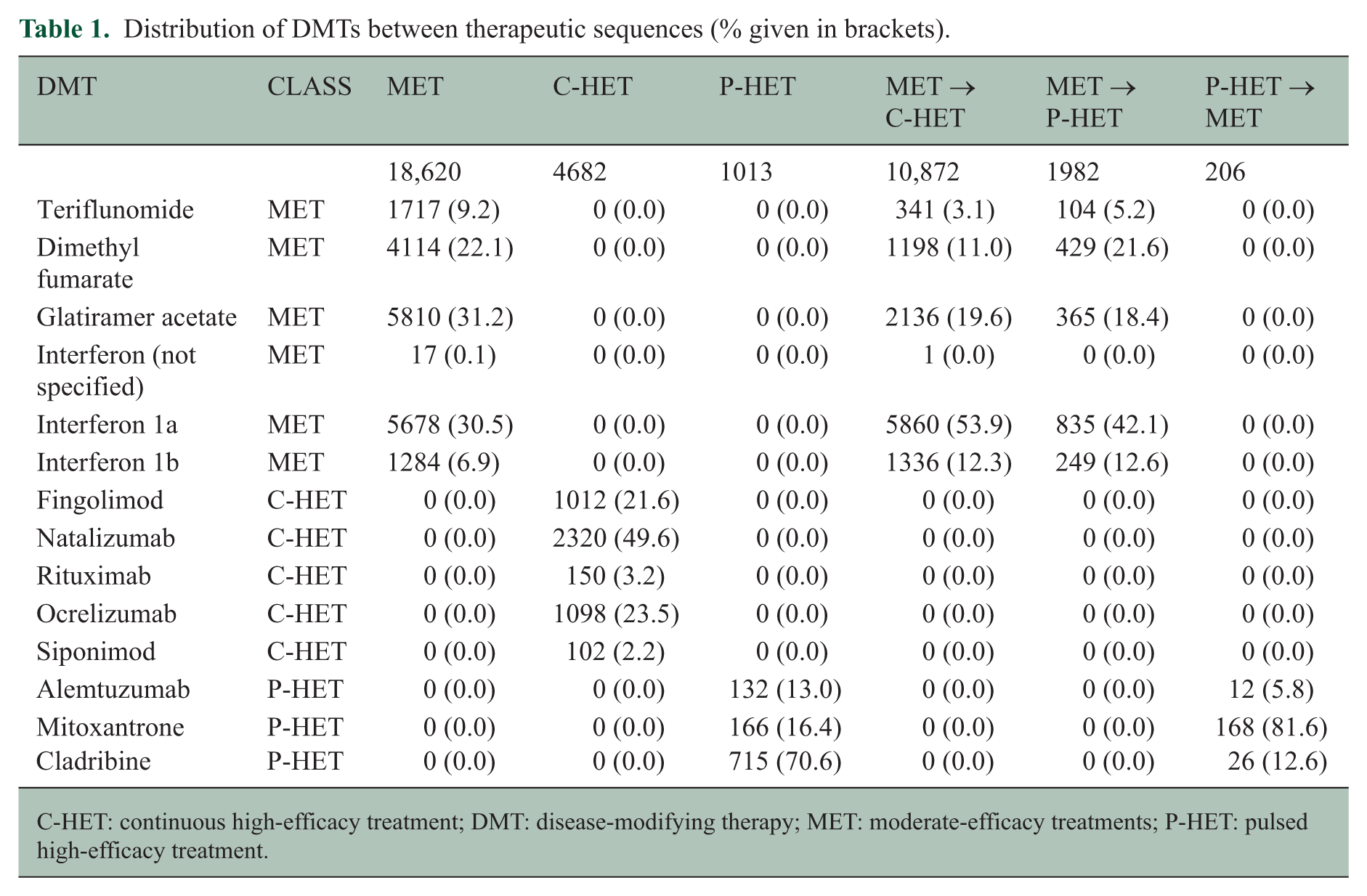
C-HET: continuous high-efficacy treatment; DMT: disease-modifying therapy; MET: moderate-efficacy treatments; P-HET: pulsed high-efficacy treatment.
The following SAEs were considered in the analysis: severe infections and neoplasms (including malignancies) selected using the Medical Dictionary for Regulatory Activities (MedDRA) terminology reported in dedicated records of the I-MS&RD (see Supplementary Tables 1 and 2 for the list of MedDRA codes).
Each DMT was assigned a specific post-exposure risk window reflecting its pharmacodynamic duration and potential carry-over effects (Supplementary Table 3). When patients switched therapy, they remained attributed to both DMT cohorts until the end of each respective risk window. Outcomes were evaluated during the entire follow-up and, for two-class sequences, within each exposure period to determine temporal changes in risk.
Statistical analysis
General characteristics of the study population were summarized as medians with interquartile ranges (IQR) for continuous variables and as percentages for categorical variables. For each therapeutic sequence, baseline characteristics were established at the time of initiation of the first DMT.
The outcomes of interest were SAEs, specifically serious infections and neoplasms. Because participants could experience multiple events, the risk of SAEs was expressed as the number of events per 1000 person-years (PYs), estimated using Poisson regression models adjusted for over-dispersion to account for variance inflation. In cases with zero events, the Garwood exact correction was applied. Poisson regression was selected over alternative count-data models based on superior goodness-of-fit, as indicated by lower Akaike information criterion (AIC) values. Person-years were defined as the sum of exposure time for all individuals at risk, calculated from the start date of a DMT to the date of SAE occurrence, treatment discontinuation (including the risk window), or end of observation.
Results were reported as incidence rates (IRs) with corresponding 95% confidence intervals (95% CI) and incidence rate ratios (IRRs). IRRs were assessed using the MET class as the reference category. IRs and IRRs were adjusted for the following baseline covariates assessed at the time of first DMT initiation: age, sex, EDSS score, disease duration, MS phenotype and relapse activity in the 2 years preceding treatment onset.
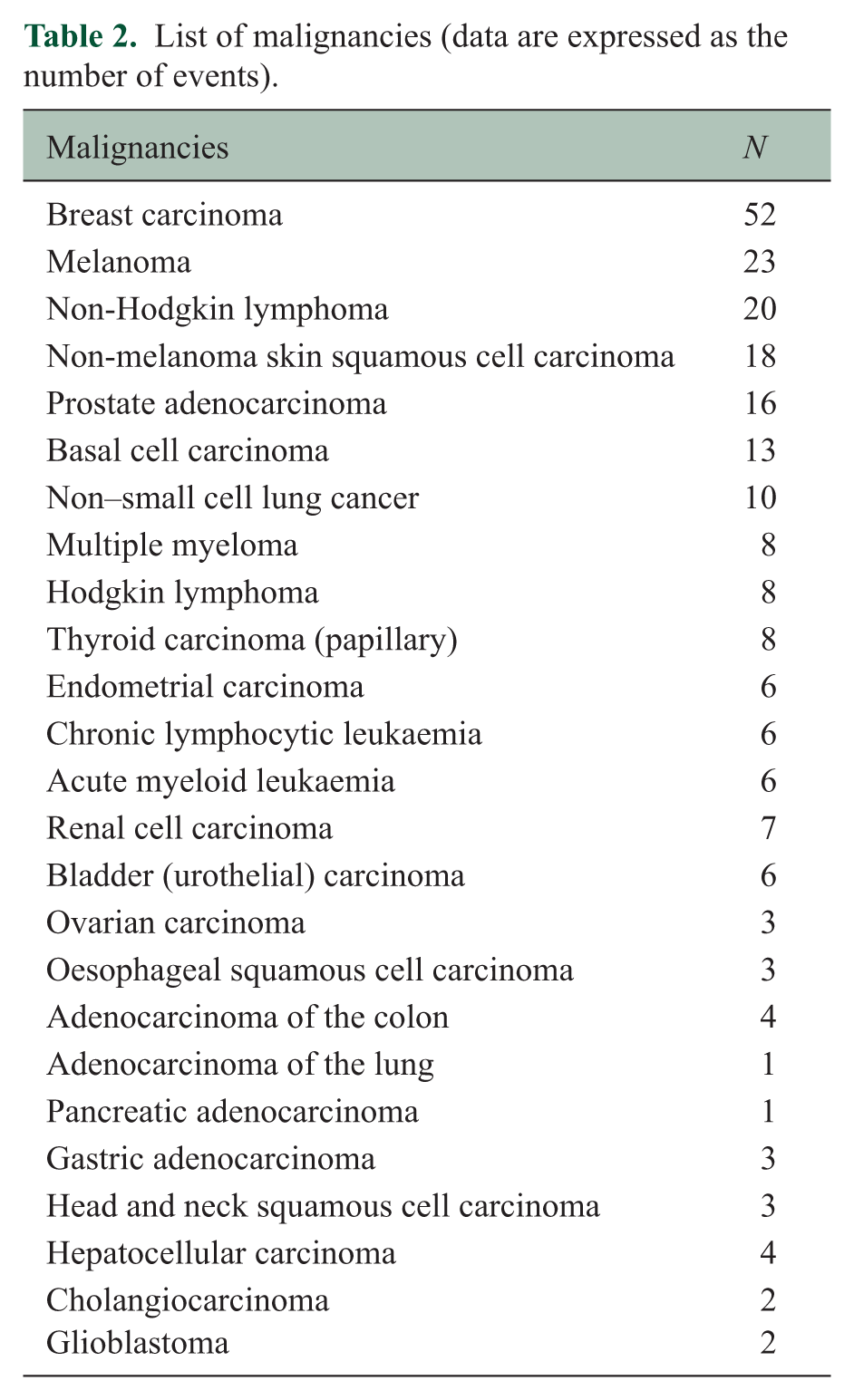
The incidence of SAEs was assessed over the total treatment exposure and stratified by two consecutive exposure periods in patients receiving multiple DMT classes to evaluate potential trends in SAE occurrence during follow-up. Given the limited number of malignancies, a detailed list is provided in Table 2.
List of malignancies (data are expressed as the number of events).
A two-tailed p value < 0.05 was considered statistically significant. All analyses were performed using R software, version 4.2.3 (R Foundation for Statistical Computing, Vienna, Austria).
Results
A total of 37,375 patients were included in the analysis, of whom 67.5% were women and 99.2% had an RRMS course. The median age at first DMT prescription was 36.0 years (IQR: 28.5–45.0), with a median EDSS score of 2.0 (IQR: 1.0–3.0) (Table 3).
Patient cohort characteristics.
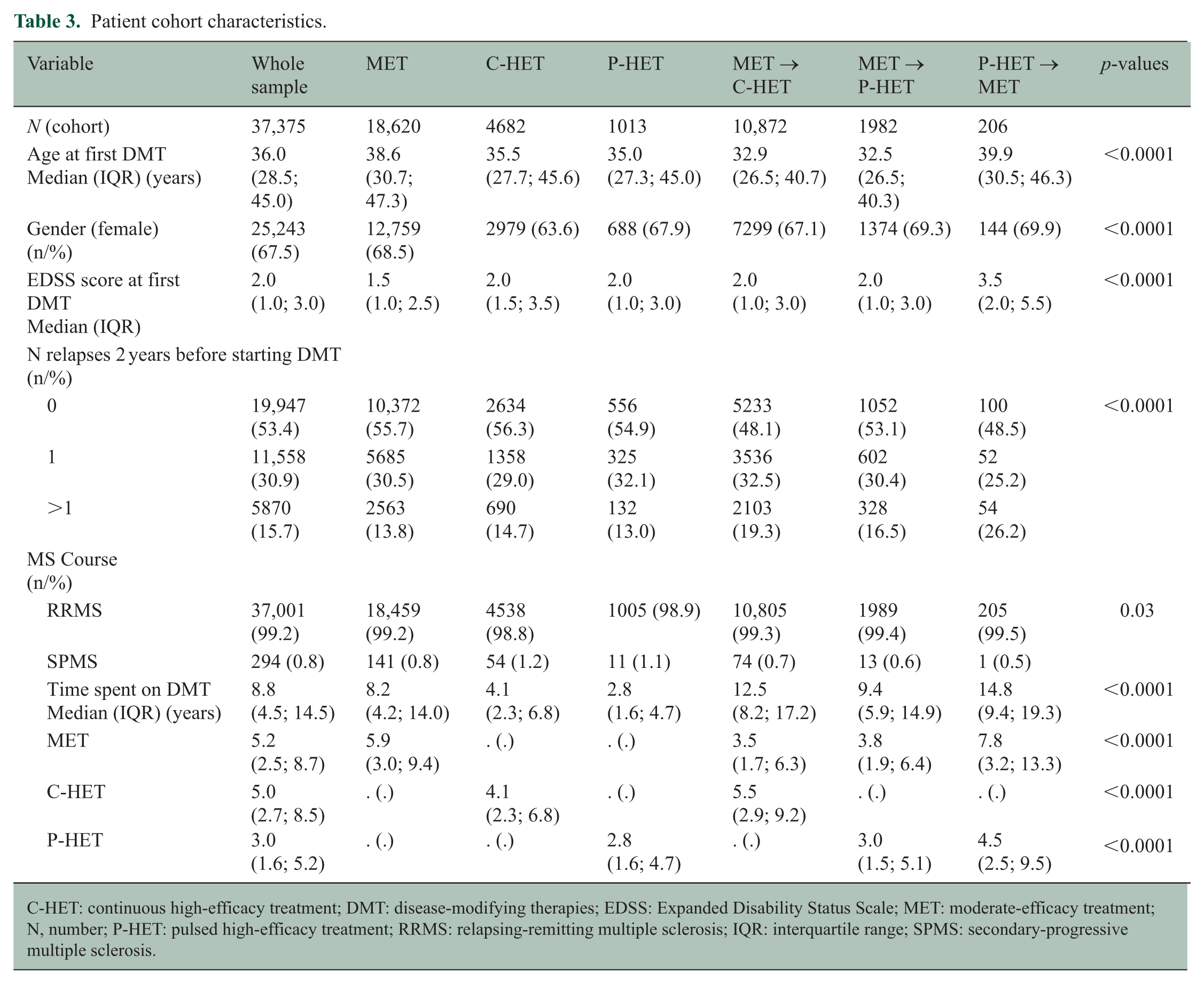
C-HET: continuous high-efficacy treatment; DMT: disease-modifying therapies; EDSS: Expanded Disability Status Scale; MET: moderate-efficacy treatment; N, number; P-HET: pulsed high-efficacy treatment; RRMS: relapsing-remitting multiple sclerosis; IQR: interquartile range; SPMS: secondary-progressive multiple sclerosis.
Patients treated exclusively with MET represented the largest subgroup (n = 18,620), followed by those with the MET to C-HET sequence (n = 10,872) and by those who received only C-HET (n = 4682). The smallest group was P-HET to MET (n = 206). Baseline disease activity differed within groups, with the P-HET to MET subgroup demonstrating the greatest proportion of patients experiencing multiple relapses in the 2 years preceding treatment onset (26.2%). Conversely, those treated only with MET, C-HET or P-HET exhibited comparatively lower relapse frequencies.
The overall median treatment duration was 8.8 years (IQR: 4.5–14.5), ranging from 2.8 years in P-HET-only to 14.8 years in P-HET to MET sequences. All baseline and exposure characteristics significantly differed across therapeutic sequences (p < 0.0001; Table 3).
Serious infections
Patients continuously treated with C-HET displayed the highest infection rate (IR: 24.82; 95% CI: 19.86–31.01; IRR: 3.12; 95% CI: 2.81–3.48; p < 0.0001) compared with MET-only (IR: 7.94; 95% CI: 6.43–9.81). A significantly increased risk was also observed in patients treated exclusively with P-HET (IR: 13.43; 95% CI: 9.36–19.28; IRR: 1.69; 95% CI: 1.25–2.29; p = 0.0008), in those who escalated from MET to C-HET (IR: 10.46; 95% CI: 8.48–12.91; IRR: 1.32; 95% CI: 1.22–1.43; p < 0.0001), and from MET to P-HET (IR: 12.30; 95% CI: 9.66–15.67; IRR: 1.55; 95% CI: 1.34–1.79; p < 0.0001). By contrast, infection rates were comparable to MET-only in patients who de-escalated from P-HET to MET (IR: 7.67; 95% CI: 4.42–13.30; IRR: 0.97; 95% CI: 0.58–1.61; p = 0.89) (Table 4, Figure 2, Panel a).
Rates of infections in each treatment group; data presented as IR, 95% CI per 1000 patient years, and IRR.
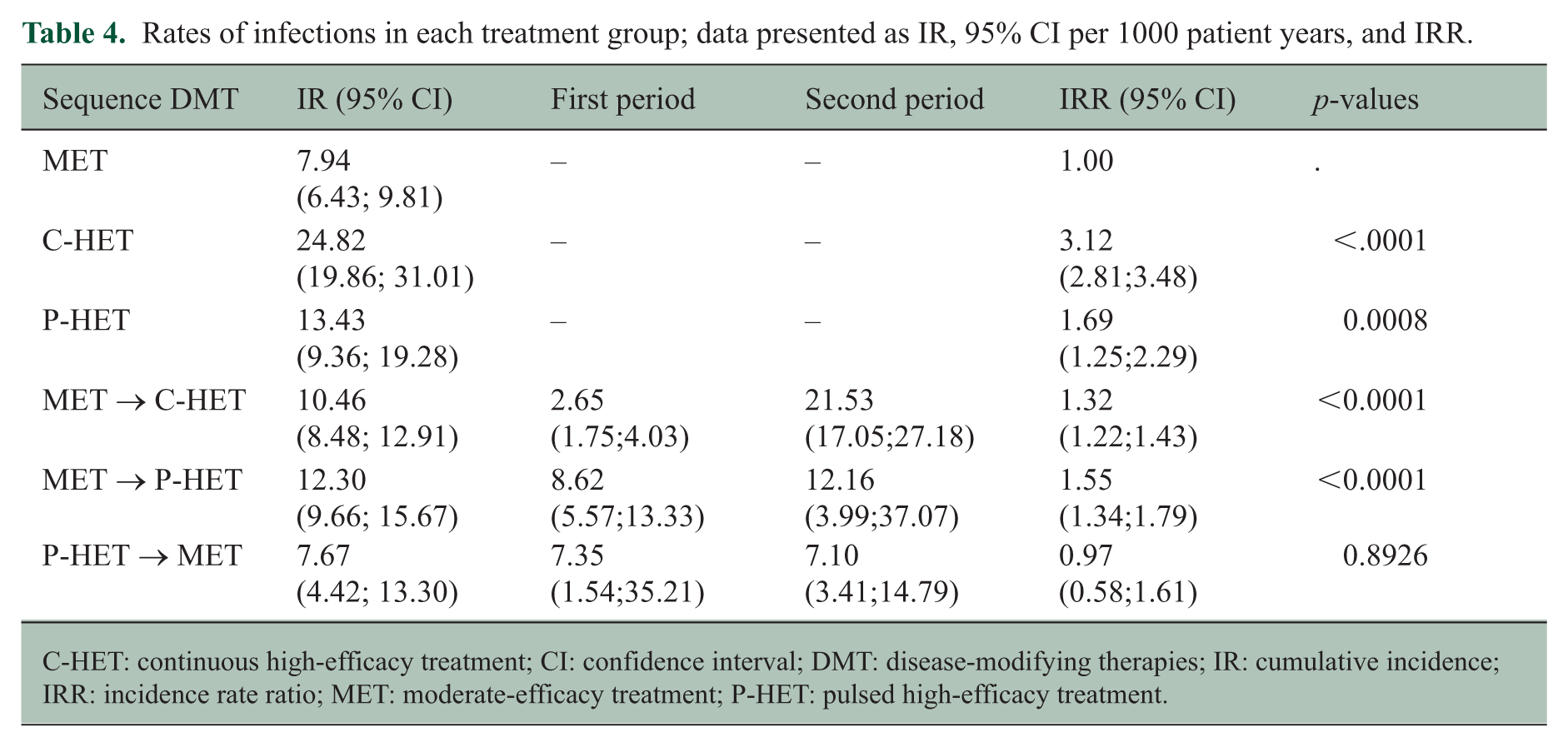
C-HET: continuous high-efficacy treatment; CI: confidence interval; DMT: disease-modifying therapies; IR: cumulative incidence; IRR: incidence rate ratio; MET: moderate-efficacy treatment; P-HET: pulsed high-efficacy treatment.
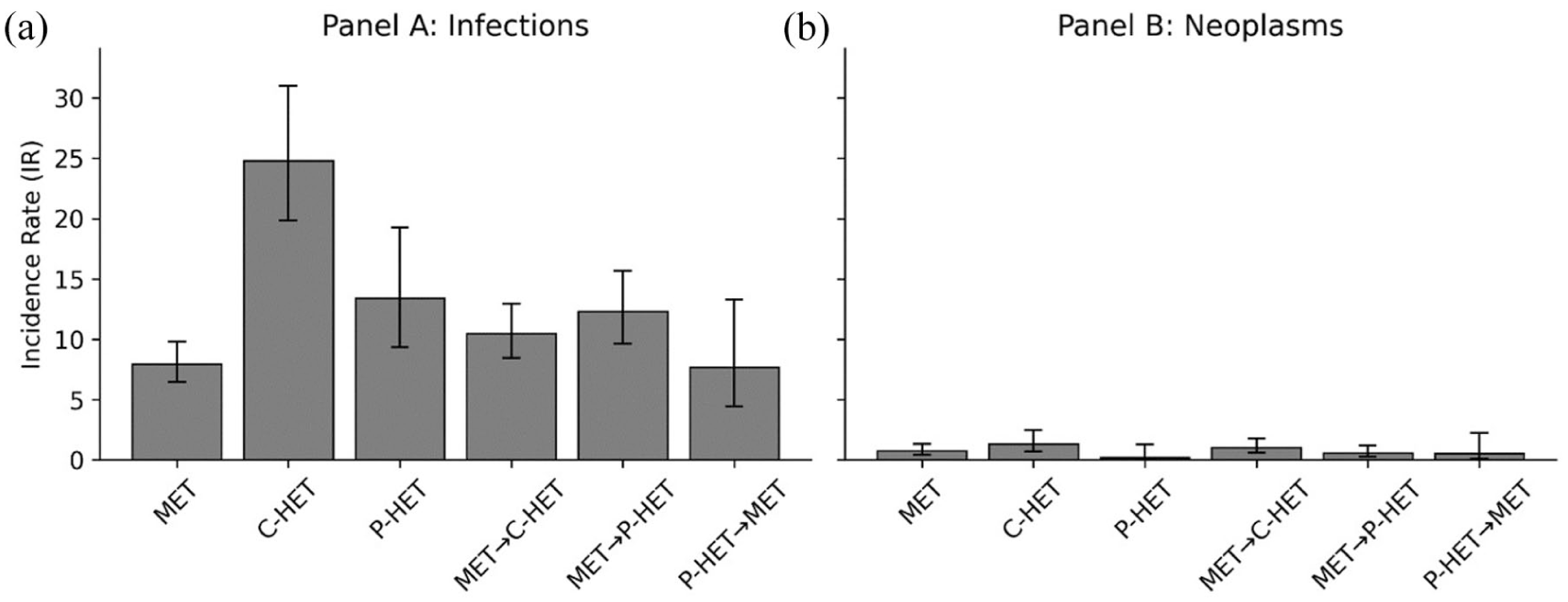
Adjusted incidence rates of serious infections (Panel a) and neoplasms (Panel b) across therapeutic sequences.
When stratified by treatment period, the infection IR increased markedly during the second treatment period in MET→C-HET (from 2.65 to 21.53) and remained elevated across both periods in MET→P-HET (8.62 and 12.16, respectively). In P-HET→MET, infection IRs remained stable across both periods (7.35 and 7.10, respectively) (Table 4).
Neoplasms
Compared with MET-only (IR: 0.74; 95% CI: 0.42–1.31), a significantly higher neoplasm incidence was observed in C-HET-only (IR: 1.33; 95% CI: 0.71–2.48; IRR: 1.79; 95% CI: 1.29–2.48; p = 0.0005) and in patients who escalated from MET to C-HET (IR: 1.01; 95% CI: 0.57–1.78; IRR: 1.36; 95% CI: 1.12–1.66; p = 0.0024). By contrast, P-HET-only (IR: 0.18; 95% CI: 0.03–1.27; IRR: 0.24; 95% CI: 0.04–1.60; p = 0.14), MET→P-HET (IR: 0.58; 95% CI: 0.28–1.20; IRR: 0.78; 95% CI: 0.48–1.28; p = 0.33), and P-HET→MET (IR: 0.52; 95% CI: 0.12–2.24; IRR: 0.71; 95% CI: 0.18–2.71; p = 0.61) showed lower incidence rates than MET-only, though these differences did not reach statistical significance (Table 5, Figure 2, Panel b).
Rates of neoplasms in each treatment group; data presented as IR, 95% CI per 1000 patient years, and IRR.
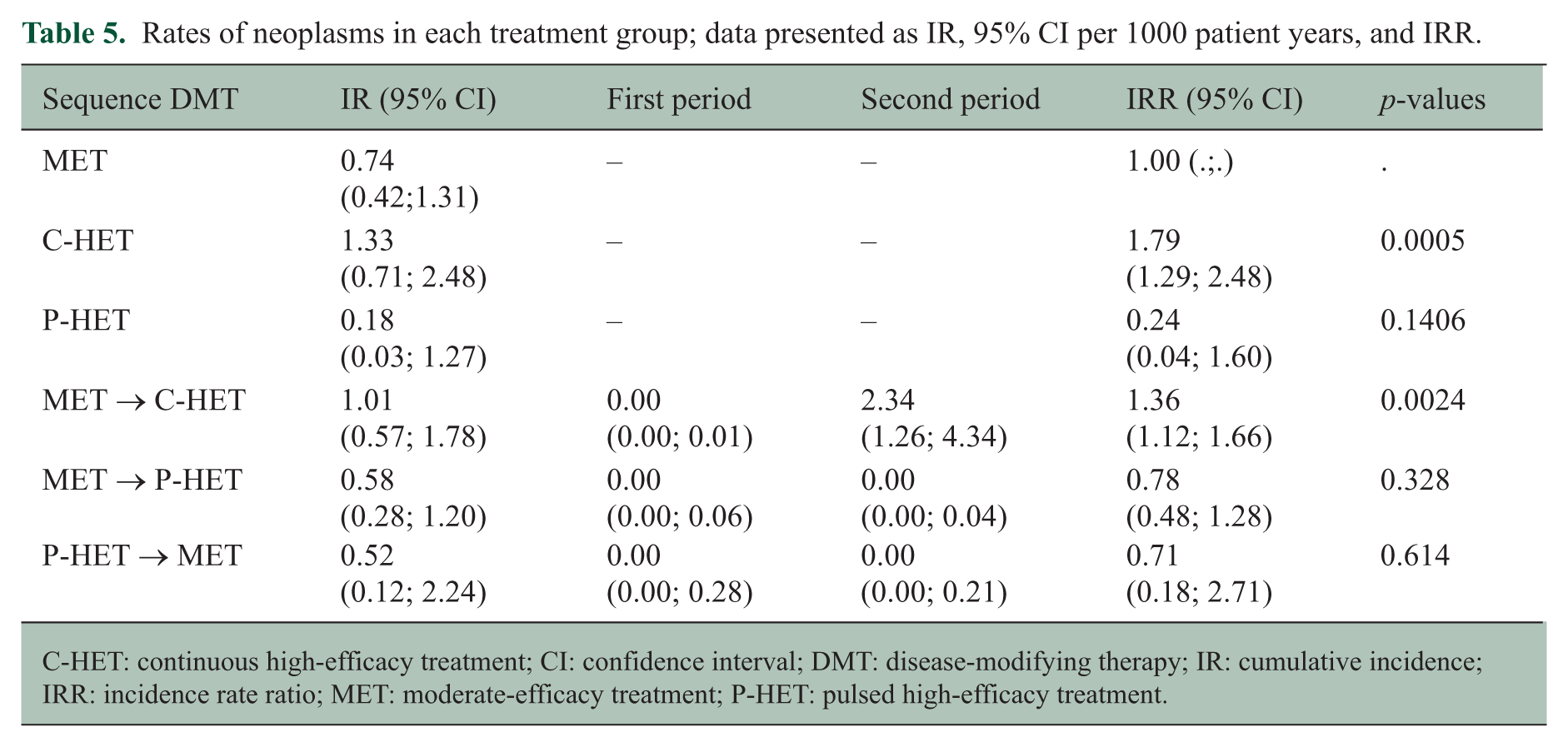
C-HET: continuous high-efficacy treatment; CI: confidence interval; DMT: disease-modifying therapy; IR: cumulative incidence; IRR: incidence rate ratio; MET: moderate-efficacy treatment; P-HET: pulsed high-efficacy treatment.
When stratified by treatment period, neoplasm risk in the MET→C-HET sequence was close to zero during the first period and emerged in the second (IR: 0.00 vs 2.34). Neoplastic events were exceedingly rare in both periods of MET→P-HET and P-HET→MET (Tables 5 and 6).
Distribution of events by sequence of DMDs.
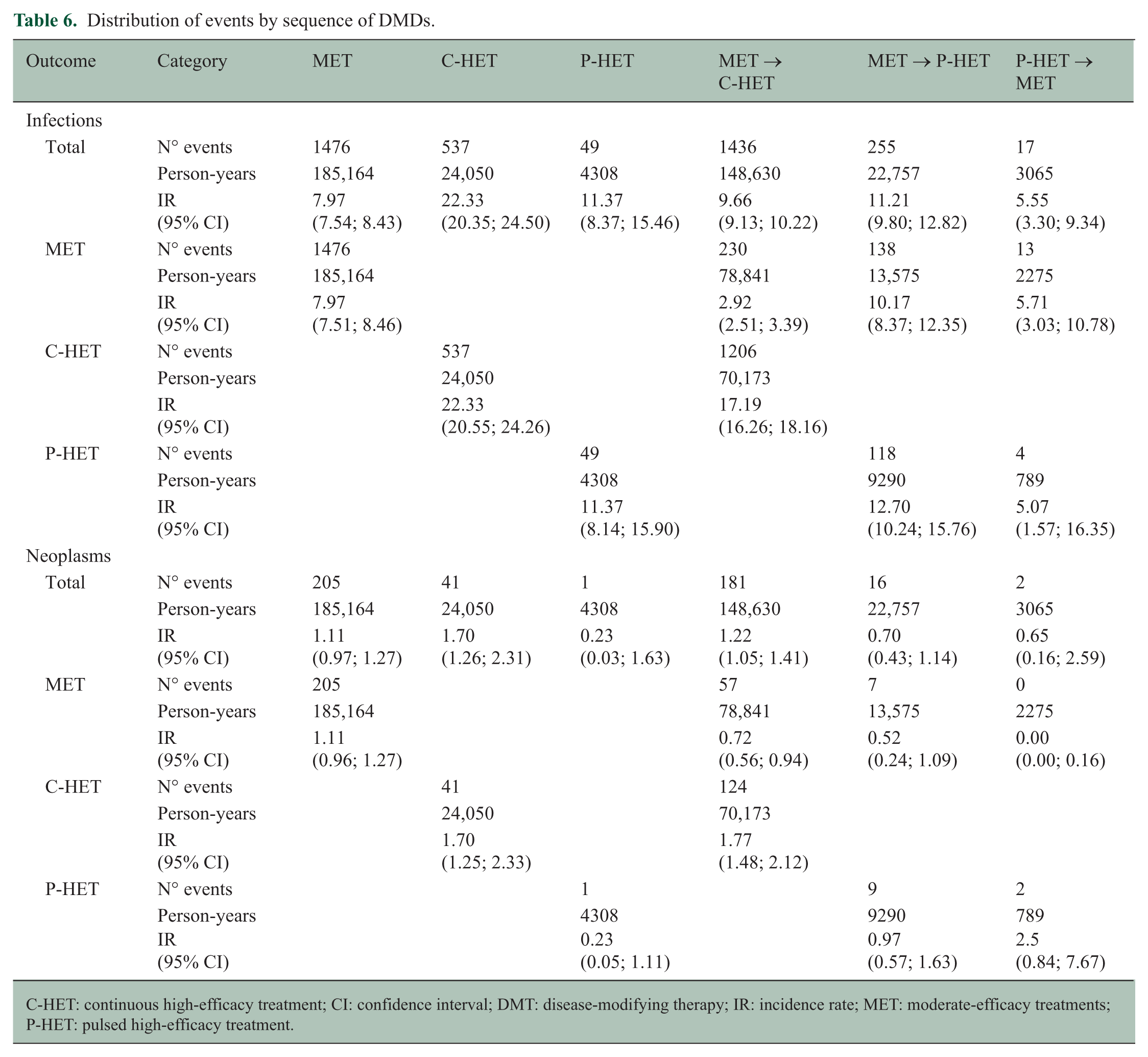
C-HET: continuous high-efficacy treatment; CI: confidence interval; DMT: disease-modifying therapy; IR: incidence rate; MET: moderate-efficacy treatments; P-HET: pulsed high-efficacy treatment.
Discussion
This is the first real-world study to compare the safety of different treatment sequences in a large national MS registry cohort, with a particular focus on long-term DMT safety – an aspect of intervention that has previously remained unexplored.13,14 Our findings demonstrate that therapeutic sequencing is a key driver of long-term safety, influenced not only by efficacy class but also by timing, order and cumulative duration of exposure.
This observation is meaningful; according to current datasets, continuous mechanisms (e.g. sustained B-cell depletion or lymphocyte sequestration) may accumulate infectious liability over time, while pulsed immune-reconstitution modalities, which allow intervals of immune recovery, do not appear to exhibit a progressive increase in long-term infection or malignancy signals. 15 The higher incidence of serious infections observed in our cohort treated exclusively with C-HET is consistent with previous registry and real-world studies reporting increased infection rates under anti-CD20 monoclonal antibody therapy, such as RTX and OCRE, as well as treatment with FNG and NTZ.16–19 As expected in real-world settings influenced by disease severity, patients treated exclusively with C-HET had higher baseline EDSS scores and greater pre-treatment relapse activity than those on other therapeutic sequences, introducing potential confounding. Multivariable adjustment for baseline disease severity confirmed that the elevated infection risk was independent of disease status, supporting a pharmacological rather than disease-related effect.
Our findings on infection are also consistent with recent observational evidence regarding anti-CD20 exposure, where hypogammaglobulinaemia is frequent and correlates with a higher risk of serious infections. These findings support immunoglobulin monitoring and the implementation of preventive strategies such as optimized vaccination timing, interval management and intravenous immunoglobulin supplementation in selected cases.20,21 Furthermore, patients following an ESC strategy – both MET to C-HET and MET to P-HET – displayed higher infection rates than those maintained on MET alone, suggesting that sequential exposure to multiple immunosuppressive mechanisms may amplify infection susceptibility through cumulative effects on immune competence.
CLAD and ALEM, prototypical P-HET agents, have shown sustained long-term safety in dedicated extension studies and real-world cohorts.22,23 In our registry cohort, however, patients treated exclusively with P-HET showed a significantly elevated infection rate relative to MET-only, a finding that warrants further investigation in dedicated studies disaggregating individual P-HET agents.
Data on neoplasm prevalence and incidence in MS patients have been conflicting.24,25 Several studies have found that while malignancy risk in MS patients may not differ from the general population, the risk appears to be lower in male patients compared with female patients and increases with age.26,27 A review of the literature 28 indicated the need for stringent follow-up of MS patients requiring DMTs. No risk of malignancy has been reported with the use of immunomodulators, 29 although immunosuppressors could trigger carcinogenesis. An Italian study demonstrated that malignancy risk is higher in MS patients who have previously received immunosuppressor therapy compared with MS patients who have not. 30 Finally, the main finding of a recent systematic review and meta-analysis is that the pooled prevalence of cancer in MS patients who received a second-line long-term therapy, such as NTZ, was 2%, indicating that such treatment intervention is not related to a higher cancer risk. 31
Overall, neoplasm incidence in our cohort remained low and consistent with long-term data from real-world and pivotal extension studies across multiple DMTs, supporting the general notion that MS therapies do not substantially increase oncologic risk. Nonetheless, neoplasm risk was significantly increased, both in patients treated exclusively with C-HET and in those escalating from MET to C-HET. Notably, within the latter sequence, neoplasm risk was concentrated almost exclusively in the second treatment period. These findings may reflect a combination of cumulative immunosuppressive exposure and heightened clinical surveillance, together with a potential biological contribution from sustained impairment of immune surveillance mechanisms during prolonged treatment.15,20,21 Our results support the evolving framework of de-escalation, conceptualized as a planned reduction of treatment intensity after durable disease control, ageing or changing comorbidity profiles.
The ECTRIMS workshop consensus offers practical algorithms and cautions that risks differ by drug mechanism (e.g. higher rebound after withdrawal of anti-trafficking therapy, changes in kinetics following anti-CD20 therapy), emphasizing the need for individualized monitoring during therapy transitions. 32
In our cohort, the P-HET→MET sequence showed infection rates comparable to MET-only and numerically lower neoplasm rates, though neither difference reached statistical significance. These findings are consistent with the hypothesis that planned de-escalation after P-HET may represent a viable strategy in carefully selected patients, pending confirmation in larger cohorts.
Some limitations inherent to the observational, registry-based design of this study must be acknowledged. As with other retrospective cohort analyses, missing or inaccurate data recorded in the registry must be considered, together with the need for more systematic and complete data entry by participating centres to strengthen analyses.
The possibility of underestimating neoplasm incidence cannot be excluded due to incomplete registration of malignant events and the latency period associated with certain tumour types relative to the duration of follow-up. Nonetheless, the overall median treatment duration of 8.8 years represents one of the most extended follow-up periods available in real-world MS registry research, which partially mitigates this concern. Furthermore, comorbidity and prior corticosteroid exposure were not included in the multivariable adjustment because these variables are often underreported in registry data, and their systematic ascertainment could not be ensured.
In addition, immunoglobulin levels were not collected within the registry, preventing any assessment of treatment-induced hypogammaglobulinaemia, a recognized risk factor for serious infections. Moreover, period-specific analyses, particularly for neoplasms, should be interpreted cautiously given the limited number of outcome events, which may reduce the robustness of these estimates. Despite these limitations, the I-MS&RD represents a unique source of long-term real-world safety data.
Conclusion
This is the first study on the influence of different therapeutic sequences on the risk of severe infections and neoplasms in a large cohort of MS patients under real-life conditions using data from the I-MS&RD. In contrast with previous years, numerous agents are now available in clinical practice and, as such, HETs are increasingly being prescribed to treatment-naïve patients or as part of an ESC strategy. Therefore, clinical practitioners need to know the risk profile of the therapeutic strategy selected for a given patient. Our findings can play an important role in this respect by providing additional safety information regarding different treatment sequences. Our results suggest that an ESC strategy is not clearly safer than an EIT approach. After multivariate adjustment among HETs, C-HET was associated with the highest cumulative risk of serious infections and neoplasms, whereas P-HET showed the lowest neoplasm incidence. Planned de-escalation following P-HET showed infection rates comparable to MET-only and a numerically lower neoplasm rate, suggesting that treatment de-intensification may represent a safe long-term strategy in appropriate patients, pending confirmation in larger cohorts. Further multicentre registry analyses will be essential to confirm and expand these observations.
Supplemental Material
sj-docx-1-msj-10.1177_13524585261457317 – Supplemental material for Profiling the long-term risk of severe adverse events in a cohort of multiple sclerosis patients treated with different treatment sequences: Results from the Italian Multiple Sclerosis and Related Disorders Registry (I-MS&RD) (ProSA study)
Supplemental material, sj-docx-1-msj-10.1177_13524585261457317 for Profiling the long-term risk of severe adverse events in a cohort of multiple sclerosis patients treated with different treatment sequences: Results from the Italian Multiple Sclerosis and Related Disorders Registry (I-MS&RD) (ProSA study) by Damiano Paolicelli, Giuseppe Lucisano, Alessia Manni, Pietro Iaffaldano, Marta Simone, Antonio Iaffaldano, Tommaso Guerra, Vincenzo Mangialardi, Francesco Patti, Eleonora Cocco, Giovanna De Luca, Pietro Annovazzi, Paolo Ragonese, Carlo Pozzilli, Matilde Inglese, Paola Perini, Claudio Gasperini, Carla Tortorella, Girolama Alessandra Marfia, Diana Ferraro, Giacomo Lus, Marika Vianello, Maria Assunta Rocca, Massimo Filippi, Antonella Conte, Silvia Romano, Vincenzo Brescia Morra, Alessandra Lugaresi, Alessia Di Sapio, Clara Grazia Chisari, Raffaella Cerqua, Umberto Aguglia, Ilaria Pesci, Carlo Avolio, Emanuele D’Amico, Roberto Bergamaschi, Rocco Totaro, Marco Rovaris, Sebastiano Crisafulli, Massimiliano Mirabella, Paola Cavalla, Roberta Fantozzi, Antonio Gallo, Maria Pia Amato, Massimo Filippi and Maria Trojano in Multiple Sclerosis Journal
Supplemental Material
sj-jpg-1-msj-10.1177_13524585261457317 – Supplemental material for Profiling the long-term risk of severe adverse events in a cohort of multiple sclerosis patients treated with different treatment sequences: Results from the Italian Multiple Sclerosis and Related Disorders Registry (I-MS&RD) (ProSA study)
Supplemental material, sj-jpg-1-msj-10.1177_13524585261457317 for Profiling the long-term risk of severe adverse events in a cohort of multiple sclerosis patients treated with different treatment sequences: Results from the Italian Multiple Sclerosis and Related Disorders Registry (I-MS&RD) (ProSA study) by Damiano Paolicelli, Giuseppe Lucisano, Alessia Manni, Pietro Iaffaldano, Marta Simone, Antonio Iaffaldano, Tommaso Guerra, Vincenzo Mangialardi, Francesco Patti, Eleonora Cocco, Giovanna De Luca, Pietro Annovazzi, Paolo Ragonese, Carlo Pozzilli, Matilde Inglese, Paola Perini, Claudio Gasperini, Carla Tortorella, Girolama Alessandra Marfia, Diana Ferraro, Giacomo Lus, Marika Vianello, Maria Assunta Rocca, Massimo Filippi, Antonella Conte, Silvia Romano, Vincenzo Brescia Morra, Alessandra Lugaresi, Alessia Di Sapio, Clara Grazia Chisari, Raffaella Cerqua, Umberto Aguglia, Ilaria Pesci, Carlo Avolio, Emanuele D’Amico, Roberto Bergamaschi, Rocco Totaro, Marco Rovaris, Sebastiano Crisafulli, Massimiliano Mirabella, Paola Cavalla, Roberta Fantozzi, Antonio Gallo, Maria Pia Amato, Massimo Filippi and Maria Trojano in Multiple Sclerosis Journal
Footnotes
Author contributions
All authors contributed to the conception and design of the study. Damiano Paolicelli and Giuseppe Lucisano performed material preparation, data collection and analysis. The first draft of the manuscript was written by Damiano Paolicelli, and all authors commented on the first draft as well as subsequent revisions. All authors read and approved the final manuscript.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: D.P. has received honoraria for advisory board membership and speaking activities, travel support, research grants, consulting fees or clinical trial support from Biogen, BMS-Celgene, Sanofi-Genzyme, Merck, Novartis and Roche. G.L. has received honoraria for advisory board membership and speaking activities, and/or travel expenses for attending congresses and meetings from Almirall, Biogen Idec, Merck Serono, Mylan, Novartis, Roche, Sanofi-Genzyme and Teva. A.M. has received travel support and advisory board or speaker’s honoraria from Biogen, Sanofi-Genzyme, Roche, Merck, Novartis and BMS outside of the submitted work. P.I. has received honoraria for lecturing and participation in advisory boards, and/or travel expenses for attending congresses and meetings from Almirall, Biogen Idec, Merck Serono, Mylan, Novartis, Roche, Sanofi-Genzyme and Teva. M.S. declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article. A.I. declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article. T.G. declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article. V.M. declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article. F.P. has received honoraria for speaking activities from Almirall and honoraria for speaking activities and advisory board membership from Bayer Schering, Biogen Idec, Merck Serono, Novartis, Roche, Sanofi-Genzyme and Teva; he has been funded by Pfizer and the Fondazione Italiana Sclerosi Multipla for epidemiological studies and has received grants for congress participation from Almirall, Bayer Shering, Biogen Idec, Merck Serono, Novartis, Roche, Sanofi-Genzyme and Teva. E.C. declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article. G.D.L. has received advisory board/speaker’s honoraria, travel support, research grants, consulting fees or clinical trial support from Actelion, Allergan, Almirall, Bayer Schering, Biogen, Celgene, EXCEMED, Genzyme, Forward Pharma, Ipsen, MedDay, Merck, Merz, Mylan, Novartis, Sanofi, Roche, Teva and their local affiliates. P.A. declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article. P.R. has received advisory board/speaker’s honoraria, travel support, research grants, consulting fees or clinical trial support from Actelion, Allergan, Almirall, Bayer Schering, Biogen, Celgene, EXCEMED, Genzyme, Forward Pharma, Ipsen, MedDay, Merck, Merz, Mylan, Novartis, Sanofi, Roche, Teva and their local affiliates. C.P. has received grants from Roche and Novartis, and personal fees from BMS, Alexion and Merck outside of the submitted work. M.I. declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article. P.P. declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article. C.G. has received speaker fees or travel expenses from Biogen, Merck Serono, Teva, Sanofi, Novartis and Genzyme. C.T. has received honoraria for speaking engagements and advisory board membership from Alexion, Biogen, BMS-Celgene, Horizon Therapeutics, Genzyme, Merck, Novartis and Roche. G.A.M. is an advisory board member for Biogen Idec, Genzyme, Merck Serono, Novartis, Almirall, Alexion and Roche and has received honoraria for speaking or consultation from Alexion, Almirall, Bayer Schering, Biogen Idec, Merck Serono, Novartis, Sanofi-Genzyme, Roche, Janssen, Viatris and BMS. She is the principal investigator in clinical trials for Biogen Idec, Merck Serono, Novartis, Roche and Sanofi-Genzyme. D.F. declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article. G.L. declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article. M.V. has received advisory board/speaker honoraria, travel support, research grants, consulting fees or clinical trial support from Actelion, Allergan, Almirall, Bayer Schering, Biogen, Celgene, EXCEMED, Genzyme, Forward Pharma, Ipsen, MedDay, Merck, Merz, Mylan, Novartis, Sanofi, Roche, Teva and their local affiliates. M.A.R. declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article. A.C. declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article. S.R. declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article. V.B.M. has received advisory board/speaker’s honoraria, travel support, research grants, consulting fees or clinical trial support from Actelion, Allergan, Almirall, Bayer Schering, Biogen, Celgene, EXCEMED, Genzyme, Forward Pharma, Ipsen, MedDay, Merck, Merz, Mylan, Novartis, Sanofi, Roche, Teva and their local affiliates. A.L. has received personal compensation from Alexion, Amgen/Horizon, Biogen, BMS-Celgene, Janssen/Johnson&Johnson, Merck Serono, Novartis, Roche, Sanofi-Genzyme and the Fondazione Italiana Sclerosi Multipla. She has also received institutional research grants from Novartis, Roche and Sanofi-Genzyme. A.D.S. declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article. C.G.C. has received grants for congress participation from Almirall, Biogen Idec, Merck Serono, Novartis, Roche, Sanofi-Genzyme and Teva. R.C. declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article. U.A. declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article. I.P. has received advisory board/speaker’s honoraria, travel support, research grants, consulting fees or clinical trial support from Actelion, Allergan, Almirall, Bayer Schering, Biogen, Celgene, EXCEMED, Genzyme, Forward Pharma, Ipsen, MedDay, Merck, Merz, Mylan, Novartis, Sanofi, Roche, Teva and their local affiliates. C.A. declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article. E.D. declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article. R.B. has received grants from Biogen, Merck Serono, Roche, Novartis and Sanofi-Genzyme, as well as personal fees from Biogen, Merck Serono, Roche, Novartis, Celgene, Janssen and Sanofi-Genzyme outside of the submitted work. R.T. has received advisory board/speaker’s honoraria, travel support, research grants, consulting fees or clinical trial support from Actelion, Allergan, Almirall, Bayer Schering, Biogen, Celgene, EXCEMED, Genzyme, Forward Pharma, Ipsen, MedDay, Merck, Merz, Mylan, Novartis, Sanofi, Roche, Teva and their local affiliates. M.R. has received personal fees from Biogen, BMS, Eli Lilly, Janssen, Roche, AstraZeneca, Bromatech, Celgene, Genzyme, Horizon Therapeutics Italy, Merck Serono S.p.A., Novartis, Roche, Sanofi and Teva outside of the submitted work. S.C. declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article. M.M. has received compensation for consulting services, speaking activities and advisory board activities from Alexion, Almirall, Bayer, Biogen, BMS, Celgene, CSL Behring, Novartis, Roche, Sanofi-Genzyme, Janssen, Merck Serono and Viatris; he has also received research support from Biogen, Merck Serono, Novartis and Roche. P.C. has received travel support, honoraria for speaking and advisory board membership from Alexion, Biogen, BMS-Celgene, Merck Serono, Roche, Novartis, Sanofi-Genzyme, Janssen and Horizon. R.F. declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article. A.G. declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article. M.P.A. has received grants from Biogen, Merck, Novartis, Roche and Sanofi-Genzyme, and personal fees from Biogen, Merck, Novartis, Roche, Sanofi-Genzyme, BMS-Celgene, Janssen, Horizon, Teva and Bayer outside of the submitted work. M.F. is Editor-in-Chief of the Journal of Neurology and Associate Editor of Human Brain Mapping, Neurological Sciences and Radiology (Neuroradiology). He has received compensation for consulting services from Alexion, Almirall, Biogen, Merck, Novartis, Roche and Sanofi; compensation for speaking activities from Bayer, Biogen, Celgene, Chiesi Italia SpA, Eli Lilly, Genzyme, Janssen, Merck Serono, Neopharmed Gentili, Novartis, Novo Nordisk, Roche, Sanofi, Takeda and Teva; compensation for advisory board participation for Alexion, Biogen, BMS, Merck, Novartis, Roche, Sanofi, Sanofi-Aventis, Sanofi-Genzyme and Takeda; compensation for scientific direction of educational events for Biogen, Merck, Roche, Celgene, BMS, Lilly, Novartis and Sanofi-Genzyme; M.F. also receives research support from Biogen Idec, Merck Serono, Novartis, Roche, the Italian Ministry of Health, Fondazione Italiana Sclerosi Multipla and ARiSLA (Fondazione Italiana di Ricerca per la SLA). M.T. has received advisory board and speaker’s honoraria and institutional research grants from Biogen, Merck Serono and Novartis.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethical considerations
This study was conducted using longitudinal, prospectively collected clinical data extracted from the Italian Multiple Sclerosis and Related Disorders Register (I-MS&RD). The I-MS&RD was approved by the Ethics Committee of the Azienda Ospedaliero-Universitaria Policlinico of Bari (Study ID: REGISTRO SM001, approved on 8 July 2016) and by the local ethics committees of all participating centres. The study was conducted in accordance with the Declaration of Helsinki.
Consent to participate
All patients provided written informed consent allowing the use of their demographic and clinical data for research purposes.
Consent for publication
Not applicable.
ORCID iDs
Data availability statement
Data will be made available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.