
Abstract
Background:
The therapeutic landscape of multiple sclerosis (MS) has evolved substantially with earlier diagnosis and increasing use of highly effective disease-modifying therapies, leading to marked reductions in relapse activity and delayed disability progression. Despite these advances, cognitive impairment remains highly prevalent.
Objective:
This topical review summarises current evidence on cognitive impairment in MS, from the earliest and preclinical stages to paediatric and ageing populations.
Results:
Particular emphasis is placed on emerging data-driven cognitive phenotypes, which capture the multidimensional nature of cognitive dysfunction and link distinct cognitive profiles to specific neuroimaging substrates. The review also discusses key neurobiological mechanisms underlying cognitive decline, including grey matter pathology, network dysfunction and synaptic alterations, as well as cognitive progression independent of relapse activity.
Conclusions:
Cognitive impairment represents a major source of disability. Implications for cognitive monitoring and management are considered, highlighting cognition as a core outcome and therapeutic target in contemporary MS care.
Introduction
Over the past two decades, the management of multiple sclerosis (MS) has changed profoundly. Earlier diagnosis, driven by revised diagnostic criteria and greater disease awareness, 1 together with the increasing availability of highly effective disease-modifying therapies (DMTs), has resulted in a marked reduction in relapse rates and a delay in the accumulation of physical disability. Long-term outcomes for many people with MS have improved substantially, although residual disability accrual and silent progression, often referred to as progression independent of relapse activity (PIRA), are increasingly recognised. 2
In this evolving therapeutic landscape, the relevance of cognitive impairment warrants renewed attention. Data from large international patient-reported outcome initiatives consistently identify cognitive difficulties among the most prevalent and impactful symptoms experienced by people with MS. These deficits are often described as ‘invisible’, yet they exert a profound influence on disease self-management, social participation and quality of life. Importantly, cognitive impairment represents one of the leading causes of work reduction or cessation, even in individuals with low physical disability.
This apparent mismatch between improved control of inflammatory disease activity and the persistent burden of cognitive dysfunction highlights cognition as a core dimension of MS-related disability. The present topical review summarises current evidence on cognitive impairment across the MS disease course and lifespan, with a focus on emerging data-driven cognitive phenotypes, underlying neurobiological mechanisms of cognitive progression beyond relapses and implications for clinical monitoring and management.
Cognitive impairment across the MS disease course and lifespan
Although early clinical descriptions by Charcot already recognised cognitive and behavioural changes in MS, such symptoms were long considered anecdotal or of limited clinical relevance. A paradigm shift occurred in the late 20th century with the establishment of neuropsychology as a recognised discipline and the development of standardised cognitive assessment batteries. In parallel, the introduction of magnetic resonance imaging (MRI) provided a window into the structural and functional substrates of cognitive dysfunction. Seminal studies demonstrated that cognitive impairment is common, clinically meaningful and closely linked to brain pathology, challenging the notion that it represents a late manifestation of disease. 3
Subsequent research has consistently shown that cognitive impairment occurs across all MS phenotypes and stages. Overall prevalence estimates range between 34% and 65%, increasing along the disease course and particularly in progressive forms. Information processing speed, learning and memory, executive function and visuospatial processing are most frequently involved. Importantly, cognitive impairment is already detectable in approximately one-third of individuals with clinically isolated syndrome (CIS), indicating that cognitive dysfunction can emerge very early. 4 Moreover, subtle cognitive changes may precede the appearance of classic neurological symptoms, suggesting that cognitive vulnerability may be part of the earliest disease processes.
Evidence from radiologically isolated syndrome (RIS) further supports this view. Even at this preclinical stage, approximately 28% of individuals exhibit subtle cognitive deficits, which have been associated with reduced total brain and cortical volumes. 5 These findings mirror patterns observed in CIS and early relapsing MS, reinforcing the concept that cognitive impairment is linked to neurodegenerative processes that may precede overt clinical disease.
Longitudinal studies in early MS have provided important insights into the evolution of cognitive impairment. While cross-sectional data demonstrate a relatively high prevalence of cognitive dysfunction already at the CIS stage, longitudinal analyses reveal marked inter-individual variability. It has to be noted that the functional impact of cognitive impairment is highly variable, as thresholds for perceiving or reporting cognitive change may differ according to vocational and social demands and daily cognitive requirements. Overall, some patients remain cognitively stable for years, whereas others experience early decline. 3 The concept of cognitive reserve offers a useful framework to explain inter-individual variability. Cognitive reserve, shaped by education, intellectual enrichment and lifestyle factors, reflects the brain’s ability to maintain function despite structural damage. In longitudinal studies, individuals with higher cognitive reserve are more resilient to MS-related brain injury and may experience delayed onset or reduced severity of cognitive impairment. 6
Paediatric-onset MS represents a particularly vulnerable condition, as disease onset coincides with critical periods of brain growth and maturation. Cognitive and behavioural difficulties in children and adolescents with MS may be disproportionate to physical disability and can interfere with academic performance and psychosocial development. Earlier studies reported prevalence rates approaching 30%, whereas more recent cohorts suggest slightly lower estimates, possibly reflecting earlier diagnosis and increasing use of highly effective therapies.7,8
Nevertheless, longitudinal studies reveal marked heterogeneity in individual trajectories, with stability, deterioration or partial improvement over time. Importantly, early cognitive worsening may reflect not only loss of function but also a failure to achieve age-expected cognitive gains, particularly in younger individuals. Moreover, early cognitive impairment has been associated with reduced educational and occupational attainment in adulthood, as well as increased psychiatric comorbidity, findings corroborated by large population-based studies.9,10
At the other end of the lifespan, the MS population is ageing, and age itself represents a major driver of cognitive decline. Normal ageing processes interact with MS-related neurodegeneration, potentially accelerating cognitive deterioration. Recent studies using artificial intelligence–based approaches suggest that the brains of people with MS appear biologically older than their chronological age, on average by a decade or more. 11 These observations highlight the complex interplay between ageing and disease-specific mechanisms in shaping long-term cognitive outcomes.
Data-driven cognitive phenotypes
Recent work has moved beyond dichotomous classifications of cognitive impairment towards data-driven approaches that recognise cognition as a continuum and explicitly account for its multidimensional nature. Using multivariate and unsupervised methods, several studies have identified distinct cognitive phenotypes, characterised by specific patterns of cognitive performance and associated neuroimaging features. This approach has helped to reconcile the marked clinical heterogeneity observed in cognitive outcomes with underlying biological substrates.
In a large multicentre study employing latent profile analysis, five major cognitive phenotypes emerged, ranging from preserved cognition to severe multidomain impairment (Figure 1). Intermediate profiles were characterised by selective or predominant involvement of specific domains, including memory, information processing speed and executive functions. Importantly, these phenotypes were associated with age, disability levels and distinct MRI signatures, supporting their biological validity. Preserved or mildly affected phenotypes showed relatively limited structural damage, whereas more impaired profiles were characterised by increasing involvement of grey matter pathology, including thalamic, hippocampal and widespread cortical atrophy, as well as higher lesion burden and diffuse white matter damage. Notably, the most severe cognitive phenotype was associated with extensive network-level disruption, consistent with advanced neurodegenerative processes. In contrast, involvement of verbal memory and verbal fluency was related to younger age and lower disability levels, in line with recent reappraisal of cognition in the modern diagnostic and treatment era.12,13
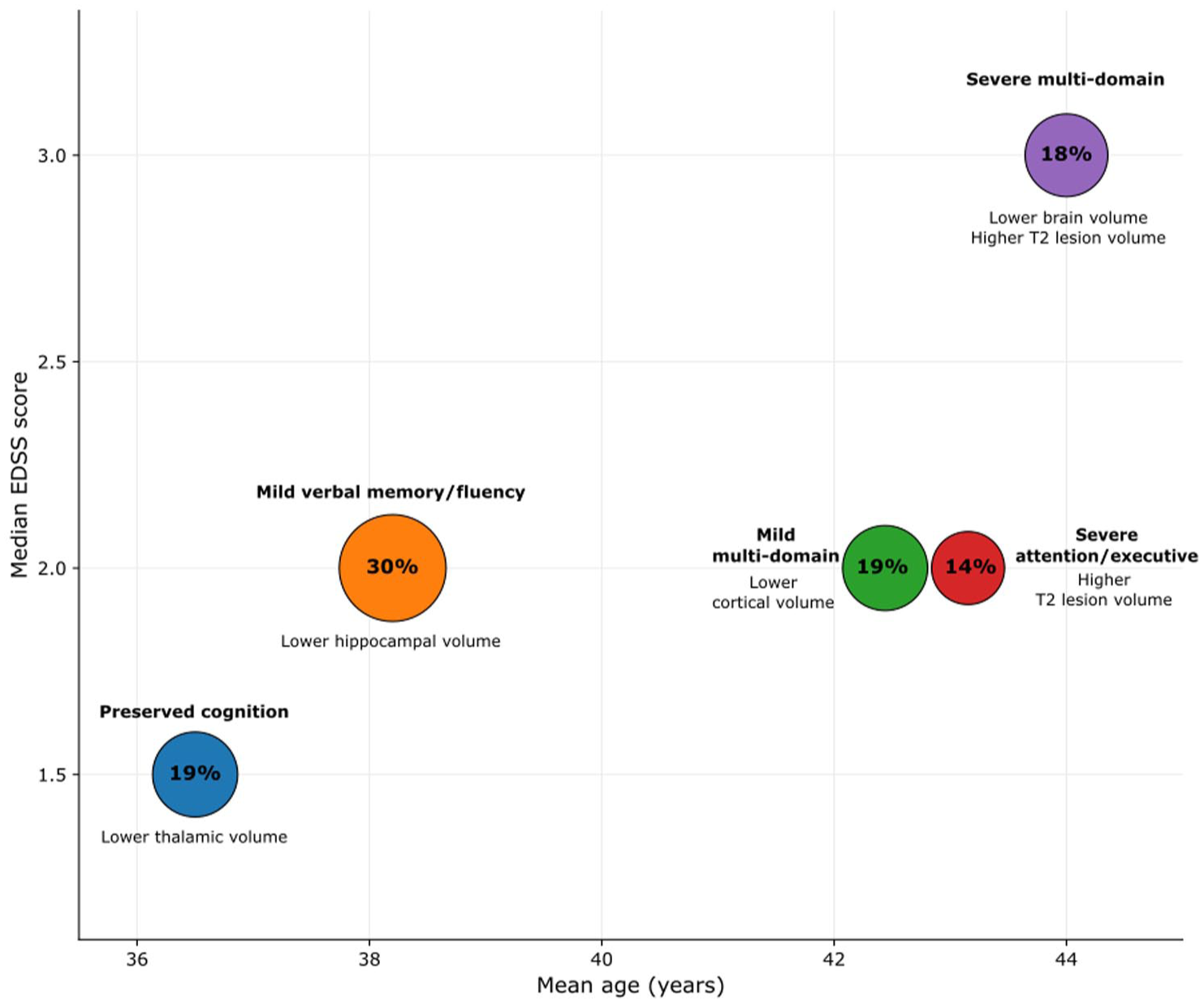
Cognitive phenotypes in MS and main MRI correlates according to age and disability.
Similar data-driven approaches from other cohorts have further refined this framework, identifying additional phenotypes characterised by selective visuospatial or memory dysfunction, and broadly replicating the association between specific cognitive profiles and regional patterns of brain damage. 14
Refinement of cognitive phenotyping has important implications for both research and clinical practice. In clinical trials, data-driven phenotypes may facilitate more precise stratification and the recruitment of biologically homogeneous patient groups, thereby increasing sensitivity to detect treatment effects. From a mechanistic perspective, this approach supports the development of targeted rehabilitative interventions tailored to the dominant substrates of cognitive dysfunction. In clinical practice, the phenotype can be assigned matching the patient’s pattern and severity of domain-specific impairments to the closest cluster-defined cognitive profile. Overall, data-driven cognitive phenotyping represents a significant step towards precision medicine in MS cognition research and may substantially improve the interpretability and translational relevance of future interventional studies.
Neurobiological substrates of cognitive impairment
A large body of imaging research has highlighted the multifactorial nature of cognitive impairment in MS. While focal and diffuse white matter damage contributes to a classical disconnection syndrome, grey matter pathology and network dysfunction are increasingly recognised as central determinants of cognitive decline.
Grey matter pathology has emerged as a strong determinant of cognitive impairment in MS. Both focal and diffuse cortical damage contribute to cognitive decline, independently of white matter lesion load. Cortical thinning has been observed early in the disease course and progresses over time, paralleling cognitive deterioration. In addition, the presence and accumulation of cortical lesions further exacerbate cognitive dysfunction.15–17
Among deep grey matter structures, the thalamus plays a central role as a strategic hub integrating information across distributed cortical networks. Thalamic atrophy is one of the earliest and most robust imaging correlates of global cognitive impairment in MS and has been shown to predict long-term cognitive outcomes. 18 Damage to other subcortical structures, including the hippocampus and basal ganglia, contributes to domain-specific deficits, particularly in memory and executive function. 19
Functional MRI studies provide insight into how the brain attempts to compensate for structural damage. Task-related studies suggest that individuals with preserved cognition can recruit additional task-relevant regions, often bilaterally. 20 Resting-state studies have highlighted dysfunction of large-scale networks, particularly the default mode network, which plays a central role in cognitive processing. 21 Network-based approaches suggest that early increases in functional connectivity may represent adaptive or compensatory mechanisms, whereas later changes may reflect maladaptive reorganisation and network inefficiency. Longitudinal data indicate that the transition from adaptive reorganisation to network failure may represent a critical tipping point in the development of overt cognitive impairment. 21
In addition to established markers of grey and white matter damage, several emerging imaging features have recently attracted attention as potential contributors to cognitive impairment in multiple sclerosis. Chronic active lesions, often identified as paramagnetic rim lesions on susceptibility-based MRI sequences, represent sites of compartmentalised inflammation and ongoing tissue injury. Although primarily studied in relation to physical disability progression, growing evidence suggests that a higher burden of paramagnetic rim lesions is associated with worse cognitive performance and accelerated cognitive decline, possibly through sustained microglial activation and downstream network disruption.22,23
Enlargement of the choroid plexus has also been proposed as a marker of chronic neuroinflammation in MS. The choroid plexus plays a key role in immune surveillance and cerebrospinal fluid homeostasis, and its enlargement has been linked to disease activity and progression. Recent studies indicate that choroid plexus volume may correlate with measures of global cognitive performance, suggesting that persistent inflammatory signalling at the brain–cerebrospinal fluid interface could contribute to diffuse cognitive dysfunction. 24
Finally, alterations of the glymphatic system have emerged as a novel area of investigation. The glymphatic pathway is involved in the clearance of metabolic waste products from the brain and is linked to sleep and vascular function. Early evidence, including paediatric MS studies, suggests that glymphatic dysfunction may be present in MS and could contribute to impaired brain homeostasis and cognitive decline. 25 Although these markers remain exploratory, their integration with established measures of structural damage and network dysfunction may help refine mechanistic models of cognitive impairment and identify new targets for monitoring and intervention.
At the synaptic level, inflammatory mediators have been shown to impair synaptic plasticity, linking neuroinflammation to network dysfunction and cognitive decline. Loss of long-term potentiation and synaptic integrity may represent a critical step towards network collapse.26,27 Preserving synaptic function and plasticity may, therefore, represent an important therapeutic goal aimed at maintaining network efficiency and delaying the emergence of clinically overt cognitive impairment.
Together, these findings support a model in which cognitive decline results from the progressive disruption of structurally and functionally integrated brain networks, driven by a combination of grey matter pathology, disconnection and synaptic dysfunction.
Cognitive progression independent of relapse activity
Cognitive worsening in MS may occur independently of overt inflammatory activity. One recognised mechanism involves isolated cognitive relapses, in which cognitive decline represents the sole clinical manifestation. Such episodes may be accompanied by MRI activity, but recovery is often incomplete. 28 Over time, the cumulative effect of isolated cognitive relapses may contribute to progressive cognitive disability. 3
More commonly, cognitive decline evolves through silent and insidious mechanisms, often referred to as cognitive PIRA, as worsening performance during relapses can recover over time. 29 Longitudinal studies have demonstrated that the majority of cognitive decline events occur independently of clinical relapses and are not captured by worsening on the Expanded Disability Status Scale (EDSS) (Figure 2). 30 Similar findings have been reported in cohorts incorporating MRI activity, indicating that conventional clinical and radiological markers substantially underestimate the true burden of cognitive disease progression. 22
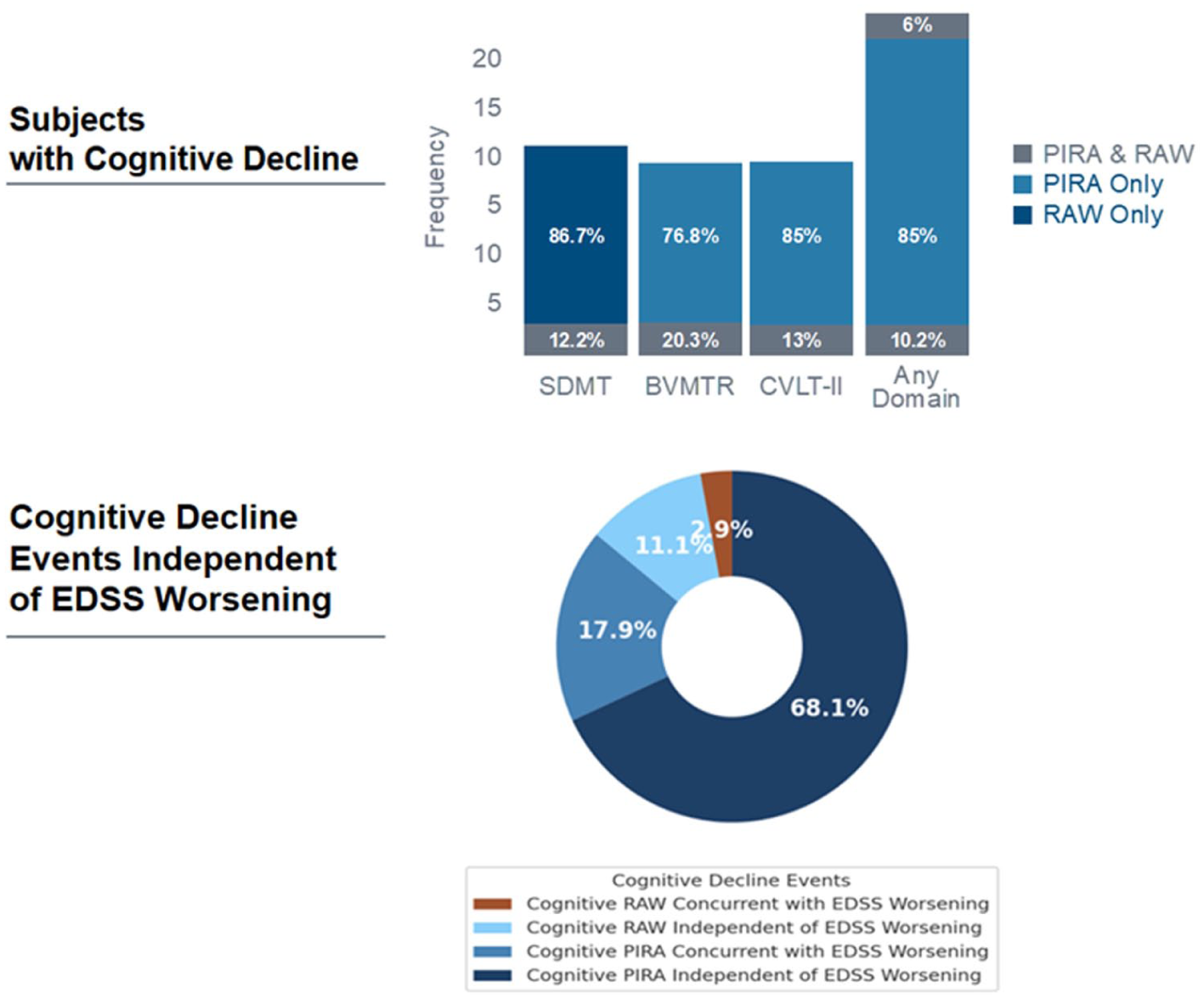
Cognitive progression independent of relapse activity.
The concept of cognitive PIRA extends current models of disease progression by explicitly acknowledging cognition as a domain in which disability may accumulate independently of relapses. Unlike physical disability progression, cognitive decline often remains clinically silent unless systematically assessed, contributing to its under-recognition in routine practice.
Importantly, cognitive PIRA appears to be only weakly associated with conventional MRI measures of inflammatory activity. This dissociation highlights a limitation of traditional outcome measures and supports the need for cognitive-specific endpoints. From a clinical perspective, recognising cognitive PIRA reinforces the importance of regular cognitive monitoring, even in patients who appear clinically stable, and raises questions regarding treatment response, as suppression of inflammatory activity alone may be insufficient to prevent cognitive decline in a subset of patients. 22
Clinical management: current status
International guidelines now recommend regular cognitive monitoring in MS. The Symbol Digit Modalities Test is the most widely used screening tool and is complemented by validated neuropsychological batteries for a more comprehensive assessment. 31 Despite these advances, heterogeneity in definitions, thresholds and criteria for cognitive impairment and change limits comparability across studies and clinical practice.
The effects of DMTs on cognition remain an area of active investigation. While early clinical trials were not designed to assess cognitive outcomes, post hoc analyses and meta-analyses suggest that treatment-related benefits on cognition are modest. 32 Notably, emerging evidence indicates that preservation of brain volume may be more closely associated with cognitive outcomes than reduction in focal inflammatory activity, with meta-regression analyses showing stronger associations with brain atrophy than with lesion load. 33 Among high-efficacy therapies, recent post hoc analyses of randomised controlled trials investigating highly effective DMT have suggested potential benefits on cognitive function, often associated with reduced brain atrophy (Supplemental Table 1). Nevertheless, the overall efficacy of DMT on cognitive outcomes in MS remains uncertain. The systematic inclusion of neuropsychological measures among primary disability endpoints – capturing domains beyond processing speed, such as memory – together with the adoption of robust methods to assess cognitive change over time, may help to clarify their impact in the future.
Beyond pharmacological treatment, cognitive rehabilitation has gained increasing recognition as a meaningful component of MS care. Although effect sizes are generally modest, improvements in targeted cognitive domains can translate into tangible benefits for daily functioning. 34 Importantly, studies incorporating advanced imaging techniques suggest that cognitive rehabilitation may induce functional and structural plasticity within relevant brain networks. 35 Integrating rehabilitation with digital technologies and multimodal interventions may further enhance accessibility, adherence and long-term effectiveness.
Future directions and conclusions
Cognitive impairment remains a major unmet need in MS. Routine cognitive monitoring, validation of digital assessment tools, standardisation of biomarkers and prioritisation of cognition as a co-primary endpoint in clinical trials represent key future goals.
A shift from reactive to preventive strategies, treating cognition as a core therapeutic target from the earliest stages of MS, may make preservation of cognitive function an achievable objective in contemporary MS care. Integrating clinical vigilance, technological innovation and mechanistic research offers a realistic path towards improving cognitive outcomes for people living with MS.
Supplemental Material
sj-docx-1-msj-10.1177_13524585261457362 – Supplemental material for Cognitive impairment in multiple sclerosis: Where do we stand today?
Supplemental material, sj-docx-1-msj-10.1177_13524585261457362 for Cognitive impairment in multiple sclerosis: Where do we stand today? by Maria Pia Amato and Emilio Portaccio in Multiple Sclerosis Journal
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: M.P.A. served on scientific advisory boards for and has received speaker honoraria and research support from Biogen Idec, Merck Serono, Bayer Schering Pharma and Sanofi Aventis, and serves on the editorial boards of Multiple Sclerosis Journal and BMC Neurology. E.P. received compensation for travel grants, participation in advisory boards and/or speaking activities from Biogen, Merck Serono, Sanofi, Teva, Roche, BMS Celgene, Janssen and Novartis, and serves on the editorial board of Frontiers in Neurology and Brain Sciences.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethical considerations
Not applicable.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Data availability statement
Data sharing is not applicable to this article as no data sets were generated or analysed during this study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.